





 , Lixia Zhong 2,3,†, Ruoyun Ma 3, Zhulin Li 3,4, Juanjuan Zhao 3
, Lixia Zhong 2,3,†, Ruoyun Ma 3, Zhulin Li 3,4, Juanjuan Zhao 31 School of Nursing, Xiamen Medical College, 361023 Xiamen, Fujian, China
2 Department of Clinical Psychology, The Eighth Affiliated Hospital, Sun Yat-sen University, 518000 Shenzhen, Guangdong, China
3 School of Nursing, Sun Yat-sen University, 510080 Guangzhou, Guangdong, China
4 Department of Nursing, Suixian Traditional Chinese Medical Hospital, 441300 Suizhou, Hubei, China
†These authors contributed equally.
Abstract
Non-suicidal self-injury (NSSI) is prevalent among adolescents with mood disorders and often exhibits addictive features. However, the specific subgroups of addictive features and their associations with the functions and severity of NSSI remain unclear.
Between September 2023 and January 2024, this study recruited 182 adolescents aged 10–24 years with mood disorders who engaged in NSSI in the past year. Participants completed assessments including: sociodemographic and clinical characteristics (general questionnaire), depressive symptoms, Hamilton Depression Rating Scale (HAMD), manic symptoms, Young Mania Rating Scale (YMRS), and NSSI addictive features, functions, and severity via the Ottawa Self-Injury Inventory-Chinese Revised Version (OSI-CRV). Latent class analysis (LCA) was employed to identify subgroups based on the 7 items of the addictive features subscale in OSI-CRV. Covariate analysis and mediation analysis were employed to distinguish the associations of latent classes of addictive features with different functions and the severity of NSSI.
LCA identified two distinct classes: High Addiction Class (50.0%) and Low Addiction Class (50.0%). Covariate analysis revealed that patients with younger age (odds ratio [OR] = 0.441, p = 0.017), higher educational level (OR = 0.385, p = 0.043), and greater depressive severity (moderate and severe, OR = 4.500, 4.830; p = 0.046, 0.017) were associated with High Addiction Class. Mediation analysis demonstrated that these addictive features classes indirectly mediated the association between NSSI functions and severity.
These findings highlight the diversity of addictive features and their impact on NSSI, thereby guiding the development of tailored interventions that address the heterogeneity of addictive features.
Keywords
- non-suicidal self-injury
- addictive features
- latent class analysis
- adolescents
- mood disorders
Mood disorders, including major depressive disorder (MDD) and bipolar disorder (BD), are leading causes of disability worldwide (McIntyre et al., 2020). Nearly three-fourths of adolescents with mood disorders have experienced non-suicidal self-injury (NSSI) in the past year (Liu et al., 2023). NSSI is defined as the direct, deliberate, self-inflicted damage to body tissue without suicidal intent and for purposes not socially or culturally sanctioned. Such behaviors may include hitting, cutting, burning, banging, scratching, and other related behaviors (Klonsky et al., 2014; Nock, 2009a). Not only can NSSI cause direct physical damage, but it can also elevate the risk of suicide (Wang et al., 2021; Willoughby et al., 2015). Furthermore, a report by the World Health Organization revealed that self-harm is the third leading cause of the disease burden among children and young adults aged 10–24 years old (GBD 2019 Diseases and Injuries Collaborators, 2020). Consequently, NSSI has emerged as a critical global public health concern, drawing the attention of numerous scholars. However, our understanding of NSSI still needs to be expanded.
Addictive features in NSSI encompass behavioral patterns akin to substance dependence, including tolerance (requiring increasingly frequent/severe self-injury to achieve the same effect), withdrawal (experiencing emotional distress when abstaining), and loss of control (Nixon et al., 2015). For instance, adolescents might report escalating cutting frequency despite physical harm, or persistent urges to self-injure even when aware of negative consequences (Nixon et al., 2015). Repetitive NSSI, in particular, exhibits multiple parallels with substance addiction, providing a comprehensive perspective for understanding this behavior (Nixon et al., 2002). Individuals who engage in NSSI often experience psychological phenomena related to addiction, such as “relapse”, “can’t/don’t want to stop”, and “getting worse/not enough” (Davis and Lewis, 2019). While various tools measure NSSI behaviors, the Ottawa Self-Injury Inventory (OSI) and its derivatives uniquely provide a quantifiable assessment of these addictive features through a subscale adapted from the Diagnostic and statistical manual of mental disorders, 4th ed (DSM-IV) substance dependence criteria (Nixon et al., 2015). Notably, applying this subscale revealed that over half of adolescents and young adults with mental disorders who engage in NSSI report experiencing three or more addictive features (Yan et al., 2024).
It is worth noting that not all individuals who engage in NSSI exhibit overt addictive tendencies. Previous studies on other addictive behaviors, such as gambling (Hong et al., 2009) and internet gaming disorder (IGD) (Colder Carras et al., 2017; Przybylski et al., 2017), has shown that these behaviors can be categorized into distinct addiction-related subgroups. Among individuals who engage in NSSI, latent profile analysis (LPA) and latent class analysis (LCA) have identified specific subgroups based on NSSI methods (He et al., 2023; Kim et al., 2023; Peterson et al., 2019; Reinhardt et al., 2022), functions (Nesi et al., 2021; Sack et al., 2024), motivation to self-injure and not self-injure (Gray et al., 2023), and other other behavioral or psychological characteristics (Chang et al., 2024; Hamza and Willoughby, 2013; Whitlock et al., 2008), as well as their combinations (Bracken-Minor et al., 2012; Case et al., 2020; de Neve-Enthoven et al., 2024; Klonsky and Olino, 2008; Schmidt et al., 2024; Shahwan et al., 2020; Somer et al., 2015). Notably, while addictive features are recognized as central to NSSI maintenance and escalation, their potential to delineate clinically distinct subgroups remains unexplored in latent variable modeling. Crucially, the majority of these studies were conducted in non-clinical populations. Only four investigations examined clinical cohorts, with two studies identifying two distinct groups based on functions (Sack et al., 2024) and methods (He et al., 2023), and two identifying three separate groups (Nesi et al., 2021; Shahwan et al., 2020). These subgroups display varying NSSI patterns and health outcomes, aiding in the identification of heterogeneity within the NSSI population and enhancing the efficiency of interventions. However, despite the profound implications of addictive features for understanding NSSI and guiding treatment, no study has yet explored potential subgroups specifically based on these addictive features. It is therefore imperative to investigate how addiction may stratify the NSSI population and how these subgroups relate to the development, functions, and severity of NSSI.
