








 , Li Li 2,†, Xue-Qian Du 3, Ying Wang 1, Shuai Chen 1, Gui-Lian Li 2, Gui-Fang Li 1,*
, Li Li 2,†, Xue-Qian Du 3, Ying Wang 1, Shuai Chen 1, Gui-Lian Li 2, Gui-Fang Li 1,*1 Department of Neonatology, Cangzhou People’s Hospital, 061000 Cangzhou, Hebei, China
2 Department of Obstetrics, Cangzhou People’s Hospital, 061000 Cangzhou, Hebei, China
3 Department of Ultrasonography, Cangzhou People’s Hospital, 061000 Cangzhou, Hebei, China
† These authors contributed equally.
Abstract
This study aims to provide the cerebellar extrauterine reference value related
to gestational age by analysing the neonatal cerebellum development with
different gestational age, by means of cranial ultrasound. A total of 376
eligible cranial ultrasound images of neonates with gestational age of 25 to 41
weeks were selected. Transverse cerebellar diameter, vermis height, vermis
diameter, vermis circumference, vermis area and vermis eccentricity ratio were
measured and followed by statistical analysis. Transverse cerebellar diameter
formed a linear equation with the gestational age, which was Y = 0.104X + 0.176,
R
Keywords
- Cerebellum
- Cranial ultrasound
- Neonatal infants
- Gestational age
The cerebellum is a part of the brain, located in the posterior cranial fossa. The upper, middle and lower pairs of the cerebellum are connected with the posterior brain stem, and the upper part of the cerebellum is separated from the brain by the cleft of the brain and the cerebellum. The enlarged part on both sides of the cerebellum is the cerebellar hemisphere, and the narrow part in the middle is the cerebellar earthworm [1]. Most of the cerebellar hemispheres are specific to higher mammals. The position of the cerebellum in the cranial cavity determines its rich afferent and efferent connections with the vestibule, spinal cord, and cerebral cortex. It is one of the body’s energetic body movement regulation centers, like a regulator in the human body, and participates in maintaining the body balance, regulating muscle tension, and coordinating voluntary movements [2, 3, 4].
The growth and development of the cerebellum take a long time, from early embryonic development to the first few years after birth, which make the cerebellum more susceptible to adverse factors and developmental abnormalities [5]. Lateral diameter of cerebellum and cerebellar vermiculate is one of the parameters of morphological evaluation of cerebellum, which is useful in monitoring the growth and development of the cerebellum in newborns.
Regarding the complete measurement of cerebellar intrauterine growth and development in neonates of different gestational ages, no research report had been declared in China. The purpose of this study is to determine the relationship between the gestational age and the cerebellar transverse diameter and cerebellar vermis compartment at birth, which is helpful in understanding the growth and development of the neonatal cerebellum, and providing relevant reference values for the clinic.
Ultrasonographic images of craniocerebral brains on the day of birth of 376 newborns with gestational age of 25 to 41 weeks were selected. The inclusion criteria of the research subject were the infants who were born from January 2014 to December 2019, both were appropriate-for-gestational-age children, no congenital abnormal brain development, no abnormalities in appearance and abnormalities of the central nervous system. Besides that, the ultrasonographic images which met the cerebellum measurement requirements were selected for measurement. This study was approved by the ethical committee of Cangzhou People’s Hospital (No. 20190611). Besides, the informed consents of newborn parents were obtained before the study.
The gestational age was calculated from the mother’s last menstrual period and corrected using ultrasound data from the first trimester. A total of 376 neonates were divided into 17 groups according to gestational age which were shown in Table 1.
| Group | |||||||||||||||||
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | |
| GA (week) | 25 | 26 | 27 | 28 | 29 | 30 | 31 | 32 | 33 | 34 | 35 | 36 | 37 | 38 | 39 | 40 | 41 |
| n | 12 | 18 | 20 | 19 | 22 | 25 | 25 | 26 | 32 | 30 | 22 | 23 | 23 | 21 | 23 | 21 | 14 |
| n, sample number. | |||||||||||||||||
The subjects were all in a quiet state, and received a bedside craniocerebral ultrasound examination, using a Philips iu Elite ultrasound diagnostic instrument, a C8-5 neonatal cranial brain probe, with a frequency of 5 to 8 MHz by taking a sagittal plane scan and adjust the probe to obtain a standard median sagittal section to fully display the cerebellar vermiform section. A coronal plane scan was adjusted the probe to obtain a standard cerebellar transverse diameter section. The best images were frozen and saved. All pictures and text data were input into the PACS system.
