


Clinical and Experimental Obstetrics & Gynecology (CEOG) is published by IMR Press from Volume 47 Issue 1 (2020). Previous articles were published by another publisher on a subscription basis, and they are hosted by IMR Press on imrpress.com as a courtesy and upon agreement with S.O.G.
 , M. Ando 1, Y. To 1, T. Koyanagi 1, H. Kondo 1, F. Eguchi 1
, M. Ando 1, Y. To 1, T. Koyanagi 1, H. Kondo 1, F. Eguchi 11 Department of Obstetrics and Gynecology, Aso Iizuka Hospital, Fukuoka, Japan
Abstract
Anti-N-methyl-D-aspartate (NMDA) receptor encephalitis is the most common form of paraneoplastic encephalitis that is associated with teratomas. Because removal of the tumor leads to better clinical outcomes, determining the location of teratomas is essential. The authors report two cases of anti-NMDA receptor encephalitis with a small ovarian teratoma that could not be detected by usual imaging. Both cases had the diagnosis confirmed laparoscopically.
Keywords
- Anti-N-methyl-D-aspartate receptor encephalitis
- Ovarian teratoma
- Laparoscopy
Anti-N-methyl-D-aspartate (NMDA) receptor encephalitis was identified in 2007 by Dalmau et al. [1]. This encephalitis is a type of limbic encephalitis that is often found in young women with ovarian teratomas. Despite the risk of fatality from NMDA receptor encephalitis, at least 80% of patients experience major neurological improvement with removal of the tumor and immunotherapy [2]. In patients with this encephalitis and ovarian teratoma, surgical resection of the tumor and subsequent immunotherapy are the treatment modalities that have the most significant effect on outcome [3]. Anti-NMDA receptor encephalitis often occurs with a small ovarian teratoma. The usefulness of explorative laparoscopy is unclear when no evidence of teratoma is available in these patients.
The authors report two cases of anti-NMDA receptor encephalitis with a small ovarian teratoma, which was undetectable by multiple imaging investigations, including CT, ultrasonography, and MRI. The teratoma was found by laparoscopy and removed by laparoscopic cystectomy.
A healthy, 31-year-old, gravida 0 woman with no past medical history developed a persistent headache for 11 days. This was accompanied by a fever and progressive abnormal behavior and loquacity, followed by a generalized seizure. On presentation, she presented with difficulty in speaking, but her vital signs, physical examination, and routine laboratory tests were unremarkable. No lesion was found on a CT scan and MRI of her brain. Cerebrospinal fluid (CSF) tests showed no inflammatory features. She was admitted to the neurological department of this hospital. Because of a high index of suspicion for autoimmune encephalitis, including anti-NMDA receptor encephalitis, some imaging tests for evaluating ovarian teratoma were performed. Pelvic CT and transvaginal ultrasonography showed a 3-cm-diameter left adnexal simple cystic mass and the authors diagnosed this lesion as a functional follicle. There were no findings of ovarian teratoma (Figure 1). She was initially treated with antiviral medicine and steroids, and plasma exchange therapy. Her symptoms progressed over the next week with hypoventilation and coma, despite these treatments. She required management with a ventilator 13 days after admission because of central hypoventilation. Serum and CSF tests for NMDA receptor antibodies were positive 33 days after admission. To perform a more detailed examination of ovarian tumor, the authors performed pelvic contrast-enhanced MRI, and the examination detected a small (17 mm in diameter) cystic mass in the right ovary, which suggested ovarian teratoma (Figure 2). The serum tumor markers carcinoembryonic antigen (CEA), CA125, and SCC were negative. A decision was made to proceed with explorative laparoscopy for tumor resection to prevent further progression of disease. Laparoscopy was performed after 38 days in this hospital. The patient’s right ovary had a small cystic mass and she underwent cystectomy of the right ovary (Figure 3). The authors made an incision in the left ovary, but no tumor was found inside. The right ovarian cyst was 15 mm in diameter and a pathological examination showed a mature cystic teratoma. After postoperative therapy, including five courses of plasma exchange, intravenous immunoglobulin therapy, and methylprednisolone pulse therapy, she steadily recovered. When she was discharged 216 days after admission, she had impairment of her short-term memory, but was psychiatrically intact and fully independent in all acts of daily living.
