



 , Daniel Sánchez-Reolid 2,3, Marta Monferrer 4, María J Montes 1, Antonio Fernández-Caballero 2, Patricia Fernández-Sotos 5, Jorge J. Ricarte 5
, Daniel Sánchez-Reolid 2,3, Marta Monferrer 4, María J Montes 1, Antonio Fernández-Caballero 2, Patricia Fernández-Sotos 5, Jorge J. Ricarte 51 Mental Health Service, Complejo Hospitalario Universitario de Albacete (CHUA), 02006 Albacete, Spain
2 Institute for Research in Computer Science of Albacete, University of Castilla-La Mancha, 02071 Albacete, Spain
3 CIBERSAM-ISCIII (Biomedical Research Networking Centre in Mental Health), 28670 Madrid, Spain
4 Mental Health Service, Hospital Castellon, 12071 Castellon, Spain
5 Department of Psychology, Faculty of Medicine, Universidad de Castilla La Mancha, 02001 Albacete, Spain
Abstract
The present study is an observational, analytical, and cross-sectional examination of how the integrated motivational volitional (IMV) model of suicide applies to a clinical population. It differentiates between two groups of patients: those exhibiting suicidal ideation (SI) and those engaging in suicidal behavior (SB). The sample consists of 93 patients, with 56 in the SI group and 37 in the SB group, with an age range starting from 14 years old.
Data collection occurred from May 2021 to December 2022 at a Suicide Risk Outpatient Care clinic. The Entrapment Scale, Defeat Scale, and Beck’s SI Scale were used as validated scales to measure cognitive variables.
Moderate to strong associations were found between internal and external entrapment, defeat, and both SI and SB for the Beck SI Scale. Specifically, for the SB group, there were strong positive correlations between internal entrapment (0.680**) and external entrapment (0.740**) with the Defeat Scale, both statistically significant at p < 0.01. In contrast, the SI group showed moderate positive correlations between internal entrapment (0.540**) and external entrapment (0.460**) with the Defeat Scale, also significant at p < 0.01.
Our results highlight the importance of motivational factors, particularly internal and external entrapment and defeat. It is proposed that these factors could be addressed by universal prevention strategies for external entrapment, and also by strengthening protective factors related to internal entrapment, such as coping mechanisms and a sense of meaning.
Keywords
- internal entrapment
- external entrapment
- defeat
- suicidal ideation
- suicidal behavior
- motivational factors
Suicide and suicidal ideation (SI) represent a globally escalating problem (World Health Organization, 2019), demanding a deeper understanding and causal explanation to develop comprehensive models aiming to design effective preventive approaches.
Suicidal behavior (SB) should be conceptualized as a complex and multifactorial phenomenon that requires a comprehensive approach focused on the individual’s life meaning and suffering within their biographical, social, and cultural context. This perspective emphasizes that SB is extraordinarily variable over time and highly dependent on contextual elements. Recently, Al-Halabí and Fonseca-Pedrero (2024) highlight the importance of integrating social determinants and addressing the dehumanization often experienced in healthcare settings, which can exacerbate the suffering of individuals with SBs. Furthermore, these authors argue that understanding SB as an existential drama rather than merely a symptom of mental illness allows for a more nuanced approach to prevention and intervention. This integrative framework aims to improve the life circumstances of those at risk and facilitate their ability to seek help when needed, ultimately guiding them toward lives worth living.
Furthermore, there is no single explanatory theory that integrates all relevant aspects of this issue; instead, several models are attempting to understand suicide from different perspectives (Klonsky et al., 2018). Among them, the integrated motivational volitional Model of Suicide (IMV) proposed by O’Connor and Kirtley (2018) has emerged as a valuable tool to address the complexity of this issue, focusing on the transition from SI to SB. It is a comprehensive conceptual framework that includes components of psychopathology, suicide research, and health psychology. The IMV model has been empirically supported in both the general population and clinical samples, as stated recently in a systematic review of 100 studies, including 138,000 participants, where only 17 studies came from hospital samples (Souza et al., 2024).
