






Clinical and Experimental Obstetrics & Gynecology (CEOG) is published by IMR Press from Volume 47 Issue 1 (2020). Previous articles were published by another publisher on a subscription basis, and they are hosted by IMR Press on imrpress.com as a courtesy and upon agreement with S.O.G.
 , S. Mantegna 1, M. Farina 1, O.E. Gallo 1, C. Pini 1, E. Tinacci 1, P.L. Cherchi 1, S. Dessole 1
, S. Mantegna 1, M. Farina 1, O.E. Gallo 1, C. Pini 1, E. Tinacci 1, P.L. Cherchi 1, S. Dessole 11 Gynecologic and Obstetric Clinic, Department of Surgical, Medical and Experimental Sciences, University of Sassari, Sassari, Italy
Abstract
Purpose of Investigation: To evaluate technique, advantages, and limits of saline infusion sonography (SIS) in assessment of endometrial, subendometrial, and myometrial pathologies. Materials and Methods: A detailed literature research on MEDLINE, Cochrane library, EMBASE, NLH, ClinicalTrials.gov, and Google Scholar databases was done up to December 2017 restricted to English articles regarding SIS, technique, advantages, and limits. The keywords used for this review were: sonography, ultrasonography, hydrosonography, hysterosonography, saline infusion sonography, and sonohysterosalpingography (sono-HSG) with foam instillation (HyFoSy) versus saline solution (HyCoSy) in the evaluation of tubal patency. Original articles, reviews, and meta-analyses were included. Results: SIS has acquired an important role in the diagnostic work-up of abnormal uterine bleeding (AUB). SIS can be considered as an alternative diagnostic modality to hysteroscopy in detecting endometrial polyps and uterine submucosal leiomyomas. SIS is performed before the beginning of the assisted conception to evaluate the uterine cavity and exclude intracavitary pathologies, such as fibroids and endometrial polyps that could hinder the assisted fertilization procedure. SIS has a similar sensitivity and specificity for tubal patency as hysterosalpingography (HSG), without the inconvenience and potential hazards of HSG, such as possible iodine-based sensitivity to the radiopaque dye and exposure to radiations. Two-dimensional (2D) SIS is already very accurate, therefore both 2D SIS and threedimensional (3D) SIS should be considered alternatives to diagnostic hysteroscopy when intracavitary pathology is suspected in subfertile women and in those with AUB. Conclusions: SIS is a technique indicated in premenopausal and postmenopausal women with abnormal vaginal bleeding and is also a valid procedure for initial outpatient screening in infertility.
Keywords
- Sonography
- Ultrasonography
- Hydrosonography
- Hysterosonography
- Saline infusion sonography
- Sonohysterosalpingography (sono-HSG) with foam instillation (HyFoSy)
- Hysterosalpingo-contrast sonography (HyCoSy)
- Tubal patency
Saline infusion sonography (SIS) is a technique in which a catheter is placed into the endometrial cavity and sterile saline solution is instilled into the uterine cavity to enhance endometrial and myometrial visualization during transvaginal ultrasonography (TVUS) [1-2]. SIS is indicated in postmenopausal women with abnormal vaginal bleeding, to distinguish bleeding caused by atrophy (the most common reason of bleeding in this age group), from anatomic lesions such as polyp, myoma, hyperplasia, and carcinoma [3]. SIS is also indicated in premenopausal women with abnormal uterine bleeding (AUB) and in patients with recurrent pregnancy loss to rule out congenital uterine anomalies. In fact, SIS can be a valuable test in the evaluation of female infertility. It is a safe procedure for the study of uterine cavity with no risk of dissemination of tumoral cells into abdominal cavity in cases of endometrial carcinoma [4]. SIS shows very accurately postpartum residual trophoblastic tissue [5]. This article reviews the literature on technique, advantages and limits of SIS. Synonymous are Saline contrast sonohysterography (SCSH), sonography, ultrasonography, hydro-sonography, hysterosonography, and sonohysterosalpingo-graphy.
