




1 Department of Obstetrics and Gynecology, Second University Hospital, Sichuan University, 610041 Chengdu, Sichuan, China
2 Key Laboratory of Birth Defects and Related Diseases of Women and Children, Sichuan University, Ministry of Education, 610041 Chengdu, Sichuan, China
3 Department of Obstetrics and Gynecology, West China Guang-an Hospital, Sichuan University, 638001 Guangan, Sichuan, China
† These authors contributed equally.
Abstract
Background: This study aims to
compare the effect of tamoxifen (TMX) vs. other regimens on endometrial thickness
(EMT), clinical pregnancy, implantation, miscarriage, and live birth rates in
women with thin endometrium undergoing frozen-thawed embryo transfer (FET).
Methods: We searched the Cochrane Central Register of Controlled Trials,
MEDLINE, EMBASE, and CINAHL from inception to November 2020 and cross-checked the
references of relevant articles. We included randomized controlled trials (RCTs)
and nonrandomized controlled trials (non-RCTs) to compare TMX with other regimens
for endometrium preparation in women with thin endometrium undergoing FET. We
pooled weighted mean differences (WMD) with 95% confidence intervals (CI) for
continuous variables (EMT) and odds ratios (OR) with 95% CI for binary variables
(i.e., clinical pregnancy rate, implantation rate, and first trimester
miscarriage rate). Results: An RCT and three controlled trials (2
before-after and 1 retrospective controlled trials) were included in the final
review. One study including 154 women and comparing TMX-FET with natural cycle
(NC)—FET showed a significant increase in EMT in the TMX cycle (7.87
Keywords
- Tamoxifen
- Thin endometrium
- Frozen embryo transfer
- Meta-analysis
The cryopreservation of embryos and frozen-thawed embryo transfer (FET), an
important part of assisted reproductive technique that enables surplus embryos
derived from “fresh” cycles to be stored and transferred at a later date, are
already widely adopted in clinical practice due to its perceived benefits,
including increasing the cumulative pregnancy rate, reducing the risk of
potentially serious complications (such as ovarian hyperstimulation syndrome) [1, 2]. Successful embryo implantation and pregnancy depend on the transfer of a
vital embryo into a molecularly receptive endometrium [3, 4, 5]. The endometrial
thickness (EMT) is one of the sonographic parameters developed in the
identification of endometrial receptivity, and the EMT assessment has become part
of standard monitoring during fertility treatment. Increased EMT is associated
with improved pregnancy rates in FET cycles [6]. A thin endometrium, which is
mostly defined as an EMT
Several strategies are developed for endometrium preparation in FET cycles, i.e., natural (NC) and ovulation induction (OI) cycles, in which ovulation is induced by letrozole or gonadotropins and hormone replacement treatment (HRT). During this treatment, the endometrium is artificially prepared by estrogen and progesterone with or without a gonadotropin-releasing hormone agonist. The systematic review does not conclude which method of endometrium preparation is the optimal [12]. For patients with thin endometrium or unresponsive to standard treatment, various therapies (such as extended estrogen administration, low-dose aspirin, high-dose vitamin E, human chorionic gonadotropins, L-arginine, vaginal sildenafil citrate, and intrauterine perfusion of granulocyte colony-stimulating factor or autologous platelet-rich plasma) have been tried [13, 14, 15, 16, 17, 18, 19]. However, some patients with a thin endometrium remain unresponsive after receiving all these therapies.
TMX, which is primarily developed for use in the treatment of breast cancer, is a selective estrogen receptor modulator that occupies estradiol-binding sites on the hypothalamic–pituitary axis and prevents the negative feedback effect of estradiol, resulting in increased endogenous gonadotropin secretion. Studies have observed that TMX significantly improves EMT compared with clomiphene citrate (CC) in anovulatory women with polycystic ovarian syndrome [20, 21, 22]. Studies also show that TMX is a promising alternative to CC for patients with thin endometrium in intrauterine insemination cycles [23, 24]. Recently, studies report the use of TMX in endometrium preparation in patients undergoing FET. However, the efficacy of TMX in endometrium preparation for infertile women with thin endometrium prior to FET is not clear. This study aims to determine whether the outcome for FET in a TMX cycle preparing the endometrium is different to that in NC, HRT, or OI cycle by using letrozole or gonadotropins through a systematic review and meta-analysis of data published in recent years.
