
 , E. Nakamura 3, K. Murakami 1, M. Ono 1, A. Nozawa 1, S. Kitamura 1, K. Sengoku 2
, E. Nakamura 3, K. Murakami 1, M. Ono 1, A. Nozawa 1, S. Kitamura 1, K. Sengoku 21 Department of Obstetrics and Gynecology, Nayoro City General Hospital, Nayoro, Japan
2 Department of Obstetrics and Gynecology, Asahikawa Medical University, Asahikawa, Japan
3 Department of Pediatrics, Nayoro City General Hospital, Nayoro, Japan
Abstract
Red blood cell alloimmunization during pregnancy causes hemolytic disease of the fetus and newborn. While alloimmunization in pregnancy is treatable with anti-D antibodies, management with other antibodies has not been studied. A 32-year-old woman had anti-E antibodies detected during pregnancy, but the titer was < 1 : 2. Her newborn was admitted to hospital because direct Coombs tests were positive. Low titers of maternal anti-E antibodies were found in the newborn. We performed phototherapy and administered intravenous immunoglobulin because the newborn showed early jaundice and hyperkalemia, which suggested hemolytic disease. After being discharged at 6 days of age, the baby was readmitted to hospital at 9 days because of recurrent jaundice and underwent phototherapy. The baby was later discharged without recurrence of jaundice. Low anti-E antibody titers in pregnancy can cause alloimmunization, which can be treated successfully. The potential risk of hemolytic disease should be considered in cases with such low titers.
Keywords
- Alloimmunization
- Anti-E antibody
- Hemolytic disease of the fetus and newborn
- Pregnancy
- Rho(D) immunoglobulin.
Red blood cell alloimmunization in pregnancy can cause hemolytic disease of the fetus and newborn (HDFN) [1]. Management of alloimmunization in pregnancy with anti-D antibody has been well studied [2]. However, management of pregnancies with antibodies other than anti-D has not been studied. The most commonly encountered irregular antibody other than anti-D is anti-E [1, 3-7]. Patients with anti-E alloimmunization rarely show severe clinical presentation because the anti-E antibody has lower immunogenicity than anti-D, anti-c, and anti-Kell antibodies [5].
A critical titer of antibodies associated with the possibility of causing HDFN can be useful for predicting anti-D alloimmunization and a low titer of anti-D antibody can be of clinical significance [2]. Generally, for antibodies other than anti-D, low antibody titers are not clinically significant. We report a case of anti-E alloimmunization in a pregnancy with a low antibody titer.
A 32-year-old-woman (gravida 3, para 2) had no history of blood transfusion. Anti-E antibodies, identified as immunoglobulin type G, were detected during her second pregnancy, but the titer was < 1 : 2. Severe jaundice did not occur in her previous baby. She presented to our hospital and underwent screening tests at 12 weeks of gestation in her next pregnancy. An indirect Coombs test was positive and anti-E antibodies with an unchanged titer were detected. The titer was monitored every 8 weeks, and it increased to 1 : 4 at 34 weeks of gestation but did not increase after delivery. Middle cerebral artery peak systolic velocity (MCA-PSV) at 22 and 32 weeks of gestation was below 1.5 multiples of the median (MoM). Fetal growth was within the normal range and no anomalies were detected. At 37 weeks and 1 day of gestation, the patient delivered a female baby weighing 2,948 g with Apgar scores of 8 at 1 min and 9 at 5 min.
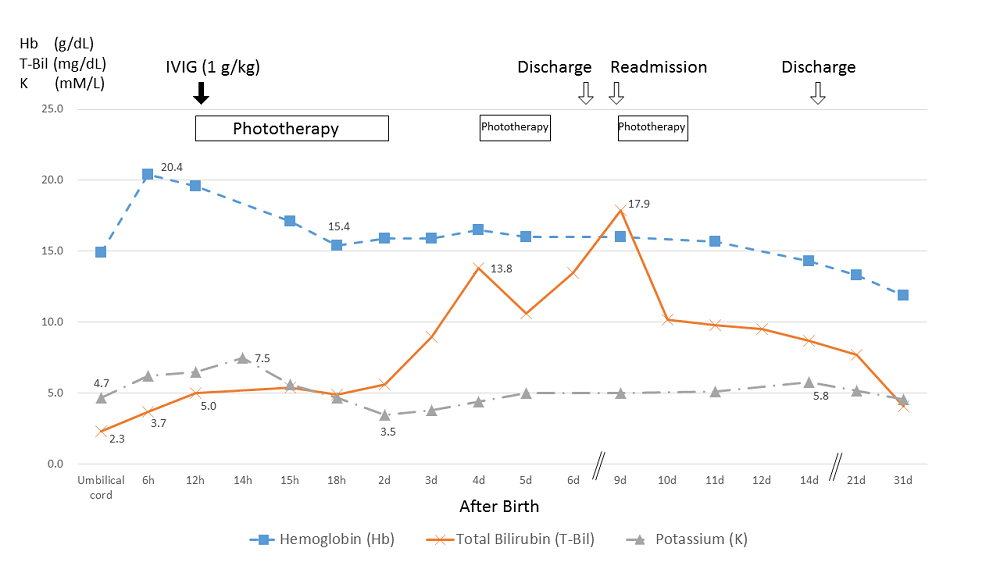
The newborn was admitted to hospital because direct Coombs tests were positive for umbilical cord blood and at 6 h after birth. The antibody elution technique showed that the baby carried maternal anti-E antibodies. We performed early treatment using phototherapy and intravenous Rho(D) immunoglobulin because the neonate showed early jaundice and hyperkalemia, which indicated hemolytic disease (Figure 1). Anemia, elevated reticulocyte counts, and erythrocyte enzymes were not detected. Administering Rho(D) immunoglobulin rapidly decreased the potassium level. The baby was discharged at 6 days of age. However, at 9 days, she was readmitted and underwent phototherapy for recurrent jaundice. The anti-E antibody titers were 1 : 2 and < 1 : 2 at 11 and 14 days of age, respectively. The baby was discharged again at 14 days of age and had a good course of recovery without any recurrence of the jaundice.