Prior LPA studies on NSSI functions (Nesi et al., 2021) and methods (Sack et al., 2024) highlight the heterogeneity of self-injury. However, the
addictive dimension of NSSI remains unexplored. This study aims to bridge this
gap by examining how addictive features intersect with functional motivations and
the severity of NSSI. The four-function model (Nock and Prinstein, 2004)
considers NSSI functions as important influence factors to NSSI addiction and
severity. NSSI functions, which refer to the motivations and reasons behind the
development or escalation of NSSI behaviors (Klonsky, 2007), have been
summarized into four broad categories: sensation seeking, internal emotion
regulation (ER), external ER, and social influence (Martin et al., 2013).
Among these, the sensation-seeking domain may be less applicable in the context
of Chinese culture, as it is represented by only two items in exploratory factor
analysis (Chen et al., 2022). Regarding the severity of NSSI, it is generally
perceived as encompassing a higher frequency of NSSI events, a great number of
injured body parts, and a wider variety of self-injury methods (Klonsky et al., 2014; Nock, 2009a). Previous studies have shown that addiction is associated
with both more NSSI functions (Yan et al., 2024) and heightened severity
(Nixon et al., 2015; Ying et al., 2024), which significantly elevates the
complexity of clinical treatment. Additionally, Luo et al. (2024)
demonstrated that addictive features play both mediating and moderating roles in
the relationship of NSSI functions and severity among adolescents with repeated
NSSI (five or more events in preceding year). Critically, NSSI functions,
particularly ER, reinforce addictive features through neurobiological pathways.
When NSSI regulates emotions, it triggers endogenous opioid release (e.g.,
The literature underscores the critical role of addictive features in the development and maintenance of NSSI. However, previous studies have primarily focused on classifying NSSI in community samples using LPA or LCA based on NSSI methods and functions. Few studies have examined the heterogeneity of NSSI in clinical samples or explored its addictive features, leading to an unclear understanding of the interplay between functions, addictive features and severity within clinical adolescent populations. Therefore, this study aims (i) to investigate the potential subgroups of NSSI addictive features by LCA; (ii) to explore the mediating effects of addictive features in the relationship between NSSI functions and severity among adolescents with mood disorders.
The following hypotheses are proposed:
Hypothesis (H1) (subgroups): based on He et al.’s (2023) identification of two distinct NSSI subgroups within a depressed adolescent sample, which closely aligns with our own cohort. We hypothesize that a similar bifurcation of two classes will emerge when classifying according to NSSI addictive features.
H2 (mediation): according to the reinforcement sensitivity theory (RST) (Gray, 1982), we hypothesize that addictive features mediate the relationship between NSSI functions (e.g., ER) and severity. Specifically, individuals with heightened behavioral activation system (BAS) sensitivity (characterized by amplified reward-seeking and approach motivation) may exhibit intensified addictive behaviors. We propose that higher levels of NSSI addiction mediate the pathway from functions to severity by reinforcing behavioral escalation, potentially through amplified reward sensitivity associated with the addictive process (Kautz et al., 2020).
Participants in the current study were adolescent inpatients with mood disorders
admitted to the psychiatric department of a general hospital in Guangzhou, China.
Convenience sampling was conducted from September 2023 to January 2024. In this
study, adolescents were defined as individuals aged 10–24 years, a range that
aligns with the latest expert consensus on adolescent development and the widely
accepted conceptualization of this life phase (Sawyer et al., 2018). Mood
disorders were diagnosed by two qualified psychiatrists in accordance with the
criteria in the International Statistical Classification of Diseases and Related
Health Problems, 10th Edition (ICD-10) by the World Health Organization
(Feinstein, 1993). Other exclusion criteria included: (i) individuals with
organic mental disorders; (ii) individuals with intellectual disability or
moderate-to-severe cognitive impairment (Mini-Mental State Examination score
A total of 268 surveys were distributed, 250 were returned, and 232 were deemed valid, resulting in an effective response rate of 92.8%. As the current study focuses on the characteristics of NSSI, only adolescents who reported engaging in NSSI within the past year preceding theri assessment (conducted between September 2023 and January 2024). This sample comprised 182 adolescents (Mage = 15.75, standard deviation [SD] = 2.82; 78.0% females), yielding a NSSI prevalence rate of 78.4%. All participants and their guardians gave written informed consent prior to their participation in the study. This study obtained approval from the research ethics committee of the Sun Yat-sen University (No. L2023SYSU-HL-061).
2.2.1.1 Sociodemographic and Clinical Variables
A self-administered questionnaire was utilized to collect sociodemographic and clinical characteristics, encompassing age, gender, body mass index (BMI), educational level, religious beliefs, number of siblings, place of residence, diagnosis, previous psychotic symptoms, age at first onset, age at initial treatment, duration of untreated period (DUP), and whether it was first onset or not.
2.2.1.2 Depressive Symptoms
The 17-item Hamilton Depression Rating Scale (HAMD) (Hamilton, 1967) was used to rate depression symptoms over the past week. It rated 17 symptoms related to depression (e.g., depressed mood, guilt, suicide). Each item is scored by uniformly trained researchers from 0 to 2, or 0 to 4, based on on-site assessments and medical records. The total score is the sum of the scores of each item, with higher scores indicating greater severity of depression. Scores of 0–7 indicate no depression, 8–17 mild depression, 18–23 moderate depression, and 24 or above severe depression.
