

Clinical and Experimental Obstetrics & Gynecology (CEOG) is published by IMR Press from Volume 47 Issue 1 (2020). Previous articles were published by another publisher on a subscription basis, and they are hosted by IMR Press on imrpress.com as a courtesy and upon agreement with S.O.G.
 , H. Bolat 1, Z. Cengisiz 1, M. Kazandi 2, B. Durmaz 1, A. Aykut 1, A. Durmaz 1, O. Cogulu 1
, H. Bolat 1, Z. Cengisiz 1, M. Kazandi 2, B. Durmaz 1, A. Aykut 1, A. Durmaz 1, O. Cogulu 11 Department of Medical Genetics, Ege University School of Medicine, Izmir, Turkey
2 Department of Obstetrics and Gynecology, Ege University School of Medicine, Izmir, Turkey
Abstract
A pregnancy loss (miscarriage) is defined as the spontaneous demise of a pregnancy before the fetus reaches viability. The term therefore includes all pregnancy losses from the time of conception until 24 weeks of gestation. Recurrent pregnancy loss (RPL) is defined as two or more losses of the pregnancy. There are many proposed reasons; however in a prominent portion of cases, the reason remains unclear. Chromosomal abnormalities have an important place in recurrent pregnancy loss. Numerical and structural abnormalities constitute a significant cause. The purpose of this study was to assess the chromosomal abnormality of 490 chorionic villus samples of the couples who experienced RPL and to provide data for both clinicians and genetic counsellors.
Keywords
- Recurrent pregnancy loss
- Abortion
- Cytogenetic abnormalities
Nearly 15% of all pregnancies end up with spontaneous abortion. Recurrent pregnancy losses (RPL) that occur before the 24th week of gestation are observed among 1-3% of pregnancy during the gestation. Different definitions of RPL have been made by the authors. Some of them define it as three or more, while others define as two or more losses of the pregnancy [1-3]. The most common abnormality of spontaneous abortion is chromosomal aneuploidy [3]. Cytogenetic abnormalities are associated with approximately 50-60% of miscarriages, in which trisomy being the most frequent, followed by polyploidy and monosomy X. Most of the chromosomally abnormal pregnancies result in miscarriage before 12 weeks of the gestation [4]. In addition to cytogenetic abnormalities coagulation protein defects, endocrinological problems, anatomic abnormalities, nutritional, and environmental factors are the other etiologic factors of RPL [5]. Unfortunately in half of the RPL cases, the exact cause of etiology cannot be identified and they are considered as idiopathic or unexplained spontaneous abortion [6]. A considerable proportion of couples who experience recurrent spontaneous abortions also exhibit balanced chromosome aberrations. Numerous studies have been investigated the proportion of chromosome aberrations among couples experiencing RPL. It is estimated to be 2.7-6.7% of couples experiencing recurrent spontaneous abortions are balanced chromosomal aberration carriers [7]. The higher the number of abortions, the more likely it is to carry chromosomal balanced anomalies. The incidence of carrier status is ~0.7% in the general population and increases to 2.2% after one miscarriage, 4.8% after two miscarriages, and 5.2% after three miscarriages [8]. Mostly observed chromosome aberrations include balanced translocations, and inversions. These balanced rearrangements may lead to an unbalanced karyotype due to segregation defects in the carrier’s gametes, which can result in spontaneous abortion, still birth or neonatal congenital defects [6].
The cytogenetic analysis of recurrent miscarriages provides valuable data to reveal the cause of the miscarriage which can avoid further costly testing. In addition, recurrent risk will contribute significantly in determining the risk for subsequent pregnancies.
Genetic testing of prospective parents can identify those who carry a disease that can be passed onto their children [9]. Cytogenetic testing of the fetuses provides information about potential birth defects and gives couples high level of probability to decide the future of their next pregnancy. The purpose of this study was to investigate 490 samples of the couples who experienced recurrent spontaneous abortions, and to evaluate fetal karyotypes. The authors also aimed to provide data for the clinicians and genetic counsellors in counselling couples who have experienced recurrent spontaneous abortion. The evaluation of a large number of cases will be an important source of information.
The study population includes 490 first-trimester chorionic villus samples obtained by evacuation (aspiration-curettage) from women with a diagnosis of missed abortion established at the ultrasound examination at Ege University Hospital between 2013 and 2015. All of these patients were informed via genetic counseling regarding the risk of having chromosomal abnormality in their fetus and procedures of testing. The test was performed only in the patients who signed written informed consent. The present study was approved by the local ethic committee, where the study was conducted.
