




Clinical and Experimental Obstetrics & Gynecology (CEOG) is published by IMR Press from Volume 47 Issue 1 (2020). Previous articles were published by another publisher on a subscription basis, and they are hosted by IMR Press on imrpress.com as a courtesy and upon agreement with S.O.G.
 , D. Ferreira 1, C. Ferreira 1, E. Pereira 1, M. Branco 2
, D. Ferreira 1, C. Ferreira 1, E. Pereira 1, M. Branco 21 Hospital da Senhora da Oliveira - Guimarães, Portugal
2 Centro Hospitalar e Universitário de Coimbra, Maternidade Bissaya Barreto, Coimbra, Portugal
Abstract
Fetal anaemia in pregnancy, although less prevalent since the introduction of anti-D immunoglobulin, remains a clinical issue. In this article the authors describe two clinical cases of challenging fetal anaemia; the first following a parvovirus B19 infection during pregnancy and the second after Rh isoimmunization (due to Rh positive maternal transfusions in childhood), sooner and more severe in a second pregnancy. A brief review of the topic was also conducted.
Keywords
- Fetal anaemia
- Parvovirus
- Transfusion
- Systolic peak middle cerebral artery
- Fetal transfusion
When any blood group factor inherited via father is not possessed by the mother, antepartum or intrapartum hemorrhage may stimulate an immunological reaction [1-3]. This can also occur if the mother received unmatched blood transfusion [1-3]. The formation of maternal antibodies is called isoimmunization, which can lead to varying degrees of transplacental passage of these antibodies into the fetal circulation, causing a sufficient immune response to destroy fetal red blood cells [1-3]. More commonly, isoimmunization occurs in subsequent pregnancies, causing haemolytic disease of the fetus or newborn (NB), characterized by hemolysis, bilirubin release, and anaemia. The severity of the disease will depend on the degree of immune response (amount of antibodies produced and their affinity for the antigens), the gestational age at the diagnosis, and the fetal capacity to replace the destroyed erythrocytes, maintaining a sufficient hematocrit for their growth and development [1-3].
Fetal anaemia in pregnancy remains a diagnosis of suspicion. The etiology includes genetic diseases, metabolic deficits, infections, and thoracic abnormalities [2]. The most frequent causes of severe fetal anaemia are erythrocyte alloimmunization, parvovirus B19 infection, chronic fetomaternal haemorrhage, genetic erythrocytic diseases, and complications of twin fetal transfusion treatment [2]. Although relatively rare, the fetus is at risk of transient aplastic crisis, high-output heart failure, non-immune hydrops or even demise [1-3].
The patient was 38-years-old, 0 Rh negative, G2 P1, with first pregnancy at risk in 2010 due to positive Coombs and a steadily increase in irregular antibodies titers. Fetal anaemia and hydramnios developed at 33 weeks, conditioning a caesarean delivery two weeks later. The newborn needed an exchange transfusion in the second week of life. The investigation highlighted a history of maternal transfusion (0 Rh positive) in her childhood (at 6-7 years). At second pregnancy (2013), fetal blood group screening in maternal blood at 18 weeks revealed Rh positive fetus. After a weekly systolic peak of the middle cerebral artery (SP-MCA) surveillance beginning at 20 weeks, nine weeks later the ultrasound was suggestive of fetal anaemia (Figure 1). Three cordocentesis were then performed with fetal blood transfusion (29, 31, and 33 weeks of gestation) (Figure 2). At 33+1 weeks a caesarean section was decided (NB 2,534 grams, 9/10 Apgar and 12 g/dL haemoglobin). A new NB blood transfusion was required at the third day of life due to a decrease in hemoglobin in the neonatal period (9 g/dL). Currently, at four-years-old, the child presents a normal psychomotor development.
