


 , R.X. Shi 1,*
, R.X. Shi 1,*1 The Second People’s Hospital of Changzhou, Nanjing Medical University, Changzhou, Jiangsu Province, 213000, P.R. China
Abstract
Purpose: The aim of this study was to investigate the safety of combined laparoscopic surgery and hysteroscopic electrosurgery for partial repair of the cesarean scar and removal of the conceptus, respectively, in cesarean scar pregnancy (CSP). Methods: This was a retrospective analysis of data from 23 patients with CSP who underwent laparoscopic surgery together with hysteroscopic electrosurgery between January 2008 and January 2016 at our medical center. Under hysteroscopic visualization, the gestational sac and the complete cesarean section scar were cut by laparoscopic surgery. Results: Patient age was 28 ± 3.3 years (mean ± SD) with a range of 22-38 years. Patient gravidity was 3.0 ± 1.2 with a range of 1-6, while parity was 1.0 ± 1.5 with a range of 1-3. Intraoperative blood loss was 100.2 ± 32.7 mL (mean ± SD), operating time was 60 ± 48.6 min and the duration of hospitalization was 5 ± 1.2 days. Surgery was successful in all patients, with no instances of bladder injury. The level of β-human chorionic gonadotropin (β-HCG) began to decrease on the second postoperative day and returned to normal levels within one month of surgery. The mean time required for normalization of serum β-HCG levels was 25 ± 5.2 days (mean ± SD) with a range of 20-35 days. Conclusions: Laparoscopic surgery combined with hysteroscopic electrosurgery for partial repair of the cesarean scar and removal of the conceptus, respectively, is a safe, feasible and effective treatment approach for CSP.
Keywords
- Cesarean scar pregnancy (CSP)
- Laparoscopy
- Hysteroscopy
The increasing rate of cesarean sections is a medical concern as well as an important socioeconomic issue. Cesarean section is the most common surgery performed in women [1]. The rate of cesarean delivery was reported to be as high as 46% in China in 2010 [2] and 33.3% worldwide in 2006 [3]. The rate of repeat cesarean delivery in America was estimated to be as high as 91% in 2010 [4]. The general public is not well informed about the risks associated with cesarean delivery.
One of the complications associated with cesarean delivery that warrants serious consideration is CSP. This condition can lead to uterine rupture and bleeding, thereby placing a significant risk on the woman’s fertility and, more importantly, on her life [5]. Although the incidence of CSP is 1/1800 [6, 7], the frequency has increased in parallel with the rising number of cesarean deliveries.
The most efficient diagnostic modality for CSP is transvaginal ultrasonography. Pelvic magnetic resonance imaging (MRI) may sometimes be necessary and is more advantageous than ultrasonography because of its excellent soft-tissue resolution and the ability to perform multi-planar imaging. However, the high cost of MRI limits its application.
Since 2012, more than 30 methods have been reported for the treatment of CSP [8]. These include methotrexate (MTX) injection [9], local MTX injection guided by color Doppler ultrasonography [10, 11], the vacuum extraction method, uterine artery embolization, as well as various types of surgery including hysteroscopy, laparoscopy with hysteroscopy, abdominal surgery and vaginal surgeries [12-16]. In the current study, we investigated the safety of an approach involving laparoscopy combined with hysteroscopic electrosurgery. We employed this method in the management of 23 CSP cases and describe here the favorable results obtained.
This retrospective study included 23 patients with CSP who underwent laparoscopic surgery with hysteroscopic electrosurgery and partial surgical removal and repair of the cesarean scar. All patients were treated from January 2008 to January 2016 at the Department of Gynecology, Second People’s Hospital of Changzhou, an affiliate of Nanjing Medical University. Patient medical history up to the time of surgery was carefully collected and all patients underwent medical and pelvic examinations. The diagnosis of CSP was made on the basis of ultrasonography and pelvic MRI findings (Figure 1). Using these methods, the myometrium thickness at the cesarean scar was determined to be < 2.5 mm and the gestational sac was a convex bladder.
