



 , Gema Aonso-Diego 1, Laura Macía 1, Carlos Llanes-Álvarez 2, Ana Isabel Álvarez-Navares 3
, Gema Aonso-Diego 1, Laura Macía 1, Carlos Llanes-Álvarez 2, Ana Isabel Álvarez-Navares 31 Department of Psychology, Faculty of Health Sciences, University of Deusto, 48007 Bilbao, Spain
2 Department of Psychiatry, Complejo Asistencial de Zamora, 49022 Zamora, Spain
3 Department of Psychiatry, Complejo Asistencial Universitario de Salamanca, 37007 Salamanca, Spain
Abstract
Suicide is a significant public health concern, and several psychological variables, such as childhood trauma, have been studied as risk factors, but this link remains unclear. The study aims to examine the association between childhood trauma (i.e., physical and emotional abuse/neglect and sexual abuse) and suicide, as well as to analyze the mediating role of alexithymia and mental health (i.e., depression and anxiety) in this relationship.
A total of 75 individuals with dual diagnosis (on average, 44.15 years old, SD = 12.15; 82.7% males) completed four questionnaires: Childhood Trauma Questionnaire, Toronto Alexithymia Scale, Symptoms Assessment-45, and Paykel Suicide Scale. Structural equation modeling was performed to examine the mediating role of alexithymia and mental health in the relationship between childhood trauma and suicidal behavior.
Both alexithymia and mental health problems mediate the relationship between childhood trauma and suicidal behavior.
This finding underscores the importance of screening for and addressing alexithymia and mental health in clinical practice, especially in suicide-prevention interventions.
Keywords
- dual diagnosis
- childhood trauma
- suicidal behavior
- alexithymia
- mental health
Suicidal ideation and attempts constitute a significant public health concern, given that they represent the foremost non-natural cause of mortality, contributing to an annual figure of over 700,000 deaths on a global scale (World Health Organization, 2019). Furthermore, suicide stands out as a main cause of disability, as the human cost stemming from suicidal behaviors is substantial, impacting individuals, families, communities, healthcare systems, and society at large.
Research has consistently shown that suicide is a complex and multifactorial phenomenon resulting from the interplay of genetic, neurobiological, psychological, and social factors (Franklin et al., 2017; Guzmán et al., 2019; Turecki et al., 2019). To understand this complexity, several theoretical models have been proposed. Among them, the integrated motivational-volitional (IMV) model of suicidal behavior (O’Connor, 2011; O’Connor and Kirtley, 2018) provides a comprehensive framework that distinguishes between predisposing factors, motivational moderators, and volitional facilitators, offering an integrated understanding of how suicidal ideation emerges and progresses to suicidal acts. This model supports a multifactorial approach and highlights potential mechanisms that may explain individual vulnerability and resilience.
It is noteworthy that individuals with substance use disorders constitute a particularly vulnerable population, displaying an elevated susceptibility to engage in suicidal behaviors (i.e., suicidal ideation and suicide attempts) (Arribas-Ibar et al., 2017; Darvishi et al., 2015; Youssef et al., 2016). Specifically, a notable prevalence of individuals with substance use disorders, ranging between 40% and 60%, have reported a history of suicide attempts (Yuodelis-Flores and Ries, 2015). Compared to the general population, those with alcohol use disorder have an almost 10-fold increase in the risk of suicide-related mortality, whereas polydrug users reach a nearly 17-fold increase in suicide rates (Wilcox et al., 2004). This risk is increased when substance use disorder co-occurs with concurrent psychological disorders, widely known as dual diagnosis (Szerman et al., 2012; Youssef et al., 2016), including major depression, and bipolar, schizophrenia, posttraumatic stress, and personality disorders (Kolla et al., 2008; Melle et al., 2010; Oquendo et al., 2010; Rojas et al., 2014; Yuodelis-Flores and Ries, 2015). Due to all the above, it is important to increase attention, both in terms of treatment strategies and research, to comprehending suicidal behavior in individuals with substance use disorders and dual diagnosis.
