




 , K.S. Lee 2,†,*
, K.S. Lee 2,†,*1 Department of Obstetrics and Gynecology, Samsung Changwon Hospital, Sungkyunkwan University School of Medicine, Changwon, Republic of Korea
2 Department of Obstetrics and Gynecology, Pusan National University School of Medicine, Busan 49241, Republic of Korea
3 Infertility Institute, Pohang Women’s Hospital, Pohang 37754, Republic of Korea
†Contributed equally.
Abstract
Purpose of Investigation: This study investigated whether cryopreservation of mouse and human blastocysts using vitrification solutions formulated with or without sucrose and Ficoll affects survival rate and pregnancy outcome. Materials and Methods: Two-cell mouse embryos were retrieved from C57BL/CBA females aged 5 weeks and cultured to the blastocyst stage. Artificial shrinkage of blastocysts was performed by blastocoel fluid aspiration before vitrification and then exposed to and vitrified-warmed in one of four different vitrification solutions: 1) 25% glycerol, 25% ethylene glycol, 20% SSS and PBS without sucrose and Ficoll (G25E25), 2) G25E25 with 0.5 M sucrose (G25E25S0.5), 3) G25E25 with 10 mg/mL Ficoll (G25E25F10), and 4) G25E25 with 0.5 M sucrose and 10mg/mL Ficoll (G25E25S0.5F10). Second, in 435 infertile women undergoing in vitro fertilization and embryo transfer (IVF-ET), artificially shrunken blastocysts were vitrified-warmed either in G25E25 (n = 206) and G25E25S0.5F10 (n = 229). Results: In the mouse series, in vitro survival rates of post-warm blastocysts were 93, 91, 90, and 90% in G25E25, G25E25S0.5, G25E25F10, and G25E25S0.5F10, respectively. No significant differences among four groups were found. In the human series, in vitro survival rates and clinical pregnancy rate of blastocysts vitrified-warmed in G25E25 were 96 and 53.3%, respectively, which were similar to those in G25E25S0.5F10 (92 and 51.9%, respectively). Conclusions: Sucrose- and Ficoll-free vitrification solutions can be successfully cryopreserved mouse and human blastocysts without compromising survival rate and pregnancy outcome.
Keywords
- Blastocyst
- Vitrification
- Sucrose
- Ficoll
- Survival
- Pregnancy outcome
Advances in embryo culture techniques used in assisted reproduction technology (ART) have shown that blastocyst transfer can be used as an alternative to cleavage stage embryo transfer [1, 2]. Blastocyst transfer has some theoretical advantages including both an improvement of uterine and embryonic synchronicity and self-selection of a viable embryo, thus resulting in better pregnancy and implantation rates as well as preventing the occurrence of multiple pregnancies [3]. In addition, advances in cryopreservation techniques such as the development of the vitrification method have resulted in improved survival rate of frozen embryos [4, 5] and increased frequency of blastocyst transfer [6].
The vitrification method was introduced by Fahy et al. in 1984 [7] and is defined as a cryopreservation method that leads glass-like solidification by dehydrating the intracellular fluid using high initial concentrations of cryoprotectants that are sufficient to prevent ice crystal formation [8]. As a result, it can overcome the critical drawback of the conventional slow-freezing method, which can cause cellular damage by intracellular ice crystal formation [9].
Vitrification solutions contain both permeating and nonpermeating cryoprotective agents [10]. Permeating cryoprotectants are added to prevent the injury caused by intracellular ice formation. Common choices of permeating cryoprotective agents include; dimethylsulphoxide (DMSO), actamide, propylene glycol, glycerol, and ethylene glycol (EG). However, if these substances reach too high concentration within the cell they can, in themselves, cause cellular damage. To help prevent the permeating agents reaching such high toxic intracellular concentrations, non-permeating agents are also added to vitrification solutions. The large macromolecule Ficoll and the saccharide sucrose are examples of such commonly used non-permeating agents. Ficoll increases the osmolarity and viscosity of the solution, thereby helping to reduce ice crystal formation [11]. Sucrose, which also exerts high osmotic activity, causes cellular dehydration by osmosis and thus further aids intracellular vitrification. Therefore, the addition of nonpermeating agents to vitrification solutions reduces final concentration of intracellular permeating cryoprotectants, while concomitantly reducing their cellular toxicity [11].
