



 , Osamu Kobayashi 1, Takahiro Nakajima 1, Takehiro Nakao 1, Chiaki Takeya 1, Mikiko Asai-Sato 1, Fumihisa Chishima 1, Misako Iwata 2, Kei Kawana 1,*
, Osamu Kobayashi 1, Takahiro Nakajima 1, Takehiro Nakao 1, Chiaki Takeya 1, Mikiko Asai-Sato 1, Fumihisa Chishima 1, Misako Iwata 2, Kei Kawana 1,*1 Department of Obstetrics and Gynecology, Nihon University School of Medicine, 30-1 Oyaguchi-kamimachi, Itabashi-ku, 173-8610 Tokyo, Japan
2 Department of Obstetrics and Gynecology, Tokyo Metropolitan Ohtsuka Hospital, 2-8-1 Minami Ohtsuka Toshima-ku, 170-8476 Tokyo, Japan
† These authors contributed equally.
Abstract
X-ray pelvimetry is used for evaluation of pelvic inlet generally to diagnose cephalopelvic disproportion (CPD) or contracted inlet. Cesarean section delivery (C/S) is often performed for labor dystocia without CPD or contracted inlet. We examined whether X-ray pelvimetry is useful to decide on mode of delivery in women with dystocia. A total of 1118 pregnant women received X-ray pelvimetry before or during labor. 205 women with cesarean deliveries for indications except for dystocia were excluded. 913 women undergoing induction/augmentation were retrospectively investigated. Obstetrical and maternal variables were analyzed by univariate, multivariate or ROC analysis. Among 913 women, 37 including three with contracted inlet and seven with CPD, gave birth by C/S, whereas 876 gave birth by vaginal delivery. Low maternal height, older age, small obstetrical conjugate, large weight and infant head size were associated with risk of C/S for dystocia. Multivariate analysis revealed that the obstetrical conjugate was an independent variable for risk of C/S. The area under the ROC curve and the optimal cut-off values, respectively, were as follows: obstetrical conjugate: 0.68 and 11.7 cm (odds ratio = 4.27), transverse diameter: 0.59 and 11.4 cm (odds ratio = 1.82), maternal height: 0.70 and 155.5 cm (odds ratio = 4.33), and maternal weight before pregnancy: 0.55 and 49.7 kg (odds ratio = 1.98). The obstetrical conjugate was an independent variable associated with risk of C/S for dystocia. Maternal height was comparable to the conjugate in term of diagnostic ability. Our data suggested that routine X-ray pelvimetry was not beneficial to identify women at risk of C/S for dystocia.
Keywords
- X-ray pelvimetry
- Labor dystocia
- Cephalopelvic disproportion
X-ray pelvimetry is a digital examination to evaluate the pelvic cavity of pregnant women and is often used for the diagnosis of contracted pelvic inlet and cephalopelvic disproportion (CPD). Women who are short in stature are occasionally subjects of pelvimetry since low maternal height is assumed to correlate with contracted pelvic inlet. In East Asia, pregnant women with low height less than 150 cm are observed, and such women are evaluated by pelvimetry as a screening test for contracted inlet. Additionally, unengaged fetal head during labor regardless of effective uterine contraction suggests CPD, and pelvimetry is considered as an objective mean precisely to distinguish CPD. Such women often receive labor induction or augmentation by oxytocin after excluding CPD. In terms of CPD diagnosis, X-ray pelvimetry is very useful because of the simple and rapid examination involved.
The guidelines of maternal-fetal medicine and/or the attached documents of pharmaceutical agents for labor induction/augmentation often show that X-ray pelvimetry is recommended to negate contracted inlet prior to induction/augmentation [1]. However, a Cochran review in 2017 reported that routine X-ray pelvimetry leads to the increased rate of cesarean delivery but does not improve other perinatal outcomes [2]. Dystocia sometimes occurs during labor due to various mechanisms, even when CPD or contracted inlet are negated. In such cases, cesarean delivery for dystocia is often performed following a trial of vaginal delivery, including pharmaceutical or mechanical induction/augmentation. The cesarean birth rate increased for a decade starting in 2000 and has remained unchanged from 2010 at 32–33% in the United States [3]. More than 85% of cesarean deliveries are performed for four major reasons: nonreassuring fetal status, fetal presentation, prior cesarean operation and dystocia. When repeat cesarean deliveries are included, approximately 60% of all cesarean deliveries are attributable to the diagnosis of abnormal labor [4]. Thus, the diagnostic criteria of the arrested labor have been revised to prevent unnecessary first cesarean deliveries for dystocia in the United State [5]. It is important for reducing the cesarean birth rate to understand the risk factors of cesarean delivery for dystocia.
