




1 Department of Obstetrics and Gynecology, Alexandria University, Faculty of Medicine, Shatby Maternity Hospital, 21526 Alexandria, Egypt
Abstract
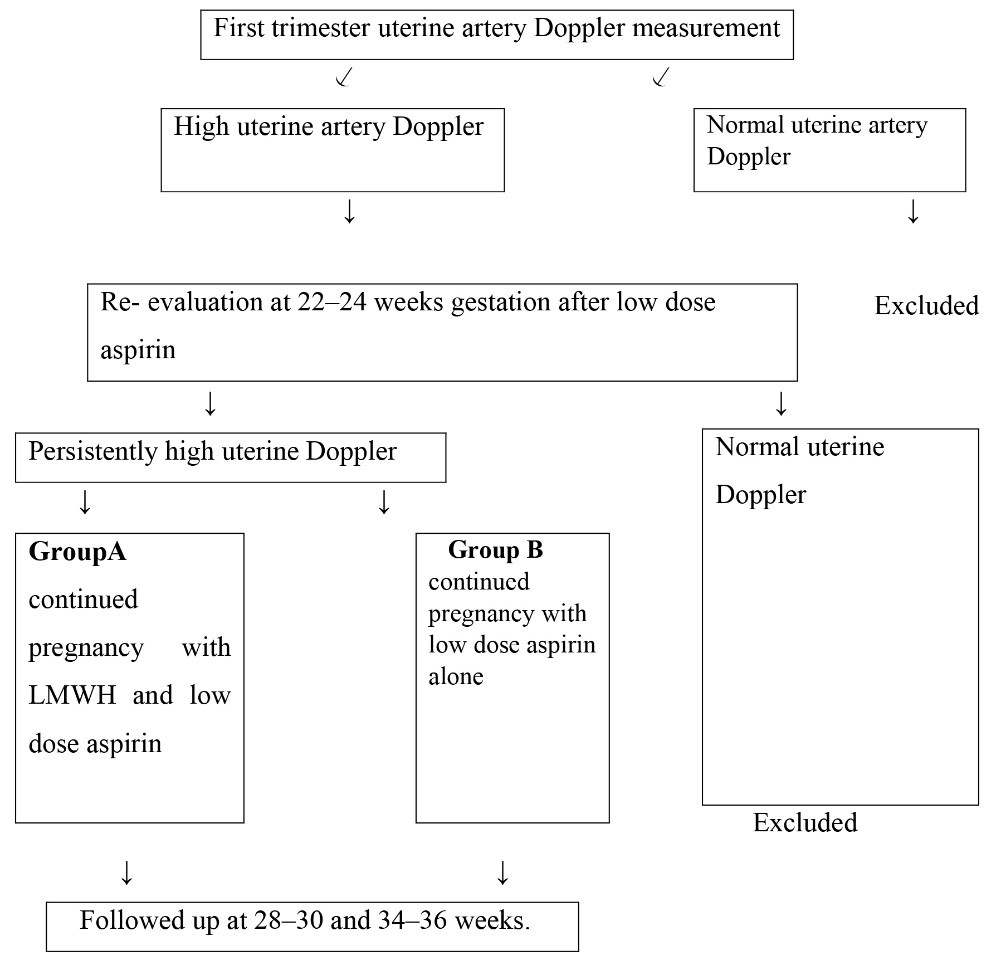
Introduction: Trophoblastic invasion converts the uteroplacental circulation into a low resistance, high capacitance system. Defective invasion causes hypoperfusion and pregnancy complications. Early pregnancy uterine artery Doppler demonstrates low end-diastolic velocities. Its PI and RI decrease with increasing gestation. Aim of the study: Examing the effect of adding low molecular weight heparin (LMWH) to low-dose aspirin on persistent high uterine artery Doppler indices and its impact on fetal growth and pregnancy outcome. Patients and methods: After approval of Alexandria university ethics committee, pregnant cases with positive past history of placental vascular complication including; placental abruption, pre-eclampsia, small-for-gestational age (SGA) pregnancies and fetal growth restriction were recruited. All selected patients were in good general health without previous history of Diabetes Mellitus or thyroid disorders or cardiac diseases. Patients with thrombocytopenia, bleeding tendencies, multiple pregnancies, and pregnancies complicated by fetal or neonatal chromosomal or structural anomalies were excluded from the study. Eligible patients were 412, all were subjected to uterine artery Doppler measurement in the first trimester. 148 cases had high uterine artery Doppler PI, they were given low dose aspirin and were re-evaluated at 22–24 weeks gestation. 58 cases had persistently high uterine artery Doppler PI, they were allocated into 2 groups each of 29 cases; Group A LMWH with aspirin. Group B only low dose aspirin. 50 pregnants with normal uterine artery Doppler PI from the start were taken as a control group. All participants were followed up at 28–30 and 34–36 weeks. Primary outcome: Normal uterine, umbilical and cerebral artery Doppler measurements after LMWH. Secondary outcome: Prevention of pregnancy complications and neonatal complications. Results: Uterine and umbilical artery Doppler and amount of liquor significantly improved. Conclusion: LMWH influenced uterine artery and umbilical Doppler measurements and amount of liquor and reduced the risk of neonatal hypoxic ischaemic encephalopathy.
