
 , H. Deng 1, X. Yang 1, J.L. Wang 1
, H. Deng 1, X. Yang 1, J.L. Wang 11 Department of Obstetrics and Gynecology, Peking University People's Hospital, Beijing, 100044, P.R. China
2 Nursing School of Peking University, Beijing, 100044, P.R. China
†Contributed equally.
Abstract
Purpose: The aim of this study was to compare mechanical bowel preparation (MBP) with oral laxative against no bowel preparation on the perioperative outcomes for pelvic floor dysfunction (PFD). The need for bowel preparation before vaginal surgery was thus also investigated. Methods: PFD patients undergoing vaginal surgery in Peking University People's hospital from September 2017 to July 2018 were randomly assigned to MBP (n = 60) or control (n = 60) groups. The two groups were compared for the incidence of preoperative abdominal symptoms and overall patient satisfaction, intraoperative visualization of the surgical field assessed by the surgeon, and postoperative recovery outcomes. Results: There were no statistically significant differences between the two groups (p > 0.05) for surgical visualization, the surgeon’s overall satisfaction, or for the rate of postoperative complications. However, patients in the MBP group reported more gastrointestinal symptoms and had reduced satisfaction compared to the control group (p < 0.05). Conclusion: The use of MBP before vaginal surgery reduces preoperative patient satisfaction while conferring no benefit in terms of optimizing surgical visualization and reducing postoperative complications. For patients with PFDs, it is safe and feasible to do without MBP before vaginal surgery.
Keywords
- Slutions
- Bwel preparation
- Plvic floor dysfunction
- Srgical procedures
- Oerative
Pelvic floor disorders (PFDs) are very common in women and include pelvic organ prolapse (POP), urinary incontinence (UI) and fecal or anal incontinence (FI, AI). Surgical treatment is generally recommended for patients with severe PFDs. One in five women are likely to undergo surgical correction for PFDs [1] with an additional 30% at risk of reoperation [2].
In theory, preoperative Mechanical Bowel Preparation (MBP) such as enema and oral laxative should reduce gastrointestinal residue and intraoperative fecal contamination. This reduces the incidence of surgical site infection (SSI) and postoperative anastomotic fistula. However, MBP is an unpleasant experience for many patients and may cause dehydration and electrolyte disturbance [3].
Recent systematic reviews of elective colorectal surgery concluded that the use of oral and/or rectal bowel preparation did not lower the risk of postoperative complications when compared to no MBP [4, 5]. Furthermore, studies have demonstrated no advantages of MBP for laparoscopic gynecologic surgery and indeed reported an increase in adverse effects [6-8]. The latest guidelines for perioperative care in gynecologic oncology strongly recommend the abrogation of routine pre-operative bowel preparation before minimally invasive gynecological surgeries [9]. Nonetheless, many pelvic reconstructive surgeons continue to use preoperative bowel preparation.
Ballard and colleagues [10] explored the need for MBP before vaginal surgeries among US patients with prolapse and concluded that the use of saline enema by pelvic floor surgeons should be reconsidered. Adelowo et al. [11] found that administration of oral sodium phosphate (NaP) enema with oral laxative before laparoscopic or robotic pelvic reconstructive surgery for UK patients with prolapse conferred no benefit for optimizing intraoperative visualization compared to NaP enema alone. In China, MBP is still used routinely before pelvic reconstruction surgeries in order to control intraoperative fecal bacterial infection. This is due to the close location of the vaginal orifice to the anus.
Few studies have investigated the need for MBP in PFD patients undergoing vaginal surgeries. Hence, the aim of this randomized clinical trial was to compare MBP with oral laxative against no bowel preparation on the perioperative outcomes of patients with PFDs.
This was a prospective, randomized controlled trial comparing bowel preparation with oral laxative versus no bowel preparation prior to pelvic reconstruction surgeries. Hospitalized patients in Peking University People’s hospital, Beijing, China, were recruited to the study from September 2017 to July 2018. Patients of any age with a diagnosis of at least one PFD and scheduled to undergo correction surgery were potentially eligible for inclusion. Aside from not consenting, patients were excluded if they were unable to tolerate oral laxatives or if they had a history of gastrointestinal surgery, diagnosis of chronic constipation, or gastrointestinal inflammation. Before the trial, patients were informed of the purpose and significance of the study.
