

1 Department of Obstetrics and Gynecology, Taipei Medical University Hospital, 11031 Taipei, Taiwan
2 Department of Internal Medicine, Taipei Medical University Hospital, 11031 Taipei, Taiwan
3 Department of Obstetrics and Gynecology, School of Medicine, College of Medicine, Taipei Medical University, 11031 Taipei, Taiwan
4 Center for Reproductive Medicine, Taipei Medical University Hospital, 11031 Taipei, Taiwan
†Contributed equally.
Abstract
Acute fatty liver during pregnancy (AFLP) is an emergency and potentially fatal condition occurring during the peripartum period. It is characterized by fatty microvascular infiltration of hepatocytes and has an incidence rate of approximately one in 7,000 to one in 20,000 pregnancies. It may induce profound liver failure and can be accompanied by renal failure, polydipsia/polyuria, disseminated intravascular coagulation, hypoglycemia, and encephalopathy. Emergency delivery at the appropriate time is crucial to control the development of AFLP. Gestational diabetes insipidus (GDI) is another rare disorder characterized by polyuria, polydipsia, and dehydration. It has an incidence rate of 2-4 cases/100,000 pregnancies and develops during the third trimester. Here the authors present the case of a patient with AFLP and transient GDI complicated with non-reassuring fetal status. The conditions were resolved after delivery and multidisciplinary intensive care.
Keywords
- Acute fatty liver during pregnancy
- Deamino arginine vasopressin
- Fetal distress
- Gestational diabetes insipidus
- Pregnancy complications
Acute fatty liver during pregnancy (AFLP) is a rare but potentially life-threatening complication that occurs during the third trimester or early postpartum period. It is characterized by fatty microvascular infiltration of hepatocytes with progressive loss of liver function [1]. Although the cause of AFLP is not entirely clear at present, some predisposing factors, such as primigravida, multiple gestation, history of AFLP, male fetus, and low body mass index, may play a role [1-4].
The most common initial presentations are non-specific symptoms, such as nausea or vomiting, abdominal pain, malaise, anorexia, and jaundice. These can rapidly progress to hepatic failure, hepatorenal syndrome, coagulopathy, and encephalopathy [1, 2]. In addition, transient polyuria and polydipsia due to decreased arginine vasopressin (AVP) levels may be observed, referring to as gestational diabetes insipidus (GDI) in this article.
AFLP can be defined by the Swansea criteria (Table 1), which has 100% sensitivity and 57% specificity with a positive predictive value of 85% and a negative predictive value of 100% [2, 5]. Patients are considered to be “positive” if at least six out of the 14 criteria are met. These criteria are used in the absence of other diagnoses of liver dysfunction, such as hemolysis, elevated liver enzymes, and low platelet count (HELLP) syndrome and preeclampsia, thereby creating challenges if clinical conditions overlap.
| Vomiting |
|---|
| Abdominal pain |
| Polydipsia/polyuria |
| Encephalopathy |
| Elevated bilirubin (>0.8 mg/dL) |
| Hypoglycemia (<72 mg/dL) |
| Elevated uric acid (>5.7 mg/dL) |
| White blood cell count (>11×10 3/µL) |
| Ascites or “Bright liver” on ultrasound |
| Elevated transaminases (aspartate aminotransferase or alanine aminotransferase >42 IU/L) |
| Elevated ammonia (>47 μ mol/L) |
| Renal impairment (creatinine >1.7 mg/dL ) |
| Coagulopathy (prothrombin time >14 s or activated partial thromboplastin time >34 s) |
| Microvesicular steatosis on liver biopsy |
Imaging findings, such as on abdominal ultrasound, computed tomography, and magnetic resonance imaging, may support the diagnosis, but such images are not required for the diagnosis [2]. A liver ultrasound may show non-specific changes, including fatty infiltration or brightness. Although a liver biopsy can make a definite diagnosis of AFLP, it is too invasive to be routinely performed [2, 5]. Early diagnosis and treatment decreased the risk of life-threatening consequences for the mother and fetus. Prompt delivery is thought to effectively improve prognosis [1, 5].
Another complication of pregnancy is GDI, which is characterized by polydipsia and hypotonic polyuria. GDI has an incidence of approximately four cases for every 100,000 pregnancies [6]. It is thought to be caused by decreased AVP levels secondary to excessive vasopressinase activity [7]. Vasopressinase is a placental enzyme that degrades both AVP and oxytocin [6] but not deamino-Cys 1,D-arg 8-vasopressin (dDAVP) [8], which is a synthetic form of endogenous AVP with a different N-terminal. Although AVP levels increase during pregnancy to maintain sufficient antidiuretic activity, vasopressinase levels from the placenta may increase as well, thereby resulting in a decreased renal effect; this increase is the main cause of subclinical diabetes insipidus [6]. However, in pregnant women with impaired liver function (such as AFLP, preeclampsia, or HELLP syndrome), the clearance of vasopressinase may be reduced, thereby unmasking the subclinical diabetes insipidus and further predisposing the patient to the severity of the disease [6, 7, 9].
