


1 Center of Reproductive Medicine, Guangzhou Women and Children’s Medical Center, Guangzhou Medical University, 510623 Guangzhou, Guangdong, China
Abstract
Background: To determine the effects of AMH and age on IVF outcomes in
women with DOR and whether the cumulative pregnancy potential after consecutive
IVF cycles is age or AMH level depended. Methods: Between
January 2014 and December 2018, 466 infertility patients (1004 IVF/ICSI cycles)
with AMH
Keywords
- Age
- Anti-Műllerian hormone
- Diminished ovarian reserve
- IVF
- Ongoing pregnancy rate
A reliable predictor of in vitro fertilization (IVF) outcomes would be useful in order to optimize individualized treatment protocols and assist in counseling patients about their chances of having successful IVF treatment. Therefore, several “ovarian reserve markers” have been investigated for the ability to predict ongoing pregnancy or live birth rates after assisted reproduction treatment (ART). Examples include follicular phase serum follicle-stimulating hormone (FSH), ultrasound assessment of the antral follicle count (AFC) and others [1, 2]. However, maternal age at embryo transfer is still the most accurate established predictor [3, 4].
Recently, anti-Műllerian hormone (AMH) has been proposed as a good predictor of both ovarian reserve and response [5, 6]. AMH has been shown to be a better indicator of a patient’s follicular response to controlled ovarian stimulation (COS) with gonadotropins than the basal levels of FSH, estradiol, inhibin B, or age [7, 8]. However, conflicting results exist regarding the association of AMH with the outcome of pregnancy after IVF treatment. Although some studies have shown that AMH is a good predictor of ovarian response and outcome of pregnancy [9, 10], others found that AMH had poor accuracy for the prediction of embryo quality and ongoing pregnancy [10, 11], suggesting that AMH is a marker of oocyte quantity rather than quality [12]. Pregnancy outcome in IVF cycles is highly associated with oocyte and embryo quality, and many studies described age but not AMH as a good predictor of quality of both oocyte and embryo [13].
Diminished ovarian reserve (DOR) defined by American Society for Reproductive Medicine (ASRM) describes women of reproductive age with regular menses have reduced fecundability and/or poor ovarian response (POR) to gonadotropin stimulation compared with women of similar age [14]. It refers to a decline in reproductive potential largely ascribed to the natural ovarian aging process [15], which is distinct from either menopause or premature ovarian failure [16].
POR is usually identified by a low follicular response to ovarian stimulation,
resulting in reduction of retrieved oocytes during IVF treatment [17]. Consensus
on its definition by the European Society of Human Reproduction and Embryology
(ESHRE) recommended the minimum criteria (Bologna criteria). At least two of the
following three conditions should be met to predict POR: (1) advanced age
(
DOR is used to describe a decreased state of ovarian reserve on the basis of ovarian reserve testing before cycle start, while POR is the poor response according to the result to ovarian stimulation during IVF. They are not interchangeable since there might exists a mismatch between patients with DOR and their ovarian response in IVF cycles.
The most common causes of DOR are different in patients of different ages. For patients of advanced age, DOR seems mostly to be correlated with the natural decline of ovarian function caused by increasing chronological age, and the decrease of oocyte number was accompanied by a significant decline in quality [19, 20]. However, in younger patients, it is most often related to heredity, environment and iatrogenic factors, such as previous pelvic or ovarian surgery [21]. Although the number of follicles was found to be decreased in these situations, the quality of oocytes was not affected. Therefore, young women with low AMH value would be predicted to have favorable IVF outcome due to a well-preserved oocyte competence and comparable good-quality embryos. A few studies have explored various indicators that predict the pregnancy rate in patients with DOR in IVF cycles. Among them, AMH as one of the most commonly ordered tests of ovarian reserve was debated on its prediction power. Ulrich et al. [22], highlighted the limitations of AMH especially for poor responders. However, more data are needed to provide sufficient evidence to suggest the use of AMH for DOR patients.
The aim of this study was to evaluate the role of serum AMH concentration and age in predicting pregnancy outcome in women with diminished ovarian reserve and whether the pregnancy rate after consecutive IVF cycles is age and/or AMH dependent.
This study was declared exempt by the ethics committee of the Guangzhou Women and Children’s Medical Center, China, and written informed consent was obtained from all patients. 466 women undergoing IVF/ICSI treatment during the period from January 2014 to December 2018 were enrolled in the study. All women had serum AMH taken on day 2–5 of their menstrual cycle.