Prior studies have yielded insights highlighting childhood trauma as a pivotal risk factor linked with suicide-related behaviors (Angelakis et al., 2020; Rogerson et al., 2023). Physical and emotional abuse and neglect during childhood, and especially sexual abuse, have emerged as key contributors to the manifestation of suicidal ideation and subsequent suicide attempts (Zatti et al., 2017). Notably, 80% who had attempted suicide in adulthood and 40% who had suicidal ideation reported a history of childhood trauma (O’Connor et al., 2018). Childhood trauma also represents a key predictor among individuals with substance use disorders (Lotzin et al., 2019; Roy, 2009; Roy, 2010; Roy and Janal, 2007; Vaszari et al., 2011). Studies have shown that a history of childhood trauma can have a significant impact on the development, severity, and progression of substance use disorders. This means that people with dual diagnosis often start using substances at a younger age, escalate their use earlier, and experience more severe psychological symptoms overall (Farrugia et al., 2011; Lotzin et al., 2019).
Despite the growing evidence of the relationship between childhood trauma and suicidal behaviors, the mechanism linking these variables remains unclear. Aligned with the IMV model, certain psychological constructs may act as mediators between distal risk factors and suicidal outcomes. Alexithymia is a personality construct representing a disturbance in the affective and cognitive function of emotion processing, characterized by difficulty identifying and describing one’s emotions. Individuals with alexithymia may struggle to recognize emotional cues in themselves and others, leading to a diminished capacity for emotional expression and introspection (Hogeveen and Grafman, 2021). This construct has been studied as a risk factor for suicide (Davey et al., 2018; Greene et al., 2020; Khan and Jaffee, 2022; Norman et al., 2020), both in general population and psychiatric and clinical population (De Berardis et al., 2017; Hemming et al., 2019; Iskric et al., 2020; Norman et al., 2020). Additionally, alexithymia has been studied as a strong risk factor for psychiatric conditions (e.g., depression) (McGillivray et al., 2017) as well as substance use disorders (Evren and Evren, 2006; Ghorbani et al., 2017; Sakuraba et al., 2009). Prior research has found an association between childhood trauma and the presence of alexithymia in the population of individuals with substance use disorders (Evren et al., 2009; Kopera et al., 2020; Zdankiewicz-Ścigała and Ścigała, 2018; Zdankiewicz-Ścigała and Ścigała, 2020). People who cannot differentiate emotional states may experience distress because they cannot employ effective strategies to regulate their emotions, and this could ultimately lead them to engage in suicidal behavior as a way of coping with stressors.
On the other hand, children who experience some kind of abuse or neglect show high rates of physical and mental health issues in adulthood, especially depressive and anxious symptomatology (Lu et al., 2008; McKay et al., 2021; McKay et al., 2022). This could impact suicide behavior both in general population (Orsolini et al., 2020) and dual-diagnosis individuals (Devin et al., 2023). Depression and anxiety are among the most consistently identified proximal risk factors for suicide and are also frequently comorbid with substance use disorders, particularly in the context of dual diagnosis (Franklin et al., 2017).
Based on this background, guided by the IMV model and supported by existing empirical evidence, the current study focused on the potential mediating role of alexithymia, depression, and anxiety in the association between childhood trauma and suicidal behavior among individuals with dual diagnosis. To our knowledge, no research has investigated whether alexithymia and mental health (i.e., depression and anxiety) serve as mechanisms linking childhood trauma and suicidal behavior among dual-diagnosed individuals. In this context, the current study aimed to examine the relationship between childhood trauma and suicidal behavior, as well as the mediating role of alexithymia, depression, and anxiety in a sample of participants in treatment for dual diagnosis (i.e., mental disorders and substance use).