Two physicians, who were familiar with ultrasound diagnosis of newborns, delineated and measured the acquired images, and measured the cerebellar transverse diameter (the maximum distance from the outer edge to the outer edge of the cerebellar transverse diameter on a coronal section, Fig. 1A), vermis height (the maximum distance between the highest point of the upper vermis of the cerebellum and the lowest point of the lower vermis, Fig. 1B), vermis diameter (the distance from the apex of the fourth ventricle to the posterior vermis of the cerebellum, Fig. 1C), vermis circumference and vermis area (a mid-sagittal section of the vermis of the cerebellum is drawn by hand, Fig. 1D). Through digital image processing algorithms of cerebellar vermis ultrasound image (Fig. 2A) after processing, the cerebellar vermis area (Fig. 2B), cerebellar vermis contour edge points were obtained after further processing (Fig. 2C), the edge points using the least-squares ellipse fitting method for ellipse fitting method (Fig. 2D) [6]. Finally, the elliptical eccentricity was calculated by including e for cerebellar vermis eccentricity, a short half shaft for ellipse fitting, b for the semi-major axis of ellipse fitting.
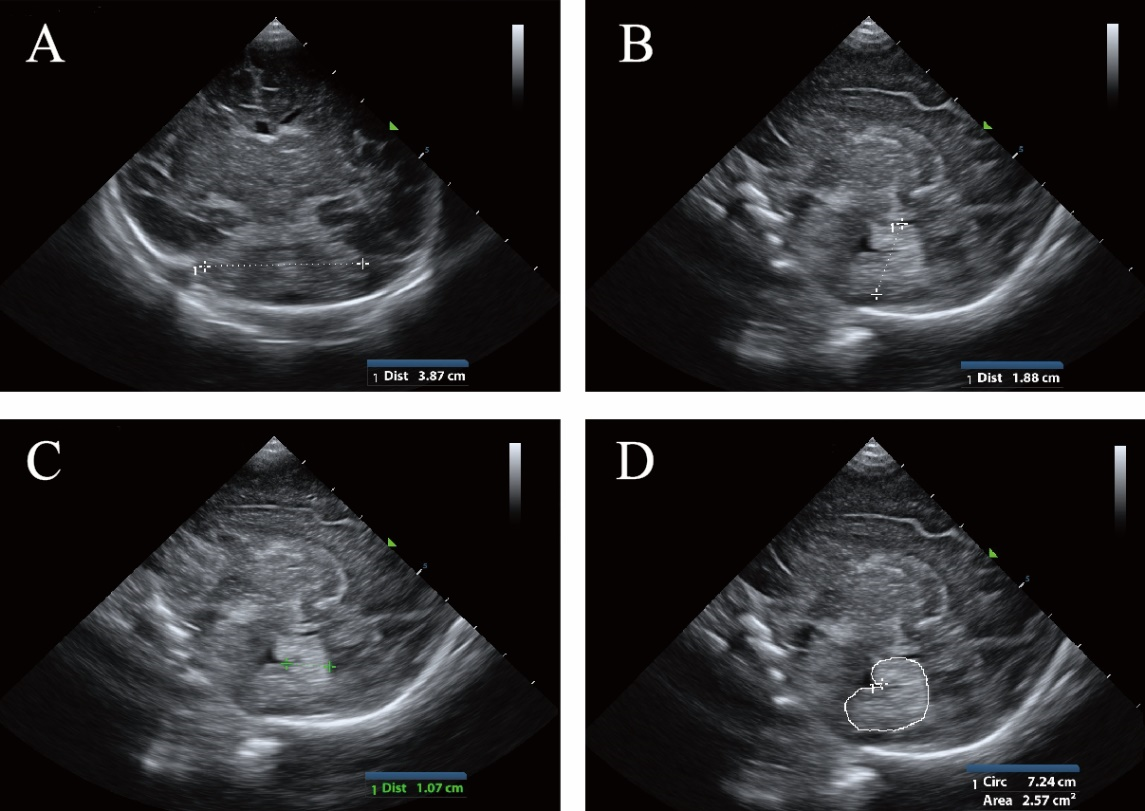 Fig. 1.