 Figure 1.
Figure 1.— Enhanced pelvic CT of case 1 shows a small functional cyst in the left ovary, but there is no evidence of a teratoma in both ovaries.
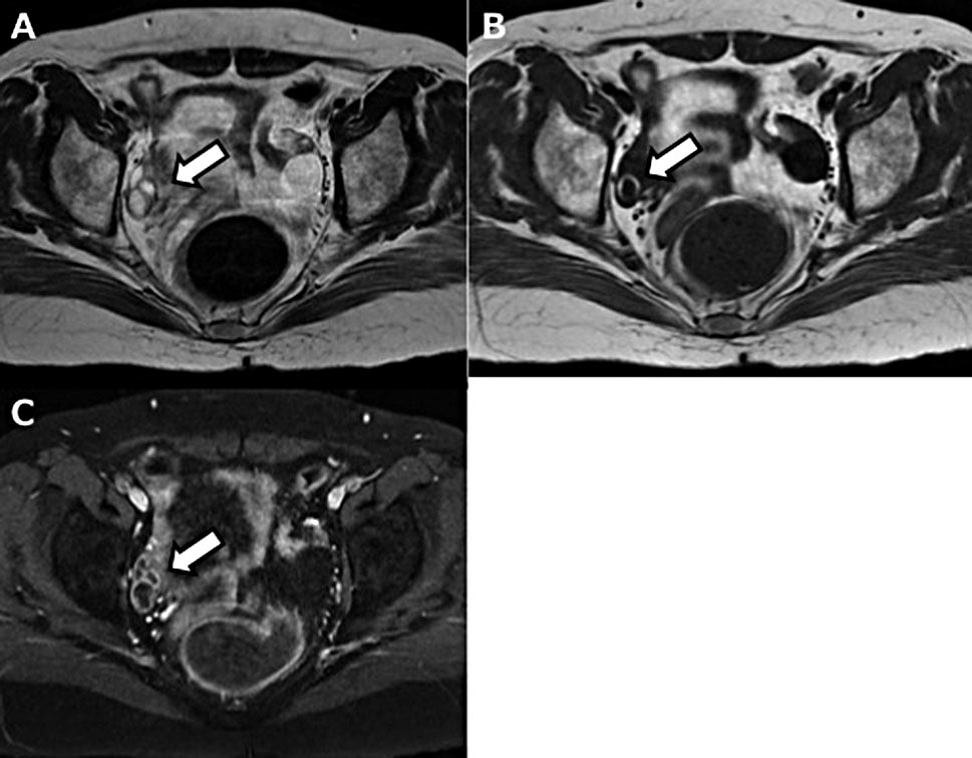
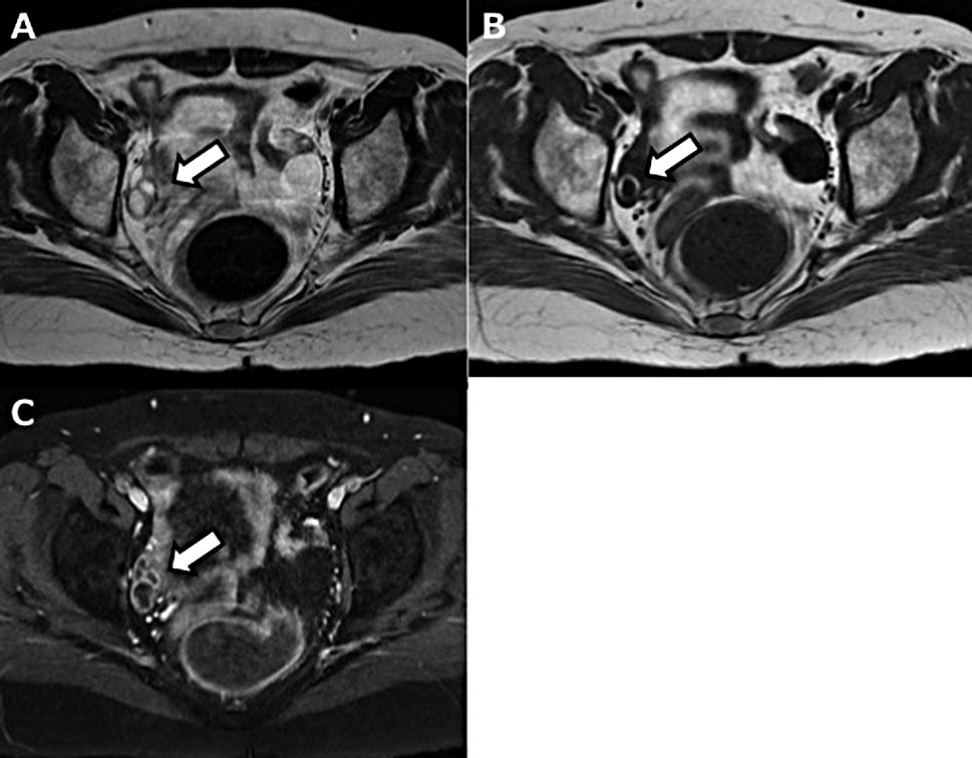 Figure 2.