2.2.1.3 Manic Symptoms
The Young Mania Rating Scale (YMRS) (Young et al., 1978) was used to rate mania symptoms over the past week. It rated 17 symptoms related to mania (e.g., elevated mood, increased activity-energy). Each item is scored by uniformly trained researchers from 0 to 4, or 0 to 8, based on on-site assessments and medical records. The total score is the sum of the scores of each item, with higher scores indicating greater severity of mania. Scores of 0–5 indicate no mania, 6–12 mild depression, 13–29 moderate depression, 30–39 severe depression, and 40 or above extremely severe mania.
2.2.2.1 Addictive Features of NSSI
The addictive features subscale of the Ottawa Self-Injury Inventory-Chinese Revised Version (OSI-CRV) was used to assess addictive features of NSSI (Chen et al., 2022). The subscale aligns with the English version, comprising 7 items scored on a scale from 0 to 4. They are Item 1 (The self-injurious behavior occurs more often than intended?), Item 2 (The severity in which the self-injurious behavior occurs has increased [e.g., deeper cuts, more extensive parts of your body]?), Item 3 (If the self-injurious behavior produced an effect when started, you now need to self-injure more frequently or with greater intensity to produce the same effect?), Item 4 (This behavior or thinking about it consumes a significant amount of your time [e.g., planning and thinking about it, collecting and hiding sharp/objects, doing it and recovering from it]?), Item 5 (Despite a desire to cut down or control this behavior, you are unable to do so?), Item 6 (You continue this behavior despite recognizing that it is harmful to you physically and/or emotionally?) and Item 7 (Important social, family, academic or recreational activities are given up or reduced because of this behavior?). A higher raw score reflects a stronger indication of addictive features in an individual’s NSSI. The reliability coefficients for the current study were good, with a Cronbach’s alpha of 0.88 for the addictive features subscale.
2.2.2.2 Functions of NSSI
The functions subscale of the OSI-CRV was used to evaluate the functions of NSSI (Chen et al., 2022). The subscale includes 15 items across three dimensions of NSSI functions: external ER, internal ER, and social influence. Each item is rated from 0 to 4, with higher raw score indicating greater motivation for NSSI. The reliability coefficients for the current study were good, with a Cronbach’s alpha of 0.88 for the function’s subscale, and 0.85, 0.68 and 0.77 for external ER, internal ER and social influence, respectively.
2.2.2.3 Severity of NSSI
The OSI-CRV was utilized to assess the severity of NSSI through a single question, the self-injury section, and the self-injury methods section (Chen et al., 2022). A comprehensive variable combining the episodes, body parts, and methods of NSSI was created to represent the severity of NSSI. A comprehensive variable, combining the frequency of NSSI episodes, the body parts involved, and the methods used were created to represent the severity of NSSI.
Firstly, the single question, “How often in the past year have you hurt yourself without the intention to kill yourself ?” was used to measure the frequency of NSSI episodes. Based on the previous research (Luo et al., 2024), the responses were categorized into 0 times, 1 time, 2 to 4 times, and 5 times or more. Individuals who selected “0 times” were dropped from the current study.
Secondly, the self-injury parts section and the self-injury methods section of OSI-CRV were employed (Chen et al., 2022), instructing individuals to identify the body parts they had previously injured and they injured most frequently, as well as the methods they had used most frequently. Self-injury parts section includes 22 possible body parts: scalp, eyes, ears, face, nose, lips, mouth, neck/throat, chest, breast, back, shoulders, abdomen, buttocks, genitals, rectum/anus, upper arms/elbows, lower arms/wrists, hands/fingers, thighs/knees, calves/ankles, and feet/toes. Self-injury methods section includes 19 possible methods: cutting, scratching/scraping, hindering wound healing, burning and scalding, biting/pinching, hitting, pulling hair, excessive drinking, drug abuse, taking too little medicine, stabbing body parts with sharp objects, choking/strangling/suffocating, hitting head hard, trying to break bones, overdosing on medication, poison, severely biting/injuring nails, eating or drinking non-food substances, and deliberately colliding with motor vehicles/standing in the middle of the road. Additionally, individuals could self-report their self-injurious behaviors in two designated sections. Subsequently, we tallied the number of body parts previously injured and categorized them into three levels: 1 part, 2 to 4 parts, and 5 parts or more. In a similar manner, the number of methods previously used was also divided into three categories: 1 method, 2 to 4 methods, and 5 methods or more.
Thirdly, scores of 1, 2, or 3 points were assigned to the frequency of NSSI
episodes, the number of distinct body parts injured, and the number of distinct
methods used, corresponding to 1 episode/part/method, 2–4
episodes/parts/methods, or
The statistical analyses consisted of three components: LCA, covariate analysis, and mediation analysis. All analyses were performed using Mplus 8.3 (Muthén & Muthén, Los Angeles, CA, USA), except for the descriptive analysis, which was performed with SPSS 25.0 (IBM, Armonk, NY, USA).
Firstly, LCA was conducted on a sample of 182 adolescents with mood disorders.
The latent class indicators encompassed the seven items of addictive features
subscale. To determine the optimal number of latent classes (or class
enumeration), a series of models were estimated and compared. This process began
with a one-class model, and models with incrementally increasing numbers of
classes (up to five classes) were evaluated (He et al., 2023). Model fit was
assessed using several criteria: (i) The Akaike Information Criterion (AIC)
(Akaike, 1987), Bayesian Information Criterion (BIC) (Schwarz, 1978), and
sample-size adjusted BIC (aBIC) (Sclove, 1987), where lower values indicating
better fit. (ii) The bootstrapped likelihood ratio test (BLRT) and the
Lo-Mendell-Rubin Adjusted Likelihood Ratio Test (LMR-LRT) were employed, where a
significant likelihood ratio test for k classes (p
Secondly, to account for the classification error inherent in latent variable modeling, demographic and clinical predictors were incorporated into the LCA using the robust three-step (R3Step) approach sequentially (Wang and BI, 2018). Based on prior literature suggesting that NSSI functions may serve as potential predictors of addictive classes, the R3Step method was also used to examine the associations between NSSI function and the latent classes (Wang and BI, 2018). Meanwhile, considering that NSSI severity could be an outcome variable influenced by latent class membership, the relationship between NSSI severity and the latent classes of NSSI addictive features was analyzed using the Bolck-Croon-Hagenaars (BCH) method (Wang and BI, 2018).