Keywords
- LMWH
- Uterine Doppler
- Umbilical Doppler
- Oligohydramnios
The placenta is important for the transport of nutrients and oxygen to the fetus. Placental remodeling occurs in two stages; the first stage starts in the first trimester, when the trophoblastic cells invade the intra-decidual portion of the spiral arteries then they deeply invade the myometrial segments of the spiral arteries from 14 weeks’ gestation causing loss of smooth muscle and elastica from the spiral arteries converting the uteroplacental circulation into a low resistance, high capacitance system [1, 2]. The second stage of placental remodeling is completed between 16 to 18 weeks gestation. Defective placental implantation leads to hypoperfusion, hypoxic reperfusion injury, and oxidative stress which is thought to underlie the pathophysiology of gestational hypertension, preeclampsia (PE), intra-uterine fetal growth restriction (IUGR), preterm labor, placental abruption, and second-trimester miscarriages [3, 4].
In the nonpregnant state and in early pregnancy, Doppler interrogation of the uterine artery demonstrates low end-diastolic velocities and an early diastolic notch. Uterine artery PI and RI values decrease with increasing gestational age due to a fall in impedance in uterine vessels following trophoblastic invasion. Resistance to blood flow within the uteroplacental circulation is transmitted upstream to the uterine arteries and can be measured as an increased pulsatility index (PI) or resistance index [5, 6, 7].
Improvements in uterine blood flow following low-dose aspirin or low molecular weight heparin (LMWH) administration has been reported to improve pregnancy outcomes particularly in those patients with decreased uterine blood flow and poor obstetric histories, such as recurrent pregnancy loss (RPL) or antiphospholipid antibody syndrome (APS) [8, 9].
In this study we aimed to examine the effect of adding low molecular weight heparin (LMWH) to aspirin on the flow velocity of uterine and umbilical arteries in cases with persistently high uterine artery Doppler, on fetal growth and pregnancy outcome.
The study was approved by ethics committee of the Alexandria faculty of the college of medicine. Informed consent was obtained prior to the initiation of the study.
Cases with positive past history of placental vascular complication including placental abruption, pre-eclampsia, small-for-gestational age (SGA) and fetal growth restriction were recruited from the ANC clinic. None of the patients had a past history of diabetes mellitus, thyroid disorders or cardiac disease. Cases of thrombophilia, thrombocytopenia, bleeding tendencies, multiple gestation, and pregnancies complicated by fetal or neonatal chromosomal or structural anomalies were excluded.
Uterine artery Doppler assessment was done in the first trimester by a transvaginal ultrasound technique using a 4.6–8 MHz transvaginal transducer placed in the anterior vaginal fornix, where a sagittal section of the cervix was obtained. The probe was moved laterally until the paracervical vascular plexus was identified. Color flow Doppler was applied and the uterine artery was identified at the level of the cervico-uterine junction. Measurements were taken at the point before the uterine artery branches into the arcuate arteries.