A total of 75 participants undergoing treatment for substance use with a concurrent dual diagnosis were recruited for the current study. All participants were receiving care at the Dual Diagnosis Unit of the Salamanca Health Complex (Unidad de Patología Dual del Complejo Asistencial de Salamanca), a specialized public service for individuals with co-occurring substance use and mental health disorders. The participants were, on average, 44.15 years old (SD = 12.15) and were predominantly male (82.7%). Their primary substance was alcohol (33.3%), followed by cocaine (28.0%) and cannabis (13.3%). Regarding concurrent psychological disorders, the most frequent were depressive disorders (35.6%), followed by personality disorders (32.9%) and anxiety disorders (16.4%). All psychological disorders were assessed by psychiatrists or a psychologist specialized in dual diagnosis through a clinical interview at baseline, following the diagnostic criteria (American Psychiatric Association, 2023). As shown in Table 1, most of the sample reported primary and secondary education. The participants were mostly unemployed, with early medical retirement being the second most frequent occupational status. Regarding their marital status, 60% of the sample reported being single.
| N = 75 | ||
| Sex (male) | 62 (82.7%) | |
| Agea | 44.15 (12.15) | |
| Primary substance | ||
| Alcohol | 25 (33.3%) | |
| Cocaine | 21 (28.0%) | |
| Cannabis | 10 (13.3%) | |
| Heroin | 8 (10.7%) | |
| Otherb | 11 (14.6%) | |
| Primary psychological disorder | ||
| Depressive disorders | 26 (35.6%) | |
| Personality disorders | 24 (32.9%) | |
| Anxiety disorders | 12 (16.4%) | |
| Psychotic disorders | 5 (6.8%) | |
| ADHD | 4 (5.5%) | |
| Bipolar disorders | 2 (2.7%) | |
| Educational level | ||
| No studies | 3 (4.0%) | |
| Primary studies | 29 (38.7%) | |
| Secondary studies | 20 (26.7%) | |
| High school | 7 (9.3%) | |
| Vocational training | 13 (17.3%) | |
| University studies | 3 (4.0%) | |
| Occupational status | ||
| Working | 4 (5.3%) | |
| Unemployed | 46 (61.3%) | |
| Student | 1 (1.3%) | |
| Retired | 12 (16.0%) | |
| Sick leave | 12 (16.0%) | |
| Marital status | ||
| Single | 45 (60.0%) | |
| Married | 10 (13.3%) | |
| Legal partner | 10 (13.3%) | |
| Divorced | 10 (13.3%) | |
Note. amean(standard deviation). bIncluding benzodiazepines (n = 2), fentanyl (n = 2), amphetamines (n = 1), methadone (n = 3), buprenorphine (n = 1), caffeine (n = 1) and opioid analgesics (n = 1). Data were missing for the variable primary psychological disorder (N = 73). ADHD, attention deficit hyperactivity disorder; N, number of participants.
This study was conducted following the principles of the Declaration of Helsinki. This study was conducted as an anonymous questionnaire survey; therefore, ethics approval was waived. All participants provided written informed consent.
Participants completed an ad-hoc questionnaire, which collected sociodemographic data (i.e., sex, age, monthly income, educational level, and marital status), as well as psychological disorders and substance use disorders. Additionally, the participants completed a set of validated questionnaires, which are outlined below.
The Childhood Trauma Questionnaire-Short Form (CTQ-SF; Bernstein et al., 2003, adapted to Spanish by Hernandez et al., 2013) was used for assessing childhood maltreatment. This questionnaire assesses five types of maltreatment: emotional abuse, physical abuse, sexual abuse, emotional neglect, and physical neglect. It comprises 28 items rated on a 5-point Likert-type scale (1 = never true; 5 = very often true). The questionnaire has excellent psychometric properties. Internal consistency ranges from 0.66 for emotional neglect to 0.94 for sexual abuse in the Spanish validation, whereas in the present study, Cronbach’s alpha coefficients ranged from 0.60 for physical neglect to 0.92 for the sexual abuse dimension.
The Toronto Alexithymia Scale-20 (TAS-20; Bagby et al., 1994, adapted to Spanish by Martínez Sánchez, 1996) measures alexithymia through 20 items. Items are rated on a 6-point Likert-type scale ranging from 0 (strongly disagree) to 5 (strongly agree) and are grouped into three dimensions: (1) difficulty identifying feelings; (2) difficulty describing feelings; and (3) externally-oriented thinking. The scale shows robust internal consistency and is highly reliable in the overall assessment (reliability was 0.77 in the original version and 0.72 for the Spanish adaptation). The current study only considers two dimensions, namely, difficulty Identifying feelings and difficulty describing feelings, whose reliability was 0.79 and 0.74, respectively.