We searched for all published clinical trials studying the impact of TMX versus other drug regimens on EMT in women with thin endometrium undergoing FET cycles. We searched the following electronic databases: the Cochrane Central Register of Controlled Trials (CENTRAL), MEDLINE (1948 to 31 November 2020) EMBASE (1989 to 14 November 2020), CINAHL (Cumulative Index to Nursing and Allied Health Literature, 1980 to 30 November 2020). In addition, we searched the following sources: China Academic Journal Electronic Publishing House (http://www.cnki.net); ClinicalTrials.gov, a service of the US National Institutes of Health (http://ClinicalTrials.gov/ct2/home); The World Health Organization International Clinical Trials Registry Platform search portal (www.who.int/trialsearch/Default.aspx); Open Sigle for grey literature from Europe (http://www.opengrey.eu/); National and international research registers including the Register of Controlled Trials (http://www.isrctn.com/). We also searched the reference lists of relevant studies, citation lists of relevant publications, abstract of major scientific meetings: American Society for Reproductive Medicine (ASRM) and European Society of Human Reproduction and Embryology (ESHRE). There were no limitations to the type or languages of the publication in these searches. The protocol of this review was registered in the International Prospective Register of Systematic Reviews (PROSPERO; CRD42020120885).
Two reviewers (ZX and YB) independently performed the searches and checked the titles and abstracts of every record retrieved. The reviewers investigated and read all potentially relevant articles as full texts for final inclusion. Discrepancies between the two reviewers were resolved by discussion with a third reviewer (ZH).
We included RCTs and non-RCTs comparing TMX with other regimens for endometrium preparation in women undergoing the FET cycle. The included comparative regimens could be aromatase inhibitors, gonadotropins, artificial cycle with estrogen and progesterone, or any other regimen. The outcomes of our review were EMT, clinical pregnancy rate per woman defined by ultrasonographic visualization of one or more gestational sacs, implantation rate, and the first-trimester miscarriage rate. Four articles were included in this review (Fig. 1).
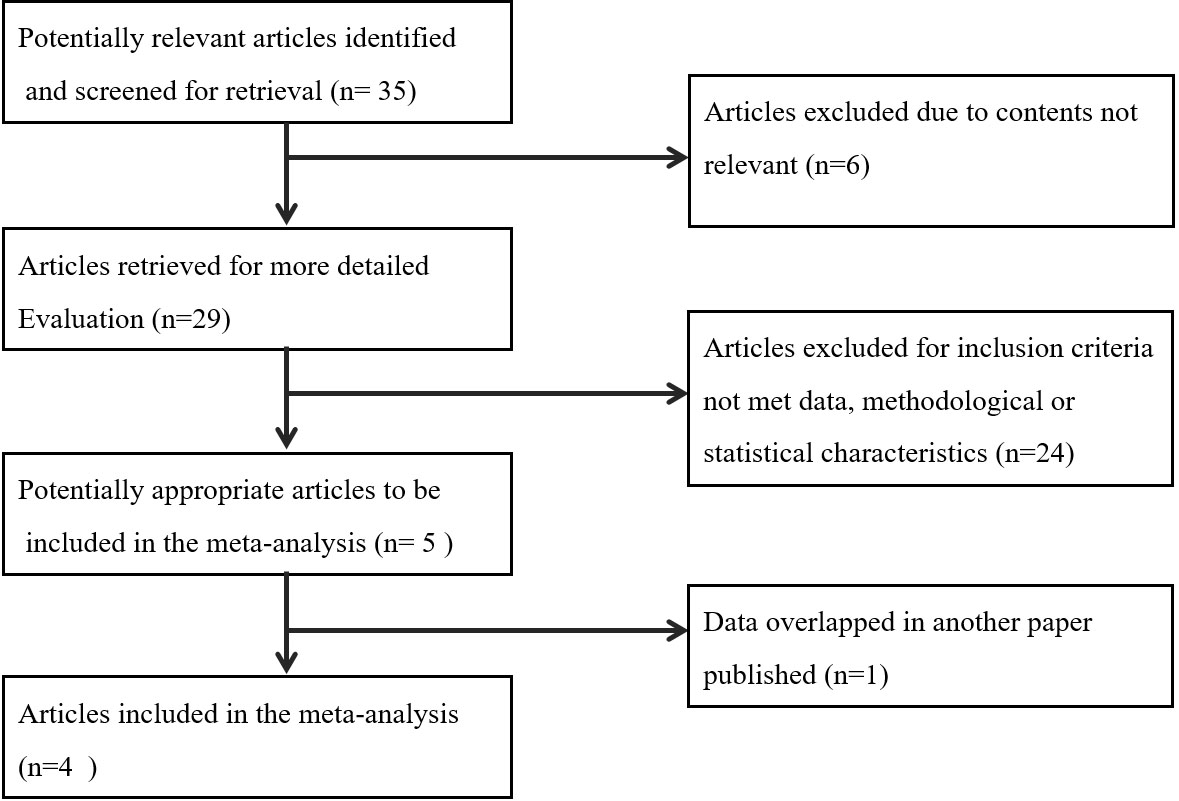 Fig. 1.
Fig. 1.Flowchart for inclusion of studies on efficacy of tamoxifen for women with thin endometrium undergoing FET for systematic review and meta-analysis.
The meta-analysis was conducted using the RevMan5.3 software (Cochrane
Collaboration, Oxford, UK). We used the I