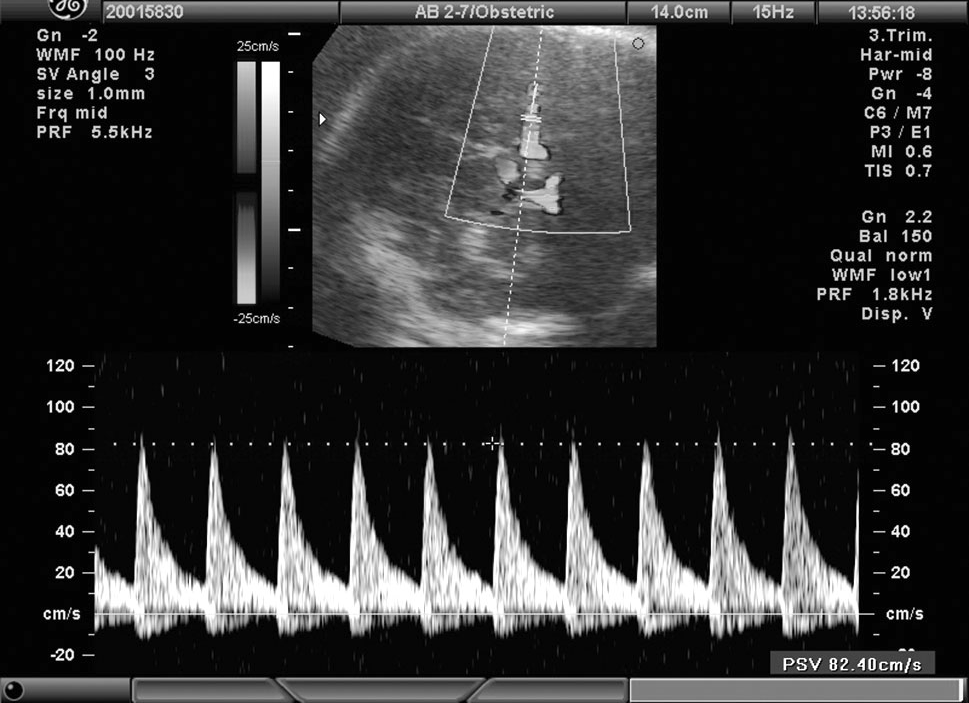 Figure 1
Figure 1— Ultrasonographic SP-MCA before treatment in fetal anaemia due to prior maternal unmatched transfusions.
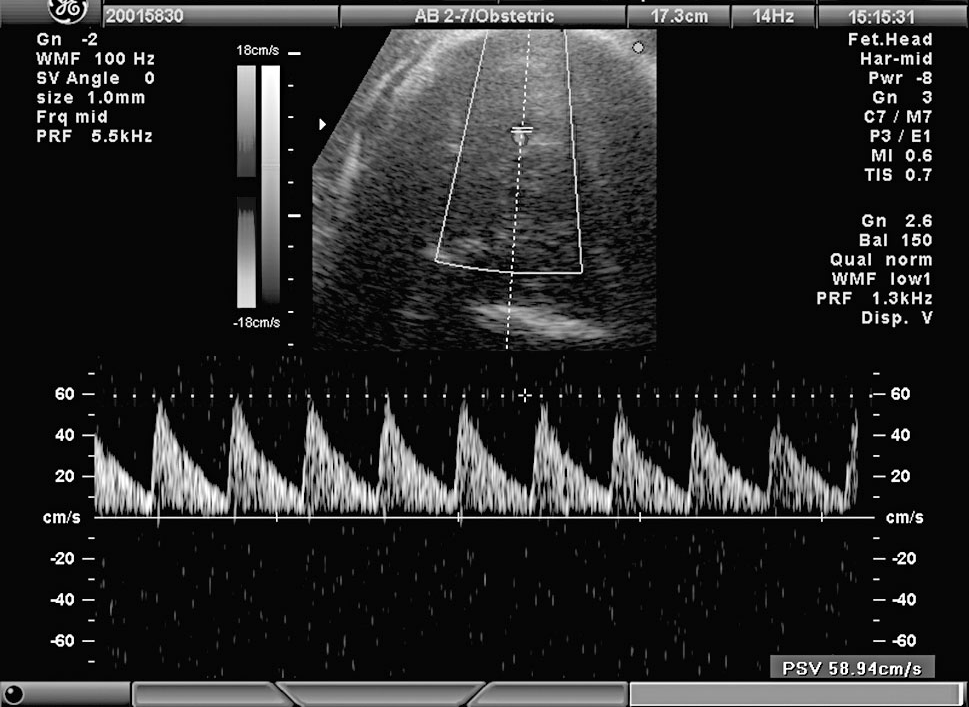 Figure 2
Figure 2— Ultrasonographic founding after fetal treatment in fetal anaemia (prior maternal unmatched transfusions).