Cases identified with high uterine artery Doppler PI were administered low dose
aspirin 75 mg tablets daily (Ezacard, Global Nabi, Egypt) and were re-evaluated
in the second trimester (22–24 weeks of gestation) by a transabdominal approach
where a 3.5-MHz curvilinear transabdominal transducer was used. A midsagittal
section of the uterus and cervical canal was obtained and the transducer was
moved laterally until the paracervical vessels were visualized. Color flow
Doppler was applied. The uterine arteries were visualized along the side of the
cervix. Pulsed wave Doppler flow velocity waveforms from the ascending branch of
the uterine artery at the point closest to the internal os were obtained, with
the Doppler sampling gate set at 2 mm. The smallest angle of
insonation (
| GA (weeks) | 5 |
50 |
95 |
| 11 | 1.18 | 1.79 | 2.70 |
| 12 | 1.11 | 1.68 | 2.53 |
| 13 | 1.05 | 1.58 | 2.38 |
| 14 | 0.99 | 1.49 | 2.24 |
| 15 | 0.94 | 1.41 | 2.11 |
| 16 | 0.89 | 1.33 | 1.99 |
| 17 | 0.85 | 1.27 | 1.88 |
| 18 | 0.81 | 1.20 | 1.79 |
| 19 | 0.78 | 1.15 | 1.70 |
| 20 | 0.74 | 1.10 | 1.61 |
| 21 | 0.71 | 1.05 | 1.54 |
| 22 | 0.69 | 1.00 | 1.47 |
| 23 | 0.66 | 0.96 | 1.41 |
| 24 | 0.64 | 0.93 | 1.35 |
| 25 | 0.62 | 0.89 | 1.30 |
| 26 | 0.60 | 0.86 | 1.25 |
| 27 | 0.58 | 0.84 | 1.21 |
| 28 | 0.56 | 0.81 | 1.17 |
| 29 | 0.55 | 0.79 | 1.13 |
| 30 | 0.54 | 0.77 | 1.10 |
| 31 | 0.52 | 0.75 | 1.06 |
| 32 | 0.51 | 0.73 | 1.04 |
| 33 | 0.50 | 0.71 | 1.01 |
| 34 | 0.50 | 0.70 | 0.99 |
| 35 | 0.49 | 0.69 | 0.97 |
| 36 | 0.48 | 0.68 | 0.95 |
| 37 | 0.48 | 0.67 | 0.94 |
| 38 | 0.47 | 0.66 | 0.92 |
| 39 | 0.47 | 0.65 | 0.91 |
| 40 | 0.47 | 0.65 | 0.90 |
| 41 | 0.47 | 0.65 | 0.89 |
Cases with persistent high uterine artery Doppler PI were allocated into 2 groups. Allocation was performed at random by an independent statistician using a shuffled deck of cards (odd numbers for Group A, even-numbers for Group B) to equilize the 2 arms among subjects.
Group A were given low molecular weight heparin (LMWH) [enoxaparin sodium (clexane 40 mg/0.4 mL Syringes), Sanofi Aventis, France] addition to the aspirin. The LMWH was administered each evening by a subcutaneous abdominal injection.
Group B received low dose aspirin alone.
These two groups were compared to a control group of 50 patients with normal uterine artery Doppler PI.
All groups were followed up at 28–30 and 34–36 weeks gestation. Measurements obtained were for uterine artery Doppler, umbilical artery Doppler, cerebral artery Doppler, estimated fetal weight utilizing biparietal diameter (BPD), head circumference (HC), abdominal circumference (AC) and femur length (FL) [12] and amniotic fluid index (AFI). Normal AFI values ranged from 5 to 25 cm [13, 14, 15, 16]. Cases were assessed for development of pregnancy complications such as preeclampsia, intrauterine growth restriction (IUGR) and preterm labor. Preeclampsia was defined according to the guidelines of the International Society for the Study of Hypertension in Pregnancy as blood pressure at least 140/90 mmHg on two occasions at least 4 hours apart with 300 mg or more proteinuria during 24 hours after 20 weeks gestation [17]. IUGR was diagnosed if the estimated fetal weight was below the 10th percentile for gestational age together with a Doppler PI in the umbilical artery above the 95th percentile, or if the estimated fetal weight was below the 3rd percentile irrespective of the umbilical artery Doppler [18]. Preterm delivery was defined as delivery before 37 weeks of gestation. All pregnant women received routine antenatal care and were followed until delivery (Table 2).
|
| Primary outcome: normalization of uterine, umbilical and
cerebral artery Doppler measurements after LMWH. Secondary outcome: prevention of pregnancy and neonatal complications. |
After delivery, neonatal outcome was assessed and Apgar scores and admission to the neonatology unit were recorded.
Statistical analysis was done using Statistical Package for Social Sciences (SPSS/version 21) software. Arithematic mean, standard deviation, number and percent were obtained. For categorized parameters, chi square test was used while for numerical data ANOVA-test was utilized to compare more than two groups. The level of significance was 0.05.
We recruited 412 cases with a positive past history of placental vascular complication in previous pregnancies. During the initial prenatal visit in the first trimester, 148 cases had high uterine artery Doppler PI. They were administered low dose aspirin and were re-evaluated during the second trimester. The uterine artery Doppler measurements reverted to normal in 90 cases while the remaining 58 cases had persistently high uterine artery Doppler PI. They were blindly allocated into 2 groups each having 29 cases. Allocation was performed at random by an independent statistician using a shuffled deck of cards (odd numbers for Group A, even-numbers for Group B) to equilize the 2 arms among subjects.
Group A received low molecular weight heparin with low dose aspirin while Group B continued low dose aspirin alone. Group A and B were compared to a control group of 50 cases with a similar past history but with normal uterine artery Doppler.