All subjects gave their informed consent before participating in the study. The study was conducted in accordance with the Declaration of Helsinki and the protocol was approved by the Ethical Review Committee of the Peking University People’s Hospital (2017-085).
The allocation sequence was generated via a random number generator (1:1) and included the numbers 0 (representing the MBP group) and 1 (representing the control group). The group allocation was stored away from the clinic and concealed in an opaque numbered envelope. Following recruitment, a research nurse assigned a number to the PFD patients according to their order of admission and opened the envelope with the same number to assign the participants into either group on the day before operation day. Details of the randomization were kept by the research nurse and all surgeons were blinded to the group allocation.
All participants were provided with instructions concerning preparation before surgery. Patients in both groups were allowed a general diet the day before surgery, with no solid food to eat after midnight and no clear liquid to drink after 6 am on the operation day. Patients randomized to the MBP group were instructed to self-administer an oral laxative (Fortrans®, Polyethylene Glycol-Electrolyte Powder). This is used routinely for preoperative bowel preparation in the Peking University People’s hospital. MBP patients were instructed to administer the laxative at 2 pm the day before operation. Administration consisted of dissolving a pack of Fortrans® (137.12 g/pack) in warm water to make a 2000 mL solution and then taking orally at a rate of about 700 mL per hour.
Demographic and clinical/surgical information (age, height, weight, diagnosis, surgery procedures) were obtained from the participants and from their medical records within 24 hours after admission to hospital or after surgery. The data included preoperative patient-reported outcomes with bowel preparation, intraoperative assessment of the surgical field by surgeons, and postoperative recovery outcomes of participants. The perioperative outcomes of participants were evaluated at three time points.
The first time point was the morning before operation. Clinical nurses evaluated patients for difficulty with the bowel preparation, completion of the assigned bowel preparation, and presence of gastrointestinal symptoms such as nausea, vomiting, abdominal cramping or pain, anal irritation, weakness, hunger, thirst or insomnia. Overall patient satisfaction was assessed using a 10-point Visual Analog Scale (1-2, dissatisfied; 3-5, average; 6-8, satisfied; 9-10, very satisfied).
The second time point was at the end of surgery. The primary surgeon who performed and supervised all surgical procedures was asked to assess the patients’ stool according to the bristol stool form scale. They were also requested to assess the visualization of surgical field, ease of bowel handling, and overall satisfaction with the preoperative bowel preparation using a 10-point VAS (1-2, poor/difficult/dissatisfied; 3-5, fair/average; 6-8, good/easy/satisfied; 9-10, excellent/very easy/very satisfied).
The third time point was the postoperative to discharge period. Patient recovery outcomes were evaluated by a clinical nurse and included the postoperative day of the first flatus, the first ambulation, the return to a general diet, the incidence of surgical site infection or other perioperative complication, and the number of postoperative hospitalization days.
Sample size estimation was based on the hypothesis that the primary outcome (adequate visualization) would be the same with or without MBP. Ballard et al. [9] previously reported adequate visualization in 85% of patients with bowel preparation. Using this result and assuming a margin of equivalence of 15% (72.25-97.75%) and with alpha set at 0.05, the study would be adequately powered (at least 80%) with 86 patients in each group (N = 172). Subject enrollment was stopped before reaching the original target of 172 due to the overwhelming evidence showing there was no difference in responses to the surgeon questionnaire between the two groups. Patients in the two study groups were compared by t-test for continuous normally distributed variables, Mann-Whitney U test for non-normal or ranked variables, and χ2/Fisher’s exact test for grouped variables. p < 0.05 was considered statistically significant. All analyses were performed using SPSS 17.0 statistical software.