SIS must be performed in the follicular phase of the menstrual cycle, after cessation of menstrual flow and before day 10, because the endometrium is thin at this time in the cycle [6]. Bleeding is not a contraindication to SIS; however, the presence of blood clots within the endometrial canal can make interpretation more difficult [6-8]. Anesthesia or analgesia are not required, usually patients tolerate the procedure quite well and antibiotic prophylaxis is not necessary [8]. The procedure is explained to the patient, including the low risk of increased bleeding, as well as the even lower risk of infection [8]. The patient should be placed in the lithotomy position. Initially, the patient undergoes routine TVUS with full evaluation of the uterus, endometrial stripe, and adnexa. A brief bimanual examination can aid in locating the cervix. Sterile technique is preferable to prevent endometritis and other infections [8]. A speculum is inserted into the vaginal introitus. The cervical os is localized and cleaned with a povidoneiodine solution or chlorhexidine gluconate. The catheter is then inserted through the cervical os into the cervical canal or uterine cavity if tubal patency should be studied [8]. The balloon tip is inflated with 1-2 mL of saline solution, depending on patient comfort, to help hold it in place. The speculum is then removed carefully to avoid dislodging the catheter. Then the vaginal probe is reinserted and a 10 mL syringe filled with sterile saline is attached to the catheter. Fluid is instilled while the transducer is moved from side to side (cornua to cornua) in a long-axis projection. The amount of instilled fluid varies, depending upon distension of the endometrial cavity as seen on the ultrasound monitor and also on patient comfort (cramps may occur). After the uterus is completely surveyed from cornua to cornua in a long-axis projection, the transducer is rotated 90 degrees into an axial plane. More fluid is instilled while fanning down toward the endocervical canal and up toward the uterine fundus to obtain a detailed survey of the endometrium (Figure 1).
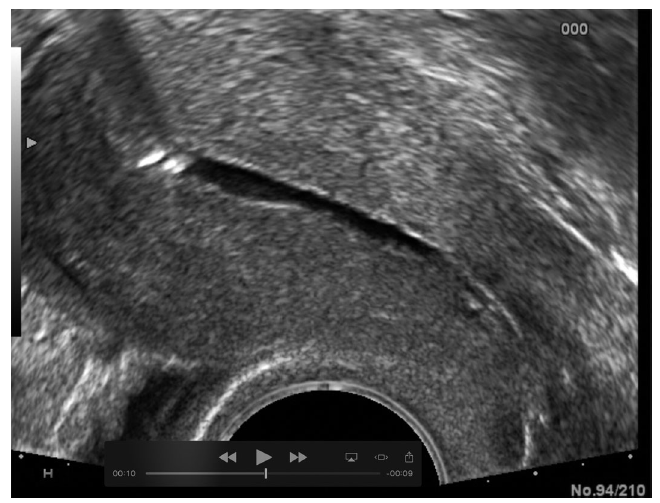 Figure 1.
Figure 1.— Normal uterine cavity under 2D SIS: sagittal scan.
Each portion of the uterine cavity should be imaged, including the cervical canal in a coronal sweep, to exclude any focal abnormality, such as polyps, myoma, hyperplasia, and carcinoma. Visualization of the endocervical canal is problematic because it is often difficult to distend this portion of the canal. Adequate visualization often requires a delicate progressive collapse of the balloon during fluid instillation into the canal and while the catheter is pulled back or passively slips out of the uterus. Color Doppler evaluation can be quite helpful to distinguish blood clots from polypoid lesions [9]. The investigation cannot be carried out in one of the following conditions: severe stenosis (obstruction of the cervical canal), which prevents the insertion of the catheter, cervical canal insufficiency due to the escape of the contrast agent through the vagina, cervical pathologies that prevent the correct insertion of the catheter (voluminous cervical polyp), pain during the pelvic examination and /or vagal reactions, vaginal blood loss, acute gynecological inflammation (vaginitis, cervicitis, endometritis), and gynecological tumors.
AUB is one of the most common gynecological conditions in women of reproductive age and is the cause of about one-third of all gynecology visits among premenopausal women and over 70% of office visits between perimenopausal and postmenopausal women. It is defined by FIGO Classification System as bleeding from the uterus corpus that is abnormal in regularity, volume, frequency or duration and occurs in the absence of pregnancy [10]. We can distinguish two main causes of AUB: “related to uterine structural anomalies” and “not related to uterine structural anomalies”.