Vitrification solutions, such as those described above, were originally formulated for cryopreservation of cleavage stage embryos. However, unlike cleavage-stage embryos, blastocyst stage embryos have large amounts of water-based fluid in the blastocoel cavity. In this respect, the most critical factor in the successful cryopreservation of blastocyst is the complete dehydration of blastocoel fluid and residual solution, thereby preventing ice crystal formation. Accordingly, some studies have reported that the clinical outcome decreases as blastocoel volume increases [12, 13]. For this reason, the blastocoel fluid of blastocysts is usually aspirated cavity prior to vitrification (referred to as artificial shrinkage) in order to completely dehydrate blastocoel fluid, thereby preventing ice crystal formation [14, 15, 16]. As blastocysts pretreated in this manner already have low blastocoel volume, we speculated that they may have no longer benefit from the further dehydrating effects of Ficoll and sucrose additives in the vitrification solution. Hence, this study investigated whether cryopreservation of mouse and human blastocysts using vitrification solutions formulated with or without sucrose and Ficoll affects survival rate and pregnancy outcome.
This study was approved by the institutional review board of Pusan National University Hospital, Korea (IRB No.: E2016024F). All animal experiments were conducted under the guidance for the Care and Use of Laboratory Animals of the National Institutes of Health, approved by the Pusan National University Hospital Institutional Animal Care and Use Committee (PNUH-2017-115).
C57BL/CBA female and male mice were purchased from the Koatech Inc. (Gyunggi-do, Korea) and housed in an animal facility under controlled conditions (22 ± 1 °C temperature, and a daily 12-hour light/12-hour dark cycle) and were fed a commercial chow diet and tap water ad libitum.
C57BL/CBA female mice aged 5 weeks were superovulated by the intraperitoneal injection with 0.1 mL of 5 IU pregnant mare’s serum gonadotropin (PMSG; Sigma, St. Louis, MO, USA) followed by injection of 5 IU of human chorionic gonadotropin (hCG; Sigma) 48 hours later. The mice were then immediately paired with an 8- to 12-week-old individual male. The following morning the mice were inspected, and those with a confirmed vaginal plug were considered fertilized. Forty-eight hours after hCG injection, the mice were sacrificed by central dislocation. Two-cell embryos were extracted from the isthmic portion of the salpinx, washed with Dulbecco’s phosphate-buffered saline (D-PBS) three times, and then cultured in 20 μL drops of Gl-plus medium (Vitrolife, V. Frolunda, Sweden) for the first 1 days, and G2-plus medium (Vitrolife) for the latter 2 days under mineral-oil (SAGE, Origio, Denmark) at 37 ºC in a 5% CO2 incubator. Te media were changed daily.
Artificial shrinkage of blastocysts was performed using intracytoplasmic sperm injection (ICSI) pipette (Vitrolife) as follows: the blastocyst was held with a holding pipette (Vitrolife) so that inner cell mass (ICM) was placed at the 6 or 12 o’clock position. And then, the ICSI pipette was pierced through the trophectoderm cells into the blastocoele cavity, and about 70% to 80% of blastocoele fluid was aspirated (Figure 1).