The patient was 32-years-old and was first surveilled with a pregnancy with normal development until week 24. In this period, fetal hydrops was observed (ascites and pericardial effusion), conditioning probable fetal anaemia - SP-MCA above 2 MoM (Figure 3). After investigation, the hypothesis of fetal infection by parvovirus B19 seemed probable, confirmed by amniocentesis. Then, managed in a tertiary hospital, a four-time cordocentesis with blood cell transfusion (fetal haemoglobin before the first transfusion - 2.1 g/dL; after four transfusions - 9.5 g/dL) was performed. Subsequently, in serial ultrasonography with SP-MCA, the fetus remained slightly above 1.5 MoM and with hydrops reversal until term (Figure 4). Eutocic delivery of NB with 2,592 grams, 9/10 Apgar occurred at 38 weeks. Blood NB samples highlighted 15 g/dL haemoglobin. Currently, at four-years-old the child presents a normal psychomotor development.
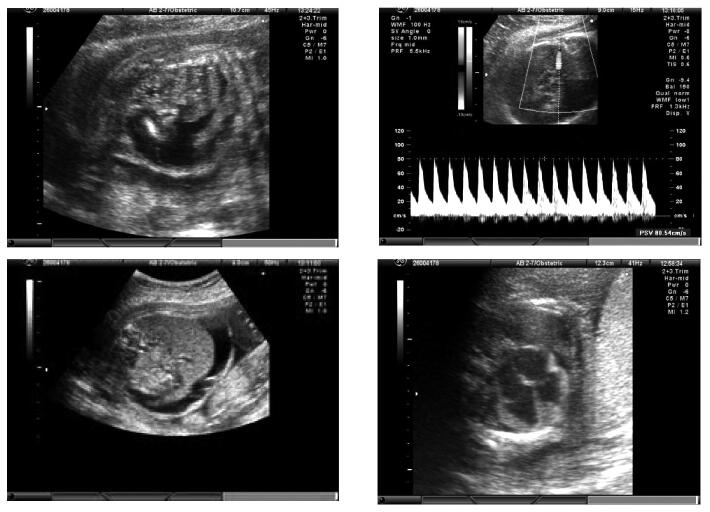 Figure 3
Figure 3— Ultrassonographic findings before the first transfusion in fetal anaemia by parvovirus B19.
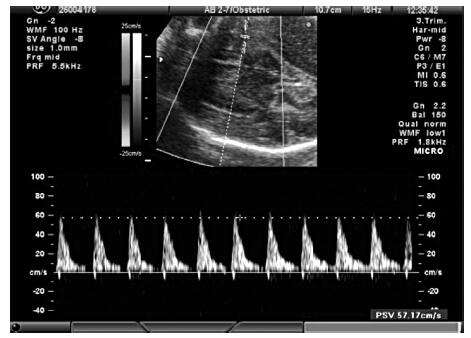 Figure 4
Figure 4— Ultrasonographic SP-MCA after fetal transfusions in fetal anaemia due to parvovirus B19.
More than 50 anti-erythrocyte antibodies have been associated with fetal haemolytic disease [2]. The most common antigens responsible for fetal erythroblastosis are anti-D, anti-K1 (Kell) and anti-c [1-4]. Despite the implementation of prophylactic anti-D isoimmunization, maternal Rh is still a cause of fetal hemolytic disease [1-3, 5].
The first step seems to be assessing paternal blood test to predict fetal Rh and determine the fetus risk of alloimmunization [2, 3, 5]. If this is negative, alloimmunization will be mainly due to past transfusions or injection sharing [2, 4, 5]. Next, if the paternal Rh is positive, free fetal DNA can be screened in maternal blood to determine the Rh type [1-3, 5]. Less commonly used option is PCR determination [2].
The first pregnancy with Rh positive alloimmunization is followed differently from subsequent ones, due to less severe fetal effects (worsening with each pregnancy) [1-5]. In the first one, the indirect Coombs titer is used not only for detection but also to characterize the degree of alloimmunization [2, 4, 5]. It is considered a screening test, with the critical titer (associated with fetal hydrops risk) being between 1/8 and 1/32 [2, 4, 5]. Until this threshold is reached, bi-monthly to monthly monitoring is acceptable; if this occurs, it becomes necessary to characterize the severity of fetal anaemia [2].