The inclusion criteria were as follows: patient aged 20–45 years, AMH
Patients were first divided into two groups (Group 1: AMH
Measure of AMH levels on the day 2–5 of menstrual cycle was carried out in the endocrinology lab of our hospital using the AMH/MIS commercially enzyme-linked immunosorbent assay kit (Kangrun Biotech, Guangzhou, China) following the manufacturer’s instructions. The lowest and highest detection level of this assays was 0.06 ng/mL and 16.0 ng/mL, respectively. The intra- and inter-assay coefficients of variation were 10% and 15%, respectively.
The stimulation protocol was a GnRH-antagonist protocol, the starting
gonadotropin dosage was dependent on the patients’ age, weight and BMI, and
adjusted according to ovarian response. A single injection of 250 mg of human
chorionic gonadotropin (hCG, choriogonadotropin alpha, Merck Serono) was
administered when two follicles of 18 mm were observed. Oocyte retrieval took
place about 36 hours after the hCG administration. Fertilization was assessed 19
A serum beta-hCG test was performed 14 days after transfer. Clinical and ongoing pregnancy was confirmed by transvaginal ultrasound at 5 to 6 weeks after transfer. A patient with no ongoing pregnancy at the end of the stimulated cycle period and with surplus cryopreserved embryos could undergo cryopreserved replacement cycles within 1 year of the patient’s start of treatment. The main outcome was ongoing pregnancy rate arising from all fresh and subsequent frozen embryo transfers within 1 year.
Statistical analysis was performed with the assistance of SPSS software
(Chicago, IL, USA) version 19 for Windows, applying parametric and nonparametric
tests when appropriate. Continuous variables were expressed as absolute numbers,
mean
Table 1 summarizes patient demographic characteristics for the four different
AMH groups. 209 patients in Group 1 undergoing 520 cycles had extremely low AMH
levels (
| Group 1 | Group 2 | P | ||
| (AMH |
(AMH 0.6–1.1 ng/mL) | |||
| No. of patients | 209 | 257 | ||
| OPU cycles | 520 | 484 | ||
| AFC | 3.2 |
4.7 |
||
| Baseline FSH (mIU/mL) | 10.2 |
7.9 |
||
| Age group (years; n, %) | ||||
| 21–25 | 1 (0.5) | 6 (2.3) | 0.209 | |
| 26–30 | 14 (7.2) | 30 (11.7) | 0.068 | |
| 31–35 | 37 (17.7) | 67 (26.1) | 0.031 | |
| 36–40 | 71 (34.0) | 87 (33.9) | 0.978 | |
| 41–45 | 76 (36.4) | 61 (23.7) | 0.003 | |
| 46–50 | 10 (4.8) | 6 (2.3) | 0.149 | |
| Mean |
38.7 |
36.7 |
0.452 | |
| Median | 40 | 37 | ||
| Type of fertility disorder (n, %) | ||||
| Primary | 56 (26.8) | 84 (32.7) | 0.168 | |
| Secondary | 153 (73.2) | 173 (67.3) | 0.168 | |
| Etiology (n, %) | ||||
| Male factors | 12 (5.7) | 25 (9.7) | 0.113 | |
| Tubal factors | 98 (46.9) | 144 (56.0) | 0.049 | |
| Menstrual factors | 80 (38.3) | 65 (25.3) | 0.003 | |
| Endometriosis | 16 (7.7) | 22 (8.6) | 0.723 | |
| Unexplained | 3 (1.4) | 1 (0.4) | 0.476 | |
Comparisons of cycle parameters between Group 1 and Group 2 are shown in Table 2.
