


 , Diana Melissa Quant 2, Talía Gómez Yepes 3,*
, Diana Melissa Quant 2, Talía Gómez Yepes 3,* , Edgardo Etchezahar 3, Paulina Arenas Landgrave 4
, Edgardo Etchezahar 3, Paulina Arenas Landgrave 41 Foro Foundation for Mental Health, C1428 Buenos Aires, Argentina
2 Center for Research in Social and Human Sciences, Fundación Seré, 110221 Bogotá, Colombia
3 Faculty of Teacher Training and Education, Autonomous University of Madrid, 28049 Madrid, Spain
4 Faculty of Psychology, National Autonomous University of Mexico, 04510 Ciudad de México, Mexico
Abstract
Dialectical Behavior Therapy (DBT) is a psychotherapeutic program developed to treat borderline personality disorder (BPD). Given the conceptualization of behavioral problems as the result of a skills deficit, skills training is presumed to be one of the primary active components of the DBT program. It is therefore essential to be able to assess the learning and use of DBT skills to manage life problems. The main objective of the study was to develop and validate the Dialectical Behavior Therapy Skills (Habilidades in spanish) scale (DBT-H) in the Argentine context. The DBT-H was designed to measure five key dimensions: Mindfulness, Interpersonal Effectiveness, Emotional Regulation, Distress Tolerance, and Radical Acceptance.
A convenience non-clinical sample of 1006 Argentine adults was assessed (58.3% women, 40.6% men, and 1.1% identified as “non-binary”), with an age range from 18 to 80 years (M = 42.33; SD = 13.21). We analyze the DBT-H, along with standard measures, including the Satisfaction with Life Scale (SWLS), the Mindfulness Attention Awareness Scale (MAAS), and the Difficulties in Emotion Regulation Scale (DERS).
Initial descriptive analysis confirmed that all DBT-H items adequately contributed to their respective subscales, with high item-total correlation and no skewness or kurtosis biases affecting their distribution. Confirmatory factor analysis supported the five-factor structure, consistent with the DBT skills components proposed by Linehan. Higher DBT-H scores were reliably associated with greater life satisfaction (SWLS) and mindfulness (MAAS). This relationship suggests that DBT skills effectively contribute to improving well-being and mindful awareness in individuals. Additionally, higher DBT-H scores correlated with fewer difficulties in emotional regulation (DERS), indicating a direct link between mastery of DBT skills and better emotional regulation.
The validation of the DBT-H as a reliable and valid tool for assessing DBT skills in the Argentine context is a significant step toward studying the efficacy of various interventions.
Keywords
- DBT
- assessment
- mindfulness
- interpersonal effectiveness
- emotional regulation
- distress tolerance
- radical acceptance
Dialectical Behavior Therapy (DBT, Linehan, 1993a) is a psychotherapeutic program developed to treat borderline personality disorder (BPD). BPD is characterized by marked emotional, interpersonal, behavioral, and self-image instability (American Psychiatric Association, 2013). A growing body of research indicates that DBT is an effective therapy for people diagnosed with BPD in both inpatient and outpatient settings (e.g., Andreasson et al., 2016; Bloom et al., 2012; DeCou et al., 2019; Linehan et al., 2006; Lynch et al., 2007; McMain et al., 2009; Panos et al., 2013).
DBT is based on a skills deficit model, which suggests that difficulties in coping with life problems and stressful events are due to a lack of skills and motivation. According to the biosocial model (Linehan, 1993a), patients with emotional dysregulation do not have the necessary skills to manage healthily with emotional arousal (Crowell et al., 2009). As a result, DBT aims to achieve five key functions within a comprehensive treatment program: (1) increasing patients’ capabilities, (2) boosting clients’ motivation, (3) generalizing skills to necessary contexts, (4) structuring the environment to reinforce desired behaviors and reduce problematic ones, and (5) enhancing the motivation and skills of therapists. To accomplish these goals, DBT comprises four treatment components or modes: group skills training, telephone coaching to promote skills generalization, individual therapy, and therapist consultation team meetings (Linehan, 1993a; Prillinger et al., 2024).