The IMV model postulates that SB results from the interaction between motivational and volitional factors, composed of three consecutive phases. In the pre-motivational phase, individuals are predisposed to SI due to a combination of biological, social, and personality factors. The motivational phase introduces concepts of defeat and entrapment, where individuals experience hopelessness and helplessness, leading to the desire for death. Finally, the volitional phase bridges the gap between thought and action, incorporating factors such as impulsivity and access to means.
Defeat, characterized by powerlessness and inability to cope with life’s challenges (Gilbert and Allan, 1998), plays a central role in the development of suicidal thoughts. On the other hand, entrapment refers to feeling trapped in one’s circumstances with no way out (external entrapment) or in one’s thoughts (internal entrapment) (O’Connor and Portzky, 2018; Taylor et al., 2011), further fueling the desire for escape through suicide (for a more detailed explanation of the IMV model, refer to O’Connor and Kirtley, 2018).
Within the model, certain aspects are of clinical interest due to their potential value in designing preventive strategies, particularly in the transition from SI to behavior. Among them, the intricate interplay between defeat, internal and external entrapment, and their significant role in predicting SI and subsequent behaviour in the clinical population, has been recently explored.
A growing body of literature is exploring how the IMV model applies to clinical samples and how the model operates on individuals with SB and those with SI but no history of suicide attempts. Regarding clinical samples, a recent systematic review (Souza et al., 2024) indicated that both internal and external entrapment were significantly associated with SI in some cross-sectional studies. However, a study suggested that only internal entrapment, and not external entrapment, was associated with SI in both cross-sectional and prospective analyses (Höller et al., 2022b). An additional study reported that internal entrapment, but not external entrapment, was associated with an increase in SI in cross-sectional analyses but a decrease in prospective analyses when accounting for defeat, as participants scored lower on all IMV model variables over the course of the study. In summary, the evidence in clinical samples supports the relationship between internal entrapment and SI, while findings regarding external entrapment are less consistent; there were few studies that differentiated between both types in terms of the IMV model.
Although the IMV model does not explicitly distinguish between internal and external entrapment, the literature suggests that measuring these dimensions separately may be relevant when assessing the risk of suicide in clinical populations. Forkman T et al. (2018), using network analysis techniques, found two separate dimensions of entrapment, supporting the idea of considering them as distinct and relevant constructs in suicide risk assessment. Furthermore, the pronounced impact of defeat on internal entrapment and its predictive effect on SI over time highlights the importance of differentiating between internal and external entrapment in understanding the experience of SI (Höller et al., 2022a).
While most individuals who experience SI do not progress to making suicide attempts (Kessler et al., 1999), it is crucial to identify predictive factors for such progression. The IMV model proposes that the factors influencing SI (motivational factors) differ from those driving SB development (volitional factors). Therefore, exploring how the model applies to different clinical groups is essential.
In a study by Dhingra et al. (2015) with 1288 healthy UK adults, distinct groups were identified (SI, SB, and controls), finding that suicide attempters differed from ideators in all volitional factors (fearlessness of death, impulsivity, exposure to SB), except discomfort tolerance. Attempters, compared to ideators, were more likely to have family or friends who self-injured or attempted suicide, showing higher impulsivity and fearlessness of death. In this study, motivational factors did not differentiate between the two suicide groups regarding thoughts of death by suicide. In another study, Wetherall et al. (2018) found demographic, motivational, and volitional differences between controls and those with suicide ideation or attempts, and specifically volitional factors distinctly separated those with ideation from those who attempted suicide. Attempters reported higher acquired capability, mental imagery of death, and impulsivity, and were more likely to know someone who attempted suicide. Cleare et al. (2021) distinguished between non-suicidal self-harm and suicide attempts, showing that variables such as SI, defeat, internal entrapment, and perceived burdensomeness were pivotal in differentiating the groups, with the strongest associations observed in the suicide attempt group.
