

 , M. Yamauchi 1, M. Kasai 1, T. Fukuda 1, T. Ichimura 1, T. Yasui 1, T. Sumi 1
, M. Yamauchi 1, M. Kasai 1, T. Fukuda 1, T. Ichimura 1, T. Yasui 1, T. Sumi 11 Department of Obstetrics and Gynecology, Osaka City University Graduate School of Medicine, Osaka 545-8585, Japan
Abstract
Background: Tuberculosis can spread to the peritoneum through the gastrointestinal tract via mesenteric lymph nodes or directly from the blood, lymph, or fallopian tubes. Tuberculous peritonitis can mimic pelvic or intra-abdominal malignancies, making the diagnosis of this disease difficult. Case: A 32-year-old female presented with tuberculous peritonitis that mimicked peritoneal cancer. Our patient presented with general fatigue, weight loss, and diarrhea, which had started 3 months prior. On examination, a thickened peritoneum and ascites, without bilateral adnexal masses, and elevated serum CA125 levels were detected. Peritoneal cancer was initially considered as the most likely diagnosis. An exploratory laparoscopy was performed, and a thickened peritoneum and whitish miliary nodules scattered throughout the abdominal cavity, including the surface of the uterus and adnexa were found. The pathological examination of the frozen resected nodule specimen showed an epitheloid granuloma. We diagnosed the patient with tuberculous peritonitis, which was established postoperatively. Conclusion: If peritoneal cancer is suspected in patients without abnormal cytology of the ascites, early exploratory laparoscopy should be performed to rule out tuberculous peritonitis in the differential diagnosis of patients with peritoneal cancer.
Keywords
- Tuberculous peritonitis
- Peritoneal cancer
- CA125
The reported incidence of tuberculous peritonitis among all forms of tuberculosis varies from 0.1%-0.7% worldwide [1]. Although tuberculous peritonitis remains a significant health problem in the developing world, recently there has been an increase in the number of patients diagnosed with tuberculous peritonitis in the Western world, where tuberculosis is generally rare. This is partly a result of an increasing number of immigrant and HIV patients [1, 2]. Tuberculosis can spread to the peritoneum through the gastrointestinal tract via mesenteric lymph nodes or directly from the blood, lymph, and fallopian tubes [1]. In previous reports, tuberculous peritonitis was shown to mimic pelvic or intra-abdominal malignancies [1-6]. The diagnosis of this disease is difficult, and therefore, laparoscopy is performed in many cases [1-6].
We present a case of a 32-year-old female patient with tuberculous peritonitis mimicking peritoneal cancer.
A 32-year-old female without a past medical history of interest developed general fatigue, weight loss, and diarrhea 3 months prior to admission to our hospital. She was referred to us from the Department of Internal Medicine and Gynecology of the previous hospital because of persistent symptoms. Although various tests including computed tomography (CT) and bacterial culture tests were performed, the diagnosis was not established. Therefore, she was referred to the Departments of Internal Medicine, Surgery, and Gynecology in our hospital to diagnose her abdominal disease, suspecting peritoneal cancer.
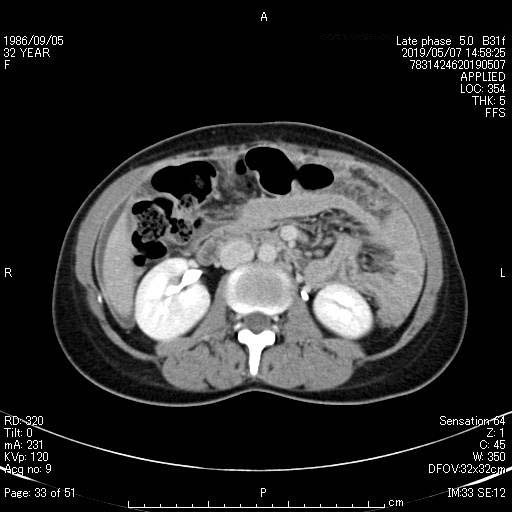
She underwent a general examination: her vital signs were normal and she had no fever. Upon abdominal examination, although the patient had slight abdominal tension, the abdomen was soft and there was no tenderness. No other symptoms such an abdominal pain, nausea, or hematochezia were observed. Laboratory investigations showed inflammatory findings (white blood cell count: 3,000 µL; CRP: 2.03 mg/dL; adenosine deaminase (ADA): 66.3 U/L). No other remarkable laboratory findings were found. CT examination of the abdomen and chest demonstrated a thickened peritoneum and ascites without bilateral adnexal masses (Figure 1). Tumor markers were as follows: CA125: 566 U/mL, CEA: 0.8 ng/mL, and CA19-9: 2 U/mL. Cytological examination of her cervix and ascites showed no abnormalities. The colon fiberscopy and photo gastroscopy examination was negative. Peritoneal cancer was initially considered the most likely diagnosis.