Finally, we conducted a mediation model to examine whether the latent classes of addictive features (categorical variable derived from LCA) mediated the relationship between dimensions of NSSI functions (continuous, standardized scores) and NSSI severity (continuous, standardized score). The model was estimated using the (weighted least squares with mean and variance adjustment) WLSMV estimator appropriate for mixed variable types (continuous outcomes with categorical mediators) (Muthén and Asparouhov, 2015). Because WLSMV estimation is incompatible with bootstrapping procedures, we determined the significance of both direct and indirect effects by examining whether their 95% confidence intervals (CIs), calculated following Shrout and Bolger’s (2002) methodology, excluded zero.
The fit statistics of 1 to 5 classes model are shown in Table 1. Based on a
comprehensive evaluation of model fit indices and clinical interpretability, the
2-class model was ultimately selected as the optimal solution. The decision was
supported by three key observations: first, the 2-class model demonstrated the
lowest BIC value, which is particularly prioritized in small sample analyses
(Nylund et al., 2007; Yang and Yang, 2007), with only marginal improvements
in AIC and aBIC when moving to more complex models; second, the more reliable
LMRT test favored the 2-class solution while the BLRT’s support for additional
classes appeared to detect statistically significant but clinically insignificant
separations (Lubke and Neale, 2006); third, both 2- and 3-class models showed
comparably high classification accuracy (entropy
| Number of classes | k | Loglikehood | AIC | BIC | aBIC | Entropy | VLMR (p) | LMRT (p) | BLRT (p) |
| 1 | 28 | –1972.125 | 4000.250 | 4089.962 | 4001.282 | - | - | - | - |
| 2 | 57 | –1761.559 | 3637.118 | 3819.747 | 3639.221 | 0.907 | |||
| 3 | 86 | –1688.584 | 3549.169 | 3824.714 | 3552.341 | 0.920 | 0.835 | 0.835 | |
| 4 | 115 | –1647.097 | 3524.195 | 3892.655 | 3528.436 | 0.917 | 0.799 | 0.799 | |
| 5 | 144 | –1614.507 | 3517.014 | 3978.391 | 3522.325 | 0.928 | 0.818 | 0.818 | 0.063 |
Note: k, number of free parameters; NSSI, non-suicidal self-injury; LL, log likelihood; AIC, Akaike information criteria; BIC, Bayesian information criteria; aBIC, sample-size adjusted BIC; VLMR, Vuong-Lo-Mendell-Rubin Likelihood Ratio Test; LMRT, Lo-Mendell-Rubin adjusted LRT test; BLRT, bootstrapped likelihood ratio test.
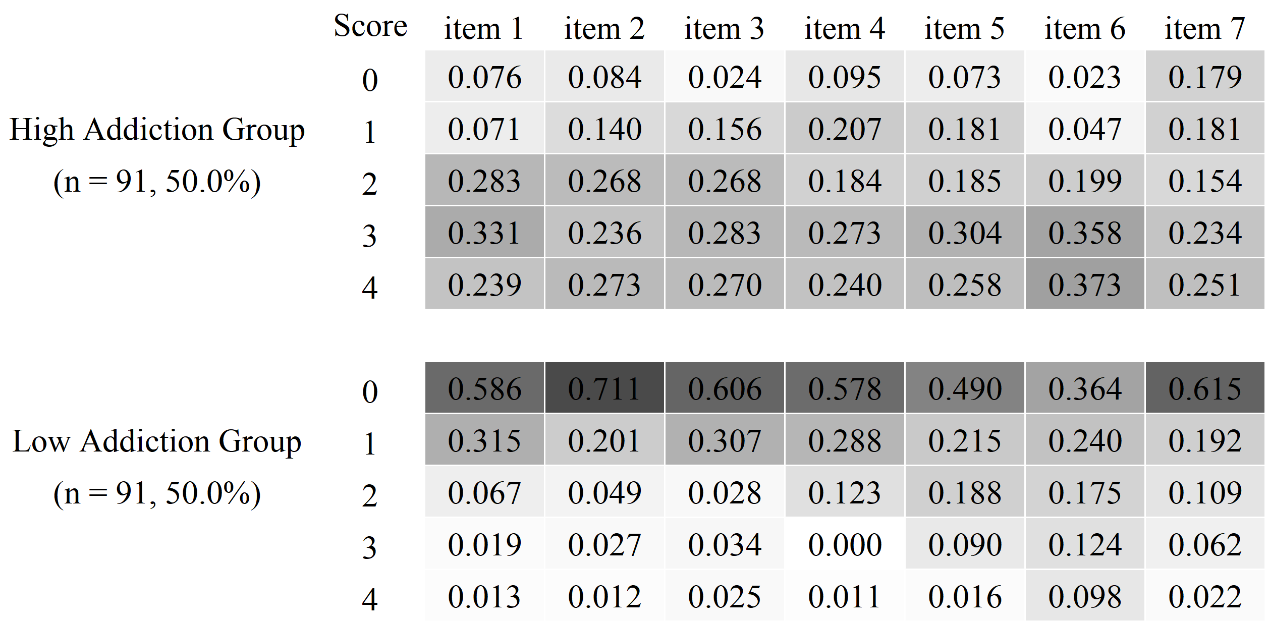 Fig. 1.
Fig. 1.
Item-probability heatmap of addictive features of NSSI across the two classes.