Currently, the use of dDAVP in symptomatic cases has been proven to be safe for the mother as well as the fetus during pregnancy [3, 6, 9, 10].
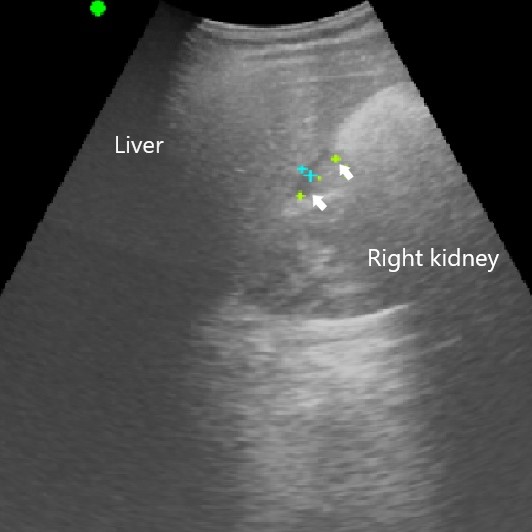
Here the authors report the case of a 35-year-old Chinese primigravida at 33 weeks of twin gestation who was admitted because of vaginal bleeding, regular uterine contraction, and short cervical length. Her previous prenatal examination was normal, and she had no history of gestational diabetes mellitus, hypertension, or diabetes insipidus. Her family history was unremarkable for endocrinopathies and liver diseases. As a tocolytic agent, she was initially given MgSO4 and subsequently atosiban. Her blood pressure remained normal during hospitalization. On day 5 after admission, she began to complain of feeling extremely thirsty with a urine output of 5700 mL in one day. She denied having nausea, vomiting, fever, or abdominal pain. At that time, her serum electrolytes and complete blood count were within normal ranges. However, one day later, she presented with vaginal bloody discharge, aggravated polydipsia, polyuria (a urine output of 6,060 ml in one day), dysgeusia, and right upper quadrant pain. Laboratory investigations reported the following results (normal ranges are presented in parentheses): white blood cell count 15,590/µL (4,000-11,000); platelet count 196,000/µL (130,000-400,000); prothrombin time 19.4 s (11-14.5), fibrinogen level 187 mg/dL (200-400), D-Dimer level 7.3 µg/mL (< 0.5), sodium level 169 mEq/L (135-147), potassium level 3.7 mEq/L (3.5-5.1), C-reactive protein level 0.87 mg/dL (< 0.5), lactate dehydrogenase (LDH) level 1,080 IU/L (<250), aspartate transaminase (AST) level 654 U/L (5-42), alanine transaminase (ALT) level 375 U/L (5-45), glucose level 94 mg/dL, albumin level 3.3 g/dL (3.5-5.2), total bilirubin level 2 mg/dL (0.20-1.0), blood urea nitrogen (BUN) level 19.7 mg/dL (6.0-20.0), creatinine level 1.2 mg/dL (0.5-0.9), and uric acid level 10.9 mg/dL (2.4-5.7). Urinalysis showed the following results: specific gravity 1.004, pH 5.5, and urine protein level <10 mg/dL. The urinary and plasma osmolality were 121 and 329 mOsm/L, respectively. To treat the patient’s developing signs of water intoxication, dDAVP was prepared if the urine output, which was measured every eight hours, which was >1,000 mL. During this time, several episodes of late deceleration of fetal heart rate tracings were noted. Therefore, an emergency cesarean delivery was indicated for maternal acute liver failure, renal dysfunction, and non-reassuring fetal status. Two living babies weighing 1,992 and 1,686 grams with Apgar scores of 6-8 and 5-8, respectively, were delivered. Uterine square sutures were performed to repair the uterine atony that occurred during surgery. To further assess the hepatic disorders, an abdominal ultrasound was performed during the puerperium; the findings demonstrated diffuse heteroechogenicity, moderate fatty change of the liver parenchyma, and a small amount of ascites (Figure 1). Anti-HAV, anti-HCV, antinuclear antibody, and anti-ds DNA were evaluated, and all displayed negative results. Postnatally, the patient experienced coagulopathy, hypoglycemia, hyperbilirubinemia, leukocytosis, and hypernatremia. By postnatal day 5, low hemoglobin levels were noted following the administration of blood products. Under the impression of persistent coagulopathy and possible oozing bleeding of the uterus, transarterial embolization was indicated. After multidisciplinary intensive care, renal function, and electrolyte levels had almost normalized by postnatal day 3. The patient’s liver impairment was resolved by postnatal day 16.
