


1 Gynecology and Obstetrics Department, General University of Catalunya, Sant Cugat del Vallès, 08195 Barcelona, Spain
2 Gynecology and Obstetrics Department, Miguel Servet University Hospital, 50009 Zaragoza, Spain
3 Gynecology and Obstetrics Department, Granada University, 1816 Granada, Spain
Abstract
Background: The signs and symptoms of the genitourinary syndrome of
menopause are well established, and there is extensive knowledge with high
scientific evidence about the response that vaginal and urinary tissues present
to various treatments. However, this does not usually apply to the vulva in
general, or any of its structures in particular, since it is included in the term
vulvovaginal. The aim of this review is to improve knowledge about the vulva and
to improve symptoms in women who experience vulvar pain associated with atrophy.
Methods: The study was registered at PROSPERO (registration number
CRD42020172102). We also assessed the quality of evidence for each outcome of
interest according to the GRADE criteria. Results: We systematically
reviewed eight studies: four with ospemifene, a pilot study with prasterone, a
study using a combination of estrogens and androgens, another study that used
CO
Keywords
- Vulvar atrophy
- Vulvar pain
- Sexual health
- Genitourinary syndrome of menopause
Estrogen and androgen deficiencies are considered to be the main pathophysiological mechanisms underlying the genitourinary syndrome of menopause (GSM). The signs and symptoms of the genitourinary syndrome of menopause are well established, and there is extensive knowledge with high scientific evidence about the response that vaginal and urinary tissues present to various treatments. However, this does not usually apply to the vulva in general, or any of its structures in particular, since it is included in the term vulvovaginal [1, 2].
In fact, recently there has been a growing awareness of the importance of the pathology of the vulva, particularly with regard to vulvar pain due to atrophy (hereafter VPA), due to the psychological and sexual repercussions for the affected women [3]. In this regard, it is thus necessary to increase existing anatomical knowledge of the vulva. One of the more important points is to know the distribution of estrogen and androgen receptors. Studies on the labia majora have shown that androgen receptors seem to be particularly abundant in epidermal keratinocytes and in dermal fibroblasts. Androgen receptors are also abundant in the epidermis, especially in the keratinocytes, and in the dermis of the labia minora and vestibule, where they are more numerous than in the vagina [4].
All of this will help us to establish a more specific diagnosis and the most effective treatments for the vulva. Although there are other causes of vulvar pain, in this review we refer to that caused by atrophy [5, 6].
The objective of this systematic review is to analyze the therapeutic options to improve quality of life of women with VPA. We must make an adequate diagnosis, rule out other pathologies that can also lead to persistent vulvar pain such as vulvodynia and, specifically, suspect those women who do not respond to conventional treatment with local or systemic estrogens.
The study was registered at PROSPERO (registration number CRD42020172102).
We searched the Scientific Information Web of Knowledge (MEDLINE, Pubmed, Scopus, and Cochrane databases) for all articles (in any language) published in peer-reviewed journals up to December 2020 using the search strategy described in Supplemental Material 1. The search criteria were applied to each database and combined with the available database-specific filters. Other publications were identified by manually searching through a reference list of papers highlighted by the search, as well as key reviews. Press reports published in peer-reviewed journals and reports available online prior to publication were also considered.
The PICOS (Population, Intervention exposure, Comparators, Outcomes, Study Design) criteria were developed a priori to guide the scope of the review, along with the procedures, selection, and synthesis of the literature search. The selection criteria were as follows: (Population) perimenopausal or postmenopausal women affected by vulvar pain due to atrophy (Interventions) any type of vulvar treatments; (Comparators) placebo or no treatment; (Outcome) primary outcomes: efficacy for treating vulvar pain; (Study Design) clinical studies. Any complete article that met the inclusion criteria was reviewed in detail. Other related papers are for reference purposes only.
We have also reviewed the grey literature, like Spanish guides [7].
To select only the relevant studies, we examined both the titles and abstracts of all citations identified by the literature search. We included all studies that investigated the specific theme of vulvar pain or vulvar symptoms due to atrophy. Duplicate studies, surveys that include perimenopausal women, or those with vulvar pain not caused by atrophy were excluded.
We synthesized the evidence according to PRISMA guidelines [8].