A summary of the characteristics of these studies is shown in Table 1 (Ref. [26, 27, 28, 29]).
| Study | Design | Population | Intervention | Comparison | Outcomes |
| Ke H et al. 2018 [26] | Before-after controlled trial | 199 women with thin EMT in previous HRT cycle | 199 cycles of TMX 20 mg/day for 5 days on day 3–7 | 199 cycles of HRT for endometrium preparation | EMT |
| Sun Q et al. 2017 [27] | RCT | 133 women with thin EMT in previous NC or HRT-FET cycle | 61 women treated with TMX 40 mg/day for 5 days on day 3–7 | 72 women treated with LE 2.5 mg/day from Day 3–7 | EMT, CPR, IR, MR |
| Tian X et al. 2015 [28] | Before- after controlled trail | 61 women with thin EMT in previous HRT-FET cycle | 61 cycles of TMX 20–40 mg/d for 5 days since day 3–5 | 61 cycles of HRT for endometrium preparation | EMT |
| Liu J et al. 2018 [29] | Retrospective controlled trial | 304 women with thin EMT in previous HRT cycle | 149 women TMX 20 mg/d for 5 days on day 3–7 | 155 women treated with hMG 75 U/day from day 3 | EMT, CPR, IR, MR |
| Abbreviations: RCT, randomized controlled trial; EMT, endometrial thickness; HRT, hormone replacement treatment; NC, natural cycle; OI, ovulation induction; TMX, tamoxifen; LE, letrozole; CPR, clinical pregnancy rate; IR, implantation rate; MR, miscarriage rate. | |||||
Only one study [26] was identified comparing TMX-FET with NC-FET, and
meta-analysis was not applied. Based on the reported outcomes, this comparison
was only possible for the EMT. NC was recommended for patients with regular
menstruation and normal ovulation. A total of 154 women with NC diagnosed with
thin endometrium (EMT
One retrospective controlled study [29] compared the effect of TMX with that of
HRT for endometrium preparation in women with thin endometrium. A total of 149
and 123 women were treated with TMX and HRT, respectively. Basal clinical
characteristics, such as age, infertile duration, and the percentage of infertile
factor, were comparable in both groups. In the TMX group, 251 embryos were
transferred into 149 women, of which 69 got clinically pregnant, and 8
experienced miscarriage. In the HRT group, 213 embryos were transferred into 123
women, of which 55 got pregnant, and 9 experienced miscarriage. Analyses showed
no significant difference in clinical pregnancy, implantation rate, and
miscarriage rate. The EMT in the TMX group (8.2
Three studies compared the EMTs in the TMX cycle and the previous HRT cycle
[26, 27, 28]. The pooled analysis showed the beneficial effect of TMX on the EMT (WMD
= 2.06, 95% CI = 1.86–2.27, P
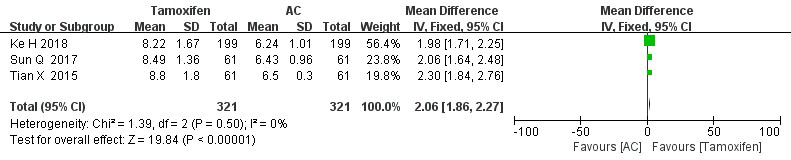 Fig. 2.