The Symptoms Assessment-45 Questionnaire (SA-45; Davison et al., 1997; adapted to Spanish by Sandín et al., 2008) is the short version of the SCL-90, maintaining the same dimensions and psychometric properties as the extended version. It comprises a total of 45 items rated on a 5-point Likert scale ranging from 0 (no symptom-related distress) to 4 (maximum distress). The questionnaire assesses 45 symptoms grouped into a total of nine dimensions: somatization, obsession-compulsion, interpersonal sensitivity, depression, anxiety, hostility, phobic anxiety, paranoid ideation, and psychoticism. In this study, only the Depression and Anxiety scales were used, composed of five items each. In the current sample, Cronbach’s alpha was 0.87 for depression and 0.86 for anxiety.
The Paykel Suicide Scale (PSS; Paykel et al., 1974, adapted to Spanish by
Fonseca-Pedrero et al., 2018) is a self-report instrument designed for
assessing suicidal ideation and behaviors within the past year. It comprises five
items with a dichotomous response format (Yes/No). Hence, the total score ranges
from 0 to 5. Higher scores indicate a higher frequency and severity of suicidal
ideation. Further, the PSS shows adequate psychometric properties, as seen by its
robust internal consistency (
Descriptive analyses and frequencies were conducted to examine the sociodemographic characteristics of participants and the main variables of the study. Additionally, bivariate Pearson correlations were calculated to test the relationships between the variables of interest (i.e., childhood trauma, alexithymia, depression, anxiety, and suicidal behavior).
Structural equation modeling was performed to examine the mediating effect of
alexithymia and mental health (i.e., depression and anxiety) on the relationship
between childhood trauma and suicidal behavior. The model fit parameters were
estimated using the maximum likelihood estimation method with a multipronged
approach. A chi-square test compared the model-implied covariance matrix to the
sample matrix. Thus, a non-significant p-value indicates no differences
between variances and, therefore, a good fit to the data. However, given the
sensitivity of the chi-square test to sample sizes (Meade et al., 2008; Mooijaart and Satorra, 2009), we relied on several valid alternative fit
indices to evaluate the model fit (Byrne, 2009; Schermelleh-Engel et al., 2003): (1) The Tucker-Lewis index (TLI), where values higher than 0.90 indicate
adequate model fit; (2) the comparative fit index (CFI), where values over 0.90
suggest good model fit; and (3) the root mean square error of approximation
(RMSEA), which evaluates the overall power and robustness of the model. RMSEA
values
Regarding the descriptive statistics and correlations for the observed
variables, Table 2 presents the means, standard deviations, and bivariate
correlations. Generally, childhood trauma variables (i.e., emotional, physical,
and sexual abuse, and emotional and physical neglect) exhibited significant
positive correlations with each other (r
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | |
| 1. Emotional abuse | - | |||||||||
| 2. Physical abuse | 0.742*** | - | ||||||||
| 3. Sexual abuse | 0.498*** | 0.407*** | - | |||||||
| 4. Emotional neglect | 0.694*** | 0.608*** | 0.205 | - | ||||||
| 5. Physical neglect | 0.612*** | 0.626*** | 0.318** | 0.627*** | - | |||||
| 6. Difficulty identifying feelings | 0.220* | 0.150 | 0.153 | 0.240* | 0.163 | - | ||||
| 7. Difficulty describing feelings | 0.185 | 0.224 | 0.106 | 0.275* | 0.111 | 0.507*** | - | |||
| 8. Depression | 0.090 | –0.042 | 0.136 | 0.107 | 0.012 | 0.548*** | 0.281* | - | ||
| 9. Anxiety | 0.162 | 0.051 | 0.258* | 0.029 | 0.062 | 0.412*** | 0.192 | 0.629*** | - | |
| 10. Suicidal behavior | 0.197 | 0.178 | 0.319** | 0.081 | 0.141 | 0.268* | 0.389** | 0.430*** | 0.492*** | - |
| Mean | 3.310 | 2.050 | 1.080 | 3.360 | 1.630 | 24.970 | 16.640 | 10.400 | 10.030 | 2.610 |
| Standard deviation | 4.960 | 3.680 | 3.280 | 4.170 | 2.600 | 8.520 | 6.840 | 6.390 | 5.630 | 2.070 |
Note. * p
Concerning alexithymia, the dimension of difficulty identifying feelings was
only associated with emotional neglect (r = 0.240), whereas the dimension of
difficulty describing feelings was not significantly linked to all childhood.