The primary outcome was the efficacy for treating vulvar pain. The secondary outcome was the security of each treatment.
NM, LB and SS designed the research study. SS extracted the relevant data on the main characteristics of the eligible studies to obtain a summary, which were narratively described and compared for analysis. LB and NM made a cross-checked data to ensure accuracy. SS analyzed the data.
We assessed the risk of bias of the eligible studies using the Cochrane tool for clinical trials, which takes into account the evaluation of five possible sources of bias (selection, performance, detection, attrition and report bias) [9]. For observational studies, we adapted the ROBINS I tool, focusing on the evaluation of the impact of the confounding variables, selection bias, outcome measures, and attrition [10].
We described the synthesis of the evidence following the PRISMA guidelines. We developed a narrative synthesis of the findings and effect estimates from the included studies focusing on the outcomes of interest, to explore the association between the treatment and the outcomes of interest.
We made explicit judgements on the certainty of the evidence for each outcome of interest according to GRADE criteria [11]. Quality will be classified as high, moderate, low or very low, based on several factors (including risk of bias, inaccuracy, inconsistency, lack of directionality and publication bias).
This is the first systematic review to evaluate the effectiveness of treatments for vulvar atrophy and VPA by analyzing these separately from treatments for vaginal atrophy and vulvodynia caused by conditions other than atrophy. Our review has identified seven publications involving 779 postmenopausal women with vulvar pain due to atrophy. All the therapeutic strategies used have been effective in treating vulvar atrophy and/or VPA.
Tables 1 (Ref. [12, 13, 14, 15, 16, 17, 18]), 2 (Ref. [12, 13, 14, 15, 16, 17, 18]), 3 (Ref. [12, 13, 14, 15, 16, 17, 18]) display a summary of the main characteristics of the selected studies (study design, population, intervention, objective and main results).
| Authors | Study design | Population | Intervention | Objective | Main results |
| Goldstein et al., 2019 [12] | RCT (NCT02638337) | 631 postmenopausal women with moderate-severe VVA. | Ospemifene 60 mg daily, 12 weeks (n = 313) 2º objective n = 154 | Primary: efficacy on bothersome symptom | Improvements in vulvoscopy images and symptomatology |
| 59.7 |
Placebo (n = 314) 2º | Secondary: changes in | |||
| 59.8 |
objective n = 150 | vulvar-vestibular images | |||
| Alvisi et al., 2018 [13] | Prospective cohort study | 20 postmenopausal women undergoing elective vaginal surgery | Ospemifene 60 mg daily, weeks (n = 11) | Primary: changes induced on epithelial thickness, glycogen content proliferation index, collagen content, and type I/III collagen ratio in vulvar and vaginal tissue | Improvement of various morphological and physiological features of both vaginal and vulvar vestibule epithelium |
| Control group with no treatment (n = 9) | |||||
| Murina et al., 2018 [14] | Prospective cohort study | 55 Postmenopausal women with moderate-severe VVA | Ospemifene 60 mg daily, 60 days | Primary: vulvar vestibule effect | Efficacy in dryness, burning, dyspareunia and vestibular trophic score |
| Secondary: sensitivity of vestibular nerve fibers | Efficacy in current perception threshold testing obtained from the vulvar vestibule | ||||
| Goldstein et al., 2018 [15] | Prospective cohort study | 8 Postmenopausal women with Dyspareunia (vulvodynia) | Ospemifene 60 mg daily, 20 weeks | Primary: vulvoscopic changes | Improvements in vulvoscopy images and pain |