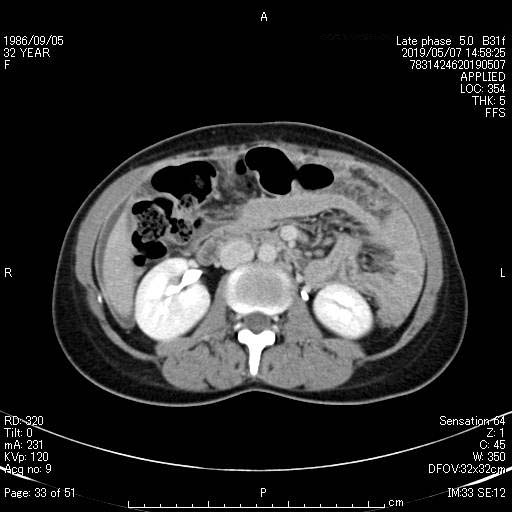 Figure. 1.
Figure. 1.— Computed tomography (CT) scan of the abdomen, which demonstrated a thickened peritoneum and ascites without bilateral adnexal masses.
The patient subsequently underwent an exploratory laparoscopy. Macroscopically, there was a moderate amount of yellow serous ascites in the peritoneal cavity. There was thickening of the peritoneum and whitish miliary nodules (< 5 mm) scattered throughout the abdominal cavity including the surface of the uterus and adnexa (Figure 2). Pathological examination of the frozen resected specimen of the nodule showed an epitheloid granuloma. At this time, we diagnosed the patient as having tuberculous peritonitis, and no further surgery was performed.
 Figure. 2.
Figure. 2.— Laparoscopic image, which revealed a thickened peritoneum and whitish miliary nodules scattered throughout the abdominal cavity.
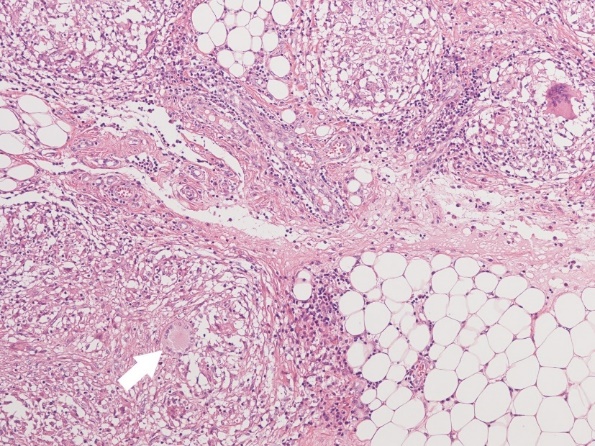
Finally, the pathological examination showed an epitheloid granuloma with epitheloid cells and multinucleated giant cells (Figure 3). We confirmed the diagnosis of tuberculous peritonitis, which was established postoperatively. At 2 weeks after the operation, the patient received anti-tuberculosis treatment, including rifampicin (RIF) 450 mg/day, pyrazinamide (PZA) 1,000 mg/day, isoniazid (INH) 200 mg/day, and ethambutol (EMB) 750 mg/day. To date, 2 months after the operation, the patient is alive with no evidence of symptoms. Serum CA125 levels also decreased significantly to 58 U/mL within 1 month after beginning treatment.