Both depression and anxiety were moderately related to alexithymia (r
The structural equation model yielded adequate fit to data, evidenced by the fit
indices [
The model shows that childhood trauma was significantly positively associated
with alexithymia (
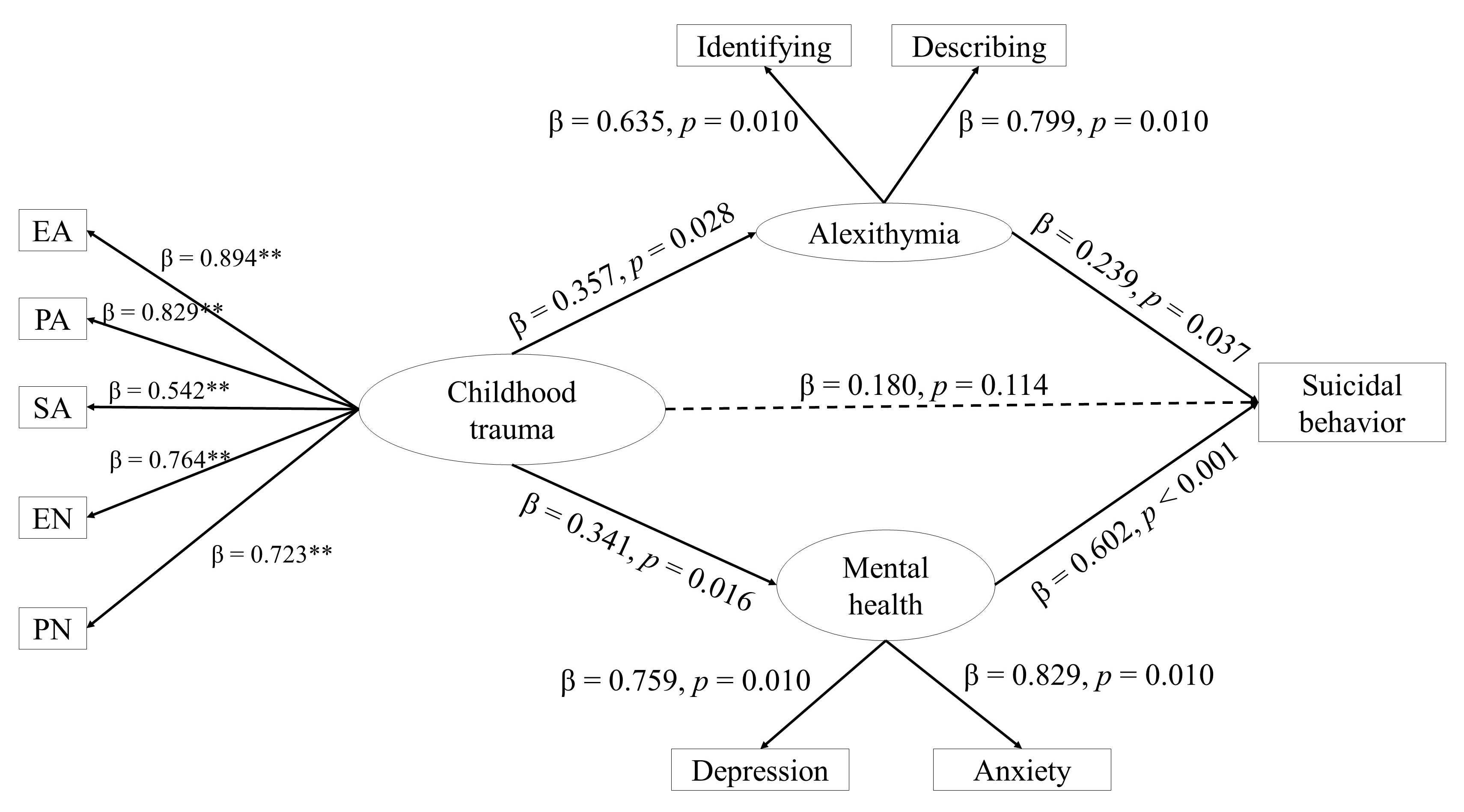 Fig. 1.