In this study, we investigate the influence of motivational factors, specifically the distinction between internal and external entrapment, as well as defeat, not only in the genesis of SI but also in individuals who have engaged in SB. Our aim is to elucidate how these variables of the model manifest in a clinical sample treated in a specialized outpatient clinic for the prevention of suicidal risk, to which they are referred during moments of crisis. Although a central assertion of the IMV is that it is the volitional phase variables that differentiate between ideation and enactment groups (O’Connor and Kirtley, 2018), our interest focuses on the motivational phase due to the notable levels of entrapment and defeat present in individuals with SB, which we propose would be higher in this group.
Therefore, this study gains relevance by analyzing the correlation of motivational factors in both clinical populations, using validated scales for measurement in a specialized context of suicidal crises. Additionally, the present study hypothesizes that O’Connor’s model applies to both clinical samples, but it is expected to be more effective in clinical samples that have engaged in SB, particularly concerning the variables of the second phase of the model, highlighting the importance of motivation in this transition. This allows for a deeper understanding of the specific dynamics operating in clinical populations, emphasizing the importance of investigating internal and external entrapment separately to identify more effective and personalized intervention strategies.
Thus, current research aims to build upon the literature findings by extending them to two areas: (1) Distinguishing between internal and external entrapment analyzing the influence of both not only on SI (measured using Beck’s SI Scale) but also on SB, (2) Explore how O’Connor’s model applies to different groups, SI (SI) and others with SB (SB), as we propose that the associations of the variables studied will correlate suicide risk to a greater extent in the group with suicide behavior.
This is an observational, analytical and cross-sectional study.
The sample is composed of 93 patients, with an age range starting from 14 years old. The mean age of patients in the SI group is 33.39 years, while in the SB group it is 28.24 years. The sample was recruited from the outpatient consultation for suicide risk prevention at a University Hospital Complex, which indicates that they are part of a clinical population. For demographic characteristics of the sample see Table 1.
| Characteristic | SI (n = 56) | SB (n = 37) |
| Total patients surveyed | 56 | 37 |
| Mean age (years) | 33.39 | 28.24 |
| Age standard deviation (SD) | 17.61 | 16.00 |
| Under 18 years (%) | 26.8% | 35.1% |
| Ages 18–29 years (%) | 26.8% | 29.7% |
| Ages 30–39 years (%) | 12.5% | 13.5% |
| Ages 40–49 years (%) | 7.1% | 8.1% |
| Ages 50–59 years (%) | 17.9% | 10.8% |
| Ages |
8.9% | 2.7% |
| Female proportion (%) | 54.5% | 78.4% |
| Primary education (%) | 50.9% | 48.6% |
| Students (%) | 41.1% | 55.6% |
| Unskilled workers (%) | 17.9% | 13.9% |
| Marital status—Single (%) | 61.8% | 61.1% |
| Marital status—Married/Cohabiting (%) | 27.3% | 25.0% |
| Childless (%) | 69.4% | 62.5% |
| Living with family of origin (%) | 58.9% | 67.6% |
| Living with own family (%) | 33.9% | 24.3% |
| Urban residence (%) | 75.5% | 80.0% |
| Perceived economic status—Middle class (%) | 50.9% | 57.1% |
SI, suicidal ideation; SB, suicidal behavior.
We included participants aged 14 years and older to comprehensively examine the application of the IMV model of suicide across different age groups. This age range allows us to capture a diverse spectrum of experiences related to SI and behavior, recognizing that both adolescents and adults may experience feelings of internal and external entrapment and defeat. While we acknowledge that the manifestations of suicidal thoughts can differ significantly between these age groups, the core psychological constructs of entrapment and defeat are relevant across the lifespan. By including younger participants, we aim to explore how these motivational factors influence SI and behavior, thereby enhancing our understanding of suicide risk in a clinical context and informing targeted interventions for individuals at varying developmental stages. The minimum number of subjects for the sample was determined by the Statulator Program (Dhand and Khatkar, 2014), which indicates that a number of 64 is needed to achieve a power of 80%.