The three groups had no significant differences as related to demographic data and duration from the last pregnancy (Table 3).
| Group A (Heparin gp) | Group B (Aspirin only group) | Group C (Control group) | ANOVA | |
| P-value | ||||
| Age | ||||
| Range | 23.0–32.0 | 21.0–33.0 | 22.0–31.0 | |
| Mean | 28.4 | 27.6 | 27.4 | 1.088 |
| S.D. | 3 | 3.9 | 2.7 | 0.341 N.S. |
| BMI | ||||
| Range | 23.5–31.0 | 23.6–31.5 | 23.0–30.4 | |
| Mean | 27.1 | 27.4 | 26.9 | 0.469 |
| S.D. | 2.2 | 2.4 | 2.4 | 0.627 N.S. |
| Duration from the last pregnancy | ||||
| Range | 1.2–4.8 | 1.3–4.5 | 1.1–4.8 | |
| Mean | 2.9 | 3.1 | 2.9 | 0.317 |
| S.D. | 1 | 1 | 1.3 | 0.729 N.S. |
| P was significant if | ||||
Uterine artery Doppler measurements during the third trimester were statistically significant among the groups [P = 0.018*]. Only one case in Group A had persistently high uterine artery Doppler PI compared to four cases in Group B. In the control group, uterine artery Doppler PI measurements remained normal throughout the pregnancy (Table 4, Fig. 1).
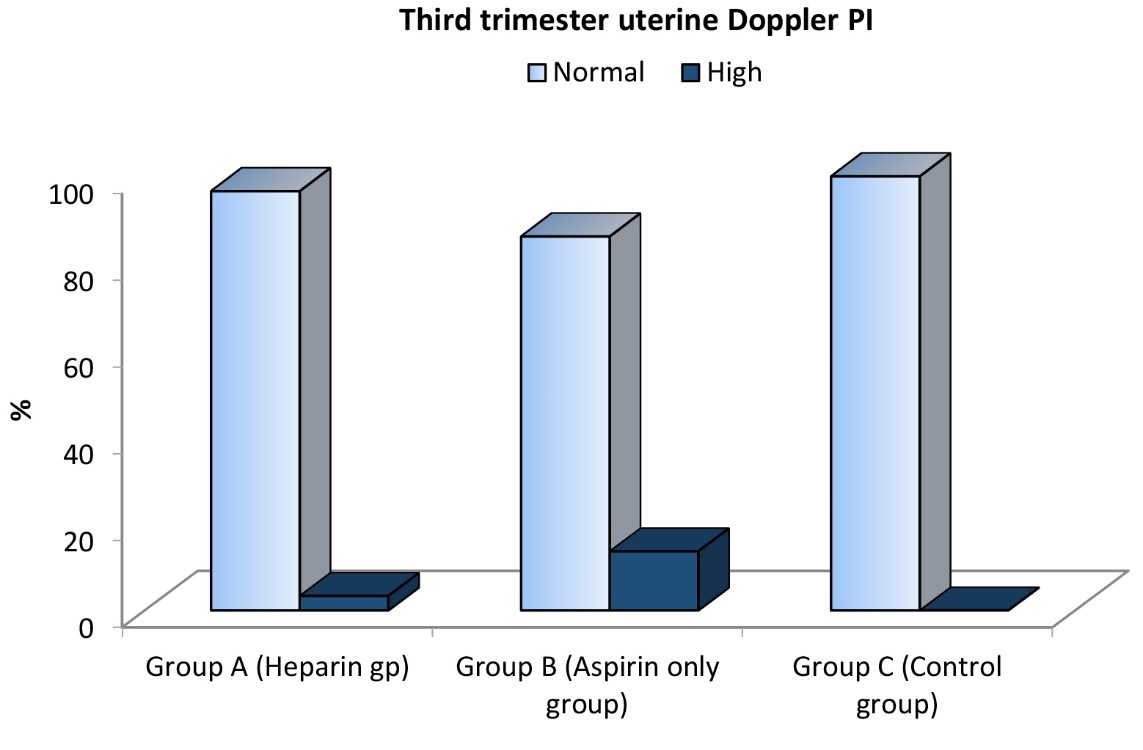 Fig. 1.