Figure 2.— T2- (A), T1- (B), and fat-suppressed T1 (C)-weighted MRI shows a small cystic mass in the right ovary of case 1, which suggests an ovarian teratoma.
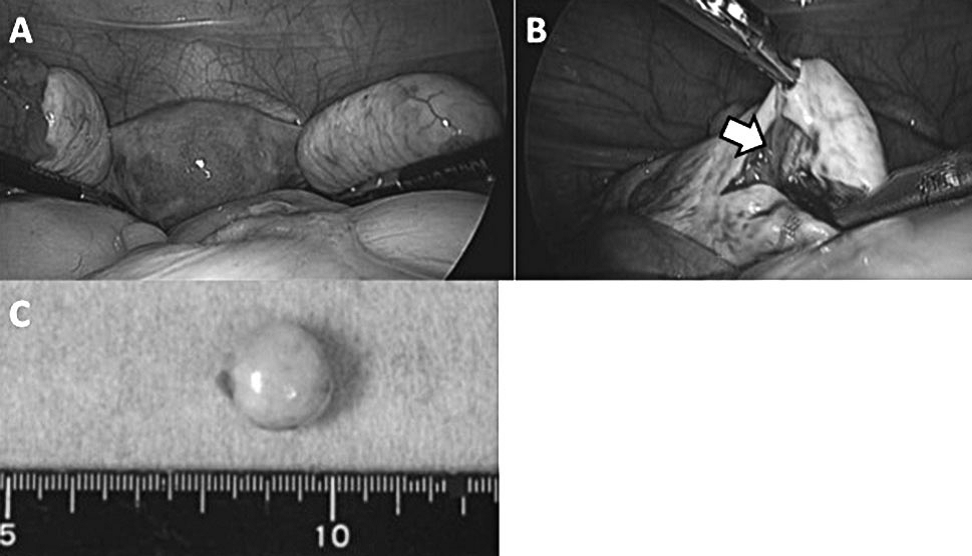
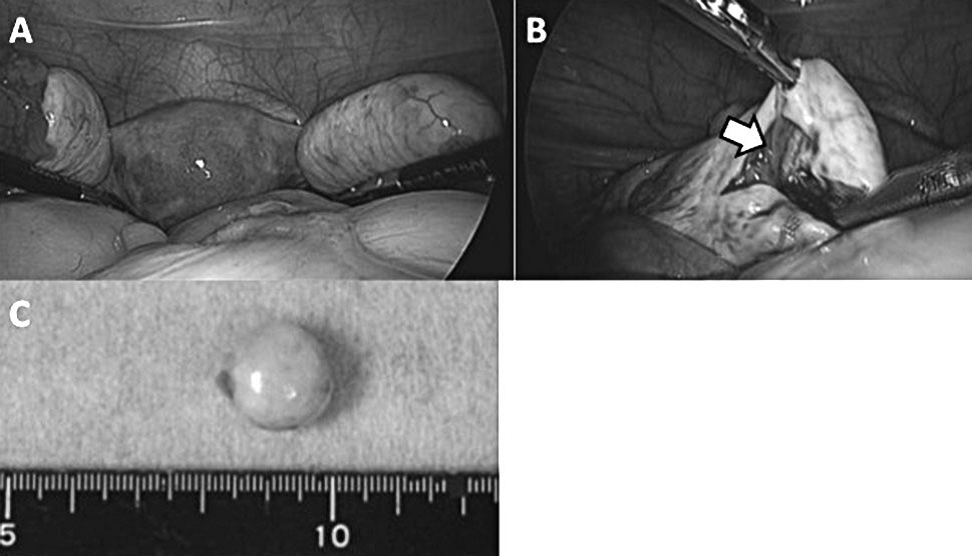 Figure 3.