The selection criteria were as follows: (a) SI/active SB. (b) Speak Spanish correctly. (c) Sign the informed consent (in the case of subjects under 18 years of age, informed consent adapted to the minor and informed consent to be completed by the legal guardian were included). Regarding the exclusion criteria, it was established: (a) Intellectual disability. (b) Pervasive developmental disorder. (c) Neurological damage that affects the completion of the questionnaires. (d) To be diagnosed with any neurological or systemic disease with significant central nervous system involvement. (e) Individuals under hospitalization. Participants were recruited from a suicide prevention outpatient clinic, so psychiatric diagnoses were not considered as an inclusion/exclusion criterion. Also, the exclusion of past and current depression was due to our focus on evaluating the specific impact of cognitive variables (internal and external entrapment and defeat) on SI. Additionally, the literature suggests that entrapment and defeat variables are independent predictors of SI, justifying their isolated analysis (Pollak et al., 2021).
Data collection was carried out from May 2021 to December 2022. Participants were collected from the monographic consultation of the Suicide Risk Outpatient Care clinic at the mental health service of the University Hospital Complex, which is composed by a psychiatrist and a clinical psychologist. The participants of this program are referred from the different Mental Health units (Psychiatric Emergency Services, Brief Hospitalization Unit, Interconsultation and Liaison Unit, External Consultations) from Primary Care and Specialized attention, when there is an active SI or behavior. After a first assessment consultation, the professionals oversaw assessing whether the patient met the inclusion/exclusion criteria for the research study. An informed consent was signed after explaining the study.
Subjects were classified and included in one group or another based on SI and behaviors presented in the last three months. If the patient presented both SI and behavior, they were included in the SB group. It was the professional who explored this information in the first interview, through the clinical interview.
Beck Hopelessness Scale, HS (Beck et al., 1974). It includes 20 items in true and false format, where three dimensions are assessed: feelings about the future, loss of motivation, and expectations. Beck and Steer have proposed the following scoring scale for its interpretation: 0–3: normal or asymptomatic range; 4–8: Mild; 9–14: Moderate; and 15–20: Severe. It has been observed that a score greater than 9 is a good predictor of eventual SB. For our study, the Spanish version was used (Rueda-Jaimes et al., 2018), which has shown adequate psychometric properties in previous studies carried out in Latin America.
Scale for suicide ideation, SSI (Beck et al., 1979). This is a hetero-applied scale developed to quantify and evaluate suicidal intentionality, or the degree of seriousness and intensity with which someone thought or is thinking of committing suicide. No validation studies have been carried out in our country, and we only have some adaptations or translations into Spanish. It consists of 19 items to quantify and evaluate SI. Each item is classified with a score from 0 to 2, with the highest score indicating greater severity.
Defeat Scale (Gilbert and Allan, 1998). The scale validated in Spanish has been used (Ordoñez-Carrasco et al., 2021). This scale is responsible for measuring the psychological construct of defeat present within the motivational phase in the Integrated Motivational-Volitional Model of SB by O’Connor and Kirtley (2018). The scale consists of 16 items, with a score range of 0 (Never) to 4 (Always) that summatively quantifies this variable. On this scale, the scores of the 16 items ranging from 0 to 4 must be added. This scale has a very high internal consistency with a Cronbach’s Alpha coefficient of 0.94 for both men and women.
Entrapment Scale (Gilbert and Allan, 1998). The scale validated in Spanish has been used for this study (Ordoñez-Carrasco et al., 2021). Through this scale, it is intended to measure the psychological construct of entrapment. This instrument is equipped with 16 items rated on a scale ranging from 0 (Not at all like me) to 4 (Extremely like me), which summatively determines the degree to which this construct is present in the target population. study. Items 1 to 10 are designed to measure internal entrapment and items 11 to 16 would measure external entrapment. It has high levels of internal consistency, with Cronbach’s Alpha for internal trapping being 0.93 and for external trapping 0.89 (Carvalho et al., 2011). In this scale it is necessary to analyze separately: Items from 1 to 10 = Internal entrapment: Add the total score. The higher the score, the more entrapment (that is, worse); Items 11 to 16 = External entrapment: Add the total score. The higher the score, the more entrapment (that is, worse).