Number of retrieved oocytes, 2 pronuclear zygotes (2PN), embryos and good-quality
embryos per cycle were significantly lower in Group 1 than those in Group 2 (all
P
| Group 1 | Group 2 | P | |
| (AMH |
(AMH 0.6–1.1 ng/mL) | ||
| OPU cycles | 520 | 484 | |
| Fresh embryo transfer cycles (n, %) | 52 (22) | 105 (30) | 0.021 |
| Cancelled transfer cycles rate | 468/520 (90.0%) | 379/484 (78.3%) | |
| Frozen embryo transfer cycles (n, %) | 184 (78) | 237 (69) | 0.021 |
| Oocytes retrieved per cycle | 2.2 |
4.0 |
|
| 2PN per cycle | 1.4 |
2.7 |
|
| Embryos per cycle | 1.2 |
2.3 |
|
| Good-quality embryos per cycle | 0.5 |
0.9 |
|
| Implantation rate | 68/408 (16.7%) | 160/624 (25.6%) | |
| Clinical pregnancy rate per ET | 56/236 (27.0%) | 127/342 (37.1%) | |
| Ongoing pregnancy rate per ET | 43/236 (18.2%) | 107/342 (31.3%) | |
| Miscarriage rate | 13/56 (23.2%) | 20/342 (5.8%) | 0.226 |
| Clinical pregnancy rate per patient | 56/165 (33.9%) | 127/229 (55.5%) | |
| Ongoing pregnancy rate per patient | 43/165 (26.1%) | 107/229 (46.7%) |
Patients were then stratified into four subgroups depending on age (
| Group A (Age |
Group B (Age | |||||
| A1 | A2 | P | B1 | B2 | P | |
| (AMH |
(AMH 0.6–1.1 ng/mL) | (AMH |
(AMH 0.6–1.1 ng/mL) | |||
| Patients | 77 | 136 | 132 | 121 | ||
| OPU cycles | 169 | 230 | 351 | 254 | ||
| Age (years) | 33.2 |
32.6 |
0.146 | 42.0 |
41.3 |
0.93 |
| AFC | 3.7 |
5.4 |
0.04 | 2.9 |
4.0 |
0.016 |
| bFSH (mIU/mL) | 10.5 |
7.9 |
0.08 | 10.0 |
7.9 |
0.002 |
| bLH (mIU/mL) | 3.9 |
3.1 |
0.03 | 3.7 |
3.5 |
0.07 |
| bE2 (pmol/L) | 155.7 |
164.0 |
0.526 | 171.6 |
167.6 |
0.205 |
| No oocyte (n, %) | 5 (6.5) | 1 (0.7) | 0.05 | 10 (7.6) | 6 (5.0) | 0.393 |
| No 2PN (n, %) | 4 (5.2) | 5 (3.7) | 0.597 | 6 (4.6) | 7 (5.8) | 0.655 |
| No embryo (n, %) | 9 (11.7) | 5 (3.7) | 0.05 | 10 (7.6) | 4 (3.3) | 0.227 |
| Fresh embryo transfer cycles (n, %) | 21 (23.9) | 67 (35.3) | 0.057 | 31 (21.0) | 38 (25) | 0.404 |
| Frozen embryo transfer cycles (n, %) | 67 (76.1) | 123 (64.7) | 0.057 | 117 (79.1) | 114 (75) | 0.404 |
Analysis of pregnancy rates in patients within age-stratified groups is shown in
Table 4. Among women under or above 38 years of age, number of retrieved oocytes,
2PN, embryos per cycle were significantly lower in the extremely low AMH (
| Group A (Age |
Group B (Age | |||||
| A1 | A2 | P | B1 | B2 | P | |
| (AMH |
(AMH 0.6–1.1 ng/mL) | (AMH |
(AMH 0.6–1.1 ng/mL) | |||
| Oocytes retrieved per cycle | 2.8 |
4.7 |
0.009 | 1.9 |
3.2 |
|
| 2PN per cycle | 1.9 |
3.2 |
0.008 | 1.2 |
2.1 |
|
| Embryos per cycle | 1.5 |
2.7 |
0.032 | 1.0 |
1.9 |
|
| Good-quality embryos per cycle | 0.7 |
1.0 |
0.178 | 0.4 |
0.7 |
|
| Cancelled transfer cycles rate | 148/169 (87.6%) | 163/230 (70.9%) | 320/351 (91.2%) | 216/254 (85%) | 0.019 | |
| Implantation rate | 45/163 (27.6%) | 113/360 (31.4%) | 0.383 | 23/245 (9.4%) | 47/264 (17.8%) | 0.006 |
| Clinical pregnancy rate per ET | 36/88 (40.9%) | 88/190 (46.3%) | 0.399 | 20/148 (13.5%) | 39/152 (25.7%) | 0.008 |
| Ongoing pregnancy rate per ET | 31/88 (35.2%) | 77/190 (40.5%) | 0.399 | 12/148 (8.1%) | 30/152 (19.7%) | 0.004 |
| Miscarriage rate | 5/36 (13.9%) | 11/88 (12.5%) | 0.834 | 8/20 (40%) | 9/39 (23.1%) | 0.174 |
| Without embryos transferred rate per patient | 18/77 (23.4%) | 11/136 (8.1%) | 0.002 | 26/132 (19.7%) | 17/121 (14.0%) | 0.232 |
| Clinical pregnancy rate per patient | 36/59 (61%) | 88/125 (70.4%) | 0.205 | 20/106 (18.9%) | 39/104 (37.5%) | 0.003 |
| Ongoing pregnancy rate per patient | 31/59 (52.5%) | 77/125 (61.6%) | 0.244 | 12/106 (11.3%) | 30/104 (28.8%) | 0.002 |
Fig. 1A presents the trend of COPR observed following more than five oocyte pick-up (OPU) and Fig. 1B shows the COPR in different transfer cycles.