Group skills training is designed to enhance skills in the four areas of dysregulation proposed by the model: emotional, interpersonal, behavioral, and cognitive/self-dysregulation (Linehan, 1993a). The training is divided into four skill modules that correspond to each area of dysregulation: (1) Mindfulness skills, aimed at observing, describing, and participating without judgment while being effective; (2) Interpersonal Effectiveness skills, for training in making requests, saying no, maintaining relationships, and self-respect; (3) Emotional Regulation skills, for training awareness and labeling of emotions, changing emotional responses, and reducing emotional vulnerability; and (4) Distress Tolerance skills, for training crisis-response strategies without worsening the situation and radical acceptance of difficult life events (Linehan, 1993b; Linehan et al., 2015; Syversen et al., 2024).
Given the conceptualization of behavioral problems as the result of a skills deficit, skills training is presumed to be one of the primary active components of the DBT program. Several studies have demonstrated that DBT skills training is a central component of treatment (e.g., Decker et al., 2019; Hatoum and Burton, 2024; Linehan et al., 2015; Miller et al., 2000; Neacsiu et al., 2010b; Nelson-Gray et al., 2006; Probst et al., 2018; Soler et al., 2009). It is therefore essential to be able to assess with a reasonable degree of reliability the learning and use of DBT skills to manage life problems.
Prior to 2010, no specific instrument existed for evaluating the use of DBT skills. Studies employed a range of psychometrically robust instruments that collectively aimed at evaluating the skills included in the various DBT modules (e.g., Revised Ways of Coping Checklist [RWCCL], Vitaliano et al., 1985; Coping Strategies Evaluation [CSE], Chesney et al., 2006; Coping Responses Inventory [CRI], Moos, 1997; Ways of Coping Scale [WCS], Lazarus and Folkman, 1984; Difficulties in Emotion Regulation Scale [DERS], Gratz and Roemer, 2004; Emotion Regulation Questionnaire [ERQ], Gross and John, 2003; Difficulties in Emotion Regulation Scale [DTS], Simons and Gaher, 2005; Kentucky Inventory of Mindfulness Skills [KIMS], Baer et al., 2004; Mindful Attention Awareness Scale [MAAS], Brown and Ryan, 2003).
While many of these instruments include items related to DBT-taught skills, some skills are not represented, and therefore not included in the evaluation scope. Another limitation is that the items sometimes refer to broad coping methods rather than specific skills use. A third limitation is that some instruments assess the use of strategies in general, rather than specifically in contexts characterized by stress or problematic situations (Vijayapriya and Tamarana, 2023).
To overcome these limitations, Neacsiu et al. (2010a) developed the only
instrument specifically designed to evaluate DBT skills: the DBT-WCCL
(Dialectical Behavior Therapy Ways of Coping Checklist). The DBT-WCCL is an
adaptation of a pre-existing scale that was not specifically designed for DBT
skills assessment: the RWCCL (Revised Ways of Coping Checklist; Vitaliano et al., 1985). During the development of this new instrument, items from the
original scale were retained, and some new items were generated and tested by DBT
experts. The final DBT-WCCL contains 59 self-report items assessing the frequency
of use of effective skills and the frequency of use of ineffective strategies for
managing difficult situations over the past month. Frequency is measured on a
scale from 0 to 3, with 0 = Never used and 3 = Frequently used.
The scale has two factors: one assesses coping through DBT skills use (DBT Skills
Subscale [DSS]) and the other assesses dysfunctional coping (Dysfunctional Coping
Subscale [DCS]). Examples of DSS items include “I tried to stay focused before
taking action” and “I was able to come up with several different solutions to
my problem”. Examples of DCS items include “I blamed myself” and “I refused
to think that it happened”. The scale is easy to understand without prior DBT
knowledge and shows high internal consistency (
The DBT-WCCL has been used in several studies (e.g., Chugani et al., 2013; Neacsiu et al., 2014; Rizvi and Steffel, 2014; Ward-Ciesielski, 2013). There is also evidence that skill acquisition, as evaluated by the DBT-WCCL, plays a role in determining treatment outcomes (Neacsiu et al., 2010b).
Despite its adequate psychometric properties, we believe that the DBT-WCCL has two limitations. The first concerns the lack of context in some items to evaluate specific DBT skills. These items are often concise and lack sufficient detail regarding the specific situation in which the skill would be most effectively applied. Without context, some items in the DBT-WCCL might lose sensitivity in assessing skill use-in-context. For example, the item “I treated myself to something tasty” could be a skillful behavior (when distress tolerance is needed) or an ineffective behavior (when problem-solving is required), depending on the context.
The second limitation is the absence of items evaluating very relevant DBT skills, such as describing instead of interpreting and judging, doing one thing at a time, opposite action, describing emotional responses, and anticipating. These skills are fundamental to the training process, and the incorporation of items that reflect them could facilitate a more comprehensive evaluation.