Fig. 1.
Structural equation modeling. Note. ** p
The current study examines the mediating role of alexithymia and mental health in the relationship between childhood trauma and suicidal behavior. Findings of the current study indicate that both alexithymia and mental health problems mediate the relationship between childhood trauma and suicidal behavior among individuals with dual diagnosis.
In contrast to prior investigations (Farrugia et al., 2011; Lotzin et al., 2019; Vaszari et al., 2011), this study revealed a distinct pattern whereby suicidal behavior exhibited a significant correlation exclusively with sexual abuse. Notably, there was a lack of substantial association between suicidal behavior and other forms of childhood trauma, namely emotional/physical abuse and neglect. One feasible explanation for this discrepancy lies in our study’s sample composition. The studies conducted by Vaszari et al. (2011) and Lotzin et al. (2019) both involved female participants exclusively. Furthermore, the study conducted by Farrugia et al. (2011) exclusively recruited individuals diagnosed with posttraumatic stress disorder, whereas our study encompassed a variety of psychological disorders. Accordingly, this underscores the significance of conducting research comprising a diverse representation of both substance use and psychological disorders to establish robust conclusions.
Consistent with previous research (Kopera et al., 2020; Zdankiewicz-Ścigała and Ścigała, 2018; Zdankiewicz-Ścigała and Ścigała, 2020), childhood trauma is associated with alexithymia, particularly the dimension of difficulties in describing feelings. Conversely, the dimension of difficulties in identifying feelings has shown a limited association with childhood trauma (i.e., only with sexual abuse). Prior studies have found that the correlation between childhood trauma and alexithymia is higher among people with psychological disorders and substance abuse (for a review, see De Berardis et al., 2017). Firstly, alexithymia may be a symptom of depression or anxiety (Lenzo et al., 2020; Lyvers et al., 2017; Sagar et al., 2021), and hence, a moderate correlation is found between the variables. On the other hand, one of the most widespread explanations is related to substance use as a way of coping with the distress caused by childhood trauma (Heggeness et al., 2020; Thorberg et al., 2011).
Findings indicate that childhood trauma is not directly related to suicidal behavior, but the two variables are related through the mediating effect of alexithymia and mental health problems. In other words, although no direct association was found between childhood trauma and suicidal behavior, the data support a significant indirect pathway via alexithymia and mental health symptoms, suggesting a potential underlying mechanism linking early adverse experiences with suicidal behavior. To our knowledge, no prior works have analyzed the mediating role of mental health and alexithymia among individuals with dual diagnosis. Notwithstanding, the effect of childhood trauma on mental health and other emotion-related variables is well-documented in longitudinal studies (McKay et al., 2021; McKay et al., 2022), as is the impact of mental health on suicidal behavior (Gili et al., 2019).
On the other hand, alexithymia could act as a mediator in the relationship between childhood trauma and suicidal behavior. Although no prior studies have analyzed the mediating role of alexithymia in individuals with dual diagnosis, this relationship has been examined in adolescents with mental health problems (Li et al., 2023; Titelius et al., 2018), male prisoners (Zhang et al., 2021), or individuals with substance use disorders (Di Nicola et al., 2024). Similarly, emotion regulation, a construct closely linked to alexithymia (Preece et al., 2023), has been studied as a mediator in general population (Laghaei et al., 2023; Turton et al., 2022) and psychiatrically hospitalized adolescents (Poon et al., 2023).