| Secondary: pain changes | |||||
| Goldstein et al., 2020 [16] | Prospective cohort study | 16 postmenopausal women with vulvodynia | Prasterone (DHEA) 6.5 mg vaginal insert daily, 20 weeks | Primary: Vestibular changes | Improvement in vestibular images and pain |
| Secondary: Pain changes | |||||
| Nohales et al., 2020 [17] | Prospective cohort study | 29 postmenopausal women with vestibulodynia and VVA symptoms | Estriol 50 mcg + testosterone 2% daily, 12 weeks | Primary: effect on vulvar discomfort symptoms | Differential diagnosis between vulvodynia an VVA (vulvovaginal atrophy) nsufficiently or poorly treated |
| Murina et al., 2016 [18] | Prospective cohort study | 33 patients with vestibular atrophy and vestibulodynia | Three sessions of vestibular Fractional CO |
effectiveness and safety | Efficacy and safety |
| RCT, randomized control trial; DHEA, Dehydroepiandrosterone; VVA, vulvovaginal atrophy. | |||||
| Authors | RCT | Random | Allocation | Blind | Time from menopause | Drop out (%) | Adverse effects |
| Golsdtein et al., 2019 [12] | Yes | Yes | Yes | Yes | Not described | 10.9 | 26.3% hot flushes |
| (median age: 60 years) | |||||||
| Alvisi et al., 2018 [13] | No | No | No | No | In months: 190 |
Not described | Not described |
| Murina et al., 2018 [14] | No | No | No | No | Not described | 5.5 (hot flushes) | 21% hot flushes |
| Goldstein et al., 2018 [15] | No | No | No | No | Not described | Not described | Non-serious, the % of hot flushes is not described |
| Goldstein et al., 2020 [16] | No | No | No | No | Not described | 31.25 | Not observed |
| Nohales et al., 2020 [17] | No | No | No | No | 12.6 years average (1–41) | 6.9 (adverse effects) | 20.7% hair growth, 17.2 % irritation/acne |
| Murina et al., 2016 [18] | No | No | No | No | Not described | 32.4 | Not observed |
| RCT, randomized control trial. | |||||||
| No of studies | Study design | Risk of bias | Inconsistency | Indirect evidence | Inaccuracy | Other considerations | Certainty |
| 1 [12] | RCT | Low | No | Low | Low | None | |
| 6 [13, 14, 15, 16, 17, 18] | Prospective cohorts | High | No | High | High | None | |
| RCT, randomized control trial. | |||||||
As shown in Fig. 1 (PRISMA Flowchart), the literature search strategy identified
289 articles. Of these, 282 were excluded at various stages of the search.
Finally, we systematically reviewed eight studies: one of the articles describes
an ad hoc study of a RCT with ospemifene [12], three are prospective cohort
studies that also use ospemifene [13, 14, 15], one is a pilot study with prasterone
[16], another study was conducted in Spain using a combination of estrogens and
androgens [17], a study was included that used CO
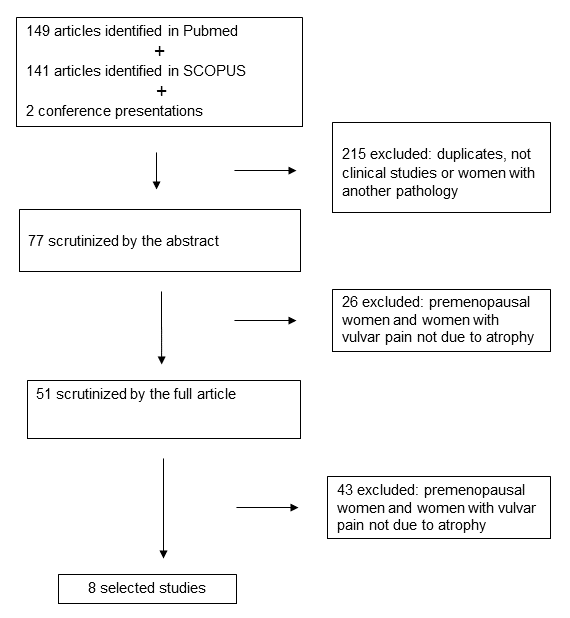 Fig. 1.
Fig. 1.Prisma Flowchart.
Meta-analysis was not possible due to the heterogeneity and small sample size of the included studies.
Most of the studies were considered to be of low to medium quality, primarily because they are not RCTs, or because of the small sample size or high dropout rates (see Tables 2,3).
All studies included heterosexual patients.
Among the described treatments was the use of ospemifene orally at a dose of 60 mg daily for a time period of between 60 days and 20 weeks [12, 13, 14, 15]. These studies report preliminary data showing improvements of vulvar and vestibule trophism [20].
Prasterone showed in an open-label prospective survey, improve in the
vulvoscopic results and dyspareunia, in women that used vaginal prasterone [16].
