
 , Min-Yan Zhang 1, Shen Liu 1, Kang Li 1, Jun-Jie Fu 1, Peng Lin 1
, Min-Yan Zhang 1, Shen Liu 1, Kang Li 1, Jun-Jie Fu 1, Peng Lin 11 Department of Pediatric Urology, Fuzhou Children’s Hospital, 350001 Fuzhou, Fujian, China
Abstract
Background: Adnexal torsion in Children is a rare event, and oophoropexy for the prevention of adnexal torsion in children is still controversial. The aim of this study was to analyze how retorsion can be prevented. Method: We performed a retrospective review of hospital charts of all patients aged 0–18 years with a diagnosis of adnexal torsion at the fuzhou Children’s Hospital at Fujian province, from august 2014 to august 2019. Result: In total, 10 patients were included in the study. The average age of the patients was 5.5 years (range: 2 months–10 years). Clinical presentation: included pain(n = 9), vomiting(n = 3), and abdominal mass (n = 1). Surgical procedures included: laparoscopy (LP): cystectomy with detorsion (n = 5); cyst aspiration with detorsion (n = 1), and detorsion with oophoropexy (n = 2). One case underwent salpingo-oophorectomy LP (n = 1), which was converted to open laparotomhy Sapingo-oophorectomy. Recurrence occurred in two cases. Case 5 had recurrent adnexal torsion after oophoropexy with absorbable suture. The second episode was treated with oophoropexy with non-absorbable suture and multiple points fixed. During the operation, the right ovarian ligament was longer, and hypermobile. Case 6 had recurrent cyst aspiration and the second episode was treated with cystectomy with oophoropexy. During the operation, the ovarian ligament was hypermobile. Follow-up: ultrasound showed normal ipsilateral adnexal, and no ovarian atrophy in eight patients. Conclusion: The recurrence of ovarian torsion in children may be caused by ovarian etiology and abnormal ovarian ligaments. Oophoropexy can prevent ovarian retorsion with non-absorbable sutures and multiple points fixed.
