

Clinical and Experimental Obstetrics & Gynecology (CEOG) is published by IMR Press from Volume 47 Issue 1 (2020). Previous articles were published by another publisher on a subscription basis, and they are hosted by IMR Press on imrpress.com as a courtesy and upon agreement with S.O.G.
 , P. Wang 1, T. Zou 1, Z. Zhang 1, W. Liang 1
, P. Wang 1, T. Zou 1, Z. Zhang 1, W. Liang 11 Guizhou Provincial People’s Hospital, Guiyang, China
Abstract
Immune imbalance of T cells in the maternal-fetal interface is reported to be associated with unexplained recurrent spontaneous abortion (URSA), such as Th17/Tregs/Th1/Th2 cell. The authors’ previous finding demonstrated that the percentage of Th1 cells was higher in the decidual tissues of patients with URSA. However, whether Th17 and Treg cells are altered in URSA remains unknown. In this study, the authors measured the percentage of Th17 and Treg cells by flow cytometry in 30 URSA patients and 30 normal pregnant women. They found that there were a higher proportion of Th17 and a lower number of Treg cells in the decidual tissue of URSA compared to those in normal controls. In conclusion, the results indicate that the changes in the proportion of Th17 and Treg cells in the maternal-fetal interface may be related to the occurrence of URSA.
Keywords
- Maternal-fetal interface
- Th17 cells
- Treg cells
- Unexplained recurrent spontaneous abortion
Two or more spontaneous miscarriages prior to 20 weeks is defined as unexplained recurrent spontaneous abortion (URSA) [1], occurring in 1-5% of human pregnancies [2]. In addition to chromosomal abnormalities, anatomical malformations, endocrine or infectious diseases, there is still more than 70% of patients with unknown etiology and its is referred to as URSA, which is closely associated with the immunological imbalance at the fetomaternal interface [3]. The embryo expresses paternal antigens which are foreign molecules to the mother, and may be viewed as an allograft. Whether maternal immune system can recognize and tolerate the embryo as well as its antigen may be essential for a successful pregnancy.
A previous study indicated that altered immune balance between Th1 and Th2 plays an important role in the pathogenesis of URSA with a predominance of Th1-type reactivity [4]. Consistent with this, the current authors’ previous study showed that the number of Th1 cells and the Th1/Th2 ratio were higher in URSA patients compared to normal pregnant controls [5], further supporting the role of imbalance of Th1/Th2 in the development of URSA. In recent years, Thl/Th2 might not be the only factor explaining the autoimmunity and transplantation tolerance. Physiological and pathological pregnancy might involve a more complicated molecular mechanism, such as Thl/Th2/Thl7 and Treg cells [6, 7]. However, the exact role of Th17 and Treg cells in URSA remains poorly understood.
In this study, the authors evaluated the expression profiles of Th17 and Tregs cells in patients with URSA through measuring the frequency of Th17 and Treg cells in URSA patients and normal pregnant women controls by fluorescence-activated cell sorting (FACS). The authors found that Th17 were significantly increased and Treg cells were decreased in decidual tissue in URSA patients compared with control tissue, indicating that variations in Th17 and Treg cells may be related to the pathogenesis of URSA.
A total of 30 female patients with URSA from Guizhou Provincial People’s Hospital were enrolled in this study from January 2012 to December 2015. Thirty women with normal pregnancies (no abortion, preterm birth or hypertensive disorder complicating pregnancy anamnesis) were enrolled as control subjects at the same time. Individuals with infectious, endocrine, metabolic, autoimmune or chromosomal diseases were excluded from this study. There were no significant differences in the age and weeks of gestation between the two groups. Clinical characteristics of two group women are summarized in Table 1. Informed consent was obtained prior to enrollment from all the subjects and the study was approved by the ethics committee of Guizhou Provincial People’s Hospital.
| Group | n | Age (years) | Weeks of gestation |
|---|---|---|---|
| URSA | 30 | 28.23±4.17 | 8.31±1.27 |
| Normal pregnancy | 30 | 27.67±3.92 | 7.80±1.56 |
Decidual sections (2 g) were obtained from each patient, followed by cut into small pieces (1 mm), and strained through a 50μm gauge nylon mesh. The cell suspension was used for lymphocyte purification using Ficoll reagent. After isolated, lymphocytes were harvested, washed and resuspended in phosphate buffered saline (PBS). The cell count was adjusted to 1×106/mL for flow cytometry analysis within eight hours.
For analysis of Th17, the cells were incubated with PerCP-conjugated anti-human CD4 at 4˚C for 15 minutes. After surface staining, the cells were fixed and permeabilized with BD Cytofix/Cytoperm solution and stained with fluorescein isothiocyanate (FITC)-conjugated anti-human IL-17A.
For Treg analysis, the cells were incubated with PerCP-conjugated anti-human CD4 and FITC-conjugated anti-human CD25 at 4˚C for 15 minutes. After surface staining, the cells were fixed and permeabilized with BD Cytofix/Cytoperm solution and stained with phycoerythrin (PE)-conjugated anti-human Foxp3.
All antibodies were purchased and data from the stained cells were collected using a flow cytometer (Becton-Dickinson) and analyzed by Flowjo software.