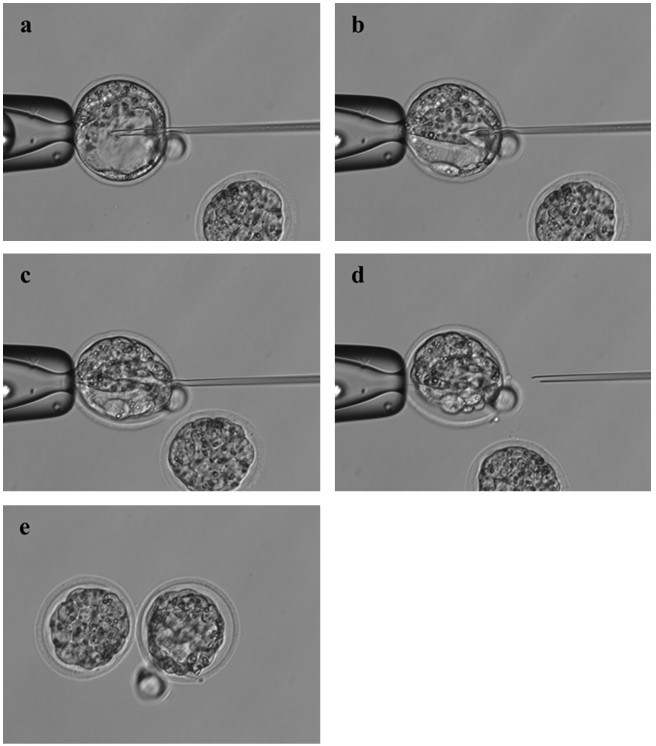 Figure 1.
Figure 1.— Artificial shrinkage (AS) of Mouse expanded blastocyst with an intracytoplasmic sperm injection (ICSI) pipette. (a) A Mouse expanded blastocyst was immobilized with a holding Micropipette connected to Micromanipulation. Inner cell Mass (ICM) was located in the 6 or 12 o’clock position. (b) The ICSI pipette was slowly inserted into the blastocoele at the 3 o’clock position. (c) The blastocoele fluid was aspirated completely, resulting in shrinkage of blastocoeles. (d)Micro-injection pipette was slowly removed from blastocoeles. (e) A Mouse expanded blastocyst was completely shrunken. Magnification is ×200.
All solutions and pre-treatment steps described below were performed at room temperature. The shrunken blastocysts were placed in equilibration solution I (G10) and II (G10E20) for one minute. Solution G10 consisted of 10% glycerol, 20% synthetic serum substitute (SSS) and phosphate-buffered saline (PBS), and solution G10E20 consisted of 10% glycerol, 25% ethylene glycol, 20% SSS and PBS. Following this treatment, the equilibrated blastocysts were transferred into one of four different vitrification solutions with and without sucrose and Ficoll for about 10 seconds. The four different vitrification solutions were composed as follows: 1) 25% glycerol, 25% ethylene glycol, 20% SSS and PBS (G25E25, sucrose- and Ficoll-free), 2) G25E25 with 0.5M sucrose (G25E25S0.5), 3) G25E25 with 10mg/mL Ficoll (G25E25F10), and 4) G25E25 with 0.5M sucrose and 10mg/mL Ficoll (G25E25S0.5F10). And then the blastocysts were quickly loaded onto cryoloop. Immediately after loading of blastocysts, the cryoloop was plunged into liquid nitrogen.
The warming solution was prepared by adding 0.5M, 0.25M, and 0.125M sucrose to base Medium consisting of PBS and 20% SSS. The cryoloop containing blastocysts was removed from the liquid nitrogen and placed immediately into the 0.5M sucrose solution. After one Minute, blastocysts were sequentially transferred into the 0.25M and 0.125M sucrose solution for one Minute each. Then, blastocysts were washed and kept in the base Medium for 5Minutes and subjected to assisted hatching (AH) with partial zona dissection Method (Figure 2). After AH, blastocysts were further cultured in G2-plusMedium (Vitrolife). About 3-4 hours after warming, the blastocysts were examined on an inverted Microscope at X400 Magnification, and survival was assessed based on the Morphological integrity of the blastomeres, ICM and trophectoderm and re-expansion of the blastocoele. The surviving rates of post-warm blastocysts were calculated as the number of hatching embryos regarded as viable or healthy developing embryos divided by the total number of vitrified blastocysts.