The acronym PALM-COEIN is used to indicate the main causes of AUB (polyp, adenomyosis, leiomyoma, malignancy and hyperplasia - coagulopathy, ovulatory dysfunction, endometrium, iatrogenic, and not yet classified) [11]. AUB can be acute or chronic. Acute AUB refers to an episode of intense bleeding of severe quantity that requires immediate intervention to prevent anaemia. Medical history should include a description of the patient’s bleeding patterns, such as any recent variations in quantity, duration, frequency, and associated pain. In addition, relevant medical conditions should be sought (i.e. thyroid disease, hypertension, kidney disease, anorexia/bulimia, psychiatric conditions, and other clinical conditions) as they can contribute to ovulatory dysfunction. Any relevant family history should be discussed (i.e. bleeding disorders/coagulopathies), as well as gynecological and obstetric history. A list of drugs should also be obtained because some of these can contribute to AUB (e.g. hormones, anticoagulants/fibrinolytics, psychotropic drugs). After a careful anamnestic collection of the clinical history of the patient and blood tests that exclude problems related to coagulation, it is necessary to frame the problem through diagnostic tests. Polyps and leiomyomas are the most common pathology in these women. SIS has acquired an important role in the diagnosis of AUB, establishing itself as a complementary method to conventional TVUS in the evaluation of these cases [12].
Endometrial polyps are neoformations of the mucosa of the body of the uterus (Figure 2). The peak of incidence is between 40 and 49 years, while in reproductive age the prevalence is 20-25% [13-14]. In postmenopause the endometrial polyp is rarer. The upper third or the lower part of the endometrial cavity are mostly involved; the macroscopic colour is yellowish-red, translucent appearance with haemorrhagic, and necrotic areas. The cause of endometrial polyps is unknown. According to a study of Baiocchi et al. 2009, 3.5% of endometrial polyps may have malignant elements. Overall, the incidence of neoplasia is 3-4% [13].
 Figure 2.
Figure 2.— Endometrial polyp under 2D SIS.
Occasionally uterine contractions that attempt to expel the neoformation are associated with pelvic pain and bleeding.
TVUS sometimes allows to identify the polyp and its location inside the uterus, but SIS permits the definitive diagnosis in cases of thick endometrium; hysteroscopy is the main examination that allows visualization and removal of the polyp in the same setting [14].
Leiomyoma is a benign tumor of the smooth muscle of the uterus responsive to steroid hormones, originating from the clonal expansion of single myometrial cells (Figure 3). The uterine leiomyoma in 95% of cases is localized in the body and only rarely, approximately in 5% of cases in the uterine cervix. It has the form of a nodular knot with variable contours. Depending on the uterine layer and the site where the nodes evolve, leiomyomas can be distinguished as: subserousal - when they develop under the peritoneum that covers the uterus; sessile or pedunculated with large or with thin implantation basis, respectively, intramural - when development is within myometrium; submucousal - when they protrude into the uterine cavity, lifting the endometrial mucosa and sometimes ulcerating it; infralegamentary - when they develop between the two peritoneal pages of the wide ligament, growing inside it; cervical - if they develop in the overlying portion of the cervix.
 Figure 3.
Figure 3.— Uterine submucous leiomyoma under 2D SIS.
Histologically the constituent elements of the fibroma are in part represented by smooth muscle cells with fused nuclei with more or less abundant stroma. In subserous leiomyomas, symptomatology is almost always absent and the finding is often occasional, during a gynecologic examination. In other cases, the most frequent symptom is menorrhagia (30-40%) and sometimes also metrorrhagia, polymenorrhea, and anaemia.