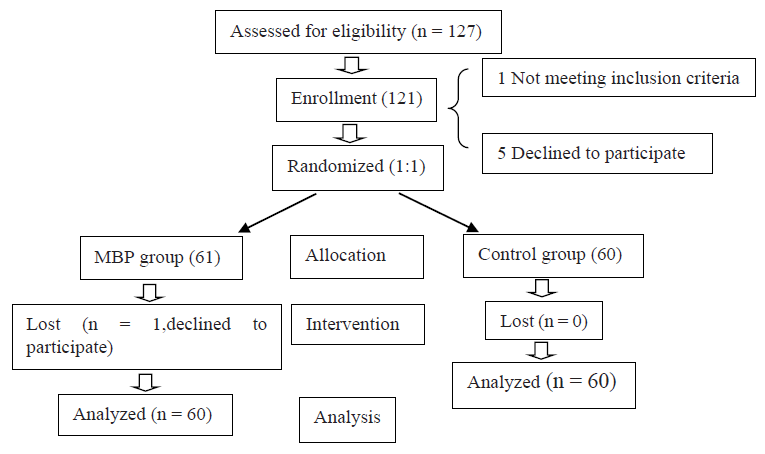
Figure 1 shows the participant flow in the study. In total, 121 patients were enrolled and randomized to either the MBP or control groups. One patient randomized to the MBP group asked to withdraw from the study. A total of 60 patients in each group completed the study and their demographic and surgical characteristics are shown in Table 1. There were no significant differences between the two groups (p > 0.05) for age, body mass index, history of PFD surgeries, diagnoses, anesthesia, laparoscopic-assistance, surgical procedure, intraoperative complications, estimated blood loss or operative time.
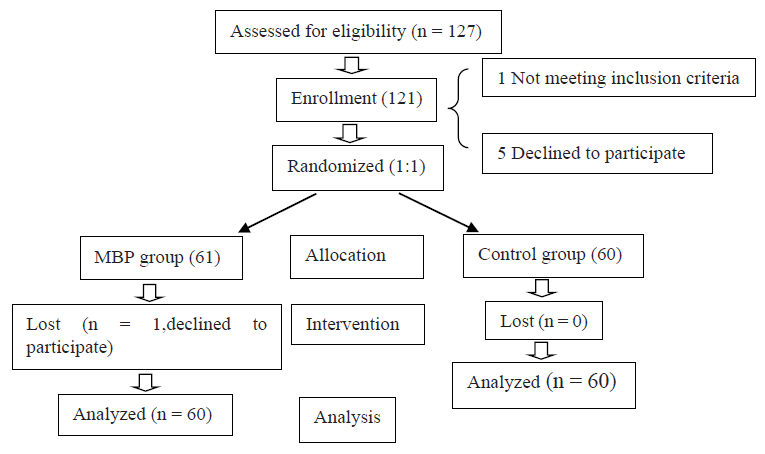 Figure 1.
Figure 1.— Participant flowchart.
| Characteristics | MBP group (n = 60) | Control group (n = 60) | p value |
|---|---|---|---|
| Age (years) |
0.591a | ||
| Body Mass Index (kg/m2) | 28.52 ± 5.71 | 27.83 ± 3.91 | 0.511a |
| Previous PFDs surgery, yes | 2 (3.3) | 3 (5.0) | 0.123b |
| Diagnoses | |||
| Prolapse | 59 (98.3) | 57 (95) | 0.412b |
| Urinary incontinence | 32 (53.3) | 35 (58.3) | 0.384b |
| Anal incontinence | 5 (8.3) | 8 (13.3) | 0.781b |
| Anesthesia | 0.464b | ||
| Intravenous anesthesia | 15 (25.0) | 13 (21.7) | |
| Spinal anesthesia |
12 (20.0) |
14 (23.3) |
|
| Laparoscopic-assisted surgery, yes | 6 (10.0) | 4 (6.7) | 0.454b |
| Procedures | |||
| Concurrent hysterectomy | 39 (65.0) | 43 (71.7) | 0.581b |
| Concurrent suspension | 23 (38.3) | 28 (46.7) | 0.211b |
| Concurrent anterior/posterior repair | 14 (23.3) | 12 (20.0) | 0.450b |
| Tension-free vaginal tape | 7 (11.7) | 5 (8.3) | 0.259b |
| Intraoperative complications, n (%) | 0 | 0 | --- |
| Estimated blood loss (mL) | 100 (50-150) | 95 (20-150) | 0.434c |
| Duration of surgery (min) | 112 (50-150) | 105 (40-145) | 0.331c |
Data are presented as mean ± SD, median (interquartile range) or n (%). SD, standard deviation; CSEA, combined spinal and epidural anesthesia. pa, t test; pb, χ2 test; pc, U test.