We have perform routine X-ray pelvimetry to evaluate the pelvic cavities of all pregnant women prior to pharmacological induction/augmentation. No study has ever conducted X-ray pelvimetry on all pregnant women undergoing the induction/augmentation. In this study, we retrospectively investigated their obstetrical variables, including evaluation of the pelvic inlet (obstetrical conjugate and transverse diameter) to determine whether routine X-ray pelvimetry can identify women at risk of cesarean delivery for dystocia. Our data could provide obstetricians with a basis of for considering the indications for X-ray pelvimetry in the management of labor and delivery.
This study was a retrospective survey study of pregnant women who delivered at the Tokyo Metropolitan Otsuka Hospital. This study was approved by the Ethics Committee of our hospital, and decisions of enrolled pregnant women to be included in this study were expressed by the opt-out approach.
A total of 1118 pregnant women had received X-ray pelvimetry at the end of pregnancy from 2014–2017 in the Tokyo Metropolitan Otsuka Hospital. The X-ray pelvimetry was performed routinely prior to pharmaceutic and/or mechanical methods of labor induction/augmentation to negate contracted inlet or CPD. Among 1118 women who received X-ray pelvimetry, 205 women with C/S due to reasons as following were excluded; nonreassuring fetal status, twin pregnancy, maternal hypertensive disorder, breech presentation, threated uterine rupture after previous uterine surgery, and intrauterine infection. The remaining 913 were included in our analysis dividing into two groups: cesarean (n = 37) and vaginal (n = 876) delivery groups (Fig. 1).
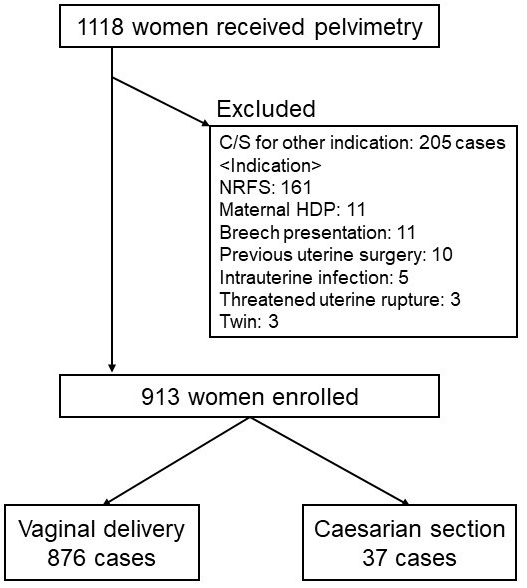 Fig. 1.
Fig. 1.Subject of this study. Among 1118 women who received X-ray pelvimetry, 205 women with C/S due to reasons other than dystocia were excluded. The remaining 913 were divided into two groups: cesarean (n = 37) and vaginal (n = 876) delivery groups.
X-ray pelvimetry was performed by the Guthmann and Martius methods, which are standard for the evaluation of the pelvic inlet [6]. The obstetrical conjugate and transverse diameter of all cases were measured using a ruler by a specialist in maternal-fetal medicine. CPD was diagnosed due to unengaged fetal head, suspected large for date infant and maternal contracted inlet. Maternal contracted inlet was diagnosed by the definition of the Japanese Society of Obstetrics and Gynecology (JSOG) as follows: the obstetrical conjugate measures 10.5 cm or more for normal, 9.5–10.5 cm for relatively contracted, and less than 9.5 cm for contracted inlet; and the transverse diameter measures 11.5 cm or more for normal, 10.5–11.5 cm for relatively contracted, and less than 10.5 cm for contracted inlet [7].
Patient back grounds and obstetrical and infant variables were investigated retrospectively. The data including the obstetrical conjugate and transverse diameter were collected by examining medical records. All data were anonymized and kept strictly confidential by the investigators.
Comparisons in these variables between cesarean versus vaginal delivery groups
were made by the Mann-Whitney U test since the distribution of each data was
non-uniform. Chi square test was also performed for categorical data. The
independent risk factor for cesarean birth was analyzed by multivariate
regression analysis. P value
To determine which variables are related to risk of C/S for labor dystocia, we focused on women with cesarean delivery for dystocia and then compared them to those with vaginal delivery. 913 women were included for final analysis. Overall, 37 (4%) of 913 women underwent C/S for dystocia, while 876 women gave birth by vaginal delivery (summarized in Fig. 1). Among them, seven cases were diagnosed as CPD according to the clinical situation.