Fig. 2.Endometrium thickness in FET cycles, TMX versus HRT: pooled result of all studies.
Clinical pregnancy rate, implantation rate and miscarriage rate were available in only one study [27], which compared TMX–FET with HRT–FET, and meta-analysis was not applied.
One prospective randomized [27] and one retrospective [29] controlled studies
compared TMX and OI with medicines other than TMX for endometrium preparation in
women with thin endometrium undergoing FET. No significant difference in EMT was
found between TMX and OI groups with Letrozole/hMG in the included studies. Given
that considerable heterogeneity was detected (I
In one before–after control study [26], 161 women with thin endometrium in
previous hMG cycles were treated with TMX in the following cycle, and the EMT was
significantly improved with the TMX administration (6.34
No significant difference in clinical pregnancy (OR = 1.03, 95% CI = 0.71–1.51), implantation (OR = 1.03, 95% CI = 0.76–1.38), and miscarriage (OR = 0.91, 95% CI = 0.40–2.06) rates were observed (Fig. 3B–C).
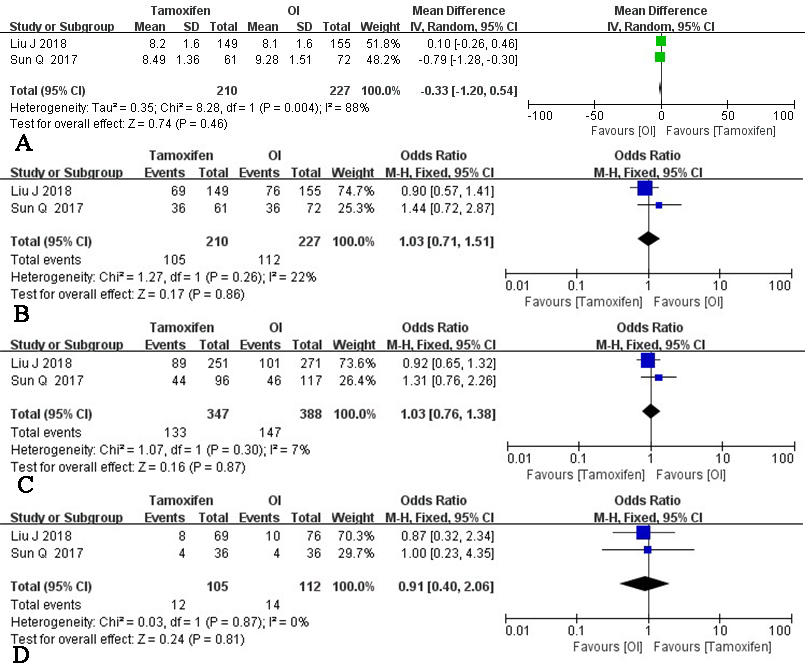 Fig. 3.
Fig. 3.TMX versus OI: pooled result of all included studies. (A) Endometrium thickness. (B) Clinical pregnancy rate. (C) Implantation rate; (D) Miscarriage rate.