Pain is not considered as one of the specific symptom of the leiomyoma [14]. The diagnostic modalities used currently include conventional TVUS, bidimensional (2D) and tridimensional (3D) SIS, hysteroscopy, and uterine curettage [15, 16]. SIS has acquired an important role in the diagnosis of AUB, establishing itself as a complementary method to conventional TVUS in the evaluation of these cases [12]. A systematic review of diagnostic studies that compared 2D- and/or 3D-SCSH with hysteroscopy and anatomopathology was conducted according to PRISMA and SEDATE recommendations [17]. This systematic review aimed to evaluate the accuracy of 2D- and 3D-SCSH in diagnosing endometrial polyps and submucosal leiomyomas in women of reproductive age with AUB. A total of 1,398 citations were identified and five studies were included in the systematic review and meta-analysis. Pooled sensitivity and specificity of 2D-SCSH in detecting endometrial polyps were 93% (95% CI, 89-96%) and 81% (95% CI, 76-86%), respectively, with pooled LR+ of 5.41 (95% CI, 2.60-11.28) and LR- of 0.10 (95% CI, 0.06-0.17). In the detection of submucosus uterine leiomyomas, pooled sensitivity and specificity were 94% (95% CI, 89- 97%) and 81% (95% CI, 76-86%), respectively, with pooled LR+ of 4.25 (95% CI, 2.20-8.21) and LR- of 0.11 (95% CI, 0.05-0.22). 2D-SCSH had good accuracy in detecting endometrial polyps and submucosus uterine leiomyomas, with areas under the summary receiver operating characteristic (SROC) curves of 0.97 ± 0.02 and 0.97 ± 0.03, respectively. In their review, the inclusion criteria led to retrieval of studies with at least 60% of the women being of reproductive age and at least 50% of the women having menstrual disorders. Among the studies included in the systematic review, all provided information that allowed the calculation of the accuracy of 2D-SCSH for the diagnosis of endometrial polyps, but only four studies provided data on submucosal uterus leiomyomas. The meta-analysis showed good accuracy of SCSH in the detection of endometrial and submucosal polyps, and uterine leiomyomas, with a higher sensitivity for the diagnosis of the latter [17]. These results demonstrated that, in women with AUB, 2D-SCSH can be considered as an alternative diagnostic modality to hysteroscopy in detecting uterine submucosal leiomyomas. Studies that analyzed the diagnostic accuracy of 3D-SCSH could not be compared due to high heterogeneity related to menopausal status, type of technique used, and primary outcome being investigation of infertility.
In the literature, there are a considerable number of studies examining the accuracy of SIS in patients with AUB, but the analyzed populations are heterogeneous, including postmenopausal women or women with infertility [18-19]. Matthews et al. [11] emphasized on the high sensitivity (96-100%) of SIS and a high negative predictive value (94%-100%) in the evaluation of the uterus and endometrium for intracavitary uterine lesions.
A systematic review conducted by Maheux-Lacroix et al. [20] has instead evaluated the diagnostic accuracy of SIS compared to TVUS in reference to histo- pathological samples obtained from hysteroscopy or hysterectomy for the diagnosis of polyps and submucousal leiomyomas in women with AUB.
From this systematic review, it can be observed that vaginal ultrasound has a low detection rate of intracavitary anomalies with particularly low sensitivity in postmenopausal women and women with polyps. In comparison, SIS has a high-quality diagnostic accuracy and a detection rate similar to hysteroscopy, though it is less specific. All three procedures are well-tolerated with few negative results and great success rates. More than one-third (37%) of intracavitary anomalies have not been identified with TVUS, sensitivity was particularly low for polyps, with almost half of them lost. The study that most closely resembles the present analysis was a systematic review by Farquhar et al. in 2003 [21] in which the primary objective was to determine the diagnostic accuracy of TVUS, SCSH, and hysteroscopy in the investigation of AUB (Figure 4).