Fig. 1.The measurement of (A) transverse cerebellar diameter; (B) vermis height; (C) vermis diameter; (D) vermis circumference and vermis area using ultrasound examination.
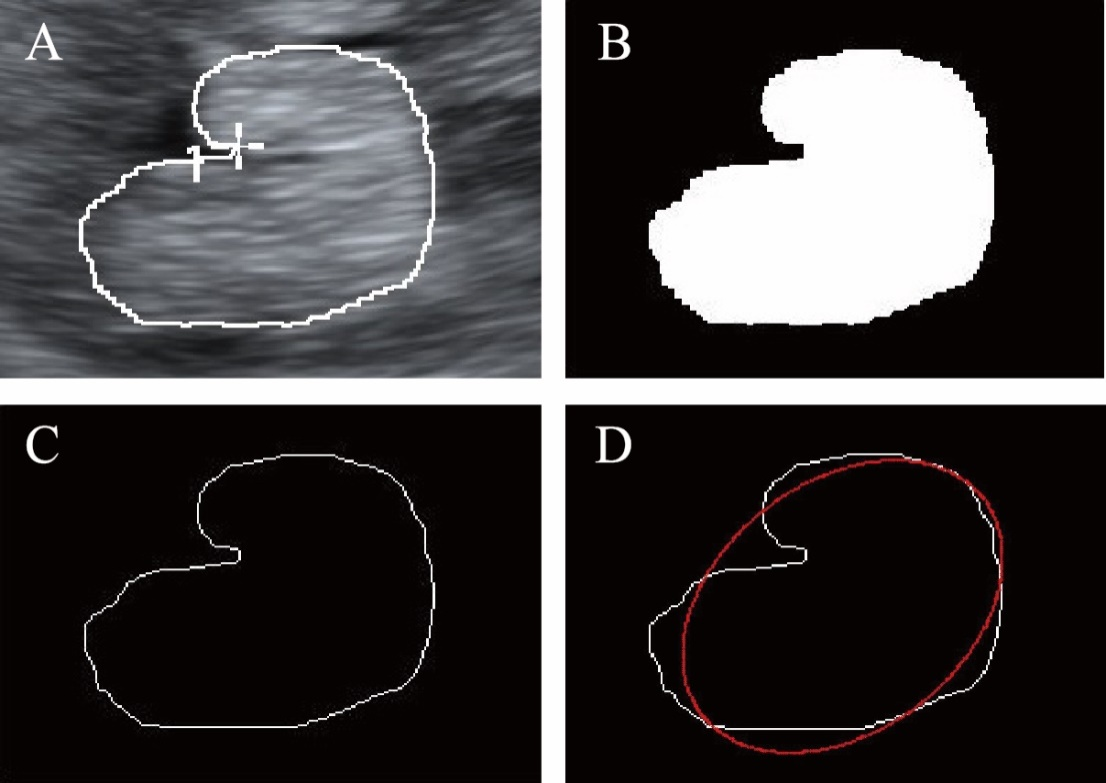 Fig. 2.
Fig. 2.The measurement of vermis eccentricity ratio.
Two physicians made two measurements at different times, and all measurements were tested for inter-group and intra-group repeatability, and the average value of the four valid measurements was taken.
