


Clinical and Experimental Obstetrics & Gynecology (CEOG) is published by IMR Press from Volume 47 Issue 1 (2020). Previous articles were published by another publisher on a subscription basis, and they are hosted by IMR Press on imrpress.com as a courtesy and upon agreement with S.O.G.
 , B. Nikolic 1,2, A. Jurisisc 1,2, N. Zečević 1,2, R. Aničić 1,2, M. Jeftović 3
, B. Nikolic 1,2, A. Jurisisc 1,2, N. Zečević 1,2, R. Aničić 1,2, M. Jeftović 31 The Obstetrics and Gynecology Clinic Narodni Front, Belgrade, Serbia
2 University of Belgrade School of Medicine, Belgrade, Serbia
3 Clinic of Gynecology and Obstetrics, Clinical Center of Serbia, Belgrade, Serbia
Abstract
Cervical pregnancy is a rare form of ectopic pregnancy with frequency less than 1%. Etiology is not sufficiently clarified, and a treatment depending on several factors begins with a conservative one, mainly in asymptomatic patients, and most often goes from methotrexate, through curettage to hysterectomy in case of profuse and life threatening bleeding. The present case reports a 35-year-old patient, without most commonly mentioned etiological factors for cervical pregnancy, who underwent curettage in eight weeks of amenorrhea with administration of a chemical coagulant, human fibrinogen, and human thrombin set.
Keywords
- Cervical ectopic pregnancy
- Curettage
- Chemical coagulant
- Human fibrinogen
- Human thrombin
Cervical pregnancy is a rare and dangerous form of ectopic pregnancy. Incidence of this form of heterotopic pregnancy is less than 1% of all ectopic pregnancies, (1 per 2,500-18,000 pregnancies). [1] Etiology is not sufficiently clear, but the use of an intrauterine device, previous curettage or cesarean sections, and most of all artificial reproductive technology (ART), may have an important role. It is most often presented as painless vaginal bleeding, which depending on its intensity, may be life threatening, but can also be asymptomatic. Therapy approachs are very diverse, from conservative treatment with methotrexate to more radical treatment such as hysterectomy [2]. In the case presented here, the treatment consisted of curettage with application of chemical coagulant, human fibrinogen, and human thrombin set, which arrested the bleeding completely.
A healthy, 35-year-old patient without previous labors and abortions came for examination due to absence of menstruation and poor painless vaginal bleeding. A period of amenorrhea lasted for a seven weeks and two days. At examination, poor brown vaginal discharge from the cervical canal was noticed under a speculum. Bimanual examination revealed an elongated, enlarged, and softened cervix, and the adnexa was bilaterally free and insensitive. Ultrasonography revealed empty cavum uteri with decidual alteration of endometrium being 8.41-mm thick and the gestational sac off diameter 16.35 mm in the cervical canal without visible embryonic echo (Figure 1). The internal os was closed and the cervix enlarged with present vascularization of chorionic tissue verified by color Doppler (Figures 1 and 2). B-hCG value was 25,538 IU/L. General condition of the patient and vital parameters were stable, and complete blood count was normal. On the second day of the patient hospitalization, the patient underwent curettage with local application of chemical coagulant, human fibrinogen and human thrombin set, and sutures were placed at the level of the internal os of uterus at positions 3, 6, 9 and 12 o’clock. On day 2 after the intervention was performed, values of B-hCG dropped to 8,880 IU/L, and after eight days they were 62 IU/L. The patient was discharged from the clinic in good general condition and was advised for further follow-ups.
 Figure 1.
Figure 1.— Ultrasonography view of the gestational sac in the cervical canal. OUI - closed internal os.
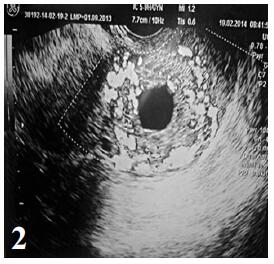 Figure 2.
Figure 2.— Doppler view of flow within chorionic tissue
Cervical pregnancy is one of the rarest forms of ectopic pregnancies and most commonly it is a consequence of ART [1]. Risk factors include cervical and uterine anomalies, previous curettages or cesarean sections, smoking, tubal factor infertility or IVF treatment [3]. It can be asymptomatic, but patients usually attend the clinic due to heavy painless vaginal bleeding. Paalman and McElin described the most acceptable clinical criteria for the diagnosis of cervical pregnancy: 1) painless bleeding from the uterus after period of amenorrhea, 2) disproportionately enlarged cervix, 3) ovular tissue completely placed in endocervix, and 4) closed internal os of the uterus with partially open external os of the uterus [4]. Ushakov et al. established that diagnostic accuracy by the transvaginal US examination is 87.5% [5]. In other cases, MRI can be successfully used as an additional method [6-8]. In differential diagnosis, cervical pregnancy can be misinterpreted as spontaneous abortion when pregnancy tissue is found within the cervical canal [9]. In the case presented here, all aforementioned criteria for diagnosis of cervical pregnancy were met by ultrasonography and therefore an additional diagnostic procedure was not necessary. In the case of spontaneous abortion, there is the open internal os, cervix is not elongated and enlarged, and bleeding is often followed by pain. There are various approaches to the treatment of cervical pregnancy. A conservative treatment with methotrexate can be used in patients without pronounced symptomatology. In patients with vaginal bleeding, the treatment is most often the curettage, and in case of profuse bleeding which endangers patient’s life, hysterectomy is performed [10]. Patients should be informed on potential risks for future ectopic pregnancies and spontaneous abortions due to possible cervical insufficiency.