Samples were collected in warmed RPMI 1640 medium supplemented with fetal calf, L-glutamin and antibiotics and delivered immediately to the laboratory. Samples were examined under a dissecting microscope and were separated from maternal decidua and blood clots. They were divided into fragments of 3-5 mg, which were processed independently and 10-12 pieces were planted in one flask. The culture was maintained for 10-14 days at 37ºC and 5% CO until cell growth was observed under an inverted microscope. CVS samples were collected in warmed RPMI 1640 medium supplemented with fetal calf, L-glutamin and antibiotics and delivered immediately to the laboratory. Samples were examined under a dissecting microscope and were separated from maternal decidua and blood clots. They were divided into fragments of 3-5 mg, which were processed independently and 10-12 pieces were planted in one cell culture flask containing 5 ml Bio-AMF-1 medium including supplements with additional penicillin-streptomycin at 1% and 5 mM l-Glutamine. Three flasks were used for each sample. The culture was maintained for 10-14 days at 37°C with 5% CO2 and passaged when 90% confluence was reached. Between one and four preparations were obtained from each flask, depending on the initial amount of the tissue. G-banding was performed for chromosomal sample preparation, following the ISCN standard to analyze the karyotypes. Karyotype was performed using Cytovision software and analyzed by fully automated metaphases finder system. The number of metaphases examined was at least 20 and increased in mosaic cases. Positive results were described as following two groups: 1) numerical abnormality and 2) structural abnormality. After the conclusion of the testing, genetic counseling was given to all patients about the significance of the results who decided subsequent pregnancies.
Among the 490 samples, 357 were successfully karyotyped (culture success rate: 73%). One hundred and thirty-three samples (culture failure rate: 27 %) failed to produce metaphase chromosomes due to insufficient quality for cytogenetic analysis. In addition, 46% of the samples had normal karyotype and 27% samples had chromosomal abnormalities. Ten (2%) of them were complex chromosomal abnormalities and three (1%) of them were structural chromosomal abnormalities. In the cases of cytogenetic abnormalities, 128 (26%) numerical chromosomal aberrations were established. There were also 17 (3%) triploidies and six (1%) tetraploidies, resulting in a total number of 124 single chromosome abnormalities identified. Also two sample were translocation type (t1;5 and t 1;18) abnormality, as well as two of the complex abnormality group were Robertsonian type translocation. Karyotype descriptions of the cases with double trisomies were 48,XX,+16,+21, 48,XX,+9,+15, 48,XY,+16,+20, 48,XY,+14,+16, and 48,XY, ,+3,+22 (4%). Results are summarized in Table 1 and in Figure 1.
| Normal Karyotype | Number of cases (46%) |
|---|---|
| 46,XY | 83(17%) |
| 46,XX | 140 (29%) |
| Chromosomal abnormalities | 134(27%) |
| Triploides | 17(3%) |
| Tetraploides | 6 (1%) |
| *Viable trisomies | 15 (3%) |
| +21 | 7 |
| +18 | 3 |
| +13 | 5 |
| Other trisomies | 71(14%) |
| +3 | 2 |
| +6 | 1 |
| +7 | 1 |
| +8 | 6 |
| +9 | 2 |
| +12 | 1 |
| +14 | 6 |
| +15 | 8 |
| +16 | 22 |
| +17 | 3 |
| +20 | 4 |
| +22 | 15 |
| Monosomy | 12(2%) |
| 45,X | 12 |
| Structural chromosomal abnormalities | 3 (1%) |
| **46,XX,t(1;5) | 1 |
| **46,XX,t(1;18) | 1 |
| 46,X, del(18)(p11.2) | 1 |
| Complex chromosomal abnormalities | 10(2%) |
| 48,XX,+16,+21 | 1 |
| 48,XX,+9,+15 | 1 |
| 70,XXX,+20 | 1 |
| 46,X,+22 | 1 |
| 46,XX,rob(13;14),+22 | 1 |
| 48,XY,+16,+20 | 1 |
| 48,XY,+14,+16 | 1 |
| 71,XXY,+16,+22 | 1 |
| 48,XY,+3,+22 | 1 |
| 46,XY,rob(13;14),+13 | 1 |
| Culture failure | 133(27%) |
| Total | 490(100%) |
*Trisomies are shown in practical way (not full ISCN karyotyping style).
**In some karyotypes presenting structural rearrangement, the exact breakpoints cannot be given due to metaphase resolution level.
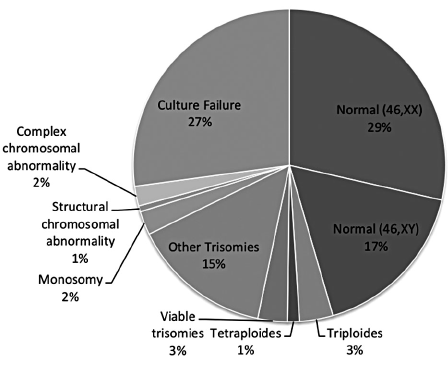 Figure 1.