This research aimed to develop a new instrument (DBT-H, Dialectical Behavior Therapy Habilidades “skills in Spanish”) with easy-to-understand language, not requiring prior DBT knowledge, that incorporates contextual information and is tailored to the specific demands of DBT skills assessment. Additionally, the project aimed to analyze the relationships between DBT-H and other relevant variables such as mindfulness, life satisfaction, and difficulties in emotional regulation. The following hypotheses were proposed: higher DBT-H scores will correlate positively with higher scores in Mindful Attention Awareness Scale (MAAS) and Satisfaction Whit Life Scale (SWLS), and negatively with higher scores in Difficulties in Emotion Regulation Scale (DERS).
The sample was selected for convenience and consisted of 1006 adults from different regions of Argentina, aged between 18 and 80 years (M = 42.33; SD = 13.21). Of these, 58.3% were women, 40.6% were men, and 1.1% identified as “non-binary”. Regarding educational level, 3.3% of the sample had only completed primary education (either fully or partially), 25.1% had completed secondary education (either fully or partially), 32.5% had a tertiary education (comparable to an associate’s degree), and 39.1% had completed university studies. In terms of social class, 10.2% of participants identified as lower class, 38.7% as lower-middle class, 42.3% as middle class, and 8.8% as upper class.
DBT-H Scale. The scale was developed to assess five groups of skills across a total of 35 items (see Table 1). The subscales are Mindfulness (e.g., “When I engage in activities, I feel fully involved with what I am doing and do not think about anything else”, “I can distinguish facts from my own interpretations of those facts”), Interpersonal Effectiveness (e.g., “In my interpersonal relationships, I can express my opinions and protect what is important to me”, “I know how to reduce behaviors from myself or others that I dislike”), Emotional Regulation (e.g., “I tend to check if I am interpreting the situation correctly before taking action”, “When I feel a strong emotion, I make sure to have the correct information before taking a course of action”), Distress Tolerance (e.g., “When I have a problem I cannot solve immediately, I manage to think about something else”, “I know how to calm myself down when I experience intense emotions”), and Radical Acceptance (e.g., “I try to be effective in my actions, setting aside who is right”, “I can move forward despite facing unexpected obstacles”). The response format of the scale is Likert-type, with five response options ranging from 1 = Never to 5 = Always. Higher scores indicate a higher level of proficiency in each skill.
| Mindfulness ( |
M | SD | S | K | r-i | |
| 1. I can focus my mind on what I am doing, without getting distracted by thinking about other things. | 3.66 | 0.96 | –0.69 | 0.18 | 0.58 | 0.78 |
| 6. I can notice the thoughts that come into my mind without being carried away by them. | 3.44 | 0.99 | –0.36 | –0.34 | 0.47 | 0.80 |
| 11. I feel fully involved in what I am doing and do not think about anything else. | 3.80 | 0.94 | –0.51 | –0.24 | 0.64 | 0.77 |
| 16. I can distinguish between the facts and my own interpretations of those facts. | 3.95 | 0.85 | –0.80 | 0.79 | 0.41 | 0.81 |
| 21. I can participate in activities without getting distracted. | 3.85 | 0.87 | –0.74 | 0.56 | 0.63 | 0.77 |
| 26. When I decide, I am able to pay attention to what is happening without thinking about the past or the future. | 3.73 | 0.99 | –0.66 | 0.01 | 0.53 | 0.79 |
| 31. I feel connected to what I am doing. | 4.14 | 0.75 | –0.79 | 1.02 | 0.59 | 0.78 |
| Interpersonal Effectiveness ( |
||||||
| 2. I know how to ask others for what I need. | 3.61 | 1.12 | –0.35 | –0.93 | 0.51 | 0.78 |
| 7. If I need someone to change their behavior, I know how to bring it up. | 3.32 | 0.95 | –0.21 | –0.29 | 0.58 | 0.76 |
| 12. I manage to maintain important relationships for me by balancing my desires with those of others. | 3.73 | 0.88 | –0.61 | 0.25 | 0.51 | 0.77 |