Table 2 presents the associations between sociodemographic and clinical
characteristics with two latent classes of addictive features in NSSI. Compared
to adolescents aged 10–14 years, those aged 15–19 years had lower odds of being
in the High Addiction Class (
| High addiction class | Low addiction class | p | OR | 95% CI | |||
| (n = 91, 50.0%) | (n = 91, 50.0%) | ||||||
| Age (years) | |||||||
| 10–14 | 46 (50.5) | 29 (31.9) | Reference | ||||
| 15–19 | 35 (38.5) | 48 (52.7) | –0.818 | 0.017 | 0.441 | (0.225, 0.864) | |
| 20–24 | 10 (11.0) | 14 (15.4) | –0.840 | 0.095 | 0.432 | (0.161, 1.157) | |
| Gender | |||||||
| Male | 15 (16.5) | 25 (27.5) | Reference | ||||
| Female | 76 (83.5) | 66 (72.5) | 0.686 | 0.077 | 1.985 | (0.929, 4.242) | |
| BMI classification (kg/m2) | |||||||
| Low ( |
30 (33.0) | 29 (31.9) | 0.244 | 0.488 | 1.277 | (0.640, 2.545) | |
| Normal (18.50–24.00) | 41 (45.0) | 50 (54.9) | Reference | ||||
| Overweight or Obesity ( |
20 (22.0) | 12 (13.2) | 0.747 | 0.094 | 0.474 | (0.880, 5.066) | |
| Educational levels | |||||||
| Middle school and below | 55 (60.4) | 40 (43.9) | Reference | ||||
| Senior or vocational high school | 26 (28.6) | 33 (36.3) | –0.586 | 0.096 | 0.557 | (0.279, 1.110) | |
| College and above | 10 (11.0) | 18 (19.8) | –0.954 | 0.043 | 0.385 | (0.153, 0.970) | |
| Religious beliefs | |||||||
| Without | 87 (95.6) | 84 (92.3) | Reference | ||||
| With b | 4 (4.4) | 7 (7.7) | –0.626 | 0.358 | 0.535 | (0.141, 2.033) | |
| Siblings | |||||||
| Having siblings | 74 (81.3) | 70 (76.9) | Reference | ||||
| The only child | 17 (18.7) | 21 (23.1) | –0.280 | 0.466 | 0.755 | (0.355, 1.607) | |
| Place of residence | |||||||
| City | 56 (61.5) | 53 (58.2) | Reference | ||||
| Town | 21 (23.1) | 22 (24.2) | –0.107 | 0.778 | 0.899 | (0.428, 1.888) | |
| Countryside | 14 (15.4) | 16 (17.6) | –0.198 | 0.648 | 0.820 | (0.350, 1.921) | |
| Diagnosis | |||||||
| Mood disorder (not specified) | 38 (41.8) | 46 (50.5) | Reference | ||||
| BD | 28 (30.7) | 26 (28.6) | 0.279 | 0.448 | 1.321 | (0.643, 2.716) | |
| Depressive disorder | 25 (27.5) | 19 (20.9) | 0.490 | 0.215 | 1.632 | (0.752, 3.540) | |
| Previous psychotic symptoms | |||||||
| Without | 49 (53.8) | 58 (63.7) | Reference | ||||
| With | 42 (46.2) | 33 (36.3) | 0.431 | 0.177 | 1.539 | (0.824, 2.875) | |
| DUP (years) | |||||||
| 46 (50.5) | 56 (61.5) | Reference | |||||
| 1–2 | 32 (35.2) | 20 (22.0) | 0.702 | 0.056 | 2.018 | (0.982, 4.148) | |
| 13 (14.3) | 15 (16.5) | 0.056 | 0.900 | 1.058 | (0.438, 2.554) | ||
| Depressive symptoms | |||||||
| No depression | 4 (4.4) | 13 (14.3) | Reference | ||||
| Mild depression | 24 (26.4) | 31 (34.1) | 0.981 | 0.151 | 2.668 | (0.699, 10.187) | |
| Moderate depression | 14 (15.4) | 11 (12.1) | 1.504 | 0.046 | 4.500 | (1.030, 19.660) | |
| Severe depression | 49 (53.8) | 36 (39.5) | 1.575 | 0.017 | 4.830 | (1.318, 17.706) | |
| Manic symptoms | |||||||
| No mania | 80 (87.9) | 75 (82.4) | Reference | ||||
| Mild mania | 11 (12.1) | 16 (17.6) | –0.462 | 0.446 | 1.036 | (0.263, 1.509) | |
| Moderate mania | 0 (0.0) | 0 (0.0) | - | - | - | - | |
| Severe mania | 0 (0.0) | 0 (0.0) | - | - | - | - | |
Note: a means using the low addiction class as the reference class. b includes Buddhism, Taoism and Christianity.
OR, odds ratio; CI, confidence interval; BMI, body mass index; BD, bipolar disorder; DUP, duration of untreated period.
Table 3 presents the total and subscale scores for NSSI functions in the two
latent classes. Base on R3step analysis, higher score on the external ER
(
| High addiction class | Low addiction class | p | OR | 95% CI | Cohen’s d | |||
| (n = 91, 50.0%) | (n = 91, 50.0%) | |||||||
| Functions of NSSI | 32.44 |
21.18 |
0.095 | 1.100 | (1.049, 1.153) | 0.960 | ||
| External ER | 13.53 |
9.13 |
0.177 | 1.194 | (1.106, 1.289) | 0.868 | ||
| Internal ER | 10.81 |
6.69 |
0.243 | 1.276 | (1.158, 1.405) | 0.966 | ||
| Social influence | 8.10 |
5.35 |
0.127 | 0.002 | 1.135 | (1.048, 1.229) | 0.567 | |
Note: a means using the low addiction class as the reference class.
ER, emotion regulation.
BCH analysis revealed a significant difference in NSSI severity between the High
Addiction Class and the Low Addiction Class (7.49
As shown in Fig. 2A, among the body parts injured, the top four were the “lower arms/wrist” (n = 126, 69.23%), “hands/fingers” (n = 89, 48.90%), “upper arms/elbows” (n = 50, 27.47%), and “thighs/knees” (n = 50, 27.47%). No individuals reported injuring the “breast”, “buttocks”, or “rectum/anus”. Regarding the most frequently injured parts, the top four were the “lower arms/wrists” (n = 112, 61.54%), “hands/fingers” (n = 42, 23.08%), “upper arms/elbows” (n = 22, 12.09%), and “thighs/knees” (n = 15, 8.24%). No participants reported the “rectum/anus”, “buttocks”, “back”, “breast”, “chest”, “nose”, or “eyes” as their most frequent parts of injury.