SPSS 22.0 and Microsoft Excel 2017 were used for statistical processing and
analysis. All measured data were expressed as mean
The paired sample t-test was utilized to test the repeatability between and
within groups. The results showed that P
As shown in Table 2, the cerebellar transverse cerebellar diameter, vermis height, vermis diameter, vermis circumference, vermis area were all increased with gestational age. However, the vermis eccentricity ratio showed a reduction as the gestational age increased.
| Group | GA (week) | n | Transverse cerebellar diameter (cm) | Vermis height (cm) | Vermis diameter (cm) | Vermis circumference (cm) | Vermis area (cm |
Vermis eccentricity ratio |
| 1 | 25 | 12 | 2.79 |
1.41 |
0.72 |
4.95 |
1.43 |
0.68 |
| 2 | 26 | 18 | 2.82 |
1.46 |
0.77 |
5.73 |
1.71 |
0.59 |
| 3 | 27 | 20 | 2.88 |
1.52 |
0.78 |
6.19 |
1.88 |
0.61 |
| 4 | 28 | 19 | 3.08 |
1.58 |
0.82 |
6.46 |
2.00 |
0.61 |
| 5 | 29 | 22 | 3.14 |
1.68 |
0.85 |
6.61 |
2.11 |
0.60 |
| 6 | 30 | 25 | 3.33 |
1.73 |
0.93 |
6.73 |
2.25 |
0.59 |
| 7 | 31 | 25 | 3.39 |
1.88 |
0.97 |
7.05 |
2.46 |
0.65 |
| 8 | 32 | 26 | 3.49 |
1.86 |
1.01 |
7.21 |
2.55 |
0.59 |
| 9 | 33 | 32 | 3.65 |
1.98 |
1.10 |
7.59 |
2.89 |
0.58 |
| 10 | 34 | 30 | 3.75 |
2.06 |
1.17 |
8.03 |
3.33 |
0.56 |
| 11 | 35 | 22 | 3.80 |
2.17 |
1.23 |
8.45 |
3.64 |
0.58 |
| 12 | 36 | 23 | 3.91 |
2.16 |
1.21 |
8.33 |
3.59 |
0.53 |
| 13 | 37 | 23 | 3.98 |
2.20 |
1.31 |
8.51 |
3.94 |
0.52 |
| 14 | 38 | 21 | 4.12 |
2.25 |
1.33 |
9.08 |
4.26 |
0.51 |
| 15 | 39 | 23 | 4.19 |
2.35 |
1.38 |
9.35 |
4.51 |
0.49 |
| 16 | 40 | 21 | 4.32 |
2.43 |
1.46 |
9.81 |
4.85 |
0.50 |
| 17 | 41 | 14 | 4.33 |
2.54 |
1.54 |
10.07 |
4.95 |
0.45 |
| GA, gestational age; n, sample number. | ||||||||
Transverse cerebellar diameter increased linearly with increasing gestational
age. As shown in Fig. 3, Pearson correlation analysis showed a positive linear
correlation between cerebellar transverse diameter and gestational age, r = 0.857,
P
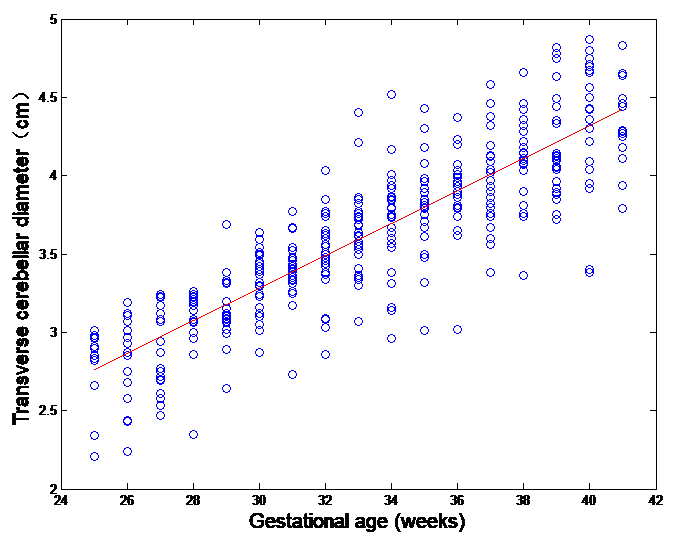 Fig. 3.