| 17. In my interpersonal relationships, I can express my opinions and take care of what is important to me. | 4.05 | 0.77 | –0.60 | 0.20 | 0.55 | 0.77 |
| 22. I know how to reduce behaviors of mine or others that I don’t like. | 3.60 | 0.84 | –0.48 | 0.36 | 0.51 | 0.77 |
| 27. I know how to communicate that someone’s behavior was not to my liking or was not good for me. | 3.57 | 1.00 | –0.26 | –0.56 | 0.54 | 0.77 |
| 32. I know how to increase behaviors of mine or others that I like. | 3.74 | 0.87 | –0.46 | 0.02 | 0.53 | 0.77 |
| Emotional Regulation ( |
||||||
| 3. I usually make sure I am interpreting the situation correctly before acting. | 3.71 | 0.92 | –0.58 | 0.10 | 0.57 | 0.81 |
| 8. When I feel intense emotion, I make sure I have the correct information before taking any course of action. | 3.71 | 0.98 | –0.61 | –0.04 | 0.62 | 0.80 |
| 13. When I have a problem, I can think of different ways to solve it and choose the one that is most likely to be helpful. | 4.05 | 0.88 | –0.90 | 0.71 | 0.51 | 0.82 |
| 18. Even when I am experiencing intense emotions, I can identify what is most helpful for me and do it. | 3.52 | 0.92 | –0.29 | –0.40 | 0.54 | 0.81 |
| 23. When I act, I consider the possible consequences of my behavior. | 3.88 | 0.98 | –0.74 | 0.01 | 0.62 | 0.80 |
| 28. I can do something different from what my emotion urges me to do if that is the best thing for me (for example: not fighting even when feeling angry). | 3.71 | 0.92 | –0.52 | 0.01 | 0.56 | 0.81 |
| 33. I usually pay attention to the consequences of my behavior when deciding how to act. | 3.82 | 0.88 | –0.81 | 0.77 | 0.63 | 0.80 |
| Distress Tolerance ( |
||||||
| 4. When I feel intense emotion, I can do things to calm myself down. | 3.64 | 0.86 | –0.46 | 0.25 | 0.54 | 0.86 |
| 9. I can help myself get through a painful situation by giving myself a pleasant moment—like going for a walk, having a nice tea, praying, etc. | 3.45 | 1.08 | –0.29 | –0.68 | 0.62 | 0.85 |
| 14. When I have a problem that I cannot solve immediately, I can manage to think about something else. | 2.91 | 1.05 | 0.10 | –0.57 | 0.63 | 0.85 |
| 19. I know how to calm myself when I feel an emotion very intensely. | 3.39 | 0.94 | –0.18 | –0.40 | 0.67 | 0.84 |
| 24. I know how to improve the moment for myself when I am in a painful situation—taking a break, doing something special for myself, etc. | 3.31 | 1.00 | –0.14 | –0.53 | 0.75 | 0.83 |
| 29. When it’s not helpful to keep thinking about the same thing, I know how to distract myself. | 3.26 | 1.02 | –0.13 | –0.62 | 0.71 | 0.84 |
| 34. I am able to take a pause before acting, even in difficult situations. | 3.44 | 0.93 | –0.41 | –0.03 | 0.57 | 0.86 |
| Radical Acceptance ( |
||||||
| 5. I plan my actions based on how things are rather than how they “should be”. | 3.67 | 0.90 | –0.55 | 0.21 | 0.32 | 0.71 |
| 10. I stick to my plans or projects even if the conditions are not exactly what I expected. | 3.48 | 0.96 | –0.12 | –0.61 | 0.32 | 0.71 |
| 15. I recognize that painful moments in life are inevitable. | 4.46 | 0.82 | –1.92 | 2.13 | 0.29 | 0.71 |
| 20. I can make the necessary changes and do whatever the situation requires to achieve my goals. | 3.72 | 0.86 | –0.42 | 0.04 | 0.53 | 0.66 |
| 25. I try to be effective in my actions, putting aside who is right. | 3.48 | 0.94 | –0.52 | 0.17 | 0.43 | 0.68 |
| 30. I can move forward even when I encounter unexpected obstacles. | 3.97 | 0.76 | –0.44 | 0.22 | 0.56 | 0.65 |
| 35. I manage to let go of the debate over who is right and prioritize what is important to me. | 3.78 | 0.94 | –0.48 | –0.29 | 0.55 | 0.65 |
Note. S, Skewness; K, Kurtosis; r-i, item-total
correlation;
Satisfaction with Life Scale (SWLS; Diener et al., 1985), Spanish version
(Dimitrova and Domínguez, 2015; Esnaola et al., 2017). The SWLS measures subjective
criteria of life satisfaction with five items (e.g., “In most ways, my life is
close to my ideal”, “So far, I have achieved the things that are important to
me in life”, “If I could live my life over, I would change almost nothing”).