Keywords
- Adnexal torsion
- Children
- Oophoropexy
- Recurrence
Adnexal torsion (AT) involves the twisting of all adnexal components (fallopian
tube and ovary) causing an impairment of blood flow. AT has a reported prevalence
of 2.7% and incidence of 4.9 per 100,000 women
We performed a retrospective review of hospital charts of all patients aged 2
months–18 years with a diagnosis of ovarian torsion at Fuzhou Children’s Hospital
in Fujian Province from August 2014 to August 2019. Patients were excluded if
they were
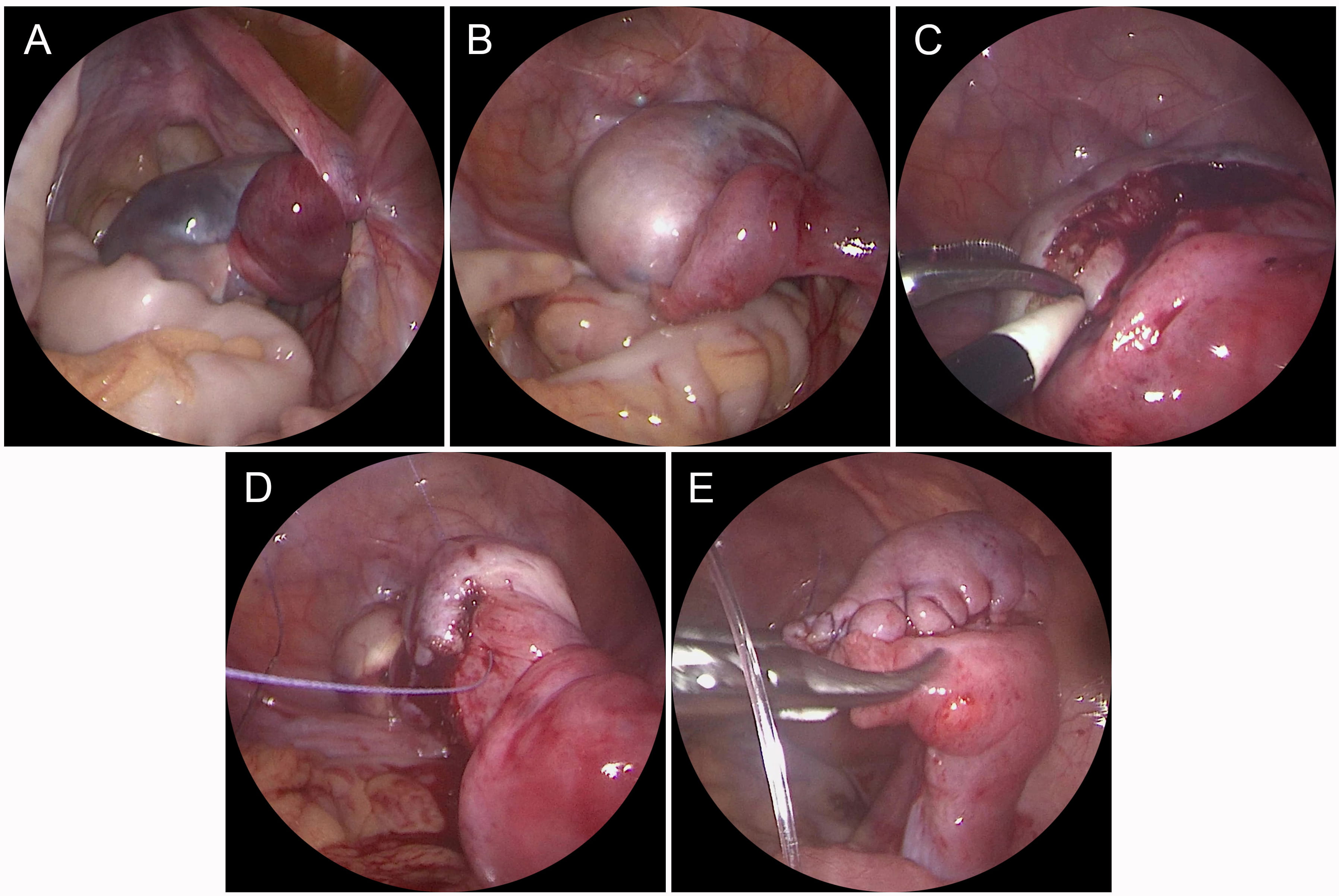
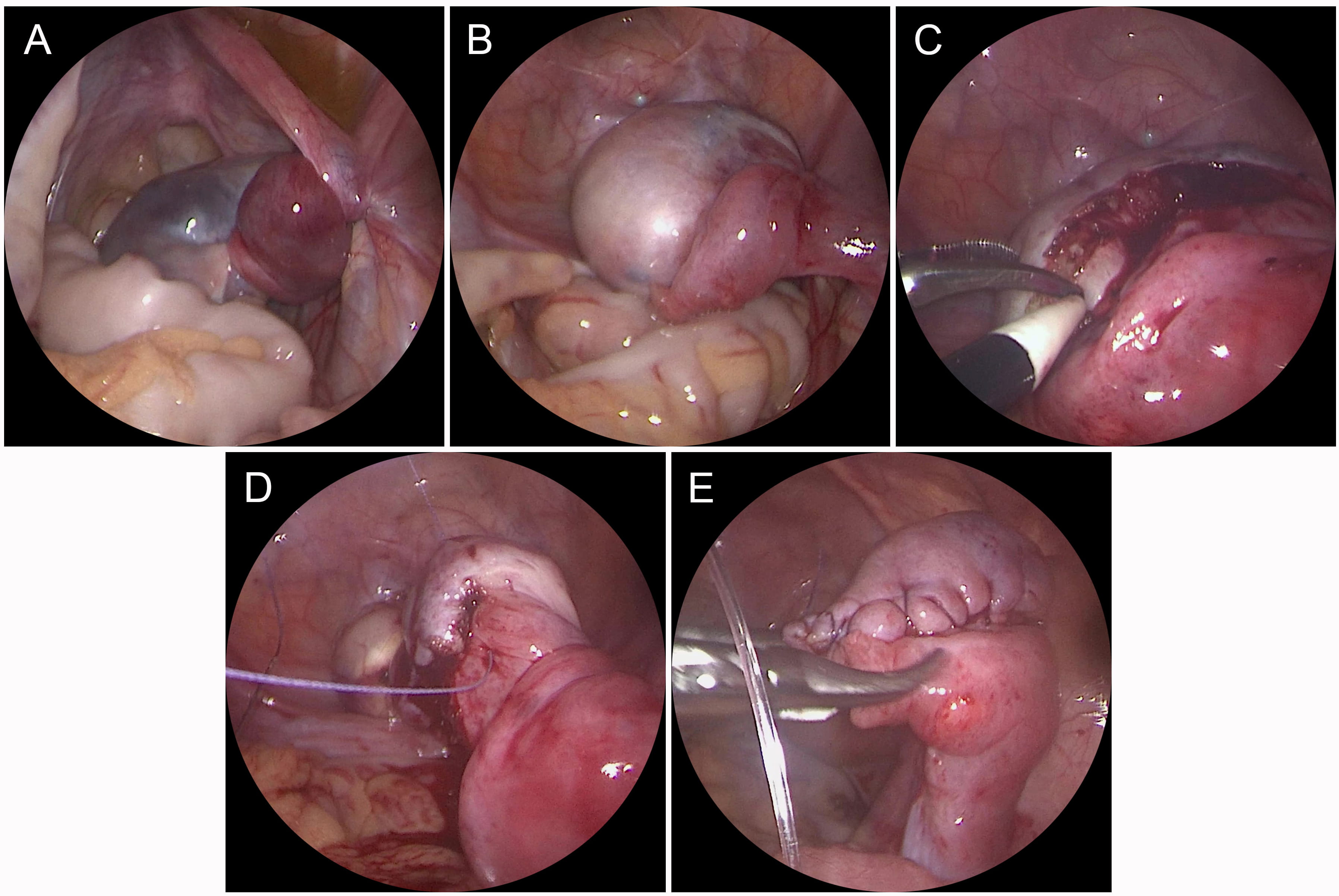 Fig. 1.
Fig. 1.Case 10 surgical procedure. (A) Right ovarian torsion
(720
| Case # | Age (years) | Clinical presentation | Diagnostic imaging | Surgical procedure | Pathology | Second surgical procedure | Follow-up(years) |
| 1 | 0.2 | Vomiting irritability distension | US: L (5.3 |
OP, Sapingo-oophorectomy | Ovarian cyst with hemorrhagic necrosis | - | 3 y, US: normal contralateral ovary |
| 2 | 2.3 | Pain, vomiting | US: L (4.2 |
LP, cystectomy with detorsion | Mature teratoma | - | 6 y, US: normal |
| 3 | 5 | Right lower quadrant pain | US: R (5.5 |
LP, cystectomy with detorsion | Simple ovarian cyst | - | 5 y, US: normal |
| 4 | 5.3 | Right lower quadrant pain | US: R (5.4 |
LP, cystectomy with detorsion | Mature teratoma | - | 4 y, US: normal |
| 5 | 8 | Right lower quadrant pain, vomiting | US: Right enlarged ovary, ascites (+), color Doppler blood flow (-), CT: enlarged ovary | LP, detorsion with oophoropexy (non-absorbable sutures and multi-point fixation to the back of the uterus) | - | LP, detorsion with oophoropexy (non-absorbable sutures and multi-point fixation to the back of the uterus) | 1.3 y, US: normal |