The EMT is one of the most important factors affecting the pregnancy outcome of
FET [30, 31]. In medicated FET cycles, an EMT of 9–14 mm measured on the day of
progesterone supplementation is associated with higher implantation and pregnancy
rates compared with an EMT of 7–8 mm [6]. Clinical pregnancy and live birth rate
are significantly lower in women with EMT
Recently, TMX is reported in the endometrium preparation in women with thin endometrium undergoing FET [26, 27, 28, 29, 35]. However, whether TMX has benefit in improving FET outcomes for these women remains unclear. Therefore, a meta-analysis is expected to provide us with reliable and comprehensive results.
This study includes 1 RCT and 3 non-RCTs. One controlled trial has compared TMX
with NC in women with thin endometrium undergoing FET by studying 154 women [26].
These women have thin endometrium (
One retrospective controlled study [29] has compared 149 and 123 women undergoing TMX treatment and HRT, respectively, for endometrium preparation. No significant difference in CPR and IR is observed. The TMX-treated group appears to have lower miscarriage rate than the HRT-treated group, but no statistical significance is observed. The EMT is significantly higher in the TMX group. Three studies [26, 27, 28] have included 321 women with thin endometrium who used HRT, failed to receive embryo transfer due to thin EMT, and switched to TMX for endometrium preparation in the following cycle. The meta-analysis shows significantly improved EMT following the use of TMX.
A randomized controlled study [27] and a retrospective controlled study [29] comparing the TMX cycle with OI cycle (with hMG in Liu’s study, and letrozole/hMG in Sun’s study) in women with thin endometrium for endometrium preparation are identified for meta-analysis. No significant difference is observed in CPR, IR, and miscarriage rate between TMX and OI groups. The pooled data for CPR and miscarriage rate analyses coincide with the results of the two included studies [27, 29]. The results of one RCT [27] show significantly higher implantation rates in the TMX cycle groups, whereas the pooled data does not show the difference in IR between the TMX and OI groups.
No significant difference in EMT is found in TMX and OI treatments on the pooled data from these two studies [27, 29]. Considering that the included two studies have substantial between-study heterogeneity, we are cautious to conclude the role of TMX on EMT versus OI by using letrozol/hMG from this meta-analysis. In Ke’s study [26], 161 women have experienced at least two cycles of ineffective endometrial preparation with HRT by using estrogen and OI with hMG. The TMX administration based on about one-third of the routine dosage of estrogen and hMG results in remarkably improved EMT, suggesting the unique role of TMX in the growth of endometrial growth.
In this study, the included RCT provides information on how randomization is achieved and gives clear methods of allocation concealment. Blinding is not described in the trials, but blinding is not likely to cause performance or detection bias in this review. The other three included controlled trials provide low-quality evidence. All included trials have an unclear risk of reporting bias for the major outcome because live birth is not reported. This finding demonstrates the need for researchers to extend follow-up period to report this outcome measure. Given the limited number and the small size of available RCTs, conclusions from this review remain tentative. Therefore, sufficiently powered RCTs should be designed and performed to assess the therapeutic effect of TMX on thin endometrium cases for FET. To the best of our knowledge, this study is the first meta-analysis, which investigates whether TMX does any good for patients with thin endometrium undergoing FET. In conclusion, the TMX may play a beneficial role in improving EMT for women with thin endometrium, but its role on CPR, IR, or miscarriage rate in FET cycles are unclear because insufficient data on these cases can be retrieved.
ZYH, ZX and YB reviewed all articles. In the case of conflicting opinions as to whether a study should be included, QHM and FLL resolved the issue. ZYH and ZX performed data extraction, all statistics, and drafted the article. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript.
Not applicable.
The authors thanks all those who provided help during the writing of this manuscript. The authors also gratefully acknowledge all the peer reviewers.
This research was funded by the National Natural Science Foundation of China, grant number 81200453.
The authors declare no conflict of interest.