The SWLS uses a seven-point Likert response format, ranging from 1 = Strongly
disagree to 7 = Strongly agree. The scale’s consistency was adequate for this
study (
Mindful Attention Awareness Scale (MAAS; Brown and Ryan, 2003), Spanish
version (Barajas and Garra, 2014). The MAAS is a unidimensional scale
consisting of 15 items (e.g., “I tend to walk quickly to get where I am going
without paying attention to what I experience along the way”), using a six-point
Likert scale (from 1 = Almost always to 6 = Almost never) to assess the trait of
mindfulness in daily life. Higher scores indicate higher levels of mindfulness.
The Cronbach’s alpha of the original scale was
Difficulties in Emotion Regulation Scale (DERS). The DERS (Gratz and Roemer, 2004) is a self-report measure with 36 items across six facets (Clarity,
Impulse, Goals, Awareness, Acceptance, and Engagement) of emotional regulation.
Items are rated on a scale from 1 = Almost never (0–10%) to 5 = Almost always
(91–100%). Internal consistency for each dimension was adequate
(0.712
Ad hoc Sociodemographic Questionnaire. Participants were asked to provide information on their age, gender, education level, and social class.
Individuals who met the age criteria (18 years or older) and geographic region requirements were invited to participate through social media (Facebook, Instagram, and Twitter), based on predetermined quotas for sample distribution, to complete a survey (we use Survey Monkey platform, Survey Monkey Inc., San Mateo, CA, USA; version current as of 2025). Participants who did not answer more than 5% of the survey were excluded from the final analysis. Additionally, the survey platform also monitored participants’ IP addresses to prevent duplicate responses. The sample was one of convenience (not representative of the population). Participants were informed that the data collected in this study would be used solely for academic and scientific purposes and would be protected in accordance with Argentina’s National Law 25,326 on the protection of personal data. All procedures conducted in our study adhered to the ethical standards of the institutional research committee and the 1964 Helsinki Declaration and its subsequent amendments or comparable ethical standards. Participants then completed the protocol—administered online— which included all the measures. The DBT-H scale items were developed based on five skill groups: Mindfulness, Interpersonal Effectiveness, Emotional Regulation, Distress Tolerance, and Radical Acceptance.
First, a descriptive analysis of the DBT-H items (means, standard deviations,
and dispersion measures) was conducted. For skewness and kurtosis, the parameters
proposed by Botella et al. (1993) were followed, where values between –1.4
and 1.4 are considered adequate. For item-total correlation (r-i), the
recommendations of Hair et al. (2010) were followed (adequate value
First, the descriptive statistics of the DBT-H items were analyzed (Table 1). All indicators were adequate for the 35 items of the scale. No skewness or kurtosis biases were observed according to the parameters proposed by Botella et al. (1993), and all components added reliability to their respective factor. Overall, all items contributed appropriately to their respective subscale, as they showed an adequate correlation with the total scale, and the reliability of each subscale did not improve by removing any item.
As can be seen in Table 1, all the descriptive statistics were adequate for the DBT-H scale items. No skewness or kurtosis bias was observed, and all items added reliability to their own factor. In general, all the items contribute adequately to the set of each subscale, since they present’s an adequate correlation with the total scale, and the reliability of each subscale it is not improved by eliminating any item.