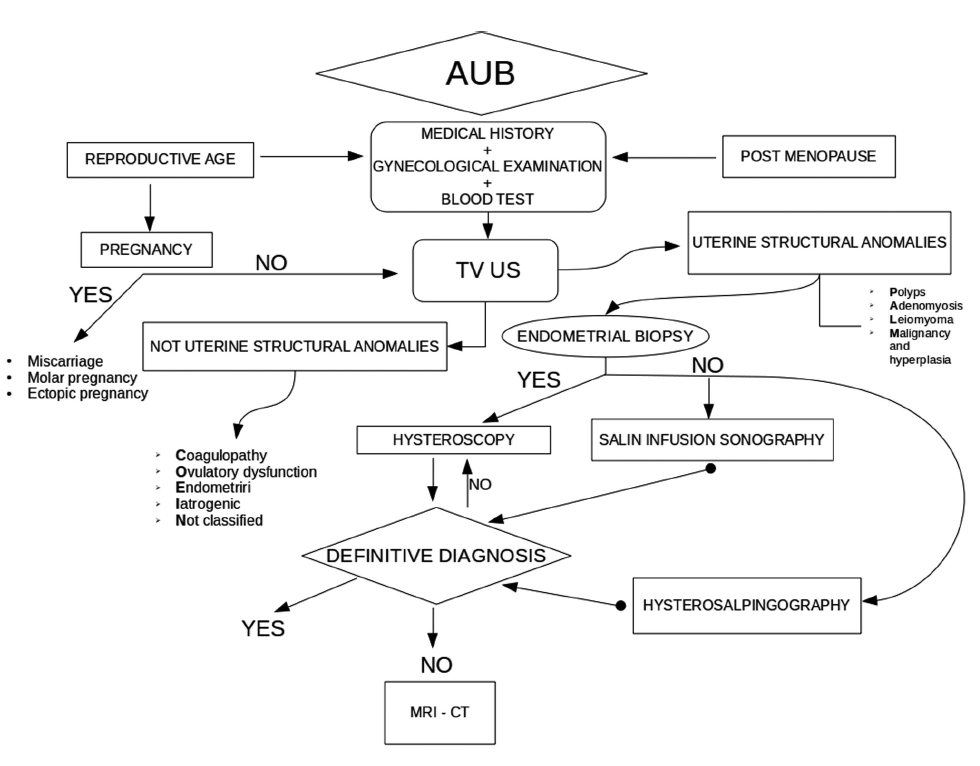 Figure 4.
Figure 4.— Care pathway for abnormal uterine bleeding (AUB).
The desire to have a child is a basal instinct in women, which guarantees the continuity of the species. Advances in medicine have revolutionized the diagnosis and treatment of infertility in the last 20 years, allowing couples 20 years ago could not have children, to become parents. In fact, since Edwards and Steptoe in 1980 had for the first time realized the fertilization of an oocyte outside the maternal environment, more and more innovative techniques have been introduced in the infertility therapy that have radically modified the prospect of a couple long-eager to get pregnant [14]. One in seven couples have difficulty in conceiving and a majority of them undergo in vitro fertilization (IVF) treatment in order to maximize their chances of becoming pregnant [22]. The most critical step for successful IVF outcome is embryo implantation, which is influenced by a positive cross-talk between an adequate quality embryo and a receptive endometrium.
A favourable uterine cavity environment influences endometrial receptivity and any uterine cavity pathologies in subfertile women can therefore interfere with the implantation process [23]. Uterine pathology is represented by: uterine leiomyoma, endometrial polyps, synechiae, and uterine malformations (uterus septum is the most frequent associated with infertility). The relationship between leiomyomas or large uterine polyps and infertility still remains controversial today. Many hypotheses have been advanced on the mechanisms by which the presence of leiomyomas or polyps can cause infertility, but none is supported by convincing evidence. However, a number of observations lead us to believe that leiomyomas can reduce fertility [24]. Approximately 40% of female infertility seems to be due to functional but especially anatomic changes of the fallopian tubes, in most post-inflammatory cases, secondary to a sexually transmitted ascending infection (Gonococcus, Chlamydia, etc.) capable of interfering with the tube-ovarian function.