As shown in Table 2, 7 patients in the MBP group experienced difficulty performing the preoperative bowel preparation. All other patients in the two groups finished the preparation as outlined in the guidelines. Compared with the control group, MBP patients reported significantly more gastrointestinal symptoms such as abdominal cramping or pain, abdominal bloating or swelling, anal irritation, and weakness. Moreover, the satisfaction scores for patients in the MBP group were lower than those reported by the control group (p < 0.05).
| Outcomes | MBP group (n = 60) | Control group (n = 60) | p value | |
|---|---|---|---|---|
| Difficulty with the bowel preparation | 15 (25.0) | 0 | < 0.001d | |
| Completed assigned bowel preparation | 60 (100) | 60 (100) | --- | |
| Self-reported symptoms | ||||
| Nausea | 5 (12.0) | 2 (3.3) | 0.181b | |
| Vomiting | 3 (5.0) | 0 | 0.074d | |
| Abdominal cramping or pain | 18 (30.0) | 3 (5.0) | < 0.001b | |
| Abdominal bloating or swelling | 24 (40.0) | 2 (3.3) | < 0.001b | |
| Anal irritation | 32 (53.3) | 2 (3.3) | < 0.001b | |
| Weakness | 4 (6.7) | 0 | < 0.001d | |
| Hunger | 15 (25.0) | 10 (16.7) | 0.123b | |
| Thirst | 10 (16.7) | 8 (13.3) | 0.341b | |
| Insomnia | 3 (5.0) | 2 (3.3) | 0.781b | |
| Overall satisfaction,10-point VAS(1-10) | 6 (3-9) | 10 (8-10) | < 0.001c | |
Data are presented as n (%) or median (interquartile range). pb, χ2 test; pc, U test. pd, Fisher’s exact test.
Table 3 shows the intraoperative assessment of surgical field by the primary surgeon. There were 16 cases of stooling in the surgical field among patients in the MBP group compared to 6 in the control group (χ2 = 2.485, p = 0.042). Analysis of the anesthesia type among the stooling patients showed no significant difference between the two groups (χ2 = 9.035, p = 0.23). Surgical visualization, bowel handling and overall satisfaction were not statistically different between the MBP and control groups (p > 0.05).
| Variable | MBP group (n = 60) | Control group (n = 60) | p value |
|---|---|---|---|
| Stooling on the field | 0.041b | ||
| No | 41 (68.3) | 54 (90.0) | |
| Watery stool (BSFS type 7) | 10 (16.7) | 3 (5.0) | |
| Mushy stool (BSFS type 6) | 6 (10.0) | 2 (3.3) | |
| Soft blots stool (BSFS type 5) | 3 (5.0) | 1 (1.7) | |
| Estimated stooling | 0.030b | ||
| < 15 mL | 13 (21.7) | 5 (8.3) | |
| 15-30 mL | 2 (3.3) | 0 | |
| > 30 mL | 4 (6.7) | 1 (1.7) | |
| Easiness handling bowel,10-point VAS (1-10) | 0.680b | ||
| Very easy (9-10) | 30 (50.0) | 32 (53.3) | |
| Easy (6-8) | 20 (33.3) | 21 (35.0) | |
| Average (3-5) | 7 (11.7) | 5 (8.3) | |
| Difficult (1-2) | 3 (5.0) | 2 (3.3) | |
| Surgical visualization,10-point VAS (1-10) |
0.557b | ||
| Fair (3-5) | 6 (10.0) | 3 (5.0) | |
| Poor (1-2) | 2 (3.3) | 2 (3.3) | |
| Overall satisfaction,10-point VAS (1-10) | 0.070b | ||
| Very satisfied (9-10) | 30 (50.0) | 34 (56.7) | |
| Satisfied (6-8) | 25 (41.7) | 20 (33.3) | |
| Average (3-5) | 3 (5.0) | 4 (6.7) | |
| Dissatisfied (1-2) | 2 (3.3) | 2 (3.3) | |
Data are presented as median (interquartile range) or n (%). BSFS, Bristol Stool Form Scale; VAS, visual analogue scales. pb, χ2 test.