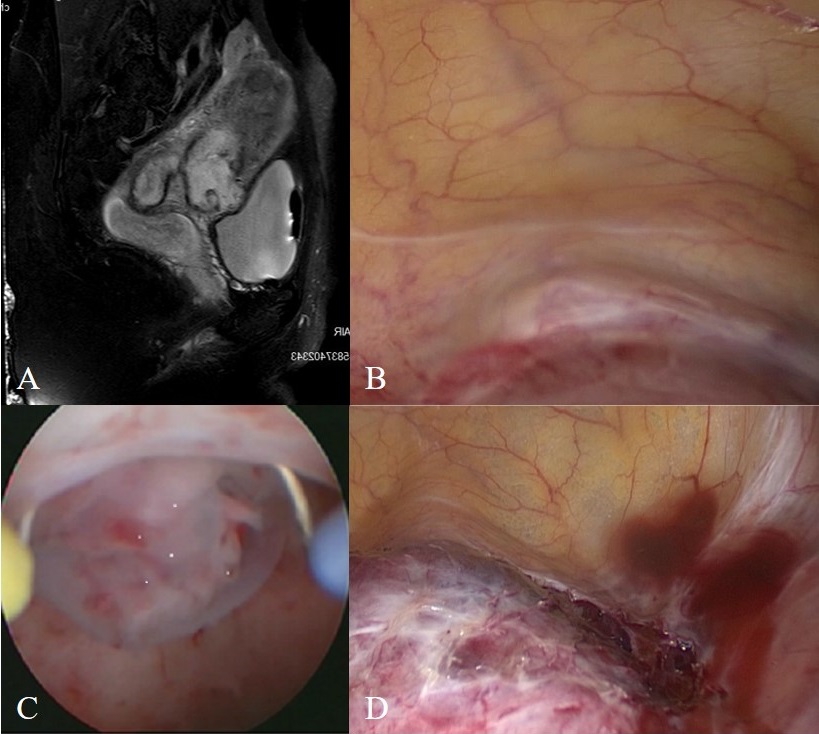 Figure 1.
Figure 1.— (A) Magnetic resonance imaging showed the gestational sac at the uterine isthmus scar. (B) Laparoscopic view showed the surface of the cesarean scar pregnancy. (C) Detection of the gestational sac was found on a previous cesarean scar. (D) Hysteroscopic view of the cesarean scar pregnancy followed the separation of adhesions between the uterine scar and the bladder.
All surgeries were performed by the same surgeon (RS) and with the same medical team. Further, all patients attended follow-up visits at 1, 3 and 12 months.
The operation was performed under general anesthesia and with patients in the Trendelenburg position. The abdomen was inflated with CO2, followed by insertion of a 10-mm trocar through the umbilicus and three 5-mm trocars into the hypogastrium. An ultrasonic scalpel (Johnson & Johnson) was used to separate adhesions between the uterine scar and the bladder, thus preventing injury. The cervix was then dilated using Pratt dilators up to 35 F. The distention medium was 1.5% glycine and the pressure of inflation varied depending on the patient’s systolic pressure. During operation, the input and output volumes of the saline solution were measured. Electrosurgery was performed at settings of 120 W and 100 W for cutting and coagulation, respectively. Under hysteroscopic visualization, the gestational sac was cut using the loop of the hysteroscope. Coagulation was used to control bleeding from the periphery of the lesion. Before cutting the cesarean section scar, hysteroscope light was inserted into the diverticulum to guide the direction and allow the complete cesarean section scar to be cut by laparoscopic surgery. The incision was closed by laparoscopy in three layers with 1/0 PolysorbTM to consolidate the uterine isthmus.
The pelvic cavity was washed with saline solution to minimize the risk of adhesions and to check for unusual bleeding. The incision in the peritoneum was closed by continuous suture with 1-0 Vicryl®. Methotrexate (MTX) injection was administered in the myometrium near the wound to prevent residual villi. The sample obtained through laparoscopy was examined pathologically.
The mean intraoperative blood loss, mean operative time and mean duration of hospitalization were 100.2 ± 32.7 mL, 60 ± 48.6 min, and 5 ± 1.2 days, respectively. There were no instances of bladder injuries and all surgeries were successfully completed. In all cases, pathological examination of the excised tissue revealed the presence of some villi and some degree of necrosis (Figure 2). The patients’ β-human chorionic gonadotropin (β-HCG) levels decreased on the second postoperative day but had completely normalized one month after the operation. The average time required for normalization of the serum β-HCG level was 25 ± 5.2 days (range, 20-35 days).