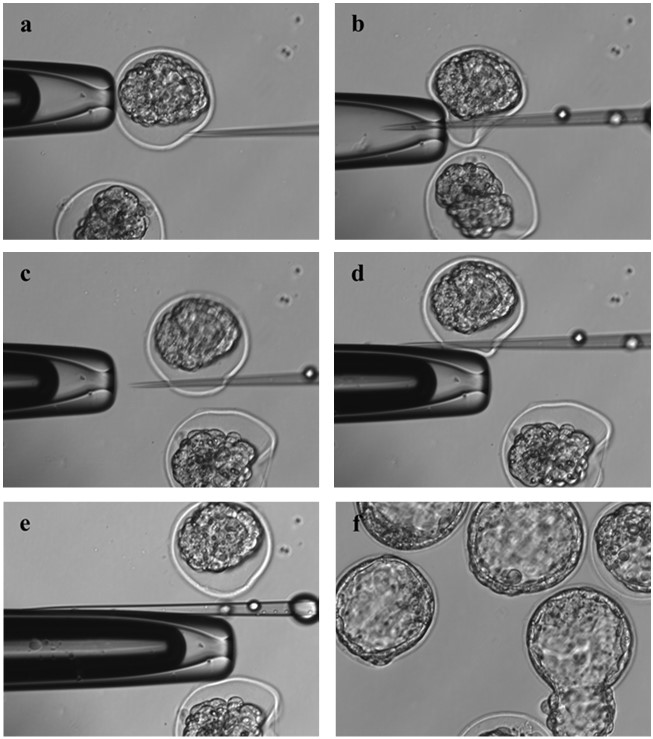 Figure 2.
Figure 2.— Assisted hatching (AH) of vitrified-warmed Mouse blastocyst by partial zona dissection. (a) A vitrified-warmed Mouse blastocyst was held with a holding Micropipette at the 9 o’ clock position, and then intracytoplasmic sperm injection (ICSI) pipette was approached to the perivitel line space (PVS) at about the 4 o’ clock position. (b, c) ICSI pipette was penetrated to the zona pellucia (ZP) through the PVS. (d) The ZP was split by rubbing the ICSI pipette against the edge of the holding pipette. (e) AH was completed by partial zona dissection. (f) An assisted hatched blastocyst was normally expanded and hatched. Magnification is ×200.
The human study was carried out on a total of 442 infertile women who underwent frozen-thawed blastocyst transfer from March 2014 to December 2018 at the infertility Center, Pusan National University Hospital. This was approved by the Institutional Review Board of Pusan National University Hospital (IRB No.: E2016024F) and written informed consents were obtained from patients under the approval of the IRB. For IVF, controlled ovarian stimulation (COS) was applied to infertile women individually using gonadotropin releasing hormone (GnRH) antagonist, Mid luteal long GnRH agonist, ultra-long or ultra-short GnRH agonist protocols. Gonadotropin was treated with recombinant FSH alone (Puregon, MSD, USA or Gonal-F, Merck Serono, Switzerland) or a Mixed protocol with hMG (Menopur, Ferring Pharmaceuticals, Switzerland). The dosages of gonadotropin were decided by age, anti-Müllerian hormone (AMH) and basal FSH levels. The final follicular Maturation was Made with recombinant hCG 250 Mg SC (Ovidrel, Merck Serono, Switzerland) or GnRH agonist 0.2 Mg (Decapeptyl, Ferring Pharmaceuticals, Switzerland), when two or More follicles had reached at Mean diameter of 18 Mm.