Statistical analyses were conducted using SPSS (version 27.0, IBM Corporation,
Armonk, NY, USA). To analyze the correlation between the variables of entrapment
(both internal and external) and defeat, the scores obtained from each of the
scales provided to the individuals were used, which were correlated according to
the type of patient, using Spearman’s correlation. Statistical power (1 -
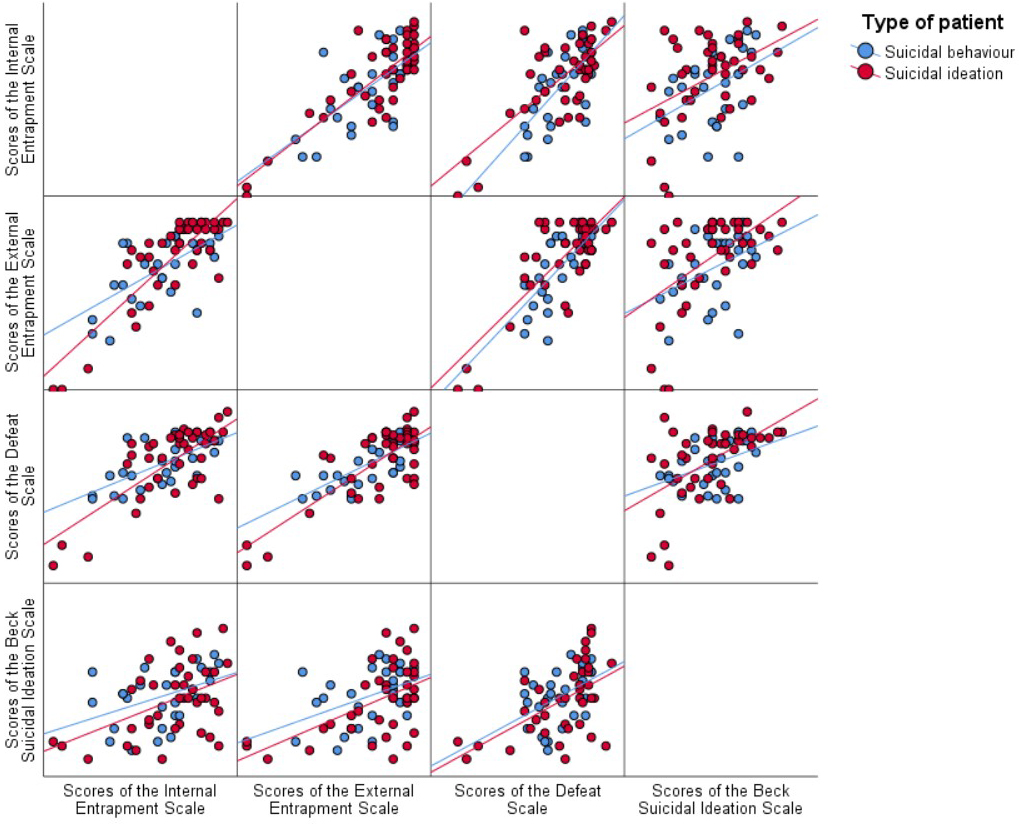 Fig. 1.
Fig. 1.
Matrix of scatter graphs of the correlations obtained for the scores of the Entrapment Scale (internal and external), Defeat Scale, and Beck’s SI Scale depending on the type of patient.
Clinical and demographic information is summarized in Table 1. The correlations obtained for the scores of the Entrapment Scale (both internal and external) and the Defeat Scale with the Beck SI Scale, in both groups of participants (SI and SB) are presented in Table 2.