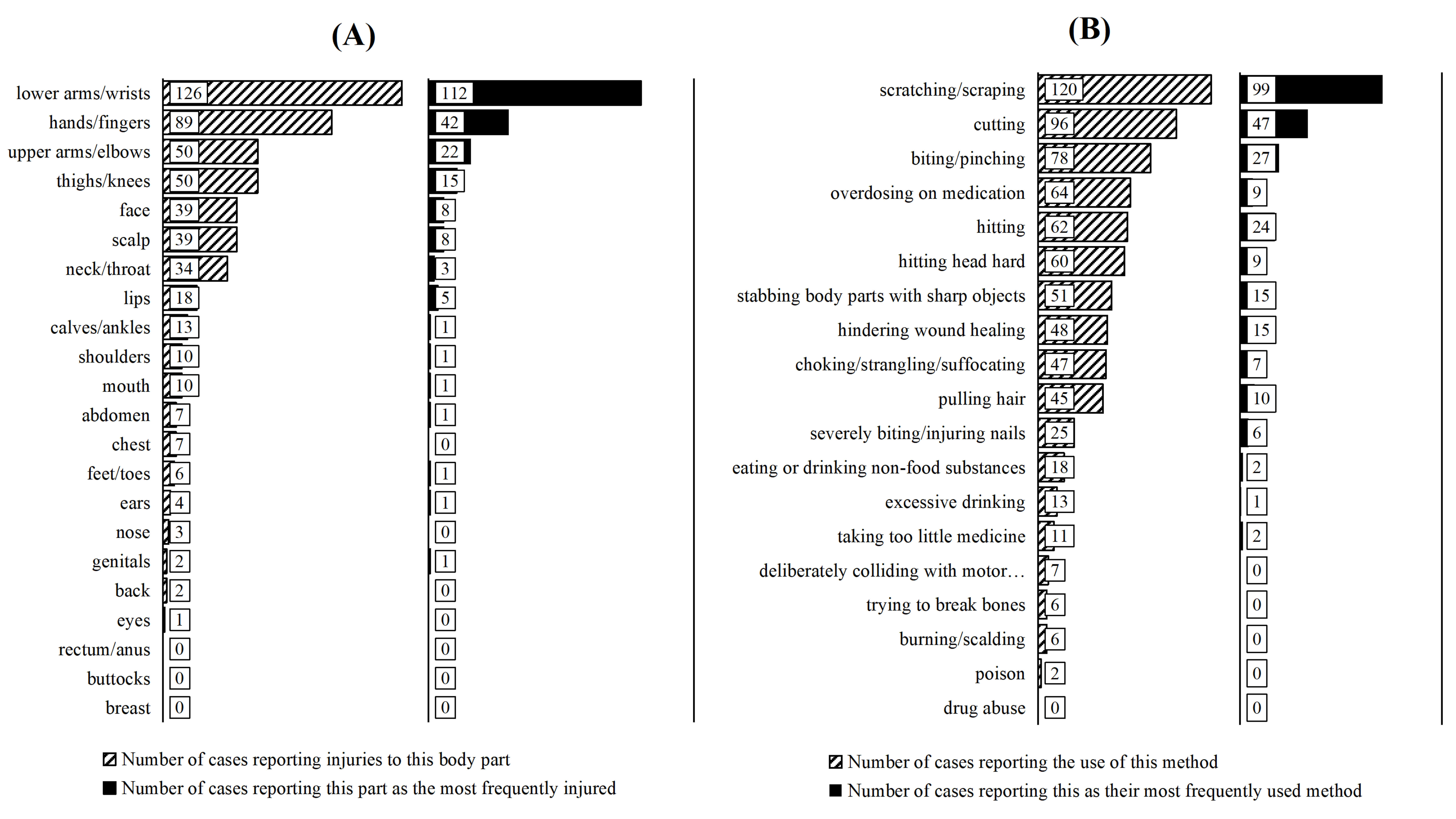 Fig. 2.
Fig. 2.
The body parts (A) and methods (B) of NSSI in all adolescents with mood disorders (n = 182).
As shown in Fig. 2B, among the self-injury methods ever used, the top four were “scratching/scraping” (n = 120, 65.93%), “cutting” (n = 96, 52.75%), “biting/pinching” (n = 78, 42.86%), and “overdosing of medication” (n = 64, 35.16%). No individuals reported using the method of “drug abuse”. Among the most frequently used self-injury methods, the top four were “scratching/scraping” (n = 99, 54.40%), “cutting” (n = 47, 25.82%), “biting/pinching” (n = 27, 14.84%), and “hitting” (n = 24, 13.19%). No participants reported “burning/scalding”, “trying to break bones”, “overdosing of medication”, “intentionally colliding with motor vehicles/standing in the middle of the road”, or “drug abuse” as their most frequently used method.
As shown in Table 4 and Fig. 3, the mediation analysis revealed distinct
pathways through which the two latent classes of addictive features (with the Low
Addiction Class as reference) mediate the relationship between three functional
dimensions and the severity of NSSI. For external ER, although the total effect
on NSSI severity was non-significant (
| Model path | p | 95% CI | Ratio of effect values | ||
| Total effect | External ER – severity | 0.084 | 0.326 | (–0.084, 0.226) | — |
| Internal ER – severity | 0.461 | (0.277, 0.644) | 100.0% | ||
| Social influence – severity | 0.031 | 0.705 | (–0.128, 0.189) | — | |
| Direct effect | External ER – severity | –0.031 | 0.723 | (–0.202, 0.140) | — |
| Internal ER – severity | 0.272 | 0.007 | (0.074, 0.470) | 59.1% | |
| Social influence – severity | 0.036 | 0.626 | (–0.109, 0.181) | — | |
| Indirect effect | External ER – high addiction class a – severity | 0.115 | 0.044 | (0.003, 0.227) | 136.9% |
| Internal ER – high addiction class a – severity | 0.188 | 0.006 | (0.053, 0.324) | 40.9% | |
| Social influence – high addiction class a – severity | –0.006 | 0.908 | (–0.100, 0.089) | — |
Note: a means using low addiction class as the reference class; — non significant effect.