Next, we compared between the C/S for dystocia vs. vaginal delivery groups in
various obstetrical variables to identify a possible warning sign of C/S for
dystocia (Table 1). Low maternal height, older age, small obstetrical conjugate,
large weight and head size of infant were associated with risk of C/S for
dystocia with significant differences (Mann-Whitney U test; P
| Obstetrical variable | C/S (n = 37) | Vaginal delivery (n = 876) | P value** |
| Mother | |||
| Age* | 37.0 |
33.0 |
0.004 |
| Parity* | 0.0 |
0.0 |
0.675 |
| Height* | 154.0 |
158.0 |
|
| BW before pregnancy* | 49.7 |
52.0 |
0.275 |
| BW at delivery* | 62.6 |
63.7 |
0.862 |
| Pelvimetry | |||
| Gestational week of measure* | 39.0 |
39.0 |
0.353 |
| Obstetrical conjugate* | 11.6 |
12.2 |
|
| Transverse diameter* | 11.8 |
11.8 |
0.050 |
| Delivery | |||
| Gestational week of delivery* | 40.0 |
40.0 |
0.016 |
| Intervention for delivery | 0.148*** | ||
| No intervention | 9 | 183 | |
| Induction | 16 | 270 | |
| Augmentation | 12 | 423 | |
| Newborn infant | |||
| BW* | 3315.0 |
3112.5 |
|
| Head circumference* | 34.3 |
33.5 |
|
| Biparietal diameter (BPD)* | 9.6 |
9.3 |
0.036 |
| Gender | 0.759*** | ||
| Male | 17 | 425 | |
| Female | 20 | 451 | |
| *: Median and SD. **: P value by Mann-Whitney U test. ***: P value by Chi square test. | |||
Older pregnant women are likely to undergo C/S due to not only their cervical
resistance, uterine dysfunction or both but also maternal exhaustion. Indeed,
maternal age in the C/S group (37.0
| Variables | Odds ratio | 95% CI | P value* |
| Mother | |||
| Age | 0.95 | 0.86–1.04 | 0.30 |
| Height | 1.05 | 0.92–1.20 | 0.49 |
| Pelvimetry | |||
| Obstetrical conjugate | 3.13 | 1.32–7.14 | 0.01 |
| Transverse diameter | 2.44 | 0.95–6.25 | 0.06 |
| Delivery | |||
| Gestational week of delivery | 0.93 | 0.55–1.59 | 0.80 |
| Newborn infant | |||
| BW | 1.00 | 1.00–1.01 | 0.42 |
| Head circumference | 0.83 | 0.47–1.45 | 0.51 |
| BPD | 0.36 | 0.06–2.22 | 0.27 |
| **: P value by Logistic regression analysis. | |||
A correlation between maternal height and the obstetrical conjugate in Asian
women has not been clarified, although the two maternal physical characteristics
are likely to correlate to each other. We then plotted the two variables of 913
women, as shown in Fig. 2. The open and closed dots indicate women with vaginal
delivery (n = 876) and cesarean delivery (n = 37), respectively (Fig. 2A). The
dots show the significant correlation between maternal height and the conjugate
(R = 0.483, P
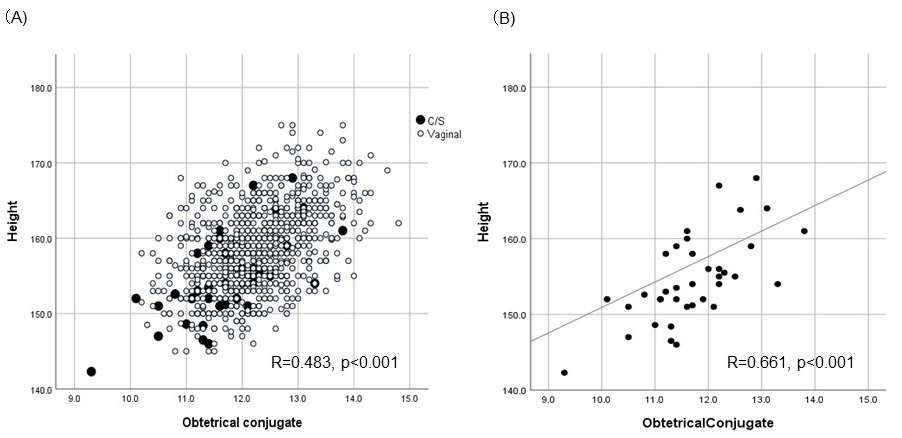 Fig. 2.
Fig. 2.Correlation between the obstetrical conjugate and maternal height. (A) Open dots indicated women with vaginal delivery and close dots indicated women with C/S for dystocia. (B) Close dots (women with C/S) were taken up and linear line indicated correlation (R = 0.661).