Figure 3.— Even in laparoscopic surgery of case 1, the right ovary has a normal appearance (A), but a small lesion can be seen by an incision (B). The excised tumor is a cyst of 15 mm in diameter (C).
An 18-year-old, gravida 1, para 0 woman with no past medical history visited the emergency unit in this hospital with complaints of impairment of consciousness and hypothermia. She presented with a persistent headache for 14 days, accompanied by progressive abnormal behavior and confusion. On presentation, she was confused and could not communicate with others, but her vital signs, physical examination, and routine blood tests were unremarkable. No lesion was found in a head CT scan of her brain. Brain MRI showed bilateral medial temporal lobe hyperintensity. CSF tests showed no inflammatory features. She was admitted to the neurological department of this hospital. Because of the possibility of autoimmune encephalitis, imaging tests for evaluating ovarian teratoma were performed. Pelvic CT, transvaginal ultrasonography, and pelvic contrast-enhanced MRI showed no abnormal lesion in both ovaries, except for a small (17 mm in diameter) cystic mass in the right ovary in MRI (Figure 4). This lesion suggested an ovarian follicle because it was detected as a low-intensity area in a T1-weighted image and a high-intensity area in a T2-weighted image (Figure 5). The serum tumor markers CEA, CA125, CA19-9, and SCC were negative. Because results were not yet available from anti-NMDA receptor antibody studies, she was initially treated with antiviral medicine and steroids, and plasma exchange therapy. Her symptoms rapidly progressed. Her seizures became intractable and she developed persistent autonomic instability and dyskinesia. She required management with a ventilator eight days after admission. Serum and CSF tests for anti-NMDA receptor antibodies were positive 41 days after admission. The authors discussed with her family and neurologists about the risks and benefits of explorative laparoscopy. A decision was made to proceed with laparoscopy to evaluate and remove the ovarian tumor. Laparoscopy was performed after 77 days in this hospital. Laparoscopic evaluation (Figure 6) showed normal-appearing pelvic organs, including both ovaries. The authors made an incision in the right ovary and found a small cystic mass, which contained hair and fat. They performed laparoscopic cystectomy of the right ovary and also confirmed that there was no tumor inside the left ovary. The tumor of the right ovary measured 15 mm in diameter and a pathological examination showed a mature cystic teratoma of the right ovary. After postoperative therapy, including several courses of plasma exchange, intravenous immunoglobulin therapy, and methylprednisolone pulse therapy, she gradually and steadily recovered. When she was discharged after 144 days in from this hospital, she had a sleep disorder, but was psychiatrically intact.
 Figure 4.
Figure 4.— Enhanced pelvic CT of case 2 shows no evidence of an adnexal tumor.