| 6 | 10 | Right lower quadrant pain | US: Right enlarged ovary, ascites (+), color Doppler blood flow (-), CT: enlarged ovary | LP, detorsion with oophoropexy (non-absorbable sutures and multi-point fixation to the back of the uterus) | - | - | 2 y, US: normal |
| 7 | 7 | Pain | US: R (4 |
LP, detorsion with aspiration cyst | Second episode: simple ovarian cyst | LP, cystectomy with detorsion and oophoropexy (non-absorbable sutures and multi-point fixation to the back of the uterus) | 2 y, US: ipsilateral ovary smaller than the contralateral one, but blood flow normal |
| 8 | 5.5 | Pain, vomiting | US: L (7.2 |
LP, cyst aspiration with cystectomy and detorsion | Mature teratoma | - | 5 y, US: normal |
| 9 | 9 | Pain, abdominal mass | US: R (10.0 |
LP converted to OP, Sapingo-oophorectomy | Mature teratoma with hemorrhagic necrosis | - | 2 y, US: normal contralateral ovary |
| 10 | 3.4 | Pain | US: R (5.5 |
LP, cystectomy with detorsion | Mature teratoma | - | 2 y, US: normal |
| (-), absent; (+), detection; LP, laparoscopy; OP, Open laparotomy; US, ultrasonography. | |||||||
Ten pediatric patients with AT were enrolled in this study. The mean (range) age of patients was 5.5 (0.2–10) years. All patients had a premenarchal status, and two patients experienced recurrent torsion. Clinical presentation included pain (n = 9), vomiting (n = 3), and abdominal mass (n = 1). Patients were divided into four groups based on their first surgical procedure: cystectomy with detorsion (n = 5); cyst aspiration with detorsion (n = 1); detorsion with oophoropexy (n = 2); and salpingo-oophorectomy (n = 2) (Table 1).