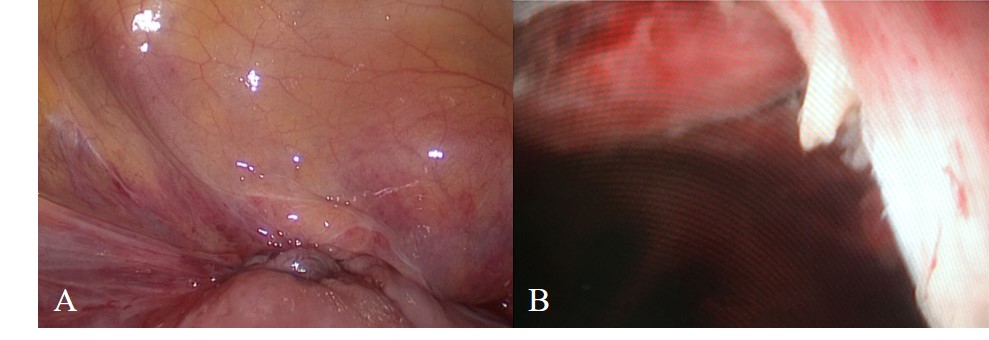 Figure 2.
Figure 2.— The incision was closed by laparoscopy in three layer to consolidate the uterine isthmus. Under hysteroscopic visualization, no gestational sac and no diverticulum were found after the operation.
In 5 of the 23 cases, the scar pregnancy had been misdiagnosed as an early intrauterine pregnancy during the initial evaluation with abdominal ultrasound. These 5 patients presented with miscarriage, resulting in severe, life-threatening hemorrhage. All 5 cases were successfully managed using the approach of laparoscopy combined with hysteroscopy, giving favorable outcomes. Fortunately, hysterectomy was not required with any of these patients.
The management of CSP without causing severe adverse sequelae such as hysterectomy presents a major challenge in obstetric practice. While various treatment approaches have been reported in the past, their efficacy and safety are debatable. In the present study, we evaluated the safety and efficacy of laparoscopic surgery for partial repair of the cesarean scar at the uterine isthamus, and of hysteroscopic electrosurgery for removal of the gestational sac along with the decidua and villi. The successful combination of laparoscopy and hysteroscopy for the management of individual cases has been reported previously [17]. Wu et al. also compared the combination of laparoscopic and hysteroscopic approaches with other methods such as uterine embolization and found the former to be more effective and safer [18]. Our findings also demonstrate this combined approach is safe and effective for the management of CSP.
In the present study, a laparoscopic approach was used for partial repair of the cesarean section scar. Because of the tissue damage associated with a cesarean section scar, the villi and decidua tend to invade the myometrium. The cicatrix of the previous cesarean section at the uterine isthmus lacks muscle cells and thus cannot produce uterine contractions. Under laparoscopic visualization, we could effectively and safely use an ultrasonic knife to precisely dissect adhesions between the bladder and uterine scar, without any incidence of bladder injury. Preoperative and perioperative interventions, including intramuscular MTX or oral mifepristone, are likely to reduce bleeding and the need for postoperative blood transfusions. We administered a MTX injection in the myometrium to eliminate villi in our patients.
A CSP can sometimes be misdiagnosed as an intrauterine pregnancy, especially when abdominal ultrasound is used. In such cases, curettage without proper evaluation may result in severe and possibly life-threatening vaginal bleeding which may necessitate hysterectomy and therefore jeopardize the patient’s fertility. However, with our treatment approach we were able to successfully manage the misdiagnosed cases without any instance of hysterectomy.
Some types of surgery for CSP, such as trans-cervical resection of the gestational sac by hysteroscopic treatment, are simple and show rapid recovery, but have a high risk of bladder injury and uterine perforation. Raimondo et al. recommended that hysteroscopic surgery is not suitable if the gestational sac is close to the bladder and the cesarean scar is < 4 mm thick by ultrasonography or pelvic MRI findings [19]. Others have suggested the combination of laparoscopic and hysteroscopic approaches was more suitable if the cesarean scar was < 2.5 mm [20], and that the vaginal approach was also appropriate.
Our study does have some limitations such as a small sample size, a retrospective design, and the lack of a control group. However, this is mainly because CSP is relatively rare and difficult to diagnose. Evaluation of reproductive outcomes were not possible, since the longest follow-up period was one year. Nevertheless, the success rate in our study was 100% and we believe that large-scale studies involving multiple centers may further corroborate our results. In conclusion, the combined approach of laparoscopic surgical repair of the cesarean scar together with hysteroscopic electrosurgery for removal of the conceptus appears to be safe, feasible and effective for the conservative management of CSP.
All patients who participated in this study did so in the context of mutual trust, open communication and informed consent. The study protocol was approved by the ethics committee of our institution (approval number: [2018] KY026-01).
This study was supported by Changzhou Sci & Tech Program (CJ20180074) and the Affiliated Changzhou No.2 People’s Hospital of Nanjing Medical University (2018K006).
The authors declare no conflict of interest.