Next, the construct validity of the DBT-H was analyzed, exploring whether the
data presented an adequate fit for the second-order model with five correlated
factors (Fig. 1). The model fit indicators were adequate for the sample used
(
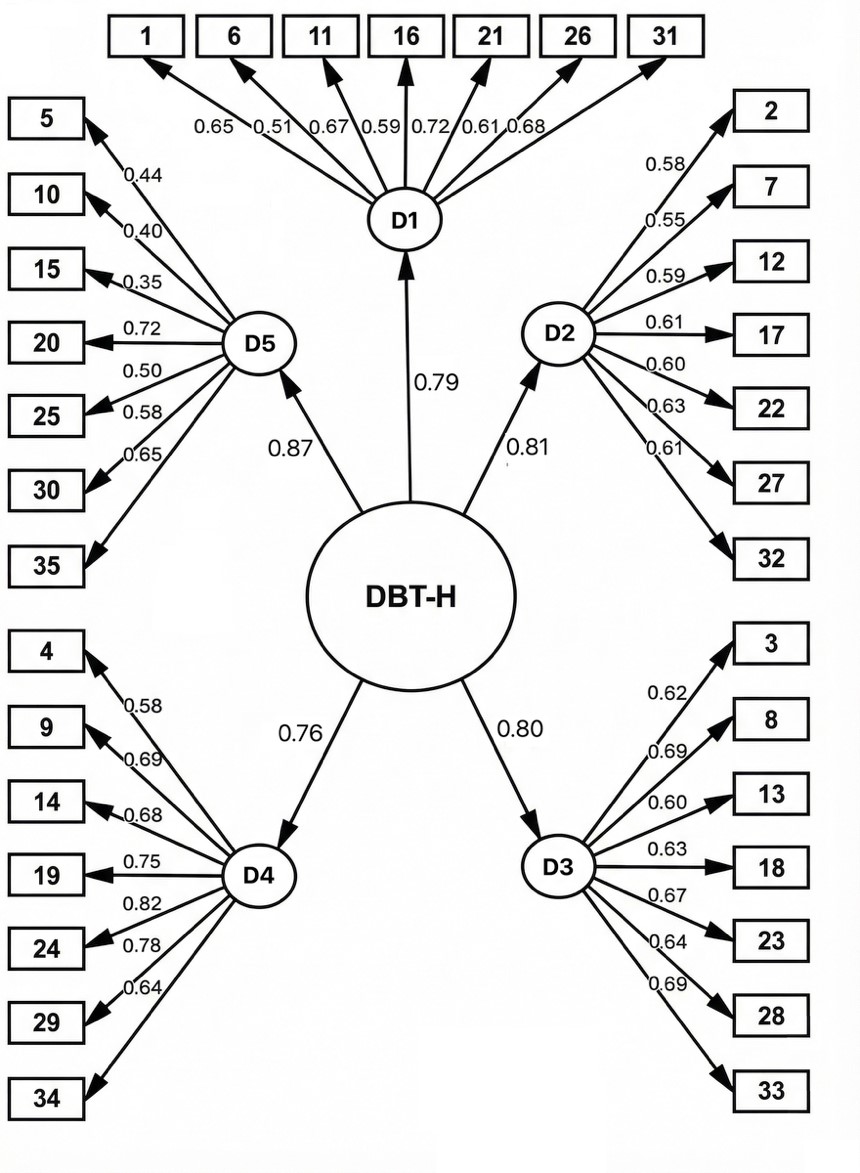 Fig. 1.
Fig. 1.
Second-order model for the five Dialectical Behavior Therapy skill groups. Note. D1: Mindfulness; D2: Interpersonal Effectiveness; D3: Emotional Regulation; D4: Distress Tolerance; D5: Radical Acceptance.
To examine whether the scale demonstrated factorial invariance across gender, we
conducted a multi-group confirmatory factor analysis (CFA) comparing the fit of a
model with equality constraints on factor loadings and intercepts for males and
females. The results indicated that the model did not demonstrate strong
factorial invariance across gender. Specifically, the comparison of the
configural model (no equality constraints) to the model with equality constraints
on factor loadings and intercepts showed a non-significant change in fit
(
Furthermore, to increase the empirical support we calculated the convergent and
discriminant validity for the CFA model. Convergent validity was assessed using
AVE, and the results indicate that all factors met
the recommended threshold of AVE
Subsequently, the relationships between the total scale and the five dimensions of the DBT-H, the SWLS, MAAS, and the dimensions of the DERS were analyzed (Table 2).