Tubal pathology includes: proximal, distal occlusion, perifimbrial adhesions, and hydrosalpinx [14, 25]. SIS is performed before the beginning of the assisted conception to evaluate the uterine cavity and exclude intracavitary pathologies, such as leiomyomas and endometrial polyps that could hinder the assisted fertilization procedure; it is also a valuable aid in the study of sterile couples as a diagnostic means of control or confirmation of tubal patency in women who have already undergone other radiological examinations or surgical interventions, for the restoration of tubal patency, or for the control of tubal patency after ectopic pregnancy [14]. Obajimi and Ogunkinle [26] in their retrospective study conducted on 760 patients who had SIS prior to assisted conception, between January 2008 and December 2010, and reported that 46% of the patients had intrauterine pathologies: submucosal leiomyomas in 48.57% of the pathologies, followed by adhesions (28.57%), and endometrial polyps (22.86%). The authors then compared the results of SIS with hysteroscopy and the following were calculated for each examination: sensitivity, specificity, and positive predictive and negative predictive values, respectively. The mean age of the study group was 38.4 ± 6.70 years and the mean body mass index was 24.0 ± 3.76 kg/m2. They concluded that the diagnostic accuracy of SIS for leiomyomas and polypoid lesions was in agreement with subsequent hysteroscopy findings (sensitivity of 96% and 94%, respectively). Therefore from this study it is clear that the SIS is a useful screening tool in evaluating the endometrial cavity with its high negative predictive value for submucosal leiomyomas (96%), endometrial polyps (99%), intrauterine adhesions (95%), and it is a valid procedure to be used as an initial outpatient screening tool in infertility work (Figure 5). A systematic review and meta-analyses by Seshadri et al. [18] compared SIS with hysteroscopy, to evaluate the diagnostic accuracy in the diagnosis of intrauterine pathologies in subfertile populations. The sensitivity of hysteroscopy is considered to be nearly 100% in the literature [27-29]. However, it is an invasive procedure which may require local anaesthetic or sedation in some cases and does not allow concurrent assessment of the myometrium wall and adnexal structures [30, 31]. They considered prospective and retrospective comparative studies and randomized, case control, cohort, and cross-sectional studies. The quality assessment of the studies was carried out by using the QUADAS tool as suggested by the Cochrane handbook for diagnostic accuracy systematic reviews. From a total of 1,700 citations, 20 studies were included in the final analysis. There were 15 prospective studies and three retrospective studies, as well as two randomized studies included in the review. The pooled sensitivity of SIS in the detection of all intrauterine abnormalities was 0.88 with a 95% CI of 0.85-0.90. The pooled specificity of SIS in the detection of all intrauterine abnormalities was 0.94 with a 95% CI of 0.93-0.96. The positive and negative likelihood ratios were 20.93 (95% CI 9.06 - 48.34), and 0.15 (95% CI 0.10-0.22), respectively. The likelihood ratio of >10 indicates that the SIS result has a large effect on increasing the probability of disease presence and it is a near perfect test in discriminating normal uterus from those with intracavitary pathology. The pooled sensitivity and specificity of SIS in the detection of intrauterine polyps were 0.82 (95% CI 0.76-0.86) and 0.96 (95% CI 0.95-0.98), respectively. The positive and negative likelihood ratios were 34.66 (95% CI 8.12-147.92) and 0.22 (95% CI 0.13-0.39) The post-test probability for the detection of intrauterine polyps was 0.87 (95% CI 0.79- 0.94). The pooled sensitivity and specificity of SIS in the detection of submucousal leiomyomas were 0.82 (95% CI 0.69-0.92) and 0.99 (95% CI 0.98-1.00), respectively. The likelihood ratios were 44.14 (95% CI 17.77-109.64) and 0.26 (95% CI 0.15-0.45). The post-test probability for the detection of submucous leiomyomas was 0.95 (95% CI 0.86-1.00). The pooled sensitivity and specificity of SIS in the detection of congenital uterine anomalies were 0.85 (95% CI 0.79-0.90) and 1.00 (95% CI 0.99-1.00), respectively. The positive and negative likelihood ratios were 53.87 (95% CI 26.78-108.38) and 0.19 (95% CI 0.10- 0.35). The post-test probability in the detection of congenital uterine anomalies was 0.99 (95% CI 0.96-1.00). The pooled sensitivity and specificity of SIS in the detection of intrauterine adhesions were 0.82 (95% CI 0.65-0.93) and 0.99 (95% CI 0.98-1.00), respectively.