Our multivariate analysis revealed that the obstetrical conjugate was an independent variable associated with risk of C/S for dystocia. We also demonstrated the correlation between the conjugate and maternal height. We then tried to examine whether alternative maternal variables could be warning signs of C/S for dystocia compared with the obstetrical conjugate by ROC curve analysis (Fig. 3). We considered that ROC curve analysis can evaluate various maternal variables as measures that either confirm the presence of risk of C/S or rule out the risk. ROC curves of the maternal variables height, weight before pregnancy, the obstetrical conjugate and transverse diameter were calculated by plotting the sensitivity versus 1-specificity of each threshold value. These ROC curves provided areas under the ROC curve (AUCs) and the optimal cut-off value of each variable and enabled us to compare the diagnostic abilities of the four variables to discriminate the possible risk of C/S in women with dystocia. The AUCs and the optimal cut-off values, respectively, were as follows: maternal height (bold line): 0.70 and 155.5 cm (odds ratio = 4.33, sensitivity = 64.9%), maternal weight before pregnancy (dotted thin line): 0.55 and 49.7 kg (odds ratio = 1.98, sensitivity = 51.3%), obstetrical conjugate (bold dotted line): 0.68 and 11.7 cm (odds ratio = 4.27, sensitivity = 59.5%), and transverse diameter (thin line): 0.59 and 11.4 cm (odds ratio = 1.82, sensitivity = 40.5%) (Fig. 3). The lines for maternal height and the obstetrical conjugate overlapped each other, and these AUCs (0.70 vs. 0.68) were clearly higher than those of maternal weight and transverse diameter. The odds ratios of C/S at the optimal cut-off value were 4.33 for maternal height and 4.27 for the obstetrical conjugate, indicating that maternal height was comparable to the obstetrical conjugate as a measure to discriminate the maternal risk of C/S.
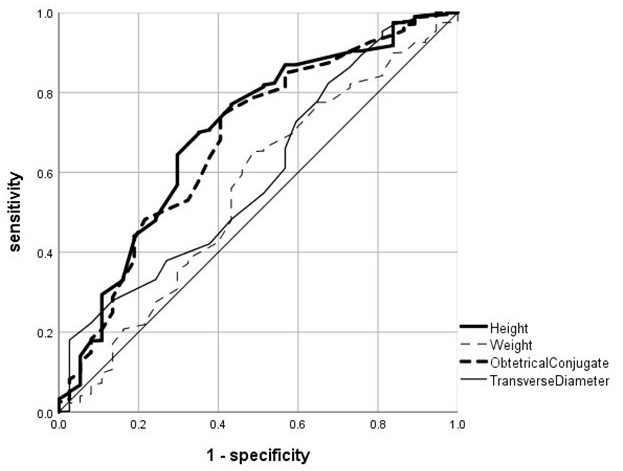 Fig. 3.
Fig. 3.ROC curve analysis of four maternal variables for risk of C/S. ROC curves of maternal height (bold line), maternal weight before pregnancy (dotted thin line), obstetrical conjugate (bold dotted line), and transverse diameter (thin line) were shown. The curves were calculated by plotting sensitivity (Y-axis) versus 1-specificity (X-axis) of each threshold value.
In this study, we investigated the association between measures (the obstetrical conjugate and transverse diameter of pelvic inlet) of X-ray pelvimetry and cesarean delivery for labor dystocia using data from 913 women in labor. Our data indicated that the obstetrical conjugate was an independent variable correlating inversely with the incidence of C/S for dystocia but that maternal height could be a comparable variable to the conjugate in terms of the discrimination of the risk of C/S.
X-ray pelvimetry is a useful measure to evaluate the inlet to exclude CPD or contracted inlet and is recommended prior to labor induction/augmentation to negate the contracted inlet according to a guideline of maternal-fetal medicine in Japan [1]. Thus, we have routinely performed pelvimetry on all women who are to undergo induction or augmentation for various reasons. However, among 913 women, contracted inlet was only observed in four women (4/913 = 0.4%). Conversely, a Cochran systematic review demonstrated that women who receive X-ray pelvimetry are likely to undergo C/S. Dystocia is not only one of the major reasons for C/S but is also associated with pelvic disproportion, which is evaluated by pelvimetry. Then, we took an interest in the clinical question of whether measurements obtained from X-ray pelvimetry are associated with the incidence of C/S and influence our decision of mode of delivery in the cases of dystocia. Our database of more than one thousand measures obtained from routine X-ray pelvimetry was valuable to clarify this question. The Cochran review performed in 2017 identified five studies with a total of 1159 women, and these studies compared X-ray pelvimetry (n = 582) versus no pelvimetry (n = 577) [2]. The number of women who received X-ray pelvimetry in our study was greater than that in the Cochran review.