Fig. 1.Comparison between the three studied groups regarding third trimester uterine Doppler PI.
| Third trimester uterine Doppler PI | Group | Total | |||
| Group A (Heparin gp) | Group B (Aspirin only group) | Group C (Control group) | |||
| Normal | No. | 28 | 25 | 50 | 103 |
| % | 96.6% | 86.2% | 100.0% | 95.4% | |
| High | No. | 1 | 4 | 0 | 5 |
| % | 3.4% | 13.8% | 0.0% | 4.6% | |
| Total | No. | 29 | 29 | 50 | 108 |
| % | 100.0% | 100.0% | 100.0% | 100.0% | |
| X |
8.034 | ||||
| P | 0.018* | ||||
|
X | |||||
Umbilical artery Doppler measurements were statistically significant among the three groups [P = 0.034]. In Group A, the same patient with the abnormal artery Doppler also had an elevated S/D ratio. In Group B, six cases had abnormal umbilical artery Doppler measurements; three of them were the same cases with abnormal uterine artery Doppler, and the other three had normal uterine Doppler. One case with an abnormal uterine artery Doppler had absent end diastolic flow. In the control group, only one case had an elevated S/D ratio (Table 5, Fig. 2).
| Umbilical Doppler | Group | Total | |||
| Group A (Heparin gp) | Group B (Aspirin only group) | Group C (Control group) | |||
| Normal | No. | 28 | 23 | 49 | 103 |
| % | 96.6% | 79.3% | 98.0% | 95.4% | |
| Abnormal | No. | 1 | 6 | 1 | 8 |
| % | 3.4% | 20.6% | 2.0% | 7.4% | |
| Total | No. | 29 | 29 | 50 | 108 |
| % | 100.0% | 100.0% | 100.0% | 100.0% | |
| X |
6.25 | ||||
| P | 0.034* | ||||
| X | |||||
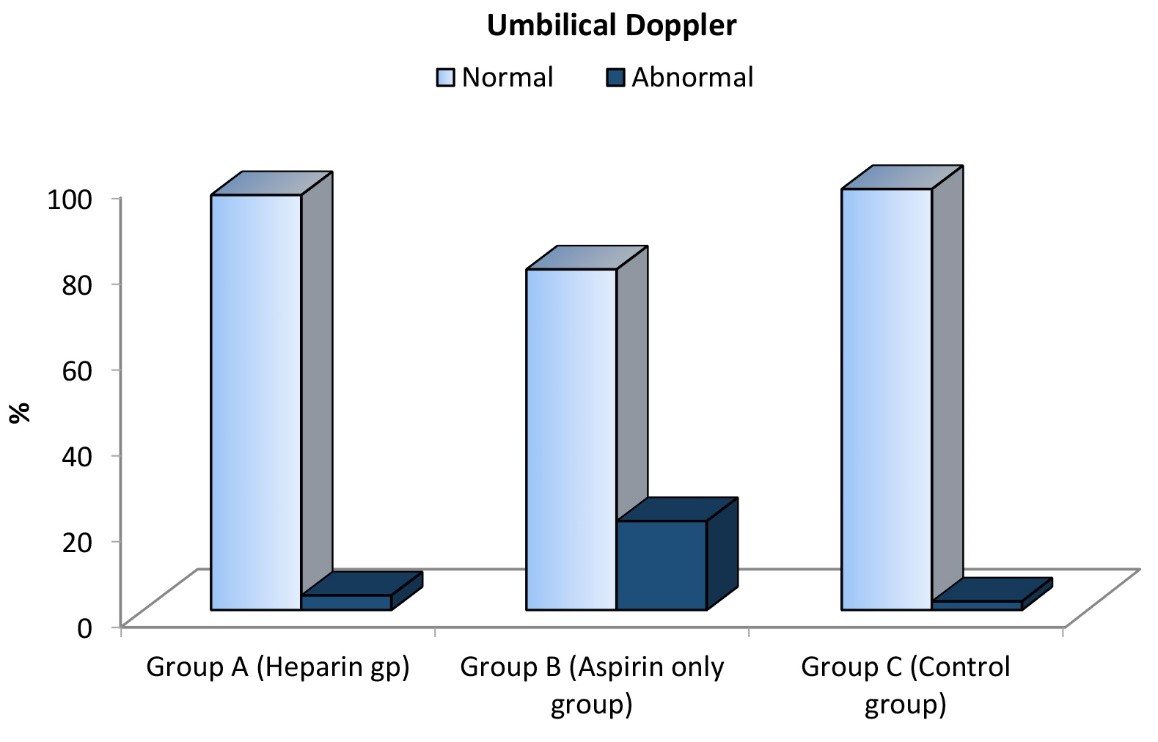 Fig. 2.
Fig. 2.Comparison between the three studied groups regarding umbilical Doppler.