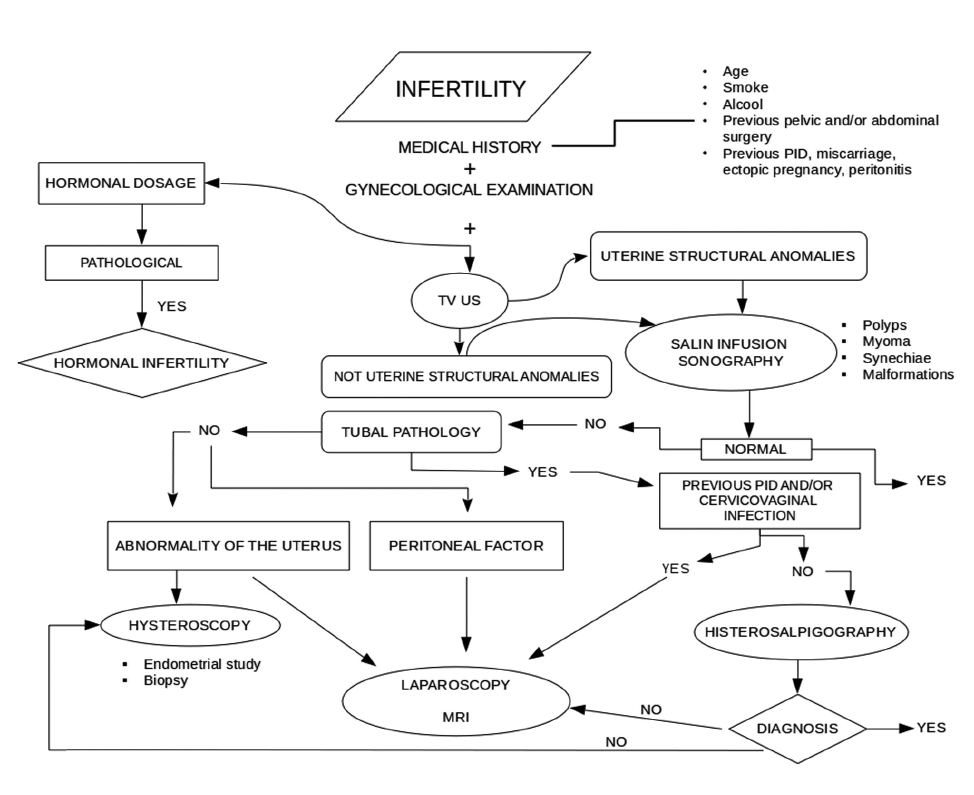 Figure 5.
Figure 5.— Care pathway for infertility work-up.
The positive and negative likelihood ratios were 34.58 (95% CI 16.68-71.70) and 0.36 (95% CI 0.22-0.58). The post-test probability in the detection of intrauterine adhesions was 0.87 (95% CI 0.75-0.99). These results showed that SIS is a highly sensitive investigative modality in the detection of intrauterine abnormalities, such as uterine polyps and submucous leiomyomas in subfertile women prior to IVF treatment, in comparison to the gold standard, hysteroscopy, and that SIS is as sensitive and specific as hysteroscopy in detection of intrauterine abnormalities (polyps, submucous leiomyomas, congenital uterine anomalies, and adhesions). Given the high prevalence of intrauterine abnormalities in subfertile women and the high diagnostic accuracy of SIS, the clinical application will be for this technique to be used as a first line screening tool in the assessment of subfertile women and reduce the need for invasive diagnostic procedures such as hysteroscopy (Figure 5).
Other procedures used in the diagnostic protocol of infertility are: hysterosalpingography (HSG), which is a radiological procedure, which allows, through the introduction of a radio-opaque contrast medium inside the cervical canal, the assessment of uterine cavity, and Fallopian tubes; magnetic resonance imaging (RMI), particularly useful for evaluating the myometrium and ovaries; laparoscopy with chromopertubation (or dye) test, accurate to diagnose the causes of tubal occlusion and to study of the pelvic peritoneum [32]
Luciano et al. [33] evaluated benefits and accuracy of hysterosalpingo-contrast sonography (HyCoSy) in the study of tubes, compared to HSG and laparoscopic cromopertubation; the sensitivity and specificity for HyCoSy in determining tubal patency compared with laparoscopic chromopertubation were 97% and 82%, respectively; the positive predictive value was 88% and the negative predictive value was 95%. The authors [33] concluded that HyCoSy had a similar sensitivity and specificity for tubal patency as HSG, without the inconvenience and potential hazards of HSG, such as possible iodine-based sensitivity to the radiopaque dye and exposure to radiations. Considering that laparoscopic chromopertubation is the gold standard, HSG and HyCoSy are equally effective in the diagnosis of tubal patency. HyCoSy is an inexpensive technique, rapid, well-tolerated, and one of the most important advantages are the possibility of obtaining information on the status of the tube and the uterus in just one investigation time. HyCoSy allows to perform a continuous real-time survey, does not require the use of irritating contrast agents and does not involve exposure to ionizing radiation (as HSG), but it is a simple TVUS and therefore it is repeatable [32]. For selected patients with tubal pathology, HyCoSy should be performed as screening and HSG should be applied in second instance only in such cases (Figure 5).