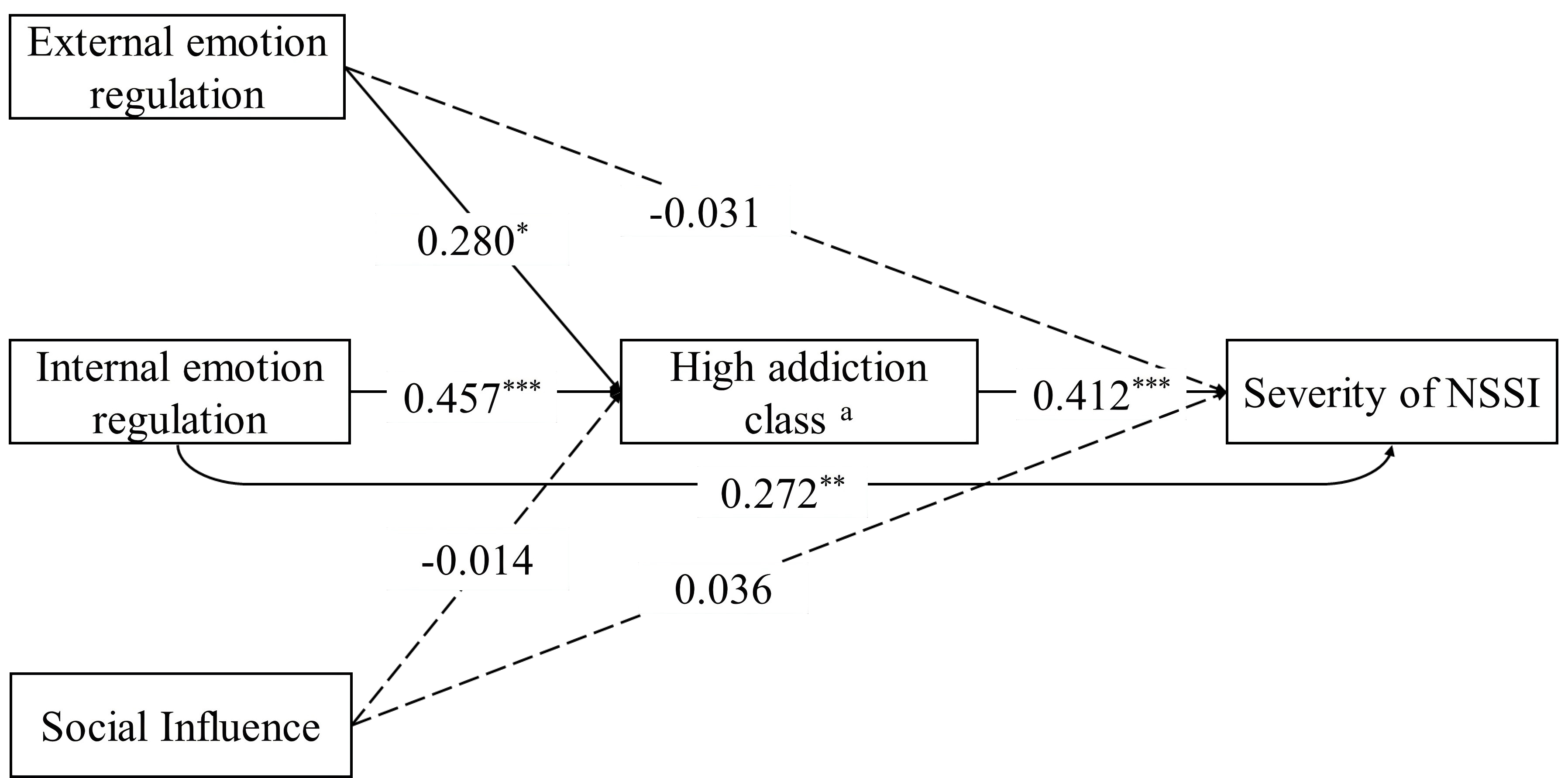 Fig. 3.
Fig. 3.
Mediating effect of addictive features in the relationship
between functions and severity of NSSI. Note: a means using the
Low Addiction Class as the reference class. *p
To the best of our knowledge, this is the first study to identify latent subgroups based on the addictive features of NSSI. Our findings revealed two distinct latent classes of NSSI addictive features among adolescents with mood disorders, which exhibited differences in sociodemographic and clinical characteristics, as well as NSSI functions and severity of NSSI. Furthermore, these latent classes of addictive features mediated the relationship between NSSI functions and the severity of NSSI.
Consistent with our H1 and previous studies on addictive behaviors (Colder Carras et al., 2017; Hong et al., 2009), this study identified two latent classes of NSSI addictive features. This finding extends prior evidence that addictive behaviors frequently co-occur and exhibit stability (Sussman et al., 2015), suggesting shared psychological and neurobiological mechanisms across distinct manifestations. Critically, our results align with a core diagnostic feature of addiction: individuals recognize that their behavior is harmful yet struggle to control it. This manifests as both psychological and physiological dependence on certain substances or behaviors, along with developing tolerance over time (American Psychiatric Association, 2013). Low NSSI addiction may involve weaker dependency and tolerance, while high NSSI addiction requires escalating severity and/or frequency to achieve the same alleviating effects. In addition, treatments proven effective for other forms of addiction may also benefit NSSI behaviors. For example, low dose naltrexone (an opioid antagonist) can reduce or eliminate self-injurious behaviors in NSSI patients (Karakuła-Juchnowicz et al., 2024).
Current findings align with previous NSSI heterogeneity research. Indeed, He et al. (2023) reported two subgroups among depressed adolescents engaging in NSSI: Low Suicidal Ideation (60.4%) and High Suicidal Ideation (39.6%). Similarly, Sack et al. (2024) identified functional classes in psychiatric inpatients youth: Single/Avoidant Function (58.8%) and Multiple Functions (41.2%). Yu (2013) theorized that NSSI can be categorized as either pathological or developmental. Pathological NSSI constitutes maladaptive behavior rooted in biological and/or psychological foundations, developmental history, and individual-environment interactions, reflecting heightened sensitivity to social stimuli. Developmental NSSI represents situational behavior specific to adolescence, primarily driven by external environmental pressures (Yu, 2013). Given established correlations between addictive features, NSSI functions and severity of NSSI (Martin et al., 2013; Nixon et al., 2015; Yan et al., 2024), we support two clinically distinct NSSI subgroups in adolescents with mood disorders. These subtypes can be further refined and offer practical utility in guiding clinical interventions (Nock and Favazza, 2009b; Yue et al., 2021).