Figure 1.— Distribution of cytogenetic abnormalities
Recurrent pregnancy loss is a devastating reproductive problem in the field of Obstetrics. Most of the causes of first-trimester abortions are numerical and/or structural chromosomal disorders. On the other hand there are several factors including, immunological, endocrinological, anatomical, and environmental abnormalities associated with recurrent pregnancy loss. Despite developments in Genetics and Obstetrics, miscarriages continue to be a frequent unlucky episode during pregnancy, besides a challenge to professionals in these areas, but also a source of anxiety for parents, especially in cases of recurring miscarriages. A great part of first-trimester miscarriages are due to chromosomal abnormalities [10]. Chromosome analysis from the abortion material helps us to detect whether any type of chromosomal abnormality in the fetus is the reason of the abortion. Chromosome abnormalities were observed in 27% of miscarriage materials assessed in this study which is a little lower than the confirming previous data from the literature, which has shown that 35% to 50% of all first trimester miscarriages are caused by chromosome abnormalities [11]. For instance, Zhang et al. investigated chorionic villi of 252 cases of missed abortion and detected chromosomal abnormality in 58.09% of the cases (81 were trisomy, 29 were monosomy X, and 17 were polyploidy) [12].
Lower success rate in this study can most likely be attributed to the high culture failure. In order to increase the number of chromosomal anomalies, polymerase chain reaction and comparative genomic hybridization are useful techniques for cases in which there is no cell growth in growth medium or when there is contamination by maternal cells [13]. To prevent the contamination of chorionic villi, being very careful during specimen collection is essential. The rate of cell growth failure mentioned in the literature ranges from 10% to 15%, which is in a lower rate found in this study (27%). This condition may be attributed to lack of viable trophoblastic cells. The number of viable cells decreases as the intervention time lapses.
The most frequent isolated chromosomal anomaly in this study was that of chromosome 16, which concurs with data from the literature (Table 1) [14]. The occurrence of trisomies is associated with aged mothers, which currently is a problem in the light of the increasing maternal age in most countries [15]. Some studies suggest that miscarriages without karyotype alterations, which could have other causes than genetic, are more frequent in women less than 35-years-old [16].
Polyploidies and monosomy X are also common causes of miscarriage, which was confirmed by this study. These abnormalities, however, do not have an evident association with maternal age [15]. Monosomy X and triploidies were seen in 5% of the total anomalies in this study. As polyploidy anomaly, tetraploids also account for about 1% of anomalies and no association was found with maternal age together with monosomy X and triploidies.
Numerical chromosomal abnormalities are much more frequent in abortion materials than structural abnormalities. Zhang et al. [10] concluded that chromosome abnormalities, 90% of which were numerical and 10% of which were structural. In the present study the authors found numerical and structural abnormalities 88% and 12%, respectively.
Although an isolated episode of miscarriage is a random event in the vast majority of cases and a full etiological investigation is not formally indicated, some authors suggest that, in these cases, the cytogenetic analysis could be comforting from a psychological perspective for patients aged 35 or older. In a similar study in which 420 abortion materials were classified according to maternal age, Stephenson et al. found that 46% of the abortions had a chromosomal abnormality. The authors suggest investigating other etiologic factors after two early abortions with normal karyotype, as they provide more effective therapeutic measures in early diagnosis and treatment [16]. In addition, cytogenetic evaluation performed in isolated cases allows the determination of changes caused by random errors in the meiosis line. By this way, detecting a chromosomal abnormality will make using other research useless and obtain cost-effectiveness. It is an important issue how to obtain cost-effectiveness in use of cytogenetic analysis.
A limitation of present study is a slightly high culture failure rate which was 27%. As mentioned before by the present authors, this rate can be attributed to low number of live chorionic villus cells. On contrary this study is distinct because of the lack of recent publications on this topic in the literature. We require future investigations especially in the cases that have recurrent abortions in the first trimester.
Cytogenetic alterations, mainly aneuploidies are an important cause of miscarriages and their detection is helpful to the couple’s genetic counseling. Among over 60 described alterations, other trisomies is the most frequently found, followed by viable trisomies, triploidies, and monosomy X. Cytogenetic analysis must be conducted as routine in cases of habitual abortion, but usage in practice for isolated miscarriage episodes, in spite of being theoretically beneficial, should be confirmed in future studies.
Evaluation of chromosomal abnormalities in recurrent pregnancy losses is important to understand the associations between chromosomal abnormalities and pregnancy losses, and to provide proper genetic counseling to the parents. Clinicians should encourage families to investigate the causes of pregnancy loss thoroughly to assist in counseling regarding the risk of recurrence .
The Authors would like to thank Munise Bahar, Hatice Yılmazer, Sinem Türköz, and Halide Gül Akyar for their valuable technical assistance during 2013-2015 period.