The combination of estriol and testosterone propionate 2% for 12 weeks showed an
improve of VPA and dyspareunia in a descriptive prospective survey [17]. In both
cases, these followed the indications of the international consensus for the use
of androgenic preparations [21]. A prospective study with 33 women who presented
VPA showed improvements with the use of CO
Different alternatives can improve vulvar pain associated with atrophy: estriol,
ospemifene, prasterone, CO
We propose a therapeutic strategy where the patient expresses her preferences, based on previous experiences and treatments already carried out. In addition, we believe that correctly informing patients about VPA can help a better therapeutic response [7].
Further research is needed to find which treatment shows a superior effect on the vulva. The answer probably lies in the combination of different treatments.
VPA is the symptom of GSM that causes the most discomfort and has the greatest impact on general, psychological, and sexual health along with the quality of life of the affected women [22].
In 2015, the International Society for the Study of Vulvovaginal Disease, International Society for the Study of Women’s Sexual Health, and International Pelvic Pain Society adopted a new vulvar pain and vulvodynia terminology that acknowledges the complexity of the clinical presentation and pathophysiology involved in vulvar pain and vulvodynia, and incorporates new information derived from evidence-based studies conducted since the last terminology published in 2003 [23].
Based on the important repercussions of VPA for women’s sexual life and with the aim of promoting sexual health, health services should ensure diagnostic and therapeutic interventions related to sexuality [2, 3, 4, 5, 6]. VPA is caused by the post-menopausal decline of estrogens and androgens [24]. The fundamental differences between this condition and the pain caused by vaginal atrophy lie in the greater involvement of androgens and the effects on the innervation of the vulvar structures. The vestibule is the vulvar structure most affected by hormonal deficiencies and is the one that has the greatest impact on post-menopausal dyspareunia [18].
VPA should be distinguished from other vulvodynia, particularly in women who do not show adequate response to local or systemic menopausal hormone therapy (MHT). The management of vulvar pain due to atrophy is currently a challenge in our daily clinical practice. Relatively few studies have helped to develop tools to improve the pain suffered by these women, and the impact on their quality of life or sexual experience is severe [22].
Most studies have considered the vulva and vagina in general, few studies have considered the vulva independently of the vagina. This is important, because we already know that they are different structures, with different concentrations of receptors and that they may not respond the same to treatments.
A different physiopathology has been observed for the vulva in comparison with the vagina. Thus, as with the vagina, vulvar manifestations of GSM depend on the duration of hypoestrogenism, but also largely on hypoandrogenism. This is due to the fact that estrogens and androgens act on specific receptors which are found in varying quantities and concentrations in the epithelium, stromal tissue, muscle fibers and blood vessels of all vulvar structures [2, 3, 4, 5, 6].
There are tools that can help us to make a good diagnosis of vulvar atrophy and VPA, for example the Vulvar Health Index (VuHI) [22]. With this index we can assess the severity of the atrophy as well as the improvement that occurs with the treatments.
The main limitation of this review is the inability to conduct a metanalysis due to the heterogeneity of the reviewed studies. Most studies fail to specifically define the severity of VPA, whilst the criteria used to determine degrees of severity do not include VPA scores or the ability of this condition to alter patterns of sexual functioning. Other important limitations to consider are the small sample size of most of the studies, along with dropout rates and follow-up failures. The studies also differed in terms of outcome measurement, which hindered a pooled analysis. With the exception of one RCT using ospemifene, the quality of the studies was generally low or very low.
Thus, there is a need for high-quality trials with more participants to provide us with better grades of recommendation.
In conclusion, this systematic review reveals specific therapeutic alternatives
for the treatment of vulvar atrophy and VPA, including oral ospemifene, local
androgens, local estrogens, DHEA and CO
VPA, vulvar pain due to atrophy; GSM, Genitourinary syndrome of menopause; MHT, menopausal hormone therapy.
NM, LB and SS designed the research study. SS extracted the relevant data on the main characteristics of the eligible studies to obtain a summary, which were narratively described and compared for analysis. LB and NM made a cross-checked data to ensure accuracy. SS analyzed the data. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript.
Not applicable.
Thanks to the Your English Lab for their translation and editing. Thanks to all the peer reviewers for their opinions and suggestions.
This research received no external funding.
The authors declare no conflict of interest.
Supplementary material associated with this article can be found, in the online version, at https://ceog.imrpress.com/EN/10.31083/j.ceog4804128.