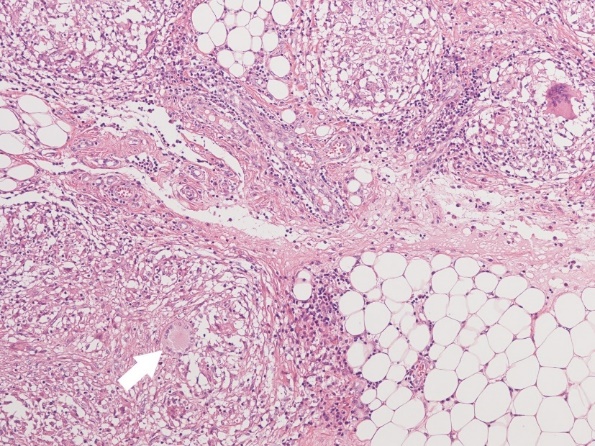 Figure. 3.
Figure. 3.— Microscopic biopsy image of tumor cells, showing an epitheloid granuloma with epitheloid cells and multinucleated giant cells (arrow) (× 400).
Peritoneal tuberculosis continues to be a significant health problem in developing countries [1-6]. In addition, the incidence of peritoneal tuberculosis in developed countries is on the rise and is mainly observed in patients with immunodeficiency associated with drug abuse, steroid therapy, alcoholism, chemotherapy, and HIV [1]. A rapid and accurate diagnosis can significantly decrease patient morbidity and mortality [1-3].
Serum CA125 is considered as a useful marker of peritoneal cancer [1-3]. CA125 was detected using immunohistochemical staining of peritoneal cancer cells and activated mesothelial cells in the pleura, pericardium, and peritoneum. Elevated CA125 levels have been seen in patients with tuberculosis-associated pleural effusion, pericardial effusion, and ascites [2]. Elevated CA125 levels may be considered as a nonspecific marker of peritoneal inflammation. In our case, imaging demonstrated a thickened peritoneum and ascites without bilateral adnexal masses as well as an elevated serum CA125 level. Thus, peritoneal cancer was initially considered the most likely diagnosis. The cytological examination of ascites showed no abnormality, which suggested the possibility of other peritoneal diseases. Therefore, we performed an exploratory laparoscopy to make an accurate diagnosis, which was established postoperatively.
There are previous reports that concluded that serum CA125 is useful in monitoring response to anti-tuberculosis treatment [2-4]. In our case, the patient received anti-tuberculosis treatment, including RIF, PZA, INH, and EMB, and the patient remained alive with no evidence of symptoms. Serum CA125 levels also decreased significantly within 1 month after beginning treatment. Serum CA125 levels may be a potential marker for monitoring disease status of peritoneal tuberculosis following treatment.
Peritoneal tuberculosis may present with nonspecific signs and symptoms such as ascites, abdominal pain, and distension, similar to a pelvic or intra-abdominal malignancy [3]. Although tuberculous peritonitis can sometimes be diagnosed clinically or radiologically, there is no single, rapid, and effective diagnostic method [2]. Peritoneal tuberculosis should be considered in the differential diagnosis of a patient with peritonitis with adnexal masses, omental caking, ascites, and elevated serum CA125. Acid-fast staining and special cultures of the ascites for Mycobacterium (M.) tuberculosis are frequently negative, and confirmation of the diagnosis requires a laparoscopic biopsy with frozen section pathological evaluation, which could spare a significant number of patients from unnecessary extensive surgery [1]. In our case, acid-fast staining and cultures of the ascites for M. tuberculosis were negative. A laparoscopic biopsy with frozen section evaluation was required to make the diagnosis, which was the only surgery necessary.
In conclusion, if peritoneal cancer is suspected in patients without abnormal cytology of the ascites, early exploratory laparoscopy should be performed to rule out tuberculous peritonitis in the differential diagnosis of patients with peritoneal cancer.
Written informed consent was obtained from the patient for publication of this case report.
Thanks to all the peer reviewers and editors for their opinions and suggestions.
The authors declare no conflict of interest.