Fig. 3.The scatter plot of transverse cerebellar diameter and gestational age.
As shown in Fig. 4, vermis height increased linearly with increasing
gestational age. Pearson correlation analysis showed a positive linear
correlation between vermis height and gestational age, r = 0.908, P
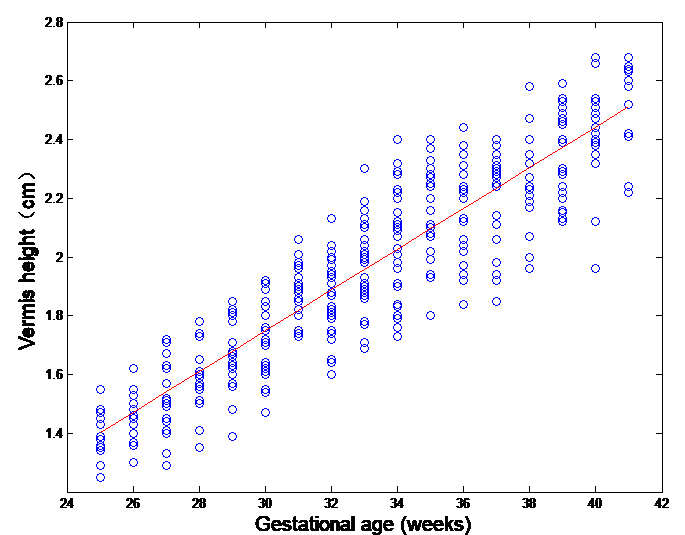 Fig. 4.
Fig. 4.The scatter plot of vermis height and gestational age.
As shown in Fig. 5, the vermis diameter increased linearly with increasing
gestational age. Pearson correlation analysis showed that the vermis diameter had
a linear positive correlation with gestational age, r = 0.866, P
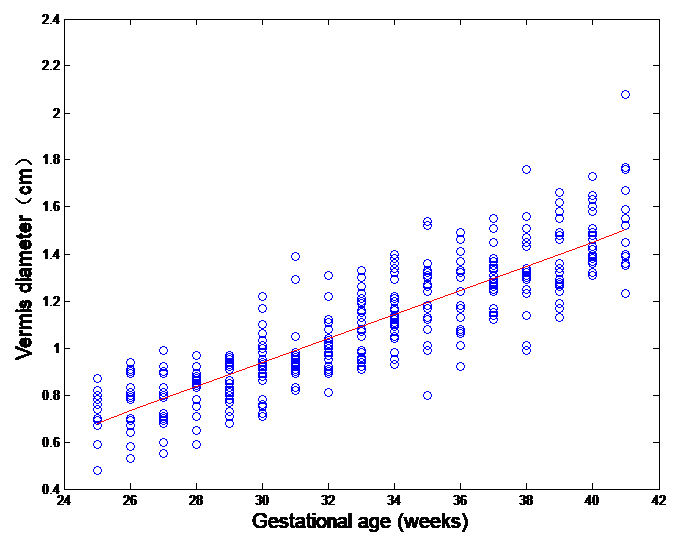 Fig. 5.
Fig. 5.The scatter plot of vermis diameter and gestational age.