| Patient group | Score on the internal Entrapment Scale | Score on the external Entrapment Scale | Score on the Defeat Scale | ||
| Beck’s Suicide Scale score | Suicidal behaviour | correlation Coef. | 0.550** | 0.430* | 0.510** |
| p | 0.002 | 0.023 | 0.004 | ||
| 1 - |
0.960 | 0.960 | 0.970 | ||
| 0.740 | 0.660 | 0.720 | |||
| n | 29 | 28 | 30 | ||
| SI | correlation Coef. | 0.360* | 0.380* | 0.470** | |
| p | 0.022 | 0.014 | 0.002 | ||
| 1 - |
0.980 | 0.980 | 0.980 | ||
| 0.600 | 0.620 | 0.680 | |||
| n | 40 | 41 | 42 |
*The correlation is significant at the 0.05 level (two-tailed); **The
correlation is significant at the 0.01 level (two-tailed); Effect size:
For participants with SB, a moderate positive correlation is observed for both internal entrapment and external entrapment with the Beck Suicide Ideation Scale. This indicates that there is a significant relationship between internal (0.550**) and external entrapment (0.430*) and SI in subjects with SB, being the correlation stronger for internal entrapment, suggesting that these factors may be associated with an increased risk of SB in this population. Also, there is a significant correlation between defeat and suicide risk measured through the Beck Suicide Ideation Scale (0.510**) in this group of individuals.
For the suicide ideation group, a weak positive correlation between the internal (0.360*) and external entrapment (0.380*) scales and the Beck SI Scale was found. This indicates that there is a significant but not very strong relationship between feelings of entrapment and suicidal thoughts in subjects with SI. Additionally, there is a moderate positive correlation between the Defeat Scale and the Beck SI Scale (0.470**), suggesting a stronger association between feelings of defeat and SI in this patient group.
In Table 3, the correlations obtained for the scores of the Entrapment Scale (both internal and external) with the Defeat Scale are presented for both the SI and SB patient groups. For the SI group, there is a moderate positive correlation between the internal Entrapment Scale (0.540**) and the Defeat Scale, as well as between the external Entrapment Scale (0.460**) and the Defeat Scale. This suggests a significant but not extremely strong relationship between feelings of entrapment and defeat in individuals with SI.
| Patient group | Score on the internal Entrapment Scale | Score on the external Entrapment Scale | ||
| Defeat Scale score | Suicidal behaviour | correlation Coef. | 0.680** | 0.740** |
| p | 0.000 | 0.000 | ||
| 1 - |
1.000 | 1.000 | ||
| 0.820 | 0.860 | |||
| n | 35 | 34 | ||
| SI | Correlation Coef. | 0.540** | 0.460** | |
| p | 0.000 | 0.001 | ||
| 1 - |
0.990 | 0.990 | ||
| 0.730 | 0.680 | |||
| n | 50 | 49 |
**The correlation is significant at the 0.01 level (two-tailed); Effect size:
In contrast, for the SB group, there is a strong positive correlation between both the internal (0.680**) and external entrapment (0.740**) scales and the Defeat Scale. This indicates a robust relationship between feelings of entrapment and defeat in participants exhibiting SB. These correlations are statistically significant at the 0.01 level, highlighting the strength of the relationships observed.
The present study broadens the literature by performing an examination of how the IMV model applies to clinical populations, in real-time suicidal crisis, by including subjects in an outpatient suicide prevention program, particularly distinguishing between participants exhibiting SI and those already engaged in SB. In this way, two primary findings emerged from this investigation. First, consistent with our initial hypotheses, the motivational moderators (internal and external entrapment, and defeat) exhibited moderated to strong associations with both SI and SB, affirming the empirical relevance of the IMV model and its clinical implications in patient cohorts. These findings align with prior literature examining the IMV model in clinical contexts, demonstrating its applicability to patient samples (Lucht et al., 2020). Moreover, motivational variables showed stronger correlations within the SB group than to the SI group, suggesting that the IMV model may perform more effectively in individuals exhibiting SB than in those with SI. Similar findings have been observed in other study such as that by Van Eijk et al. (2023), which identified distinct profiles among young adults based on IMV-derived suicide risk variables, with the higher risk of suicide behavior cluster showing stronger associations with the IMV model.