SPSS 16.0 software was used for data analysis and data are reported as means ± standard error of the mean (SE). The unpaired two-tailed Student t-test was performed to determine significant differences between two groups. P < 0.05 was considered to be statistically significant.
The total percentage of both Th17 and Treg cells analyzed by FACS analysis (Figure 1) was summarized in Table 2. It showed that the percentage of Th17 was increased and Treg cells was decreased in URSA patients compared to healthy controls, suggesting that Th17 cell responses might be enhanced in the deciduae of URSA patients.
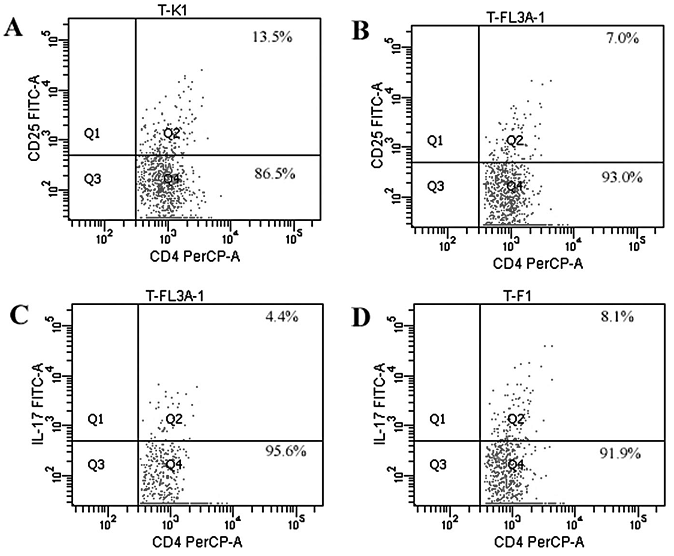 Figure 1.
Figure 1.— The percentages of Treg and Th17 cells in decidual tissues were detected by flow cytometry in URSA and in normal pregnancy. Representative flow cytometry plots of CD4+/CD25bright in normal pregnancy (A) and URSA patients (B). Representative of CD4+/IL-17+ in normal pregnancy (C) and URSA (D).
| Group | n | Treg (%) | Th17 (%) | Treg/Th17 |
|---|---|---|---|---|
| URSA | 30 | 6.93 ± 1.54* | 7.94 ± 2.21* | 0.87 ± 0.24* |
| Normal pregnancy | 30 | 13.37 ± 2.88 | 4.35 ± 1.62 | 3.07 ± 1.01 |
The maternal-fetal interface consists of placenta trophoblast and decidual tissue, and it is the area where maternal tissues come into and direct contact with the embryo. Under normal pregnancy conditions, adaptive immune responses in maternal-fetal interface are suppressed to prevent the rejection of the semi-allogeneic fetus. Therefore, the key to the success of pregnancy mainly depends on the status of the maternal-fetal interface immunological microenvironment. Once the maternal-fetal interface immune microenvironment is disrupted, abortion will take place.
Th17 cells which produce the proinflammatory cytokine, IL-17, play important roles in a variety of autoimmune diseases [8]. Normal physiological level of Th17 is to promote the embryo implantation. Once Th17 cells are increased under pathological condition, IL-17 induces inflammation as demonstrated by neutrophil infiltration and stimulation of other pro-inflammatory cytokines and chemokines [9]. which has been proposed as a pathogenic mechanism for acute transplant rejection [10]. Through mediating neutrophil infiltration, IL-6, IL-17, and IL-23 can trigger inflammation and regulate Th1/Th2 balance. In addition, excessive Th17 activity may produce cytokines that increase Th1 and NK cell activity [11], resulting in the implantation failure and repeated spontaneous abortion. In contrast, CD4+/CD25bright/ Foxp3+ Treg cells play central roles in immunoregulation and induction of tolerance. The findings of Wu et al. [12] support that the proportion of Treg cells in peripheral blood lymphocytes was significantly lower in URSA patients than that in normal women, indicating that Treg cells might contribute to maternal immune tolerance of fetal antigens. Treg cells primarily exert immunoregulation and tolerance via secretion of IL-10 and transforming growth factor (TGF)-b [13], which limit the maternal immune response to the embryo under a condition of successful pregnancy, Percentage changes in Treg cells may lead to abnormal pregnancy, such as spontaneous abortion, preterm births, and preeclampsia.
Several studies characterizing immunotherapy in URSA women reported that the outcome of subsequent pregnancies was apparently improved by injection of paternal or a third party’s leukocytes [14-16]. Consistent with the role of immune response in the pathogenesis of URSA, the present study demonstrated that Th17 level was enhanced and Treg cell was reduced in URSA patients compared to normal controls. In addition, the ratio of Treg/Th17 was significantly lower in URSA decidual tissue, illustrating a shift from Treg to Th1.
In conclusion, abnormal expression of Th17 and Treg cells were observed in patients with URSA, suggesting therapeutic targeting Th17 or upregulation of Treg might be a new approach for the treatment of URSA. Moreover, the present results highlight the importance of maintaining an immunosuppressive environment in decidual tissue during pregnancy. These experiments will potentially provide a new insight for developing treatments for URSA.
This study was supported by grants from gzwjkj2017-1-038.