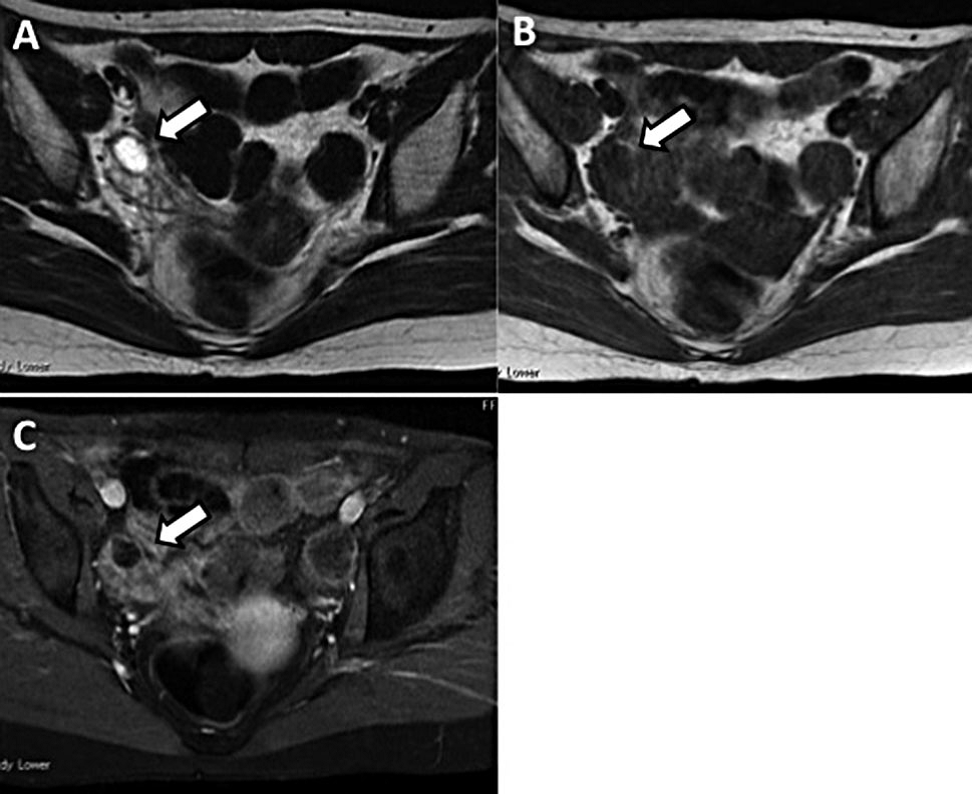
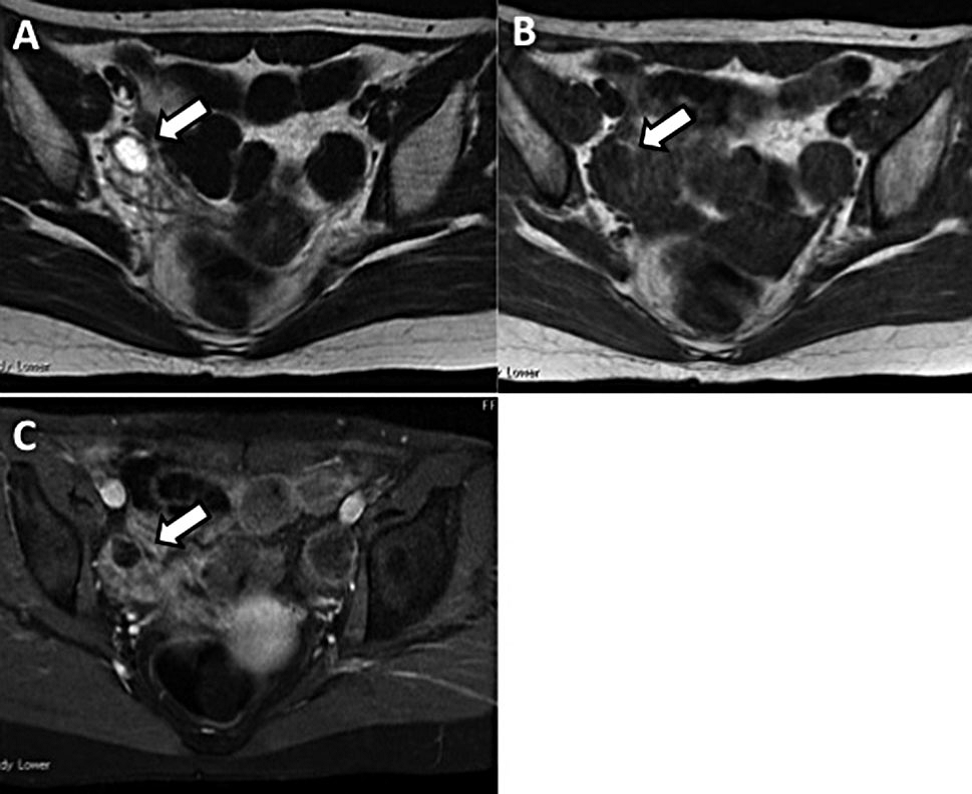 Figure 5.
Figure 5.— T2- (A), T1- (B), and fat-suppressed T1 (C)- weighted MRI shows a follicle in the right ovary of case 2, but there is no evidence of teratoma in both ovaries.