Cerebral artery Doppler measurements although were not statistically significant among the three groups [P = 0.251]. There were no abnormal cases in Group A but two cases of abnormal cerebral artery Doppler occurred in Group B both with fetal growth restriction. These 2 patients had abnormal uterine artery Doppler, abnormal umbilical artery Doppler and one case with absent umbilical end diastolic flow. Both had oligohydramnios and developed preeclampsia (PET). They were delivered at 31–33 weeks gestation with both neonates developing signs of hypoxic ischaemic encephalopathy. No cases of abnormal cerebral artery Doppler were found in the control group (Table 6).
| Cerebral artery Doppler | Group | Total | |||
| Group A (Heparin gp) | Group B (Aspirin only group) | Group C (Control group) | |||
| Normal | No. | 29 | 27 | 49 | 105 |
| % | 100.0% | 93.1% | 98.0% | 97.2% | |
| Abnormal | No. | 0 | 2 | 0 | 2 |
| % | 0.0% | 6.9% | 0.0% | 1.9% | |
| Total | No. | 29 | 29 | 50 | 108 |
| % | 100.0% | 100.0% | 100.0% | 100.0% | |
| X |
2.762 | ||||
| P | 0.251 | ||||
| X | |||||
Obstetric complications encountered were oligohydraminos, PET, IUGR and preterm labor.
Oligohydramnios was present in one case from Group A compared to four cases in Group B (two cases with IUGR and two with abnormal uterine and umbilical arteries Doppler. No cases of oligohydramnios were found in the control group which was statistically significant [P = 0.018] (Table 7, Fig. 3).
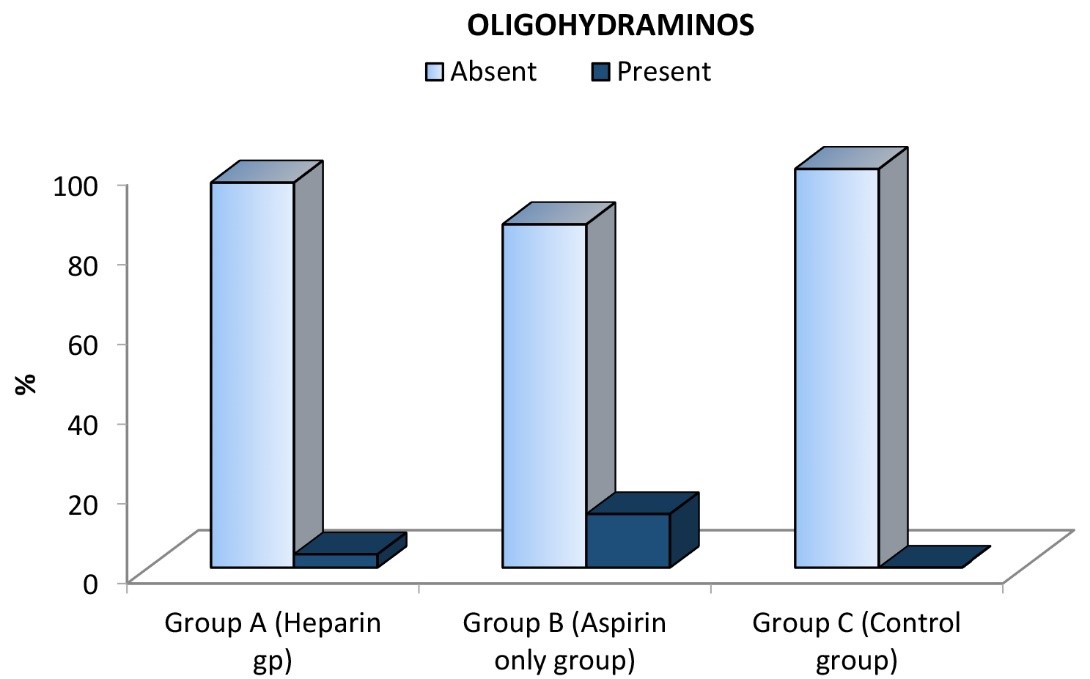 Fig. 3.
Fig. 3.Comparison between the three studied groups regarding oligohydramnios.
| Oligohydramnios | Group | Total | |||
| Group A (Heparin gp) | Group B (Aspirin only group) | Group C (Control group) | |||
| Absent | No. | 28 | 25 | 50 | 103 |
| % | 96.6% | 86.2% | 100.0% | 95.4% | |
| Present | No. | 1 | 4 | 0 | 5 |
| % | 3.4% | 13.8% | 0.0% | 4.6% | |
| Total | No. | 29 | 29 | 50 | 108 |
| % | 100.0% | 100.0% | 100.0% | 100.0% | |
| X |
8.034 | ||||
| P | 0.018 | ||||
| X | |||||
As regards Preeclamptic toxemia (PET), no cases were found in Group A compared to the two cases with IUGR in Group B (4.4) and one case in the control group. This result was not statistically significant [P = 0.251] (Table 8).