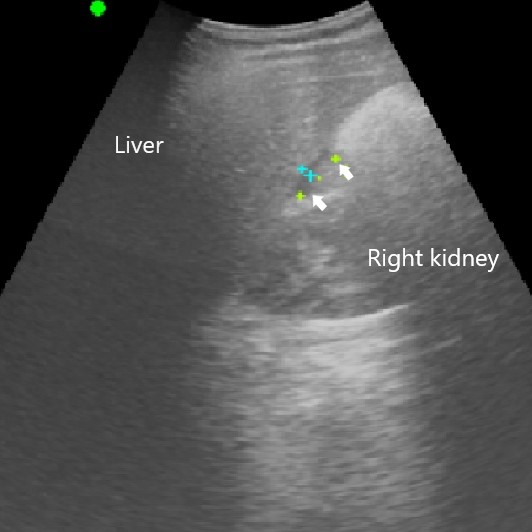 Figure 1.
Figure 1.— Diffuse heteroechogenicity, moderate fatty change of the liver parenchyma, and a small amount of ascites (arrows).
A state of aggravated polydipsia and polyuria was first noted in the present patient. Therefore, the authors performed serum and urine analyses that assessed complete blood count, serum electrolyte levels, plasma and urine osmolality, serum glucose level, liver enzyme levels, serum creatinine level, BUN, and bilirubin level. Physical examination revealed mild right upper quadrant tenderness. They referred to the Swansea criteria as the diagnostic tool for AFLP; additionally, GDI was indicated on the basis of urine osmolality measurement. Several episodes of late deceleration of the fetal heart rate were also noted on the day after the patient’s symptoms first appeared. This may be attributed to reduced placental exchange or, as deduced in this study, may be associated with maternal dehydration related to insufficient fetal blood oxidation. Although maternal survival rates in patients with AFLP have improved over the past 30 years owing to early diagnosis and treatment, fetal mortality remains high (ranging from 7% to 58%) [4]. This may be related to maternal acidosis, which has deleterious effects on the fetus, and the general complications of prematurity [2].
Previous studies have reported that the causes of AFLP may be related to increased estrogen, fatty acid metabolism disturbance, or mitochondrial dysfunction [11]. Fetal long-chain 3-hydroxyacyl CoA dehydrogenase deficiency accounts for approximately 20% of AFLP cases [12]. Long-chain 3-hydroxyacyl CoA dehydrogenase (LCHAD) is one of the enzymes involved in the beta-oxidation of fatty acids in mitochondria [2]. In fetuses with LCHAD deficiency (autosomal recessive defect), the levels of the intermediate products of fatty acid metabolism increase, and can accumulate in the maternal blood and placenta, thereby harming maternal hepatocytes [2]. Histologically, fatty microvascular infiltration of hepatocytes is a key characteristic of AFLP. Given the impaired liver function, the clearance of vasopressinase is reduced, thereby resulting in decreased AVP levels in patients with AFLP.
Differential diagnoses for this condition are difficult because of its similarities with other liver dysfunctions. Some studies have reported that AFLP may be part of the spectrum of pre-eclampsia and HELLP syndrome [1-3]. However, in the present case, AFLP was diagnosed given the patient’s coagulopathy despite normal platelet count and blood pressure and hypoglycemia; liver biopsy was not performed for the precise diagnosis because it is too invasive. On the other hand, detailed history taking is essential in the differential diagnosis of polyuria. Primary polydipsia, head trauma, and drug ingestion (such as lithium, mannitol, diuretics, SGLT2 inhibitors, and anticholinergic drugs) should be considered [6]. Other conditions that could result in solute diuresis, such as hyperglycemia, resolution of azotemia, and excess use of sodium-containing intravenous fluid, should also be assessed. If hypernatremia and low urine osmolality (< 700 mOsm/d) are simultaneously present, the patient may have central or nephrogenic diabetes insipidus. Nephrogenic diabetes insipidus can be ruled out if the urine osmolality increases after dDAVP administration.
Prompt delivery in the safest manner possible in patients with AFLP is thought to reduce the mortality and morbidity of the mother as well as the fetus, particularly when the patients have other complications, such as renal dysfunction, diabetes insipidus, coagulopathy, and non-reassuring fetal status [5]. Supportive treatment and dDAVP should also be administered if necessary.
The use of dDAVP during pregnancy is increasing [10]. In the present patient, hypernatremia rapidly improved after the emergency cesarean delivery, and her oral water intake and urine output normalized, indicating that fluid balance was established. Therefore, dDAVP was not used in this case. Although there are many case reports describing patients with AFLP and GDI, to the best of the present authors’ knowledge, this is the only case that describes this condition complicated with non-reassuring fetal status. Emergency delivery at the appropriate time and suitable supportive care before the development of further complications are the optimal management strategies.
The authors are grateful to the colleagues of Department of Obstetrics and Gynecology, Taipei Medical University Hospital, for their useful suggestions.
The authors declare no competing interests.