Fig. 1 shows the trend of COPR observed following more than five oocyte pick-up
(OPU) and four ET cycles. Analysis revealed that COPR per patient increased along
with consecutive treatments respectively in the four subgroups, especially in
Group A2 (young women
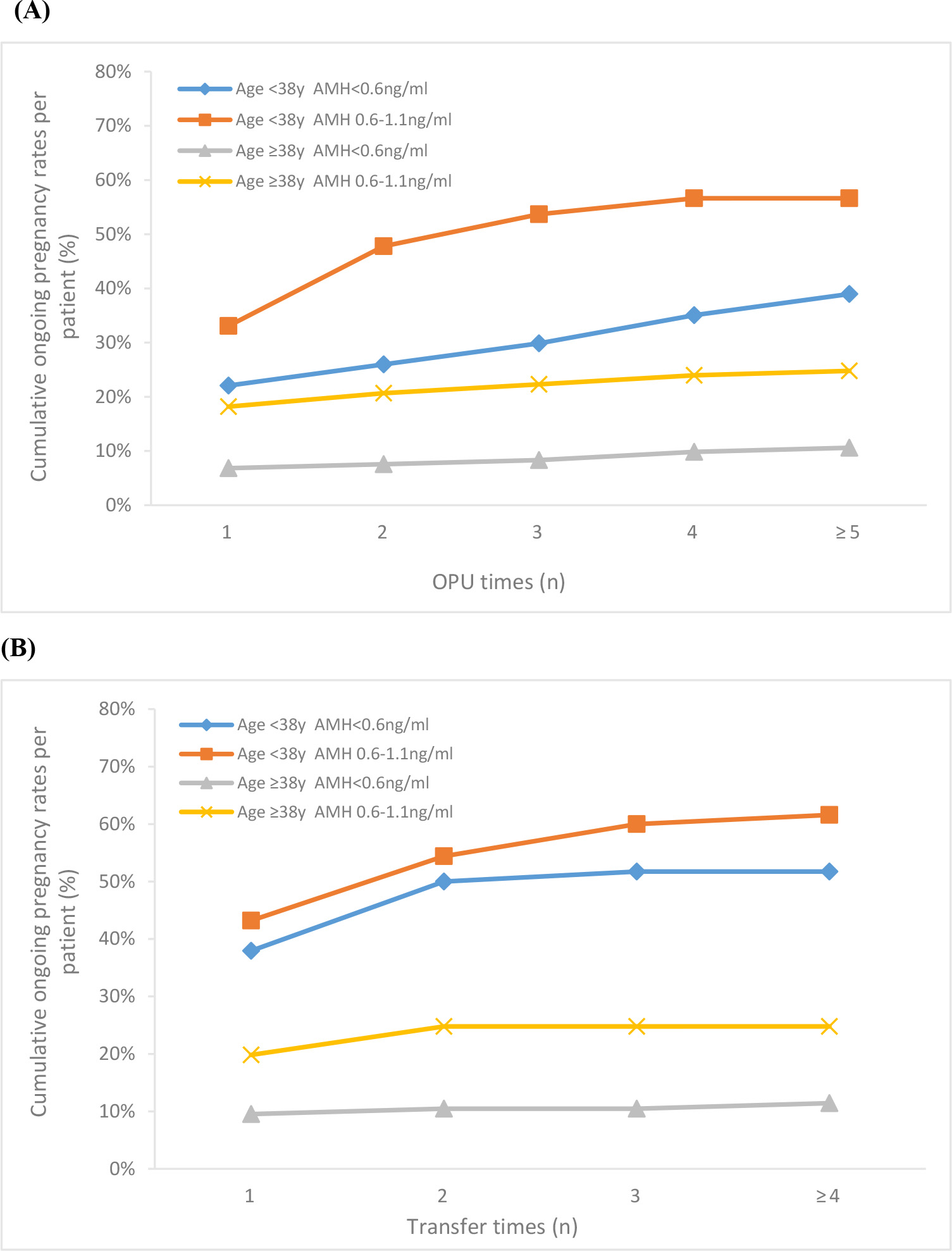 Fig. 1.