| PET | Group | Total | |||
| Group A (Heparin gp) | Group B (Aspirin only group) | Group C (Control group) | |||
| Absent | No. | 29 | 27 | 49 | 105 |
| % | 100.0% | 93.1% | 98.0% | 97.2% | |
| Present | No. | 0 | 2 | 1 | 3 |
| % | 0.0% | 6.9% | 2.0% | 2.8% | |
| Total | No. | 29 | 29 | 50 | 108 |
| % | 100.0% | 100.0% | 100.0% | 100.0% | |
| X |
2.762 | ||||
| P | 0.251 | ||||
| X | |||||
IUGR: one case of IUGR in Group A compared to three cases in Group B. No cases IUGR occurred in the control group. These results were not statistically significant [P = 0.221] (Table 9).
| IUGR | Group | Total | ||||
| Group A (Heparin gp) | Group B (Aspirin only group) | Group C (Control group) | ||||
| Absent | No. | 28 | 26 | 49 | 103 | |
| % | 96.6% | 89.7% | 98.0% | 95.4% | ||
| Present | No. | 1 | 3 | 0 | 4 | |
| % | 3.4% | 10.3% | 0.0% | 3.7% | ||
| Total | No. | 29 | 29 | 50 | 108 | |
| % | 100.0% | 100.0% | 100.0% | 100.0% | ||
| X |
3.02 | |||||
| P | 0.221 | |||||
| X | ||||||
Preterm labor was more common in Group B; three cases delivered prematurely possibly because of PET and IUGR and case secondary to preterm premature rupture of the membranes. One case in Group A due to IUGR and oligohydramnios with no cases in the control group. These results did not reach statistical significance [P = 0.063] (Table 10).
| PTL | Group | Total | |||
| Group A (Heparin gp) | Group B (Aspirin only group) | Group C (Control group) | |||
| Absent | No. | 28 | 26 | 50 | 104 |
| % | 96.6% | 89.7% | 100.0% | 96.3% | |
| Present | No. | 1 | 3 | 0 | 4 |
| % | 3.4% | 10.3% | 0.0% | 3.7% | |
| Total | No. | 29 | 29 | 50 | 108 |
| % | 100.0% | 100.0% | 100.0% | 100.0% | |
| X |
5.515 | ||||
| P | 0.063 | ||||
| X | |||||
All neonates were discharged except for one case in Group A due to respiratory distress and two cases in Group B due to IUGR and hypoxic ischaemic encephalopathy. There were no cases in the control group. This result was not statistically significant [P = 0.253] (Table 11).
| NICU admission | Group | Total | |||
| Group A (Heparin gp) | Group B (Aspirin only group) | Group C (Control group) | |||
| Absent | No. | 28 | 29 | 50 | 107 |
| % | 96.6% | 100.0% | 100.0% | 99.1% | |
| Present | No. | 1 | 2 | 0 | 3 |
| % | 3.4% | 6.9% | 0.0% | 2.8% | |
| Total | No. | 29 | 29 | 50 | 108 |
| % | 100.0% | 100.0% | 100.0% | 100.0% | |
| X |
2.750 | ||||
| P | 0.253 | ||||
Low molecular weight heparin (LMWH) used in pregnancy has been proven to reverse the natural antiangiogenic tendency of first-trimester placental villi [19]. It has been evaluated for the prevention of various placenta-mediated pregnancy complications, including severe preeclampsia and recurrent miscarriage.
In our study, cases using LMWH had statistically significant normal measurements of uterine artery, which was reflected in the course of pregnancy as related to amount of amniotic fluid. Early effects probably occur at the cellular level by decreasing trophoblast apoptosis.
Effect on performance of uterine artery Doppler has been investigated in many trials.
In 2006, researchers performed a controlled, open-labeled study which included
94 women with gestational hypertension and 30 healthy women enrolled at 24 to 26
weeks gestation. Doppler evaluation of uterine artery resistance index (RI) was
performed before and after a two-week course of LMWH or no treatment. This study
investigated whether a short course of subcutaneous low-molecular-weight heparin
(LMWH) might modify the performance of uterine artery Doppler to predict
preeclampsia and small-for-gestational age (SGA) infants in a high-risk
population. The authors found a significant decrease of uterine artery RI after
LMWH (P
These results match with ours as adding LMWH to aspirin reduced the high uterine artery Doppler PI.
A randomized controlled trial included 139 women with inheritable thrombophilia seen prior to 12 weeks of gestation with a history of previous delivery before 34 weeks of gestation secondary to hypertensive disorders of pregnancy and/or small-for-gestational-age infants. Women were randomized to receive either daily LMWH with aspirin or aspirin only and they followed with flow velocity within the uterine and umbilical arteries as well as evaluation of fetal growth. They found that addition of LMWH to aspirin did not influence fetal growth, nor did it influence uterine artery or umbilical artery flow velocity [21].