Table 4 shows the postoperative recovery outcomes for the study participants. No SSIor other postoperative complication occurred amongst the participants of either group. The postoperative day of the first flatus, the first ambulation, return to general diet, and the number of postoperative hospitalization days were all similar between the two groups (p > 0.05).
| Variable | MBP group (n = 60) | Control group (n = 60) | p value |
|---|---|---|---|
| Postoperative day of the first flatus | 2 (1, 3) | 2 (1, 3) | 0.174c |
| Postoperative day of return of general diet | 1 (1, 2) | 1 (1, 2) | 0.258c |
| Postoperative day of ambulation | 1 (1, 3) | 1 (1, 3) | 0.380c |
| Surgical site infection | 0 | 0 | --- |
| Perioperative complication | 0 | 0 | --- |
| Length of postoperative hospitalization day | 3 (2, 4) | 3 (2, 4) | 0.544c |
Data are presented as median (interquartile range) or n (%). pc, U test.
MBP before vaginal surgery was generally thought to be essential for achieving better visualization during the procedure. The present study found that ingestion of an oral laxative as MBP before vaginal surgery in patients with PFDs did not improve surgical visualization compared with no MBP (p > 0.05). Moreover, patients in the MBP group showed a higher incidence of intraoperative stooling (p < 0.05). Importantly, MBP increased the incidence of distressing bowel symptoms reported by patients, thus reducing their overall satisfaction (p < 0.05). Furthermore, the absence of preoperative bowel preparation had no significant impact on postoperative rehabilitation in patients.
The present findings are consistent with previous studies investigating the role of bowel preparation before laparoscopic gynecologic surgery. Won et al. [12] randomly assigned 308 women scheduled to undertake gynecologic laparoscopic surgery into 3 groups: fasting only (n = 86), minimal residue diet for 2 days before surgery (n = 84), and MBP with oral laxative (n = 87). These workers found no significant differences in intraoperative surgical view and bowel handling between the 3 groups. Given the significant symptoms and discomfort for patients undertaking minimal residue diet with or without MBP, Won and colleagues concluded that fasting alone without any preoperative dietary or bowel preparation is a preferable alternative for laparoscopic gynecologic surgery involving the posterior pelvic compartment.
The latest systematic review [4] of MBP analyzed 23 randomized controlled trials and 13 observational studies, comprising a total of 21,568 patients undergoing elective colorectal surgery. The results of meta-analysis found there were no significant differences in terms of the incidence of anastomotic leak, SSI, mortality, reoperation or hospital length of stay between MBP and no MBP. Ballard and colleagues [10] enrolled 150 prolapse patients into a single-blind, randomized trial to explore the effects of saline enema on vaginal surgery. Their results showed that abdominal cramping, anal irritation and fatigue were more frequent in the enema group compared to the controls, whereas the surgical field of visualization assessed by the surgeons was the same in the two groups. The data from the present study concur with the results of Ballard et al. Importantly, no positive impact of preoperative bowel preparation on postoperative recovery in PFD patients was observed.
The prospective, randomized control study design of this trial was associated with a low patient dropout rate. Moreover, all surgeries were performed by one surgeon and in a blinded manner. The preoperative patient-reported outcomes, intraoperative surgeon-reported outcomes and postoperative objective outcomes are comprehensive and reliable. The target sample size required for the study was not reached due to strong evidence showing no difference in surgical visualization between the MBP and control groups. Using the two-sided Fisher's exact test with a significance level of 0.05, the sample size in this study provided 78.4% power to detect a difference in overall SSI rate between the two groups. In view of the high incidence of symptoms related to bowel preparation and no difference in the surgeon’s assessment of surgical visualization, patient recruitment was terminated before the initial target sample size was reached.
The lack of MBP before surgery in patients with PFD improves their satisfaction while having no impact on visualization of the surgical field or on postoperative recovery. It is safe and feasible to abandon MBP before vaginal surgery in patients with PFDs. In light of these and previous findings, pelvic floor surgeons should reconsider the routine practice of MBP and especially oral laxatives for PFD patients undergoing vaginal surgery.
We are grateful to the numerous individuals who participated in this study and to those who helped during the writing of the manuscript.
All authors declare no conflict of interest in this study.