The importance of moderators related to the volitional phase have also been well established, and they are proposed by the IMV as a key factor in the model, that play a crucial role in the transition from thought to action. For instance, Wetherall et al. (2018) demonstrated that only volitional phase variables differentiated between suicide attempters and individuals with SI. Additionally, Dhingra et al. (2016) found no differences in motivational factors between suicide groups. Nonetheless, we emphasize the significance of our results, as they elucidate the role of motivational moderators in the transition from SI to SB, since they are highly correlated with suicide ideation in subjects that have already attempted suicide. Furthermore, these moderators are modifiable psychological factors that can be attended to in psychological therapy, so professionals can act in a preventive level before the patient is determined to act on their thoughts.
The relevance of addressing motivational factors, especially entrapment (both internal and external), and defeat, lies in their close association with engaging in SB, although occurring in an earlier phase. Consequently, this gives the mental health professionals more time frame than the imminent risk that confers to be in the volitional phase of the IMV model. Hence, interventions targeting these factors may potentially interrupt the progression toward the volitional phase, where the “determination to die” becomes clearer (O’Connor and Kirtley, 2018). Therefore, intervening during the phase where participants are formulating a strong desire to die and perceive no alternative, could prevent the evolution towards the volitional phase, allowing for therapeutic exploration of alternative options alongside the therapist.
In this context, the study by Besch et al. (2024) emphasizes the importance of assessing reasons for living during a suicidal crisis, suggesting that these reasons can serve as protective factors. The authors of the present article believe that these protective factors may help counteract feelings of internal entrapment and defeat. Furthermore, Al-Halabí and Fonseca-Pedrero (2024) argue that existential suffering and intolerable psychological pain are key elements in a person’s decision to commit suicide, aligning with the notion that internal entrapment can be a precursor to SB. The perceived lack of solutions to the problems causing this pain can lead to a sense of defeat, where individuals feel they have no control over their lives, a sentiment reflected in our findings. On the other hand, the contextual-functional approach proposed by these authors suggests that understanding SB must extend beyond individual diagnoses and consider the biographical and social context of the person, which can help unravel the dynamics of entrapment and defeat. This implies that interventions should focus on improving life circumstances and fostering a sense of meaning, which could assist individuals in overcoming feelings of entrapment.
Our second main finding, regarding the second hypothesis of our study, was that external and internal entrapment exhibited varying degrees of association with defeat for the two study groups. The results showed that feelings of entrapment and defeat are more strongly associated with SB than with SI, but furthermore, external entrapment is more strongly associated with defeat. Thus, our results indicate that external entrapment may be more closely related to suicide risk in the SB group.
Few studies have separated these two constructs of entrapment, particularly within clinical samples using the IMV model. Available literature presents mixed results regarding the relevance of internal versus external entrapment in SB, while limited in quantity. Rasmussen et al. (2023) and Owen et al. (2018) also reported a differential effect of external and internal entrapment, suggesting that internal entrapment may have a greater influence on SI development than external entrapment. Lucht et al. (2020) similarly found that internal entrapment mediated the effect of baseline defeat on 3-month SI, while external entrapment mediated the association between baseline defeat and 3-month suicide attempt likelihood, which is in line with our findings.
A potential explanation for the stronger correlation between external entrapment and defeat over suicide risk in the SB group could be attributed to these subjects being in a “suicidal crisis”, wherein external stressors exert a greater impact, consistent with the notion that external stressors/events may more strongly influence SI formation in higher-risk individuals. Overall, these findings suggest that the relationship between defeat and entrapment may serve as a significant indicator of suicide risk, underscoring the importance of considering these variables together in suicide risk assessment and prediction.
Our findings have relevant implications for clinical practice. First, this study contributes to understanding the psychological factors influencing SB when applying the IMV model to clinical samples, emphasizing the importance of motivational factors and specifically, the role that external and internal entrapment has on the feeling of defeat, which is a factor of great importance in developing SB. Moreover, these findings highlight the relevance of differentiating between populations with ideation vs behavior, as it provides more specific information for each group and may support the development of interventions for at-risk populations. Furthermore, we emphasize the importance of including defeat and entrapment feelings in suicide risk assessments.