Overall, two patients had recurrence. Case 5 was a 10-year-old female with
premenarchal status. Her first surgical procedure involved LP, detorsion with
oophoropexy, and single-points fixation to the back of the uterus using
absorbable sutures (Fig. 2A). No postoperative complications were observed and
she was discharged four days postoperatively. Six months later, the patient
complained of acute lower quadrant pain after mountain-climbing. Her parents
brought the child to our attention again. Pre-operative ultrasound showed an
enlarged right ovary, and color Doppler ultrasound did not detect a vascular
signal. Therefore, the patient underwent an emergency laparoscopy. A
360
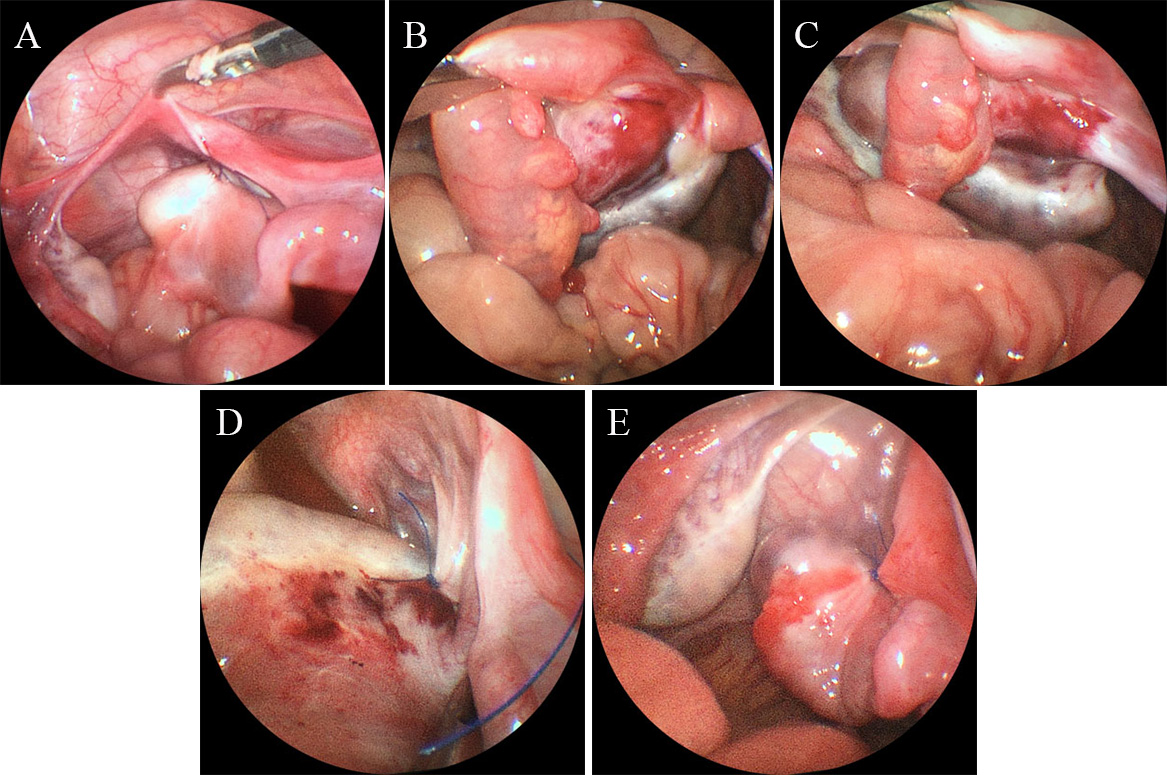
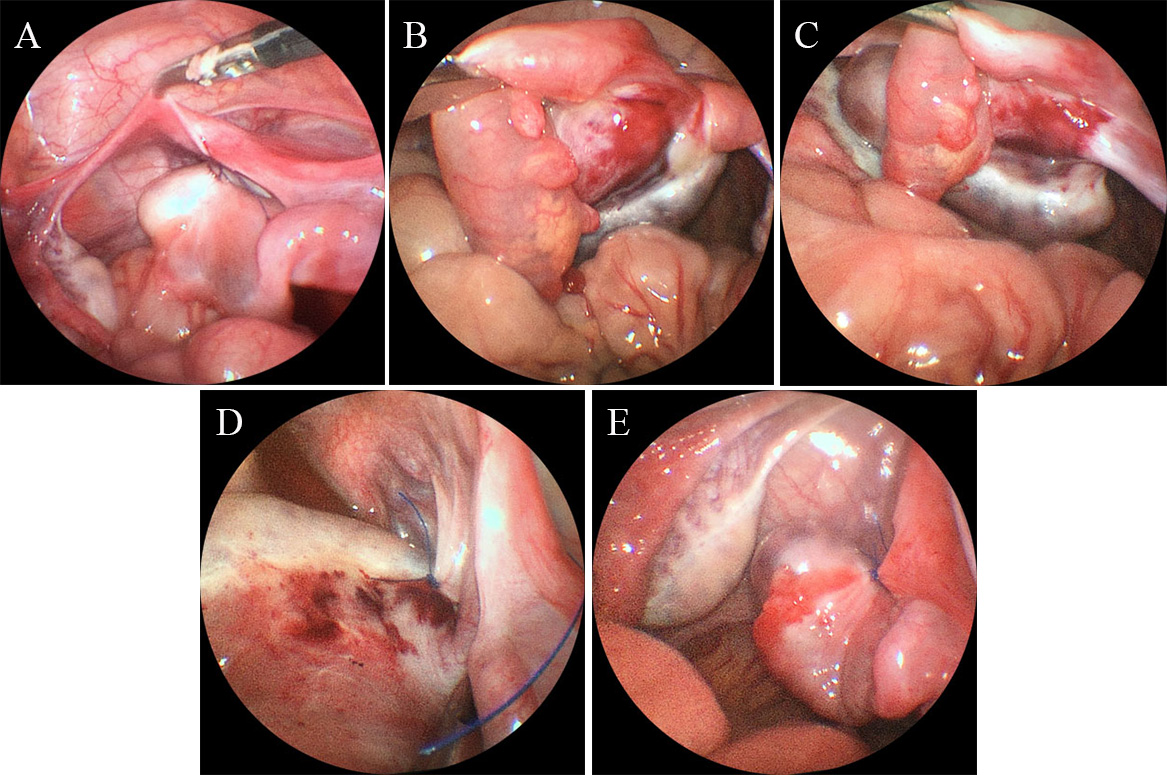 Fig. 2.
Fig. 2.Case 5 surgical procedure. (A) Ovarian fixation to the back of
the uterus using absorbable sutures and single-point fixation. (B) The
same patient underwent a second surgery due to ovarian torsion (360
Case 7 was a seven-year-old female who complained of acute right lower quadrant
pain. Ultrasound showed a right adnexal mass (4.0 cm
The average follow-up was 54.3 months. Ultrasound showed normal ipsilateral adnexal, and no ovarian atrophy was observed in eight patients.