As shown in Fig. 6, the vermis circumference increased linearly with the
increase of gestational age. Pearson correlation analysis showed a positive
linear correlation between the vermis circumference and gestational age, r = 0.888,
P
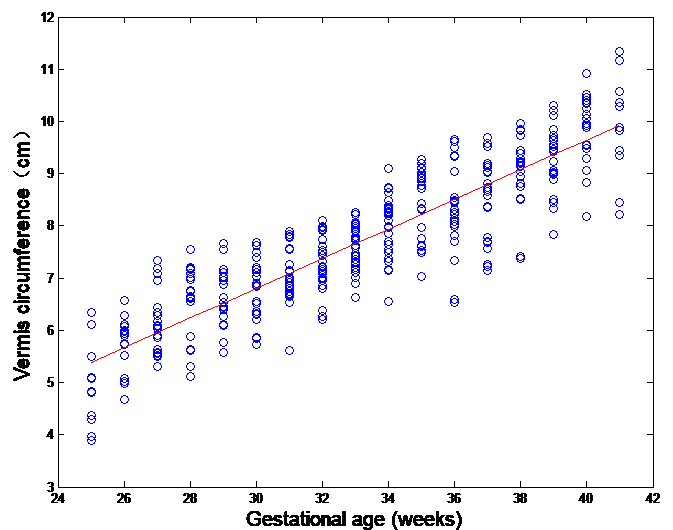 Fig. 6.
Fig. 6.The scatter plot of vermis circumference and gestational age.
As shown in Fig. 7, the vermis area increased linearly with the increase in
gestational age. Pearson correlation analysis showed a linear positive
correlation between the vermis area and gestational age, r = 0.905, P
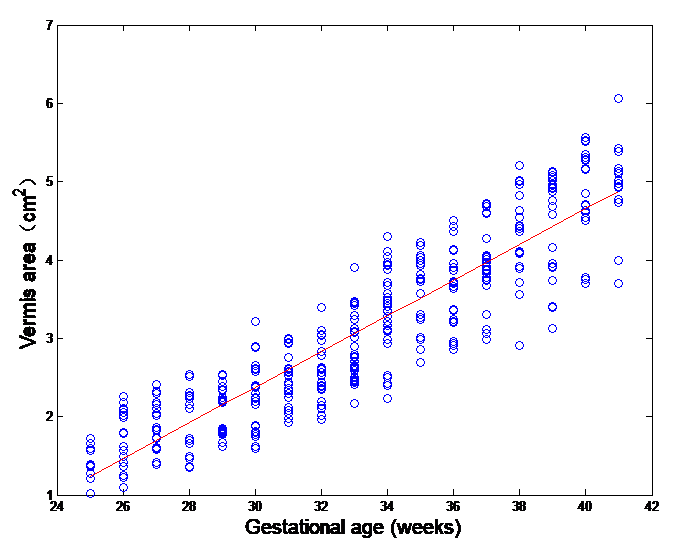 Fig. 7.
Fig. 7.The scatter plot of vermis area and gestational age.
As shown in Fig. 8, the vermis eccentricity ratio decreased linearly with the
increase in gestational age. Pearson correlation analysis showed a linear
negative correlation between the vermis eccentricity ratio and gestational age,
r = -0.376, P
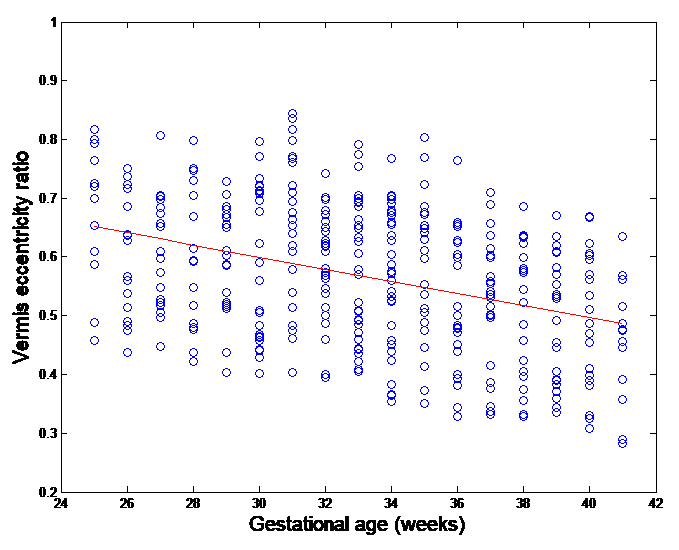 Fig. 8.