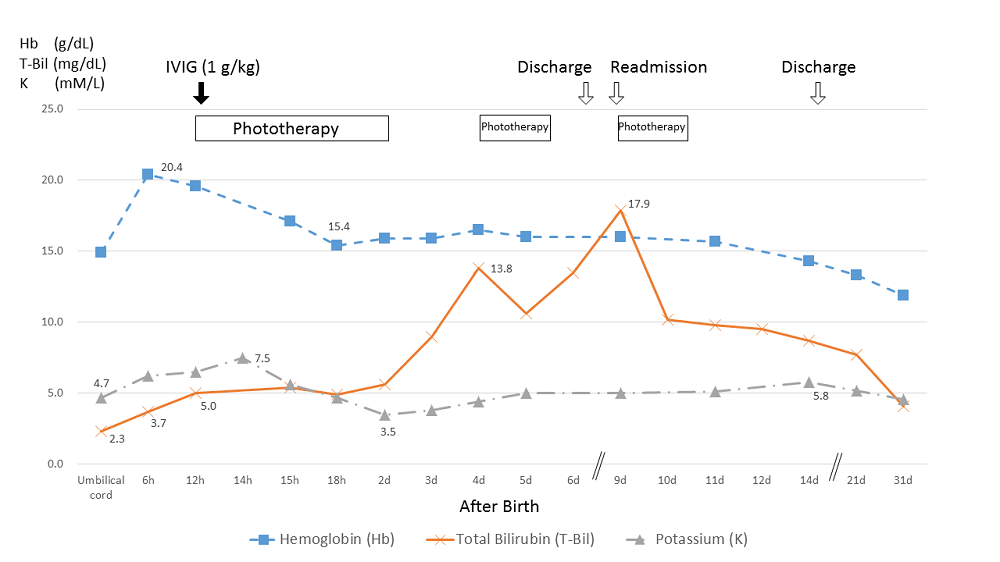 Figure 1.
Figure 1.— Neonatal clinical course and treatment regimen showing changes in hemoglobin, total bilirubin, and potassium levels. IVIG, intravenous immunoglobulin therapy
In this case, a pregnancy with a low titer of anti-E antibody led to alloimmunization. For anti-D antibodies, the guidelines of the American College Obstetricians and Gynecologists (ACOG) state that a critical titer is associated with a significant risk for severe erythroblastosis and hydrops, and critical titers in most centers are between 1 : 8 and 1 : 32 [2]. However, the critical titers of antibodies other than anti-D are controversial. Two studies on anti-E alloimmunization in pregnancy have been performed. One, by Moran et al., included 122 pregnancies complicated by anti-E alloimmunization [8]. They reported that the anti-E titer was poorly correlated with the severity of HDFN because some pregnancies with 1 : 1 of the maximum titer caused severe HDFN. Another study of 283 pregnancies by Joy et al. reported no cases of hydrops or fetal death in pregnancies with titers of less than 1 : 32 [9]. Therefore, that study suggested that the critical titer is 1 : 32. In another study, although the antigen type was different from anti-E, the authors recommended that pregnancies complicated by anti-Kell alloimmunization with titers greater than or equal to 1 : 2 should be closely monitored by ultrasonography [10]. This was recommended because there was no correlation between anti-Kell antibody titer and the severity of HDFN [10].
Management of pregnancies with anti-E alloimmunization is not clear. However, the ACOG guidelines state that care of pregnant women with irregular antibodies to one of the clinically significant minor antigens should be similar to the care of anti-D alloimmunized pregnant women [2]. If the critical titer of anti-D antibody is 1 : 8 or less, the pregnancy should be monitored with assessment of titers every 4 weeks. If the titer increases to greater than 1 : 8, ultrasonography and Doppler blood flow analysis, especially measurement of MCA-PSV, should be performed periodically. MCA-PSV results > 1.5 MoM can identify moderate and severe fetal anemia noninvasively [11, 12]. Therefore, this method has been used widely to diagnose HDFN. Although only phototherapy is required to treat mild cases of HDFN, moderate or severe cases of HDFN require intravenous Rho(D) immunoglobulins or exchange transfusion [13, 14]. In this case, the baby had a good outcome thanks to the rapid application of phototherapy and intravenous Rho(D) immunoglobulins.
Low titers of anti-E antibodies in pregnancy can cause alloimmunization. Although a critical titer of irregular antibodies can be useful clinically, the potential risk of hemolytic disease must be considered, even if low titers are present.
All subjects gave their informed consent for inclusion before they participated in the study. The study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the Ethics Committe of Asahikawa Medical University (approval number: 16231).
We thank James Cummins, PhD, from Edanz Group for editing a draft of this manuscript.
The authors declare no conflict of interest.