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | |
| 1. DBT-H | 0.911 (0.864) | 0.767** | 0.785** | 0.801** | 0.815** | 0.785** | 0.411** | 0.560** | –0.270** | –0.319** | –0.253** | –0.190** | –0.185** | –0.233** |
| 2. DBT -Mindfulness | 0.813 (0.789) | 0.565** | 0.486** | 0.505** | 0.533** | 0.330** | 0.489** | –0.173** | –0.275** | –0.210** | –0.151** | –0.174** | –0.218** | |
| 3. DBT - Interpersonal Effectiveness | 0.800 (0.807) | 0.537** | 0.504** | 0.537** | 0.318** | 0.412** | –0.114* | –0.194** | –0.146** | –0.051 | –0.098* | –0.093 | ||
| 4. DBT - Emotional Regulation | 0.834 (0.796) | 0.569** | 0.580** | 0.222** | 0.461** | –0.168** | –0.300** | –0.311** | –0.242** | –0.215** | –0.164** | |||
| 5. DBT - Distress Tolerance | 0.870 (0.833) | 0.516** | 0.383** | 0.464** | –0.168** | –0.202** | –0.155** | –0.116* | –0.107* | –0.132** | ||||
| 6. DBT - Radical Acceptance | 0.720 (0.760) | 0.307** | 0.377** | –0.195** | –0.243** | –0.201** | –0.158** | –0.171** | –0.182** | |||||
| 7. SWLS | 0.912 | 0.263** | –0.169** | –0.200** | –0.136** | –0.119* | –0.105* | –0.141** | ||||||
| 8. MAAS | 0.814 | –0.326** | –0.391** | –0.323** | –0.266** | –0.275** | –0.315** | |||||||
| 9. DERS Clarity | 0.775 | 0.439** | 0.389** | 0.357** | 0.292** | 0.375** | ||||||||
| 10. DERS Impulses | 0.876 | 0.507** | 0.364** | 0.483** | 0.413** | |||||||||
| 11. DERS Goals | 0.771 | 0.392** | 0.482** | 0.391** | ||||||||||
| 12. DERS Awareness | 0.819 | 0.400** | 0.452** | |||||||||||
| 13. DERS Acceptance | 0.749 | 0.406** | ||||||||||||
| 14. DERS Strategies | 0.712 |
Note. On the diagonal, Cronbach’s alpha (
**p
The Omega-subscale values indicate that each subscale demonstrates adequate
reliability (
The results indicated that all variables were significantly related (Table 2)
with varying strength, both for the total DBT-H and its dimensions. To address
the potential issue of false positives due to the large number of correlations
analyzed, we applied a correction method based on the Q-value approach. The
Q-value was calculated using the Benjamini-Hochberg procedure to control the
False Discovery Rate (FDR). We used a threshold of Q
The aim of this research was the development of a scale to assess DBT skills (DBT-H) in the Argentine population, providing a relevant tool for measuring the impact of the DBT skills training component (Linehan, 1993a; McMain et al., 2009) in treating personality disorders and complex issues related to emotional dysregulation. Additionally, the study explored the relationships between DBT-H and relevant variables such as mindfulness, life satisfaction, and emotional regulation difficulties. The results support the validity and reliability of DBT-H in evaluating DBT skills in everyday contexts. Five key factors were identified: Mindfulness, Interpersonal Effectiveness, Emotional Regulation, Distress Tolerance, and Radical Acceptance, aligning with the proposals of Neacsiu et al. (2010b) and Linehan (2015) and consistent with the arguments made by Dixon-Gordon et al. (2015), and in accordance with the specific needs of the biosocial model underlying DBT therapy. Significant relationships were observed between DBT skills and variables such as mindfulness (MASS), emotional regulation (DERS), and life satisfaction (SWLS). These links not only reinforce the central role of mindfulness in DBT but also highlight the effectiveness of the therapy in improving emotional regulation and enhancing quality of life in individuals with borderline personality disorder or severe emotional regulation difficulties, associating an increase in DBT skills with improved perceptions of life satisfaction (Linehan, 1993a; Neacsiu et al., 2010b). The positive correlation between DBT skills and MASS emphasizes the importance of mindfulness as a critical component of DBT, while the negative relationship with DERS suggests that greater mastery of DBT skills may contribute to a reduction in emotional dysfunction. These dynamics indicate how DBT skills training can effectively mitigate the emotional and behavioral challenges presented by personality disorders.
The development and validation of the DBT Skills Scale (DBT-H) in a Spanish-speaking context is crucial, given the proven efficacy of DBT in treating borderline personality disorder. The results confirm the efficacy of DBT-H as a valid tool for assessing DBT skills, supporting Linehan’s (1993a) skills deficit model, which posits that the absence of critical skills and motivation is fundamental to emotional dysregulation and leads to risky behaviors. Thus, having DBT-H available in clinical contexts is significant, as it allows individual therapists and skills trainers to accurately assess the level of skill acquisition and generalization by clients, facilitating the identification of specific actions to strengthen necessary skills. When patients begin DBT treatment, patients typically exhibit a level of dysregulation that impedes the learning process, as a consequence of amygdala hyperreactivity (Barrós-Loscertales et al., 2006); having additional information beyond clinical observation and self-monitoring helps clinicians to identify areas of greatest difficulty in skills and to make adjustments to treatment plans that are focused on the specific needs of clients.
