



 , Carolina C. Salazar 1, Gressley A. Valdés 1, Matías F. Silva 1, Felipe I. Varas 1, Gabriela Ayala 1, Gustavo Munro 1, Mario A. Laborda 1, Gonzalo Miguez 1, Vanetza E. Quezada-Scholz 1,*
, Carolina C. Salazar 1, Gressley A. Valdés 1, Matías F. Silva 1, Felipe I. Varas 1, Gabriela Ayala 1, Gustavo Munro 1, Mario A. Laborda 1, Gonzalo Miguez 1, Vanetza E. Quezada-Scholz 1,*
1 Department of Psychology, Faculty of Social Sciences, University of Chile, 7800284 Ñuñoa, Chile
Abstract
The fear of public speaking significantly affects those who suffer from it. The present research aimed to evaluate the efficacy of a virtual reality (VR) exposure therapy protocol for fear of public speaking.
A randomized controlled pilot study with repeated measures was conducted in an experimental group (n = 7) and a wait-list control group (n = 7). The protocol consisted of 7 to 8 sessions: 1 for psychoeducation, 1 for cognitive flexibility, 4 to 5 for VR exposure and 1 for closure. The instruments used were the Personal Report of Confidence as a Speaker-12 (PRCS-12) and the Self-Statements during Public Speaking (SSPS) scale.
A decrease was found in the scores of the PRCS-12 and in the SSPS negative self-statements subscale; however, no significant changes were reported on the positive self-talk subscale.
The results showed evidence in favor of the efficacy of the protocol. Limitations and clinical implications of the findings are discussed, as well as improvements to the protocol to obtain better results.
Keywords
- social anxiety
- fear of public speaking
- cognitive behavioral therapy
- exposure
- virtual reality
According to the World Health Organization (2022), recent years have shown an increasing mental health crisis, primarily evidenced by a 25% rise in the global prevalence of anxiety and depression-related disorders. In Chile, the “Termómetro de la Salud Mental en Chile Achs-UC” (Mental Health Thermometer in Chile Achs-UC) reveals anxiety remains the leading psychological issue in the country, with 24.8% of surveyed individuals reporting anxiety problems (Pontificia Universidad Católica, 2024). One such anxiety-related disorder is Social Anxiety Disorder (SAD), characterized by intense fear or anxiety in social situations where individuals may be judged by others (APA, 2013). Literature describes two adult subtypes of SAD: one subgroup experiences anxiety in interaction contexts (e.g., having conversations) and performance contexts (e.g., public speaking); another subgroup experiences anxiety predominantly in performance contexts, particularly during adolescence and early adulthood (Kahlon et al., 2019). This commonly manifests as fear and/or anxiety related to public speaking.
Fear of public speaking has significant consequences for affected individuals, potentially impacting job opportunities, academic performance, and social relationships (Crome et al., 2015; Girondini et al., 2023). Additionally, it can lead to increased feelings of loneliness or social isolation, a general decrease in quality of life, and increased susceptibility to developing SAD (Kahlon et al., 2019; Wittchen and Fehm, 2003) or secondary disorders such as depression and substance use disorders (Crome et al., 2015; Maldonado and Reich, 2013). These considerations are crucial since, although fear of public speaking may not always have clinical relevance, when anxiety is sufficiently intense to be incapacitating, this fear becomes pathological (Clark and Beck, 2012; Tron et al., 2014). Early treatment of this fear has been shown to reduce overall levels of SAD (Hindo and González-Prendes, 2011), thus reducing the associated social and personal costs (Kahlon et al., 2019).
Fear or anxiety related to public speaking involves cognitive, behavioral, and physiological aspects. Regarding cognitive symptoms, a set of dysfunctional beliefs, cognitive biases, and irrational thoughts that affect the individual’s attention are identified (Clark and Wells, 1995; Maldonado and Reich, 2013). In this context, de la Rubia et al. (2016) argue that elevated perceptions of social standards during public speaking lead to increased self-assessment, which impairs the individual’s performance and raises social anxiety to maladaptive levels that may impact daily life. This is expressed through dysfunctional self-statements about the situation, such as catastrophic ideas regarding one’s own performance and the audience’s reaction (APA, 2013).
An important aspect related to SSPS is the speaker’s self-efficacy, defined as the individual’s belief in their capacity to achieve a certain level of performance (Bandura, 1997). In this regard, anxiety and self-efficacy have a negative correlation; higher self-efficacy is associated with lower anxiety levels, and vice versa (Brown and Morrissey, 2004). Low self-efficacy results in poor performance outcomes and increased anxiety, making it crucial for confidence in public speaking (Verano-Tacoronte and Bolívar-Cruz, 2015). According to Méndez et al. (1999), public speaking confidence is a continuous dimension with a positive pole (confidence in public speaking) and a negative pole (fear of public speaking).
On the other hand, behavioral symptoms, according to Girondini et al. (2023), are interconnected with cognitive symptoms. In the presence of negative self-statements or low confidence during presentations, individuals may engage in various behaviors to mitigate or avoid anxiety. Typically, avoidance behaviors include actions where individuals avoid situations that cause fear (Girondini et al., 2023; Thunnissen et al., 2022). For example, a person might pretend to have a cold to skip a public presentation and avoid the associated fear. These behaviors sustain anxiety in the long term, making it crucial to intervene (Krypotos et al., 2015; Wong et al., 2023).