Research consistently indicates that adolescents with higher levels of
depression are more likely to exhibit significant addictive behaviors, aligning
with findings on NSSI, smartphone, and internet addiction (He et al., 2023; Yue et al., 2021). Coping with depressive feelings is a primary motivation for
adolescent to engage in NSSI behaviors (Nixon et al., 2002), highlighting its
role as a maladaptive ER strategy (Nock and Prinstein, 2004). While
ecological momentary assessments show short-term mood alleviation after NSSI,
this behavior ultimately impairs long-term emotional regulation (Koenig et al., 2021), potentially contributing to NSSI recurrence and addictive features.
Thus, NSSI functions as a counterproductive coping mechanism. Lower educational
levels in adolescents are also associated with higher NSSI addiction (Ying et al., 2024). Additionally, experiencing mood disorder onset and initiating
treatment at a younger age correlates with higher addiction. Given the
interrelationship nature between educational level, age, and age at onset, these
factors should be considered in conjunction. Younger age and earlier onset imply
greater susceptibility to negative emotions and a higher likelihood of addictive
features. Notably, patients with mood disorders exhibit reduced
This study revealed that the High Addiction Class exhibited more severe NSSI behaviors and higher NSSI functions than the Low Addiction Class, characterized by higher frequency, greater method diversity, broader bodily locations, and more self-injury motivations, reflecting a high demand for ER (both external and internal), as well as social influence. Results further demonstrated significant positive correlations between addictive features and both NSSI functions and severity in adolescents with mood disorders, which was consistent with findings from clinical (Martin et al., 2013; Nixon et al., 2015; Yan et al., 2024) and non-clinical samples (Luo et al., 2024). Notably, our findings confirm our H2, which posits that NSSI addictive features mediate the relationship between NSSI functions and severity, consistent with previous findings (Luo et al., 2024). According to the functional theory of NSSI, individuals eliminate negative emotions, arouse positive emotions, or influence interpersonal relationships through NSSI behaviors (Nock and Prinstein, 2004). This process of positive or negative reinforcement can enhance addictive patterns and the severity of NSSI (Chapman et al., 2006).
Notably, the non-significant direct association between external ER and NSSI severity, contrasted with its substantial indirect effect through addictive features, points to a suppression dynamic. External ER, primarily driven by interpersonal goals such as seeking social connection or eliciting care, appears to lack intrinsic neurobiological mechanisms that independently escalate NSSI severity (Blasco-Fontecilla et al., 2020; Martin et al., 2013). However, when external ER operates through addictive pathways, its dormant potential to worsen NSSI becomes evident. Specifically, the interplay between social reinforcement needs (e.g., maintaining attention through self-injury) and tolerance-driven escalation (e.g., progressively deeper cuts) creates a feedback loop. This aligns with RST, where the BAS amplifies reward-seeking tendencies, thereby fueling addictive processes. Consequently, socially motivated NSSI may transition into more severe, dysregulated behavior patterns (Gray, 1982; Kautz et al., 2020).
Furthermore, research indicates that individuals with NSSI have lower resting
levels of
These findings complement and enhance the understanding of NSSI through the addiction perspective. Future therapeutic interventions for NSSI may benefit from integrating evidence-based approaches used in addiction treatment, including pharmacotherapies targeting opioid and dopamine neurotransmitter systems (Koob and Volkow, 2016), repetitive transcranial magnetic stimulation (rTMS) for prefrontal modulation (Zhao et al., 2023), and dialectical behavior therapy (DBT) for behavioral regulation (McCauley et al., 2018).
This study examined latent classes of NSSI addictive features in a clinical
adolescent sample, providing empirical insights into NSSI heterogeneity from an
addiction perspective. It further confirmed the mediating role of these addictive
features in the relationship between NSSI functions and severity. However,
several limitations warrant acknowledgment. First, the cross-sectional design
limits our ability to explore the developmental trajectories of addictive
features in adolescents with mood disorders or to establish causal relationships
with other variables. Second, this study exclusively recruited inpatients from a
single center. The exclusion of outpatient or community-based samples may lead to
an overestimation of the severity of addictive features. Accordingly, caution
should be exercised when generalizing these findings. Third, the small sample
size with overrepresentation of females necessitates cautious interpretation of
the results. Consequently, given the sample size constraint (n = 182), the latent
class structure and mediation effects reported here should be considered
exploratory. These findings require replication in larger samples (target n
In conclusion, this was the first study to delineate the latent classes of NSSI addictive features among adolescents with mood disorders, reinforcing prior insights into the relationship between addictive features, NSSI functions, and the severity of NSSI. Our findings reveal two distinct addiction-based classes with significant differences in self-injury motivations and clinical outcomes. Notably, we demonstrate that addictive features mediate the relationship between NSSI functions and severity in this population. These results advance the understanding of NSSI progression in clinical contexts and underscore the pivotal role of addictive mechanisms in developing effective treatments for adolescents with mood disorders.
The data from this study are available from the corresponding author upon reasonable request.
XL and JZ designed the research study. LZ, RM and ZL performed the research. LZ analyzed the data. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
This study obtained approval from the research ethics committee of the Sun Yat-sen University (protocol number: L2023SYSU-HL-061). All participants and their guardians gave written informed consent prior to their participation in the study. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
The author expresses gratitude to the clinical nurses who assisted in the data collection process.
The study was supported by the Fujian Province Science and Technology Project (Grant Number 2025Y01020040).
The authors declare no conflict of interest.
During the preparation of this work the authors used ChatGpt-3.5 in order to check spell and grammar. After using this tool, the authors reviewed and edited the content as needed and takes full responsibility for the content of the publication.
Supplementary material associated with this article can be found, in the online version, at https://doi.org/10.31083/BP44481.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.