Fig. 8.The scatter plot of vermis eccentricity ratio and gestational age.
The cerebellum originates after 6 weeks of gestation and develops earlier than most intracranial brain structures, with relatively stable growth and development. The growth and development of the cerebellum have accelerated since the second trimester of pregnancy, and the growth and development are basically completed to 18 months after birth. During this period of growth and development, the cerebellum is one of the fastest growing brain structures in the brain [7, 8]. Due to the early growth of the cerebellum, rapid growth and development, and the long duration of growth and development, the cerebellum is susceptible to adverse factors in the neonatal period, especially the cerebellum of premature infants [5, 9]. The cerebellum is in a vulnerable state before and after birth. The reason may be linked to the more active proliferation and migration of cerebellar granule cells during this period [10], where granule cells are glutamate-exciting neurons [1]. The abnormal growth and development of the cerebellum during the neonatal period will affect the development of the nervous system [11]. Monitoring the development of the cerebellum can be used as an evaluation index of neuronal proliferation and migration disorders [10]. The cerebellum participates in the cognitive process, coordinates voluntary movements. Thus, the bedside cranial brain ultrasound was assessed to measure the growth and development of the cerebellum conveniently, dynamically and accurately throughout the growth and development cycle of the newborns. This is helpful for early clinical assessment of cerebellar development. This study used craniocerebral ultrasound technology to provide a complete ultrasound measurement of the cerebellar transverse diameter, cerebellar vermiform height, cerebellar vermiform diameter, cerebellar vermiform perimeter, cerebellar vermiform area, and vermis eccentricity ratio from 25 to 41 weeks of gestational age.
The cerebellum has some quantifiable indicators such as the lateral diameter of the cerebellum, the height of the cerebellar vermicompost, the perimeter of the cerebellar vermicompost, the area of the cerebellar vermicompost, and the area of the cerebellar vermicompost. Large-scale studies of cerebellar growth and development at birth are currently under-reported. This study clarified the research site of each measurement index, further clarified the measured values of relevant indicators suitable for gestational age of cerebellar growth and development in gestational age 25 to 41 weeks, including the cerebellar transverse diameter, cerebellar vermicular height, and anterior-posterior diameter, perimeter of cerebellar vermicompost, area of cerebellar vermicompost and vermis eccentricity ratio. Following consideration of the ease of operation, time-saving, and practicality of bedside cranial brain ultrasound on the day of birth clinically, the index of cerebellar vermiform height could be selected for clinical analysis and quantitative analysis. The height of the facet to assess the growth and development of the medial cerebellum. In fetal craniocerebral ultrasonography, even in situations where the double parietal diameter cannot be accurately displayed, such as fetal breech position, uterine abnormality, intrauterine growth restriction, or oligohydramnios, etc., fetal could be evaluated by measuring the lateral diameter of the cerebellum age and fetal brain development, it could be seen that the index of the cerebellar transverse diameter was more accurate than the cerebellar vermiform height to reflect the abnormal development of the cerebellum [12]. Measuring the cerebellar transverse diameter and cerebellar vermiform height simultaneously is helpful for evaluating the growth and development of the lateral and medial regions of the cerebellum, and it is also conducive to clinically assess the growth and development of the cerebellum.