Oocytes were retrieved at 36 hours after hCG administration, fertilized, and cultured in 20 μL drops of Gl-plus Medium (Vitrolife) for 48 hours and then in G2-plusMedium (Vitro life) for another 48-72 hours under Mineral-oil (SAGE) in a 37 ºC, 5% CO2 incubator. TeMedia were changed daily. Embryo transfer (ET) was performed at cleavage-stage embryo or blastocyst stage depending on the number and quality of embryos. Only supernumerary embryos were extended to culture in G2-plusMedium and Grade 3BB or better (Gardner and School raft score) blastocysts (17) were selected for vitrification freezing. Before vitrification, blastocysts were subjected with AS by blastocoele fluid aspiration, and then placed in equilibration solution I (G10) and II (G10E20) for one Minute. After equilibration, the shrunken blastocysts were transferred into one of the two different vitrification solutions, G25E25 and G25E25S0.5F10, in the same Manner as previously described for the Mouse study (Figure 3). After about 10 seconds, the blastocysts were quickly loaded onto cryoloop and the cryoloop was immediately plunged into liquid nitrogen.
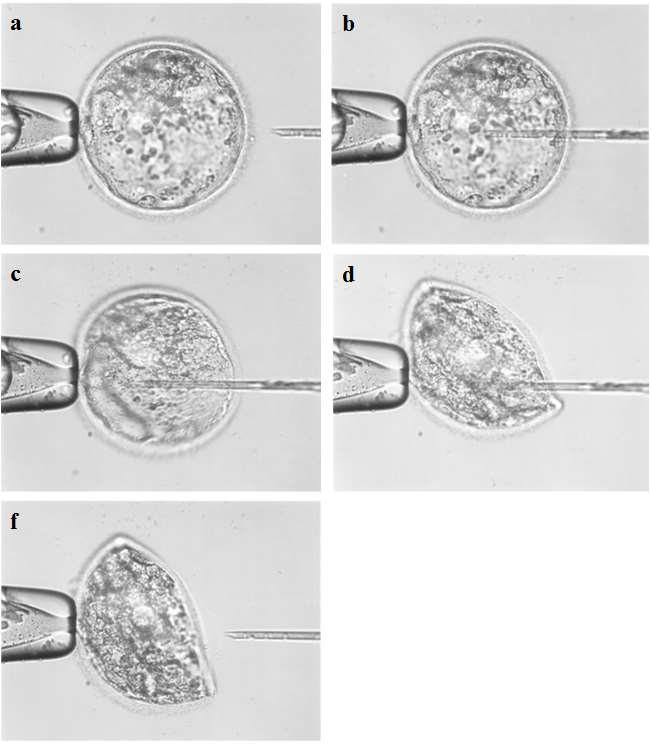 Figure 3.
Figure 3.— Artificial shrinkage (AS) of human expaned blastocyst with intracytoplasmic sperm injection (ICSI) pipette. (a) A human expanded blastocyst was held with a holding Micropipette connected to Micromanipulation. Inner cell Mass (ICM) was located in the 6 or 12 o’clock position. (b) The ICSI pipette was slowly inserted into the blastocoele at the 3 o’clock position. (c) The blastocoele fluid was aspirated completely, resulting in shrinkage of blastocoeles. (d)Micro-injection pipette was slowly removed from blastocoeles. (e) A human expanded blastocyst was completely shrunken. Magnification is ×200.
Among a total of 442 infertile women, 7 women were excluded from this study for the following reasons: women over age 40 (n = 3), poor responders (n = 2) and inappropriate endometrium for implantation (n = 2) with endometrial synechiae, unresponsive thin endometrium or abnormal anatomy of uterine cavity. The remaining 435 women were randomly divided into one of the two test groups; the G25E25 group (n = 206) and the G25E25S0.5F10 group (n = 229).
For endometrium preparation, preliminary GnRH agonist (Lucrin, 0.1 Mg/day; Abbott, USA) was injected for pituitary luteal downregulation at 21 days of last Menstruation. After starting of Menstruation, oral estradiol valerated (Progynova 2-6Mg/day; Bayer Schering Pharma, Germany) was administered to induce the secretory phase of the endometrium. The endometrial thickness (EMT) was evaluated by transvaginal ultrasonography at 15 days of the Menstrual cycle. If EMT was over 7-8 Mm, vaginal progesterone gel (Crinone 90 Mg/day; Merck Serono, Switzerland) was applied daily, if not, oral estradiol valerate was administered continuously until EMT reached 7 Mm.