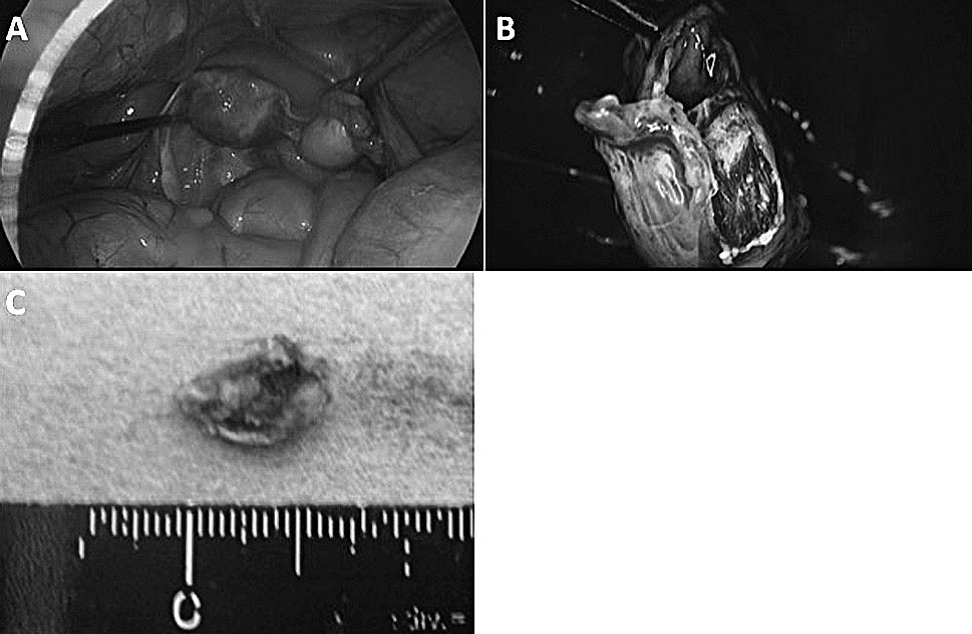
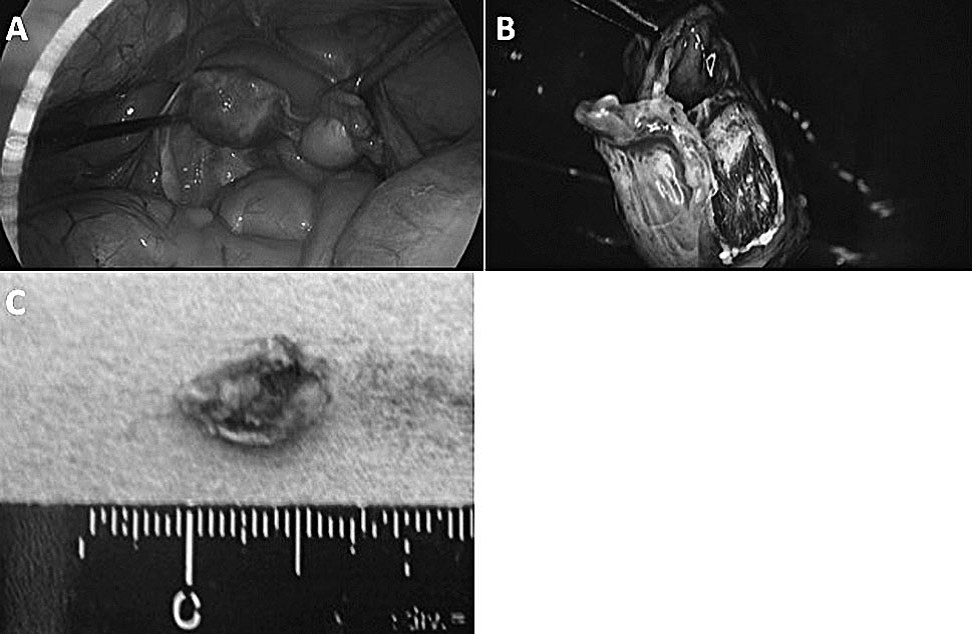 Figure 6.
Figure 6.— Laparoscopic view of case 2 in the pelvis. Both ovaries have a normal appearance (A), but a small cystic mass with a hair ball can be seen in the right ovary by an incision (B). The excised tumor is confirmed as a cystic teratoma with a macroscopic appearance (C).