Other researchers conducted a retrospective study between January 2005 and July 2010 on 64 patients using low-dose LMWH (Enoxaparine 40 mg) from the beginning of pregnancy until 36 weeks of gestation. Their aim was to investigate women with thrombophilia who used LMWH during the 18-22-week period of gestation in comparison to a control group. They found that LMWH did not influence uterine artery or umbilical artery flow velocity [22].
These studies investigated only patients with thrombophilia who have decreased fibrinolytic activity, which leads to a reduction of the trophoblast’s ability to invade the endometrium and thus compromise successful placentation. The underlying hypothesis is that thrombophilia mediated by the physiologic hyperestrogenemia of pregnancy synergistic with a genetic thrombophilia pattern promotes thrombus formation in the spiral arteries of the placenta resulting in placental insufficiency and increased pregnancy complications [23].
LMWH may have favorable effects through pathways that have nothing to do with anti-coagulation. Unfractionated heparin and LMWH promote the differentiation and invasion of extravillous trophoblast cells [24, 25] and decrease vascular resistance [26, 27, 28]. It has been reported that LMWH is associated with increased heparin-binding epidermal growth factor (HBEGF) protein expression and secretion [24, 29]. HBEGF is a member of the epidermal growth factor (EGF) family, which includes proteins that bind to tyrosine kinase receptors of the human EGF receptor (ERBB) family [30]. HBEGF specifically binds to ERBB1 and ERBB4, but is capable of activating ERBB2 through receptor transactivation [31]. Heparin is a cofactor for proteins with heparin-binding domains, including HBEGF [30]. In addition to HBEGF, heparin is required as a cofactor for fibroblast growth factor (FGF) 4 in the maintenance of rodent trophoblast stem cells [32]. In humans, cytotrophoblasts (CTBs) proliferate in response to heparin and FGF treatment [33]. These studies demonstrated that heparin can activate numerous signaling pathways that could influence trophoblast survival and function.
HBEGF contributes to trophoblast survival and extravillous differentiation
during early pregnancy and is dysregulated in placental insufficiencies [24, 34, 35, 36]. HBEGF is secreted from trophoblast cells of the human blastocyst [37].
HBGEF induces trophoblast extravillous differentiation [38], regulates
endometrial stromal cell motility at the implantation site [39] and provides
cytoprotection in an adverse environment [40]. Inhibition of HBEGF signaling by a
specific antagonist or by inhibiting ERBB receptors, abrogates its cytoprotective
function, as does removal of its cofactor heparan sulfate from the cell surface
[41]. HBEGF expression is significantly reduced in all trophoblast populations of
placentas from women with preeclampsia [36], supporting a contribution of this
deficiency to the associated cell death and poor invasion of those cells. LMWH
induces a significant increase in HBEGF protein expression and secretionand
reduces TNF-
It is unclear which of these attributes, if any, are key to improving pregnancy outcomes in women with placental insufficiency.
Multiple trials and systematic reviews have concluded that LMWH reduces the incidence of recurrent severe preeclampsia in high-risk women, as well as perinatal mortality, preterm birth, and increased infant birth weight [42, 43].
Despite the fact that we did not find statistically significant differences in fetal growth, fetal cerebral flow velocities, pre-eclampsia, IUGR or preterm labor, there remains a benefit of adding LMWH to protect the fetus against diminished cerebral blood flow in this specific population as we had only abnormal cases of diminished cerebral blood flow in the group treated with aspirin which implies that the combination treatment of LMWH and aspirin reduced the risk of occurrence of hypoxic ischemic encephalopathy.
Our results might be promising but our sample was small which made our study under-powered with a low probability of detecting an effect of practical importance. It should act as evidence for a second study to be performed with bigger sample size.
This study has focused on flow velocities of the uterine arteries and umbilical artery in a population with a history of placental vascular complication in a previous pregnancy. We found that treatment with LMWH influenced uterine artery and umbilical Doppler measurements and the amount of amniotic fluid during the third trimester and reduced the risk of occurrence of hypoxic ischemic encephalopathy in the new born.
EAAEF: designed, performed the research and wrote the manuscript.
The study was approved by Alexandria faculty of medicine ethics committee, trial registeration number 00298/2018, date of registeration 25th of January 2018. Informed Consent was signed by all participants.
Special thanks to doctor El- sayed Amr for his cooperation in statistics, and to nursing staff of the Antenatal care clinic of El- shatby hospital.
This research received no external funding.
The authors declare no conflict of interest.