In this study, we excluded women undergoing C/S due to nonreassuring fetal
status, fetal presentation or prior uterine operation from the subject of
analysis. All of the remaining 913 women received X-ray pelvimetry prior to labor
induction and/or augmentation and delivered a baby by either cesarean or vaginal
deliveries. Overall, 37 women with C/S for dystocia and 876 women with vaginal
delivery were compared. Univariate analysis revealed that maternal height and
age, infant weight and head size, and the obstetrical conjugate were associated
with risk of C/S, with significant differences. Regarding measures of X-ray
pelvimetry, a significant difference (P
Previous studies [8, 9] and a systematic review [2] have demonstrated that X-ray pelvimetry does not improve perinatal outcome and that routine X-ray pelvimetry is not useful to women with normal presentation. Regarding women with previous C/S or breech presentation, some studies have reported the usefulness of X-ray pelvimetry [10]. Our study did not address the usefulness of X-ray pelvimetry from the viewpoint of perinatal outcome, and thereby, we did not compare the outcome with the no-X-ray pelvimetry group.
In this study, the transverse diameter identified three cases of contracted inlet and one relatively contracted inlet, and all underwent C/S with CPD, while the obstetrical conjugate identified only two women with C/S among nine with contracted or relatively contracted inlet. The transverse diameter was more significant than the obstetrical conjugate in terms of the diagnostic measure of contracted inlet. Nevertheless, the abnormality detected by X-ray pelvimetry rarely occurred in our population (contracted inlet: 4/913, relatively contracted: 9/913, and CPD: 7/913 women). Several studies have reported that maternal height with or without a measure of pelvimetry can be a variable to predict dystocia [11] or CPD [12]. Maternal height is also reported to correlate to the obstetrical conjugate [13]. Indeed, our data clearly indicated the correlation between maternal height and the obstetrical conjugate, regardless of mode of delivery. Since the obstetrical conjugate was associated with risk of C/S for dystocia, maternal height in our population was thought to be an alternative variable for the conjugate. Our ROC analysis demonstrated the hypothesis that maternal height is comparable to the obstetrical conjugate to discriminate maternal risk of C/S for dystocia. Numerous previous studies have demonstrated that maternal height is inversely related to risk of not only C/S [14, 15, 16, 17, 18] but also labor dystocia [19, 20, 21, 22, 23]. Taken together with our ROC curve, maternal short stature is sufficient to be an independent variable associated with the decision of mode of delivery.
In contrast, the transverse diameter did not show high diagnostic capacity. Interestingly, the 11.4 cm cut-off value for the transverse diameter on the ROC curve was concordant with the upper criterion (11.5 cm) of a relatively contracted inlet, while 11.7 cm for the obstetrical conjugate was quite different from the upper criterion (10.5 cm) of a relatively contracted inlet.
This study has some limitations. Since this was a retrospective study, the variability of the obstetricians in charge of decision making in the choice of delivery mode could not be ruled out. We also cannot deny the possibility that the diagnosis of dystocia also varied among the obstetricians in charge. On the other hand, the strength of this study was that the X-ray pelvimetry data were available for all of the more than 900 women in labor and the data were measured by the same obstetrician using the same rules.
X-ray pelvimetry is an important measurement to evaluate the pelvic inlet, especially prior to labor induction/augmentation. However, contracted inlet is a very rare event (approximately 1%) in Asian women, and maternal height can be comparable to measures of X-ray pelvimetry. Our data indicated that routine X-ray pelvimetry is not of value to decide on mode of delivery for women with dystocia.
AUC, areas under curve; CPD, cephalopelvic disproportion; C/S, cesarean section.
KaK, YT and MI conducted this study and measured X-ray pelvimetry. YI and AK made figures and tables. OK, NakajT, NakaoT, CT, MAS, FC investigated data of patients and analyzed them by statistical methods. KeiK and AK organized this study and described the article. All authors have read and approved the manuscript.
All subjects gave their informed consent for inclusion before they participated in the study. The study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the Ethics Committee of Tokyo Metropolitan Ohtsuka Hospital (2018-77). The decision of enrolled pregnant women to be included in this study was expressed by opt-out approach, which is posted on the board in the hospital and our hospital’s web site.
We are very thankful to Mrs. Naoko Tomita for her excellent management of clinical data and edit of the manuscript.
This research was supported by Japan Agency for Medical Research and Development under Grant Number JP 20gk0110042h0002.
The authors declare no conflict of interest.