For zona thinning of blastocysts, the vitrified-warmed blastocysts were subjected to assisted hatching by partial zona dissection using intracy to lasmic sperm injection (ICSI) pipette. The vitrified-warmed blastocyst was held with a holding pipette at the 9 o’clock position and the ICSI pipette was approached to the perivitel line space (PVS) at about the 4 o’ clock position. And then ICSI pipette was penetrated the zona pellucia (ZP) through the PVS at the 4 o’ clock position. The ZP was split by rubbing the ICSI pipette against the edge of the holding pipette (Figure 4). After 3-4 hours of warming, the blastocysts were examined on an inverted Microscope at X200 Magnification, and the survival rate was calculated as the number of expanding embryos regarded as viable or healthy developing embryos divided by the total number of vitrified blastocysts. Healthy viable blastocysts were transferred into the uterus of recipient patients by soft ET catheter (Cook Medical, USA) under guidance of transabdominal ultrasonography.
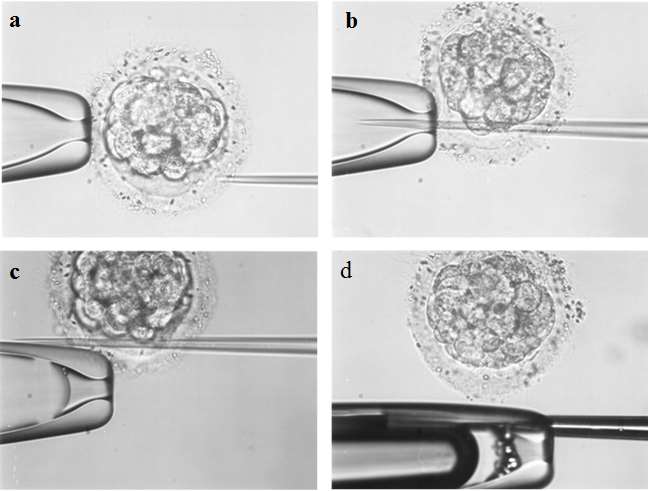 Figure 4.
Figure 4.— Assisted hatching (AH) of vitrified-warmed human blastocyst by partial zona dissection. (a) A vitrified-warmed human blastocyst was held with a holding Micropipette at the 9 o’ clock position, and then intracytoplasmic sperm injection (ICSI) pipette was approached to the perivitel line space (PVS) at about the 4 o’ clock position. (b) ICSI pipette was penetrated to the zona pellucia (ZP) through the PVS. (C) The ZP was split by rubbing the ICSI pipette against the edge of the holding pipette. (d) AH was completed by partial zona dissection. (f) An assisted hatched blastocyst was normally expanded and hatched. Magnification is × 200.
For the purposes of this study successful clinical pregnancy was defined as the visible presence of an intrauterine gestational sac at 6 weeks of gestation. Ongoing pregnancy was defined as the visible presence of fetus with cardiac activity at 10 weeks of gestation.
All data were analyzed by Chi-square test and Fisher’s extract test using the SAS® version 9.3 software (SAS Institute, Cary, NC, USA). The p value < 0.05 was considered statistically significant.
In the Mouse series, each 100 shrunken blastocysts were vitrified in one of four different vitrification solutions; G25E25 (without sucrose and Ficoll), G25E25S0.5 (with sucrose), G25E25F10 (with Ficoll) and G25E25S0.5F10 (with sucrose and Ficoll). After warming, in vitro survival rates of post-warm blastocysts were 93, 91, 90, and 90% in G25E25, G25E25S0.5, G25E25F10, and G25E25S0.5F10, respectively. There was no statistically significant difference among four groups (Table 1).
| Treatments | Number of Blastocysts | p-value | |
|---|---|---|---|
| Vitrified blastocysts | Hatching blastocysts (%) | ||
| G25E25S0.5F30 (Control) | 100 | 90 (90) | - |
| G25E25S0.5 | 100 | 91 (91) | NS |
| G25E25F30 | 100 | 90 (90) | NS |
| G25E25 | 100 | 93 (93) | NS |
Note: G25E25 = 25% glycerol, 25% ethylene glycol, 20% SSS and PBS; G25E25F30 = G25E25 + 10 mg/mL Ficoll; G25E25S0.5 = G25E25 + 0.5M sucrose; G25E25S0.5F30 = G25E25 + 0.5M sucrose + 10 mg/mL Ficoll; NS = not statistically significant (vs. control) (Fisher’s extract test).