The factor analysis confirmed the adequacy of the five-factor model, which aligns with the structure of DBT skills training and underscores the relevance of assessing each skill group within its specific context. This feature of DBT-H allows clinicians and researchers to determine the effectiveness of the skills in varied contexts, ensuring a more precise and evidence-based practical application. In clinical practice, DBT-H is regarded as an invaluable instrument, facilitating a contextualized assessment of skills. This is particularly relevant given that DBT, as a treatment, emphasizes the importance of adapting interventions to specific situations faced by clients, which is essential for effectively managing the emotional and behavioral dysregulation associated with disorders such as BPD (Linehan, 1993b; Linehan et al., 2015). For example, mindfulness is evaluated not only in terms of presence and awareness but also in how these aspects are applied during real stress situations, which is crucial for effectively managing emotional reactivity (Neacsiu et al., 2010b). By accurately identifying which specific skills need strengthening, professionals can adjust the therapeutic plan to focus on areas that maximize therapeutic benefit, optimizing long-term outcomes and reducing the incidence of relapses (Soler et al., 2009).
From a research perspective, DBT-H’s ability to assess the effectiveness of skills in specific contexts offers a valuable opportunity to study the application and outcomes of DBT skills training. This detailed evaluation allows researchers to not only corroborate the effectiveness of individual components of DBT treatment but also to understand how and when these skills are most effectively applied in clients’ daily lives. This analytical capability is essential for the ongoing development of DBT and for adjusting its methods and techniques to increase its overall effectiveness (Linehan et al., 2006; Neacsiu et al., 2010b). Additionally, it enables longitudinal studies that can trace the evolution of skills acquisition over time, providing relevant data on the sustainability and long-term impact of skills training on patients’ lives (McMain et al., 2009).
It can be observed that although the items were categorized according to the skills modules taught in a skills training workshop, the specific division of the distress tolerance module demonstrates the comprehensive and detailed approach to skills training for emotional crises and acceptance skills. The skills corresponding to this group were divided into two categories: those specifically oriented toward distress tolerance and those focused on radical acceptance. This division is logical, as learning to manage a crisis comprises a set of skills that enable individuals to tolerate distress and direct their behavior toward long-term goals; while radical acceptance is associated with the ability to recognize reality as it is, which is a more complex skill that develops once individuals have learned to effectively manage their crises and achieve greater mastery of their emotional experience.
Despite the robustness of the findings, the limitations of this study include its focus on a single linguistic and cultural region (Argentina), raising questions about the representativeness and generalizability of the findings to other Spanish-speaking contexts. Therefore, future research should explore the behavior of the scale in different Latin American countries, enabling therapists to have an instrument to identify the progress in skill acquisition in individuals within the framework of a DBT program, particularly in cases where skills training is the sole treatment option for addressing complex emotional issues. It is recommended that the DBT-H be applied and validated in clinical samples and among adolescents and individuals with basic educational levels. This will facilitate the utilization of the tool in other Spanish-speaking countries and enable an understanding of its psychometric properties in different subgroups and clinical contexts. Future research should also assess the scale’s sensitivity to change in clinical contexts to provide studies that specifically evaluate the impact of this component on client outcomes.
This study provides a solid foundation for psychotherapy and psychological assessment, emphasizing the need for valid and reliable instruments like DBT-H for Spanish-speaking populations. DBT emphasizes that a generalized skills deficit is a crucial maintenance factor for severe emotional regulation problems. Therefore, increasing individuals’ capacity to have new repertoires for effectively coping with life situations is a central focus of intervention. This highlights the importance of having a tool to specifically evaluate the effectiveness of skill use as clients progress in treatment.
The datasets generated during and analyzed during the current study are available from the corresponding author on reasonable request.
PJQ, TGY, and EE: conceptualization, methodology, formal analysis, data curation, validation. PJQ, TGY, EE, DMQ, and PAL: investigation, resources, writing—original draft preparation, writing—review and editing. PJQ and EE: supervision. PJQ, TGY, EE, and DMQ: Project administration. EE: software. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
The study was carried out in accordance with the guidelines of the Declaration of Helsinki, and the protocol was approved by the Scientific Ethical Committee of the National Council for Scientific and Technical Research (Argentina) (Protocol N.° CEI-039/25). All participants gave their informed consent for inclusion before they participated in the study.
Not applicable.
This research received no external funding.
The authors declare no conflict of interest.
Supplementary material associated with this article can be found, in the online version, at https://doi.org/10.31083/BP52649.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.