Fig. 1.Cumulative ongoing pregnancy rates per patient following
consecutive OPU (A) and ET cycles (B) for women with AMH
Our goal was to investigate the ability of AMH and age to predict IVF pregnancy
rates in women with poor ovarian reserve. However, the cut-off values of AMH for
predicting poor ovarian response (POR) varied differently from 0.1 to 2.97 ng/mL
[24]. According to the Bologna criteria of POR (AMH
Regardless of age, number of retrieved oocytes, 2PN, embryos, good-quality
embryos per cycle, IR, CPR and OPR per ET and per patient were significantly
lower in patients with AMH
Analysis of the 4 subgroups revealed several interesting trends. First, in women
older than 38, not only the ovarian response but also IVF outcomes were
significantly lower in patients with AMH
It was worth noting that the cancelled transfer cycle rate were high in all 4
subgroups, especially in patients with lower AMH. Daney de Marcillac found that
women with a decreased AMH level had a higher cancellation rate [30]. One reason
for that was no embryo or no good quality embryo formed during IVF. Lower AMH
levels in various studies have been found to be associated with poor embryo
quality [14]. Although the percentage of patients without embryos transferred was
significantly higher in patients
The main causes of AMH decrease were heterogeneous in patients of different ages. For patients in advanced age, the decrease of AMH level was mostly correlated with the natural decline of ovarian function caused by increasing chronological age, and the decrease of oocytes number was accompanied by a significant decline in quality [19, 20]. Female fecundity largely decreases in women of advanced reproductive age primarily as a result of high rate of oocyte abnormalities in chromosome alignment and microtubular matrix composition [31] as well as embryo aneuploidy [32]. However, in young patients, it was often related to heredity, environment and iatrogenic factors, such as previous pelvic ovarian surgery [21]. Although the number of follicles decreased, the quality of oocytes was not affected. Therefore, young women with low AMH value had favorable IVF outcome due to a well-preserved oocyte competence and comparable good-quality embryos.
Recent study found that poor ovarian reserve in young patients does not mean
poor IVF outcomes [33]. Study on 202 infertile women younger than 35 found the
time to pregnancy was significantly longer in the very low AMH group than in the
normal AMH group [34]. Our study also suggested that young patients, even with
extremely low AMH, were still likely to benefit from more IVF cycles. COPR in
patients under 38 increased by more than 50% after multiple oocyte retrieval
cycles reaching 57%. Similarly, Steiner et al. [35] concluded that women
with AMH
The main limitation of this historical cohort study is the relatively lower sample size in Group A1 which may limit the statistical power. Furthermore, we did not concern canceled cycles per cycle start and previous cycle attempts in other clinics, which could affect the evaluation of time to get pregnancy.
Combination of AMH and age was more reliable in the prediction of IVF outcomes in women with diminished ovarian reserve than AMH alone. For women over 38 years old, AMH and age are both useful in predicting the success of IVF treatment, whereas AMH does not appear to have much predictive utility in women under 38 years old. This should be considered when counseling women and their partners about clinical pregnancy outcomes.
LS: conception and design of the study. YD: data collection, statistical analysis, construction of Figure and Tables. PLL: follow-up of enrolled subjects. MNY, ZHC: interpretation of data. YD, ZHO drafted the article, and AM, LS revised it critically. All authors reviewed the manuscript and approved the version to be published.
This study was declared exempt by the ethics committee of the Guangzhou Women and Children’s Medical Center, China, and written informed consent was obtained from all patients.
Thanks to all the peer reviewers for their opinions and suggestions.
This study was supported by institutional funding of Youth medicine research and development program for Reproductive Medicine from Chinese Medical Association (17020150684), Health Science and technology project of Guangzhou (20211A011026 and 20201A011029).
The authors declare no conflict of interest.