A study had included the cerebellar transverse diameter while measuring the height of the cerebellar vermiform [13]. This study measured the lateral cerebellar diameter and cerebellar vermiform height of 321 gestational age children from 26 weeks to 42 weeks. A nomogram of these two indicators and gestational age was constructed. The purpose of this study was to fully evaluate the extrauterine cerebellar development suitable for gestational age children, so the cerebellar transverse diameter, cerebellar vermiform height, cerebellar vermiform anteroposterior diameter, cerebellar vermiform perimeter, and cerebellar vermiform area were measured and analysed simultaneously. 318 cases with gestational age from 25 to 41 weeks under research conditions were suitable as the research object, and the cerebellar indexes were measured. The results showed that there was a positive correlation between each index and gestational age, and all of them increased linearly with gestational age. Cerebellar vermis eccentricity ratio was negatively correlated with gestational age, along with the linear decrease in gestational age. Thus, the increase of gestational age and the appearance of cerebellar vermis looked more similar to a circle. On the other hand, along with the gestational age decreases, cerebellar vermis looked closer to the oval shape, namely the full term of cerebellar vermis shape relative to the premature infant, tend to round. Among them, the measured values of the lateral diameter of the extrauterine cerebellum and the height of the cerebellar vermiform were consistent with the findings of Imamoglu’s studies [14]. The first large sample of this study in China reported the correlation between ectopic growth of the cerebellum and gestational age suitable for gestational age, providing cerebellar transverse diameter, cerebellar vermiform diameter, anterior and posterior diameter of cerebellar vermiform, cerebellar vermiform perimeter, and cerebellar vermiform. The extrauterine reference value of the area of the body, the scatter plot of the various indexes of the cerebellum, and the gestational age were helpful for the early detection of abnormal changes in the growth and development of the cerebellum.
No domestic reports on the index of the extrauterine cerebellar transverse diameter and the height of the cerebellar vermiform had been included in the study. Chen’s study had used ultrasound to study 196 cases of fetal cerebellar vermiforms at gestational age of 35 to 42 weeks [15]. The results showed that the cerebellar vermicular diameter (height), anterior and posterior diameter, transverse diameter, perimeter, and area increased with gestational age. Tong’s group conducted a retrospective study using craniocerebral MRI and provided a normal reference range of 856 fetal cerebellar vermiform development from 23 to 40 weeks [16]. The purpose of this study was to further study the neonatal cerebellar extrauterine growth and development based on fetal cerebellum research. When comparing the data of the anterior and posterior diameter of the cerebellar vermiform and the area of the cerebellar vermiform with Tong’s group, it was found that the measured value was almost 0.8 to 0.9 times the measured value of Tong’s group [16]. The reason may be related to intrauterine and extrauterine brain ultrasound measurement technology, which needs further research to support it.
The significance of this study was to use the craniocerebral ultrasound technology to monitor and follow up various indicators of the cerebellum, especially the transverse cerebellar diameter and the vermis height, as a part of the routine bedside cranial ultrasound examination. Nomograms of the distribution curve of cerebellar index against gestational age at birth in AGA neonates had been constructed. This could help us establish normal control data and help the neonatologist to assess variations from the normal during ongoing cerebellar growth and development and to diagnose cerebellar anomalies. Cerebellar development continues after birth. During this period, some newborns may experience cerebellar development problems. Especially for premature babies, most of the cerebellar development took place in the extrauterine environment. Among them, the problems of extrauterine living environment such as breathing problems, infection problems and nutrition problems would affect the development of the cerebellum. Further studies evaluating the cerebellar growth of premature infants with a smaller gestational age and long-term neurocognitive outcomes are warranted. The sample size of gestational age-appropriate infants included in this study at smaller gestational age remained relatively small. The study is still in its infancy and its results are still preliminary. Since we did not follow up our cases with cranial sonography, this possibility was not assessed, which is a limitation of our study.
In our future studies, changes in cerebellar indicators can be monitored weekly to dynamically observe the relationship with the changes of cerebellar indicators and the outcome of neuromotor development in premature infants.
RL and GL initiated and designed the study. GL and SC supervised the study. LL, XD and GL participated in data collection. RL, YW and XD evaluated the cranial ultrasound images. All authors participated in data interpretation and contributed to drafting and revising the manuscript. All authors approved the final version published.
This study was approved by the ethical committee of Cangzhou People’s Hospital (20190611). Besides, the informed consents of newborn parents were obtained before the study.
We would like to express my gratitude to all those who helped me during the writing of this manuscript.
The project is supported by the Foundation of Health Commission of Hebei Province (Correlation between cerebellar development and neuromotor development in premature infants) (Grant No. 20200173) China.
The authors declare no conflict of interest.