The present cases are typical of anti-NMDA receptor encephalitis. Anti-NMDA receptor encephalitis is caused by an autoimmune reaction against the NMDA receptor, and is characterized by psychiatric and neurological symptoms. Patients can initially present with psychiatric symptoms, such as agitation, paranoia, hallucinations, and aggression. These patients can later develop dyskinesia, seizures, autonomic instability, a decreased level of consciousness, catatonia, and central hypoventilation. The encephalitis is a serious, but treatable condition, if recognized and treated early. The precise incidence of this encephalitis is unknown, but it appears to be more frequent than any other known paraneoplastic encephalitis. In a case series of approximately 500 patients with anti-NMDA receptor encephalitis, the average age of onset was 21 (0.7-85) years and 81% of the patients were women [4]. A total of 38% of the patients had an underlying tumor, which was most commonly an ovarian teratoma (94%). In female patients with anti-NMDA receptor encephalitis older than 18 years, the frequency of an underlying teratoma is much higher than in younger patients. Spontaneous neurological improvement has been reported, but usually occurs at the expense of a longer hospital stay with a slower recovery. Mortality for this syndrome is 4-8% [5]. In patients with anti-NMDA receptor encephalitis associated with ovarian teratoma, surgical resection of the tumor and subsequent immunotherapy are the most effective treatment strategies for improvement in symptoms. Once definitive diagnosis has been obtained, imaging studies, such as pelvic ultrasound, MRI, CT, and positron emission tomography, may be used to identify an underlying teratoma. Although approximately 80% of patients who undergo tumor removal and immunosuppressive treatment have substantial neurological improvement, only 48% of those without tumor resection have a similar degree of improvement [4]. Furthermore, in a systemic review of 100 cases of anti-NMDA receptor encephalitis, early surgical removal or immunotherapy treatment of the teratoma (within four months of onset of symptoms) showed a better neurological outcome, a lower chance of relapse, and a reduced time to recovery than late or no tumor treatment [6]. Delayed treatment may result in progression of the autoimmune process. In one series of patients with anti-NMDA receptor encephalitis, five of six patients with ovarian teratoma who did not undergo surgery died [4]. Therefore, early resection of the tumor in these patients is important for preventing worsening of neurological status. In the present cases, suspicion of this encephalitis led to a search for an ovarian teratoma, but imaging tests showed no convincing evidence of teratomas. In patients with no detectable underlying neoplasms, this syndrome may be caused by microscopic germ cell tumors that are undetectable by imaging [2]. In a systematic review of 174 cases of anti-NMDA receptor encephalitis, Acien et al. reported that even small teratomas containing nervous tissue may result in severe complications secondary to anti-NMDA receptor encephalitis. Teratomas might only be detected several years following presentation of this type of encephalitis [7]. However, recovery is less common and relapse more likely in patients without a detectable tumor. Therefore, for patients older than 12 years without detectable tumors, the authors recommend continuing immunosuppression for a minimum of one year after relapse of symptoms. Ovarian teratomas should be screened for using pelvic MRI or ultrasound every six months for four years [2]. Whether empiric exploratory laparotomy or laparoscopy and blind oophorectomies should be performed in patients with anti-NMDA receptor encephalitis without clinical evidence of a tumor is debatable. Dalmau et al. showed that among seven patients who underwent exploratory laparotomy, only one was found to have a teratoma [6]. The main complication of bilateral oophorectomy is premature menopause, including the need for hormone replacement therapy. However, a small teratoma may only be identified microscopically following oophorectomy or at autopsy. A previous report showed that a 25-year-old woman with anti-NMDA receptor encephalitis underwent bilateral oophorectomy, despite negative imaging results [8]. Twenty-nine days after her admission, histology confirmed a teratoma, and it was only after surgery that she began to recover. The present authors detected a small teratoma by laparoscopy in their patient and resected it with ovarian preservation. Because a laparoscopic examination for determining ovarian teratoma is less-invasive than laparotomy, trial laparoscopy may be acceptable for a treatment strategy if an ovarian tumor cannot be detected by various imaging tests. With appropriate diagnosis and treatment, including resection of the teratoma and immunosuppression, patients with anti-NMDA receptor encephalitis are likely to recover from their symptoms. Therefore, gynecologists should treat these patients by early detection and removal of the tumor.
The authors thank Ellen Knapp, PhD, from Edanz Group (www.edanzediting.com/ac) for editing a draft of this manuscript.