Enhancement of coping mechanisms via psychotherapeutic interventions, alongside psychopharmacological treatment, is an established method for improving symptoms of depression, such as feelings of internal defeat. Additionally, it is necessary to underscore the importance of integrating strategies that specifically target external entrapment. In this context, occupational therapy may be considered as a crucial modality, since it helps provide individuals experiencing hopelessness and a perceived lack of control over their environmental circumstances with the essential skills to navigate and resolve their external challenges.
Moreover, considering that external entrapment refers to the perception of being trapped by unfavorable external circumstances, such as adverse social conditions, it is essential, in line with the recommendations of Pirkis et al. (2023), that prevention strategies extend beyond clinical interventions. These strategies should also encompass population-level and social actions, such as awareness campaigns and the removal of barriers to accessing healthcare services. Universal prevention, aimed at raising awareness about SB across the entire population, and selective prevention, which targets more vulnerable groups, are crucial for addressing the social determinants that influence suicide risk. Recent literature emphasizes the importance of integrating social determinants into national suicide prevention plans, highlighting that macroeconomic factors, public policies, and social values play significant roles in shaping mental health outcomes, and ultimatelly impacting on feelings of entrapment, especially external entrapment, that have been linked to SI and behavior, as showed in our study.
Nonetheless, several limitations warrant consideration. Regarding the sample, it is composed of a relatively small size, which may overestimate the observed relationships between variables, and this sample originated from a specialized clinic for individuals in suicidal crisis or high risk of suicide, which should be considered when interpreting the results. Also, the broad age range in our sample, which includes participants aged 14 and older, may influence how entrapment and defeat are interpreted. Adolescents and adults may conceptualize these constructs differently due to their distinct emotional and cognitive development stages. This highlights the need for future research to consider these differences when analyzing data and developing targeted interventions for each age group. Additionally, our study did not investigate volitional factors. Further directions for future research may include evaluating how therapeutic interventions targeting motivational moderators, such are entrapment and defeat, impact the evolution of SB in individuals at high risk.
The IMV is emerging as a valid model that integrates different aspects of SB and has proved great applicability to subjects at high risk of suicide attempts, as shown in this study and others. Some specific moderators have been found in the early phases of this model, being the most relevant defeat, internal and external entrapment. In this way, they emerge as therapeutic targets for developing therapeutic strategies. The findings of this study underscore the importance of addressing motivational factors, particularly internal and external entrapment, and defeat, in the assessment and prediction of suicide risk. It is crucial to recognize that external entrapment is often influenced by broader social determinants, which necessitates the implementation of universal prevention strategies. These strategies should not only focus on clinical interventions but also encompass social and population-level actions, such as awareness campaigns and the removal of barriers to accessing healthcare services. Additionally, reinforcing protective factors related to internal entrapment, such as enhancing coping mechanisms and fostering a sense of meaning in life, can significantly contribute to reducing suicide risk. By integrating these approaches, we can create a more comprehensive framework for suicide prevention that addresses both individual and societal factors. The need to continue researching modifiable factors that confer a higher risk of suicide is of the uttermost importance given the public health problem that suicide represents globally. The results of the current study broaden the current knowledge regarding this matter.
Data supporting the findings of this study are available from the appropriate author upon reasonable request. The data is not publicly available due to ethical or privacy restrictions.
MAD: conceptualization; DSR: visualization, methodology, formal analysis, data curation; MM: resources, data curation; MJM: supervision, critical feedback on study design and data interpretation; AFC and PFS: methodology, conceptualization; JJR: supervision, conceptualization, project management. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
The study was approved by the Research Ethics Committee of the Complejo Hospitalario Universitario de Albacete. As all data were fully anonymized, no specific formal approval number was issued. The study adhered to the ethical principles of the Declaration of Helsinki (2004), the Belmont Report, and the Oviedo Convention, as well as Spanish biomedical research and data protection laws. Written informed consent was obtained from all participants or their legal guardians. All data were anonymized and handled confidentially.
Not applicable.
This research received no external funding.
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.