These results confirm previous evidence of the importance of emotional variables (e.g., alexithymia, emotion regulation) in understanding suicidal behavior (Iskric et al., 2020; Xie et al., 2021). Given the difficulties in identifying and describing feelings, this population may consume substances and engage in self-harm behaviors as a coping strategy for psychological distress (Frei et al., 2021; Heggeness et al., 2020; Rasmussen et al., 2016; Thorberg et al., 2011). Treatment has been shown to effectively modify alexithymia, leading to significant clinical benefits (Lukas et al., 2019; Norman et al., 2019; Salles et al., 2023). For all these reasons, it is crucial to incorporate psychological interventions based on alexithymia, that is, identifying and describing emotional states (Nunes da Silva, 2021). However, to our knowledge, no studies have addressed this issue in individuals with dual diagnosis. Therefore, these outcomes emphasize the need to conduct research among this population.
The findings here should be interpreted in the light of several limitations. First, the relatively small sample size may have led to insufficient statistical power to detect significant differences and to include potential confounding factors. However, it should be noted that this is a clinical population under active treatment with specific clinical characteristics. Regarding the sample, we note that we included mainly males, and substance use disorders and psychological diagnoses were highly heterogeneous. Hence, the interpretation of the results should be done with caution. Another limitation concerns the unbalanced sex distribution in the sample, which consisted predominantly of men. This limits the generalizability of the findings, as previous research suggests that men and women may differ in emotional processing, coping strategies, and the expression of suicidal behavior (Estévez et al., 2024; Miranda-Mendizabal et al., 2019). Therefore, we could not examine whether the model differed between men and women.
Further, a cross-sectional design comes with several limitations that impact the
interpretation of findings. Notably, this design also lacks information on the
temporal sequence of events, preventing the establishment of causal
relationships. In this line, it is prone to reverse causality, making it unclear
whether one variable causes another or vice versa. Additionally, cross-sectional
studies are susceptible to confounding variables, which can distort relationships
between variables. Consequently, we encourage future studies to analyze the
relationship between these variables with a prospective design. Another potential
limitation of the study is that the TLI did not reach the recommended threshold
of 0.90. This may reflect the complexity of the model, which included several
mediating variables. Still, future studies should consider testing simplified
versions of the model to further examine these relationships. Finally, concerning
the questionnaires, the variables were based on self-reported questionnaires, and
some of them were very extensive, so the information collected may have been
biased. In addition, although most subscales showed good internal consistency,
one presented a lower reliability (
While the current findings highlight key psychological mechanisms, it is important to consider that other underlying factors may also contribute to the observed associations (see Franklin et al., 2017). For instance, genetic vulnerability and neurobiological mechanisms may play a role in the development of both alexithymia and mental health problems in individuals exposed to childhood trauma. Future research should explore the interplay between biological, psychological, and environmental factors to better understand the complex pathways leading to suicidal behavior.
In conclusion, findings confirm and extend previous evidence showing the relationship between childhood trauma, alexithymia, mental health, and suicidal behavior among individuals with dual diagnosis. These results may be of scientific and clinical significance, given that they could help elucidate potential mechanisms underlying suicidal behavior in this population. From a clinical perspective, these findings emphasize the importance of early assessment of childhood trauma and alexithymia in patients with dual diagnosis, as these factors may inform suicide risk evaluation and treatment planning. Targeting alexithymia in therapy (e.g., emotional awareness, emotion labeling, and expression) may be particularly beneficial in improving emotion-regulation skills and reducing maladaptive coping strategies such as substance use or suicidal behavior. Moreover, integrating trauma-informed care and emotion-focused interventions into dual-diagnosis treatment programs may enhance outcomes, especially among those with a history of early adversity.
The data that support the findings of this study are available from the corresponding author, upon reasonable request.
AE: conceptualization, supervision. GA-D: conceptualization, formal analysis, methodology. LM: conceptualization, supervision. CL-A: adquisition of data, supervision. AIA-N: adquisition data, supervision. All authors contributed to critical revision of the manuscript for important intellectual content. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
This study was conducted following the principles of the Declaration of Helsinki. This study was conducted as an anonymous questionnaire survey; therefore, ethics approval was waived. All participants provided written informed consent.
Not applicable.
This research was supported by a predoctoral grant for training university teachers from the Spanish Ministry of Universities (ref.: FPU20/03045), and by a Postdoctoral grant from the Ministry of Science, Innovation and Universities (MCIN/AEI/10.13039/501100011033) and from the European Union NextGenerationEU/PRTR (ref.: JDC2022-048311-I).
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.