In the present study, 10 children were enrolled, and the proportion of ovaries preserved reached 80%. A total of three children underwent oophoropexy. There were two cases of normal ovarian appearance and oophoropexy performed in the first operation. Recurrence occurred in case 5. In the second operation, we observed the original fixed sutures disappear and considered recurrence to be due to absorbable suture use and single-point fixation. Therefore, for case 6, we performed oophoropexy with non-absorbable sutures and muti-point fixation for the second operation. The postoperative effect was good, and there was no recurrence. Therefore, we suggest that oophoropexy should be performed with non-absorbable sutures and multi-point fixation in the first operation for children with normal ovarian appearance.
Many articles have shown that oophoropexy is beneficial in preventing ovarian
torsion. Yaniv [6] concluded that longer ovarian ligaments may correlate with the
development of ovarian torsion, similar to what we observed during surgery.
Bertozzi et al. [7] suggested that oophoropexy should be performed at
the first episode of torsion to eliminate the possibility of recurrence, which is
consistent with our point of view. The guidelines [2] recommend that oophoropexy
be considered in situations where the ovarian ligaments are congenitally long,
patients have repeat torsion, or when no obvious cause for the torsion can be
found; however, the technical details of oophoropexy in pediatric population was
no mentioned. Lucchetti et al. [8] also stated thatoophoropexy should be
performed with permanent sutures because absorbable sutures may completely
disappear without any residual scar, which was observed in our study in case 5.
Fuchs et al. [4] reported one case of torsion recurrence 14 months after
suturing of the ovary to the lateral pelvic sidewall with an absorbable suture.
He stated that non-absorbable sutures can be used regardless which technique is
chosen; however, multi-point fixation was not discussed. From the mechanical
perspective, the fixation of
In the prensent study, five patients (50%) had an ovarian mass, similar toprevious reports [9]. All masses were larger than 5 cm and benign (5 teratomas and 3 simple cysts). Oltmann et al. [10] demonstrated a strong association of torsion with pelvic masses larger than 5 cm. The mechanism of torsion in women and girls with benign ovarian masses is likely related to the increased size and weight of the involved ovary [11]. Tsafrir [12] conducted an 11-year retrospective analysis of 216 cases of ovarian torsion and found that performing cyst drainage or cystectomy significantly reduced the chance of retorsion by 50% and 75%, respectively. In case 7 of our series, recurrence was observed two months after cyst aspiration and successfully treated with a second laparoscopy cystectomy, which confirms that removal of the etiology is effective in preventing ovarian torsion recurrence. However, it is often difficult to determine whether there is a discrete cyst, because the ovary is edematous, some authors have suggested delaying cystectomy for 6–8 weeks after edema resolution [13, 14]. Therefore, we think close postoperative monitoring is particularly important. Childress [1] also suggested that surveillance ultrasounds should be performed every three months after surgery and then every 6 months to a year for long-term surveillance.
The study’s limitations include its retrospective design and the small number of AT cases because of its low morbidity. In the future, a multicenter study will be more useful in improving the awareness regarding AT.
The results of the current study indicated that the two main risk factors for AT were ovarian pathology and elongation and hypermobility of the ovarian ligament. Therefore, reductions in pathological indications and performing oophoropexy with non-absorbable sutures and multi-point fixation to restore normal appearance can help prevent retorsion.
JW: project design, data acquisition and analysis, and manuscript writing. PL: project design, data analysis, and manuscript editing. MZ: data acquisition and analysis. SL: data acquisition and analysis. KL: data acquisition and analysis. JF: data acquisition and analysis. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript.
This study was approved by the Ethics Committee of the Fuzhou Children’s Hospital in Fujian Province and was performed in accordance with the principles laid down in the Declaration of Helsinki (FCHFJ-2020-24). Preoperative informed consent was signed in all cases.
The authors are grateful to the staff of Fuzhou Children’s Hospital in Fujian Province, who were responsible for the management of patients included in the study.
Sponsored by the key Clinical Specialty Discipline Construction Program of Fuzhou, Fujian, China (2018-56).
The authors declare no conflict of interest.