Administration of anti-D globulin after the primary immune response to the D antigen has occurred does not prevent a titer increase [2, 5]. Subsequent pregnancies are more serious due to the anamnestic response of maternal antibodies to the presence of fetal cells in the maternal circulation [1-3, 5]. If previous pregnancy was significantly affected, worst fetal anaemia is almost certain in a new pregnancy [1-3, 5]. Surveillance of the severity of anaemia should begin in this case at 16/18 weeks, and there is no need for repeating a Coombs test, as it does not predict the severity of the anaemia [2, 5]. Anaemia is characterized non-invasively by determining the SP-MCA, because hydrops may already be seen only in a severe state of fetal anaemia [2]. It is used based on the principle that the anemic fetus preserves oxygen supply to the brain by increasing of low viscosity cerebral blood flow [2]. The sensitivity of SP-MCA in the prediction of moderate to severe anaemia is around 85-90%, in the presence or absence of hydrops, with a false-positive rate of about 15% [2, 5]. Even in alloimmunized women for more than one erythrocyte antigen, there are no specific guidelines, and their gestations are followed in the same way as gestations with isolated alloimmunization [1-3].
In parvovirus B19 infection, fetal anaemia is due to maturation arrest of erythrocyte marrow precursors [6]. It can condition hydropsy due to high-output heart failure and myocarditis [2, 6].
Parvovirus B19 infection is common in children and may be asymptomatic or have mild manifestations in immunocompetent adults [6]. It primarily infects cells in accelerated division, being cytotoxic to the erythroid progenitor line, and may promote apoptosis [2]. The incidence of infection in pregnant women is about 3.5%, varying according to, for example, in occupational groups [6]. It is benign in most cases, but may cause fetal hydrops and, in extreme cases, fetal death [1-3, 6]. Fetal demise occurs mainly if the infection is documented in the first half of pregnancy (11% vs. 1%), as well as the risks of anaemia and fetal hydrops [2, 6]. Rarely the infection cause preterm birth [6]. Suspicion requires adequate monitoring [1-3, 6]. The evolution of the hydropsy is uncertain, and it may be of spontaneous resolution or condition fetal death, depending also on the severity [6]. Although congenital anomalies have been described in some cases, most pregnancies with infection do not have an adverse prognosis and parvovirus B19 does not appear to be teratogenic [2, 6].
The diagnosis of primary infection is essentially serological (IgM and IgG), although PCR techniques may be useful [1-6]. It is difficult to carry out its culture [6]. For fetal diagnosis, the method of choice, remains the isolation of small amounts of viral DNA through amniotic fluid PCR techniques [6]. If there is confirmation of infection, the clinical situation and risks should be explained, the necessary ultrasound surveillance implemented, and the possibility of intrauterine transfusion equated. This is mostly underlined in severe cases, since the fetus generally tolerates mild to moderate degrees of anaemia [1-6]. Doppler SP-MCA is effective in the non-invasive determination of the degree of fetal anaemia [1-6].
Fetal transfusion in clinical cases of fetal anaemia should be considered for hemoglobin levels below 7 g / dL (adjusted for gestational age) or two standard deviations below the mean, with erythrocytes submitted to the same quality control of the general population, preferably from Rh negative donor, irradiated, leuko-depleted, concentrated to a 75% to 85% hematocrit, CMV negative, and with less than five-day storage [2, 7]. Vascular access is mainly used, via a distal portion of the umbilical vein in the just-placental umbilical cord or intrahepatic umbilical vein, for a target of a 40-50% of final hematocrit [2, 7]. In some cases, intraperitoneal transfusion can be a choice [2, 7].
After the first transfusion, a decline in fetal hematocrit of approximately one percent per day is expected if the fetus has no hydrops (1.88 with hydrops) [2, 4, 7]. Therefore, a second transfusion will be necessary in about ten to 14 days after, depending on the hematocrit and the post-transfusion results; after the third, it is prudent to separate them three to four weeks by the suppression of fetal erythropoiesis [6, 7]. Subsequently, Doppler of the middle cerebral artery is not advised, by the presence of adult hemoglobin [2]. Ideally, they should be performed between 18 and 35 weeks (poor visualization of structures before this threshold and with risk of childbirth being lower after week 35 than transfusion) [6, 7].
Although data are still limited, fetal prognosis is good, with about 90% of children reaching a normal neurological development, even in the presence of hydrops [2, 3, 6, 7]. Delivery should be scheduled at a tertiary center [1-6].
After the onset of fetal hydrops, is important to rule out the diagnosis of anaemia. The infectious aetiology should be investigated in fetal anaemia, namely parvovirus B19 infection and Rh isoimmunization, with even more severe and early recurrences. Surveillance is critical for fetal optimization. Anaemia can be severe and benefit from intrauterine transfusion, optimizing maternal-fetal prognosis.