Based on the result on Mouse study that the survival rates of post-warm blastocysts were not affected by removing both sucrose and Ficoll, human blastocysts were vitrified in one of two different vitrification solutions, G25E25 and G25E25S0.5F10. Four-hundred and one blastocysts from 206 patients were vitrified in the G25E25 solution and 443 blastocysts from 229 patients in G25E25S0.5F10 solution. The Mean age of women was 34.4 ± 4.3 years in the G25E25 group and 33.2 ± 3.7 in the G25E25S0.5F10 group without a significant difference. Infertility duration and infertility causes had no difference between the two groups (Table 2).
| Characteristics | Vitrification solution | p | |
|---|---|---|---|
| G25E25S0.5F10 | G25E25 | ||
| Mean age (years) | 33.2 ± 3.7 | 34.4 ± 4.3 | 0.682 |
| Duration of infertility (years) |
3.9 ± 3.6 |
3.8 ± 2.5 |
0.212 |
| Infertility factor |
|||
Note: G25E25 = 25% glycerol, 25% ethylene glycol, 20% SSS and PBS; G25E25S0.5F30 = G25E25 + 0.5M sucrose + 10mg/mL Ficoll.
In vitro survival rates of vitrified-warmed human blastocysts in the G25E25 group was 96%, which was similar to that of G25E25S0.5F10 group (92%). TheMean numbers of transferred blastocysts were 1.9 and 1.8 in the G25E25 and the G25E25S0.5F10 group, respectively. The clinical and ongoing pregnancy rates in G25E25 were 53.3 and 78.1%, respectively, which was little higher than those in G25E25S0.5F10 (51.9 and 77.3%, respectively), but there was no significant difference between both groups (Table 3).
| Vitrification solution | |||
|---|---|---|---|
| G25E25S0.5F10 | G25E25 | ||
| No. of blastocyst vitrified | 443 | 401 | 0.066 |
| No. of blastocyst survived after warming | 407 | 385 | 0.087 |
| Survival rate (%) | 92 | 96 | 0.061 |
| Mean number of blastocyst transferred | 1.8 | 1.9 | 0.527 |
| No. of clinical pregnancies (%) | 119 (51.9) | 110 (53.3) | 0.391 |
| No. of ongoing pregnancies (%) | 92 (77.3) | 86 (78.1) | 0.215 |
Note: G25E25 = 25% glycerol, 25% ethylene glycol, 20% SSS and PBS; G25E25S0.5F30 = G25E25 + 0.5 M sucrose + 10 mg/mL Ficoll.
The present study shows that omission of sucrose and Ficoll from vitrification solutions in cryopreservation of blastocysts had no significant effect on the survival rate or clinical pregnancy outcome of post-warm blastocysts. To the best of our knowledge, this is the first study to report that sucrose and Ficoll may not be required components in the vitrification solutions for successful cryopreservation of shrunken blastocysts. This result is of great value in introducing a new concept about the composition of vitrification solution.
As embryos contain a large proportion of water and it is not possible to Manually remove this fluid without damaging the embryo, early IVF studies investigated alternative Methods for partial dehydration of cleavage stage embryos prior to cryopreservation. Sugars such as trehalose and sucrose were initially used to dehydrate cells by osmolarity, thereby helping to prevent ice crystal formation from damaging the embryo on subsequent freezing, and sucrose has been shown to protect cells from the rapid influx of highly concentrated permeable agents [11, 18, 19]. Previous studies have also found that Ficoll not only helps prevent ice crystal formation [11], but also slows down aqueous fluid shifts, helping to protect the outer part of the embryos containing the trophoblastic cells [20, 21]. For this reason, sucrose and Ficoll are usually added to vitrification solutions for the cryopreservation of cleavage stage embryos.