Randomised controlled trials (RCTs) and prospective cohort studies [34], conducted on a population of premenopausal and post menopausal women with AUB, performed a comparison between 2D SIS and 3D SIS, to evaluate the diagnostic accuracy of 3D SIS compared with 2D SIS in the diagnosis of focally growing lesions (presence or not) in women with AUB or subfertility; hysteroscopy was the reference test, to evaluate the diagnostic accuracy of 3D SIS compared with 2D SIS in the diagnosis of focally growing lesions (presence or not) in women with AUB or subfertility. The objective of the study was to evaluate the diagnostic accuracy of 3D SIS compared with 2D SIS according to type of abnormality for the discrimination between uterine polyps and submucous leiomyomas in women with AUB or subfertility, with hysteroscopy, and histology used as the reference. Meta-analysis revealed no statistically significant differences between 2D SIS and 3D SIS. Summary sensitivity and summary specification were higher for 3D SIS, but margins of improvement are limited because 2D SIS is already very accurate, therefore both 2D SIS and 3D SIS should be considered alternatives to diagnostic hysteroscopy when intracavitary pathology is suspected in subfertile women and in those with AUB. 3D SIS, similar to laparoscopy, is the most accurate method for the differentiation of bicornuate, septate, and arcuate uteri. There are no significant differences in diagnostic value among 3D TVS, 2D SIS, and 3D SIS or among expert 2D TVS, 3D TVS, and 2D SIS. The high diagnostic value of these ultrasonographic tools obviates the need for endoscopy in the differential diagnosis of the most common congenital uterine anomalies. The 3D SIS should be applied when the results of 3D TVS are equivocal [35]. Figure 6 shows 3D SIS in case of septate uterus.
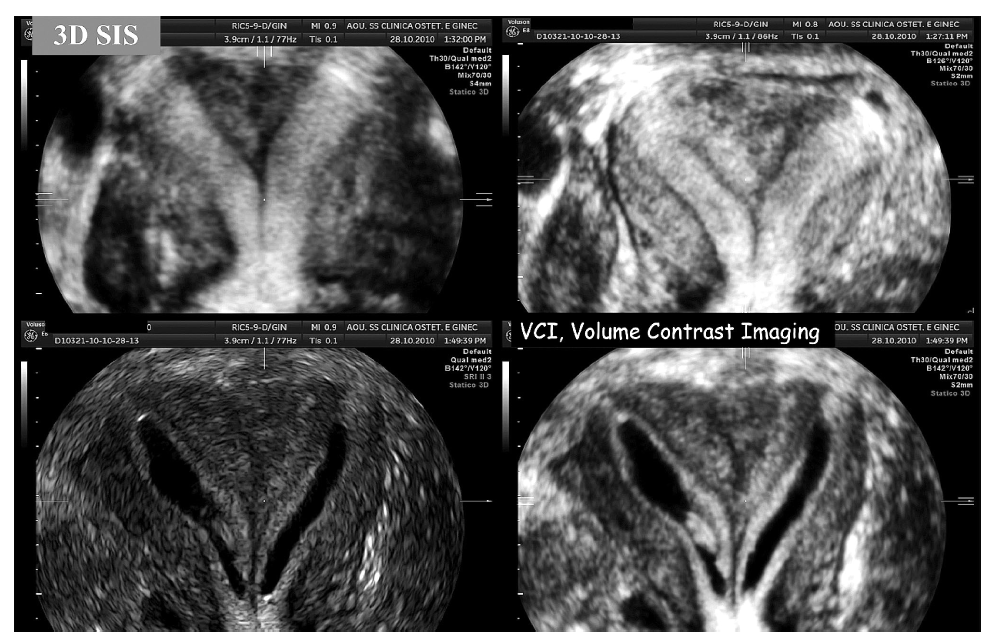 Figure 6.
Figure 6.— Uterine malformation: septate uterus on 3D SIS.
SIS is a technique indicated in premenopausal and postmenopausal women with AUB and is also a valid procedure for initial outpatient screening in infertility.
Ph. Doctor School in Biomedical Sciences, Address in Gender Medicine, Men, Woman and Child, Sassari University, Italy, supported the study.