However, unlike the cleavage-stage embryos, blastocyst-stage embryos contain a large amount of the water in a structure called blastocoel fluid. Although some studies have shown no beneficial effect of blastoceol cavity fluid aspiration before vitrification on pregnancy outcomes [22, 23], most studies have reported that artificial shrinkage of blastocysts May prevent ice-crystal formation and increase survival rate of post-warm blastocysts [14, 15, 16]. For this reason, blastocysts are usually subjected with artificial shrinkage to deplete the fluid from the blastocoele cavity prior to the vitrification process. An issue is whether sucrose and Ficoll is needed to freeze the shrunken blastocysts. Previous studies have reported that vitrification solutions without sucrose or Ficoll were used in the cryo-storage of somatic cells or stem cell [24, 25, 26]. Hiraoka et al. also reported the use of vitrification solution without Ficoll in successful cryopreservation of expanded blastocysts [25]. These results suggest that careful consideration should be given to whether the addition of sucrose and Ficoll to vitrification solution is necessary for further dehydration in the cryopreservation of shrunken blastocysts.
This study was performed preliminarily using Mouse blastocysts prior to applying to human blastocysts in order to examine the effect of both sucrose and Ficoll on the survival rate of vitrified-warmed blastocyst. Mouse blastocysts were treated by artificial shrinkage and then placed in one of four different vitrification solutions formulated with and without sucrose and/or Ficoll. The results showed that the survival rates of vitrified-warmed blastocysts were similar regardless of the addition of sucrose and Ficoll to vitrification solution. When this study was applied to human blastocysts, it was confirmed that in vitro survival rates as well as pregnancy outcomes of vitrified-warmed blastocyst did not significantly different. These results suggest that shrunken blastocysts have no longer benefit from the further dehydrating effects of Ficoll and sucrose additives in the vitrification solution.
The use of vitrification solutions without sucrose and Ficoll has the clear advantage of greater simplicity of formulation and consequent reduction in total reagent costs. Most importantly, it is possible to increase the sensitivity of the embryo to the thawing solution during thawing because the increased viscosity by Ficoll can interfere with the release of the frozen solution out of the embryo during thawing.
Artificial shrinkage by removing the blastocoele fluid has been performed by various Methods including Microneedle [12], Micropipette [28], 29-gauge needle [29], and laser pulses [30]. These methods have advantages and disadvantages in terms of convenience, shrinkage time and cost, but the cryopreservation outcomes between them were similar. The present study used an artificial shrinkage method using holding and ICSI Micropipettes [16, 30], and obtained a successful cryopreservation outcome with survival rate over 90% and a clinical pregnancy rate over 50% in humans.
One of the limitations of the present study was that human blastocysts were obtained from women that were underwent IVF-ET by differetnt ovarian stimulation protocols including GnRH antagonist, Mid-luteal long GnRH agonist, ultra-long or ultra-short GnRH agonist protocols. In general, the ovarian stimulation protocol is determined by the ovarian response considering female age and ovarian reserve. The age and ovarian response of the 442 patients participating in this study was also very diverse and this study used different ovarian stimulation protocols. However, since embryo develomental competency is ultimately determined by oocyte quality, which in turn depends on female age or ovarian response status rather than ovarian stimulation protocol, it seems unlikey that variation in the ovarian stimulation protocol would have affected the outcomesMeasured in this study.
In conclusion, the present study reveals that vitrification solution without sucrose and Ficoll can be successfully employed in the cryopreservation of Mouse and human blastocysts without compromising blastocyst survival rate and pregnancy outcome.
This study was supported by a 2-year research grant of Pusan National University.
The authors report no conflicts of interest.