Moreover, fear of public speaking is associated with increased physiological arousal before and during exposure to the feared situation (Girondini et al., 2023; Goodman et al., 2017). This can manifest through increased heart rate and respiratory rate, sweating, facial, neck, and chest flushing, shortness of breath, dizziness, vertigo, tremors, nausea, and/or vomiting (Bartholomay and Houlihan, 2016; Orejudo et al., 2012).
Cognitive Behavioral Therapy (CBT) is an effective treatment for SAD (Reichenberger et al., 2017). A central component of CBT is exposure therapy. This technique is based on the conditioned fear paradigm, which has proven to be a valid model for anxiety-related disorders (Mineka and Zinbarg, 2006). Conditioned fear is a type of associative learning in which a stimulus that initially elicits no emotional response (neutral stimulus; e.g., an audience) becomes associated with an aversive event (unconditioned stimulus or US; e.g., social rejection), thereby turning into a conditioned stimulus (CS) that predicts the occurrence of the aversive event, resulting in a conditioned fear response (CR) (Mallea et al., 2019). Consequently, an individual may experience anxiety in public speaking situations due to the association between social rejection (US) experienced during or observed in an embarrassing situation in front of others (CS).
Within the conditioned fear paradigm, extinction learning forms the basis of exposure therapy. In this type of learning, the organism is exposed to repeated presentations of the CS without the US. This procedure leads to a reduction in fear toward the CS over time, as it no longer predicts the aversive event (Mallea et al., 2019). Exposure therapy follows this same logic, patients are exposed to the fear-inducing stimulus (e.g., an audience during a public presentation) without the feared event occurring (e.g., being mocked), which leads to new learning that is incompatible with the original association (i.e., that the CS is followed by the US). Exposure can be carried out using either real-life (in vivo) or imagined stimuli (Chard and van Zalk, 2022), both of which are well-supported by extensive empirical evidence (Chesham et al., 2018).
Regarding exposure therapy for fear of public speaking, in vivo exposure exercises have been found to be impractical or unfeasible, as they would require access to and control over a real audience (Kahlon et al., 2019). On the other hand, for many clients, vividly imagining the feared scenario in imaginal exposure therapy can be difficult due to challenges in generating and maintaining a clear mental image (Krijn et al., 2004). However, virtual reality (VR) technology has emerged as a promising solution to these problems by creating a realistic virtual audience that gives the user the sensation of being present in a public speaking situation (Kahlon et al., 2019).
Currently, VR is being used to enhance anxiety treatment (Boeldt et al., 2019). During Virtual Reality Exposure Therapy (VRET), clients are exposed to computer-generated simulations of feared situations (Anderson et al., 2013). Advances in VR technology allow users to enter fully immersive and programmable environments, with simulated interactions involving virtual humans. This enables individualized, gradual, and controlled exposure that is easy for therapists to implement and potentially more acceptable to patients than in vivo or imaginal exposure (Hembree et al., 2003). Due to these advantages, VRET has the potential to increase access to exposure-based treatment, particularly for individuals with fear of public speaking (Powers and Emmelkamp, 2008; Freeman et al., 2017).
VRET has been used to treat various conditions such as SAD, generalized anxiety disorder, post-traumatic stress disorder, specific phobias, and panic disorder (Boeldt et al., 2019). Several studies have demonstrated the efficacy of VRET for anxiety disorders (Chesham et al., 2018; Krijn et al., 2004; Reeves et al., 2021), understood as producing significant improvements in participants’ mental health (Berg, 2021). This therapy has been found to be as effective as in vivo exposure therapy (Chesham et al., 2018; Reeves et al., 2021). Additionally, Kahlon et al. (2019) found that both therapist-guided and self-guided single-session VRET interventions reduced public speaking anxiety.
However, despite the evidence supporting VRET’s efficacy, the situation in Latin America reveals a lack of knowledge, research, and implementation of such therapies. Santoyo et al. (2021) conducted a systematic review on the use of VR for fear or anxiety disorders, finding that only 3% of the studies were from Latin America. Moreover, in Chile, there is limited application and evaluation of interventions for SADs. Therefore, the present study addresses the need to develop protocols with an optimal cost-benefit ratio within the Latin American context.
Consequently, the aim of this pilot study was to evaluate the efficacy of a brief VRET protocol in reducing fear of public speaking in adults. It was expected that VR would be an effective intervention for treating public speaking anxiety, as evidenced by a decrease in the symptoms experienced by individuals during public speaking situations. To this end, the protocol developed by Ayala (2022) for treating public speaking fear using VR was adapted. This protocol had previously demonstrated feasibility both in-person and remotely among university students.
A stepped randomized controlled trial was conducted with two groups randomly assigned to one of two conditions: an experimental group that received treatment according to the VRET protocol for fear of public speaking, and a control group placed on a waitlist.
Inclusion criteria were: (a) individuals over 18 years old who reported fear of public speaking, as indicated by a Personal Report of Confidence as a Speaker-12 (PRCS-12) score equal to or greater than 48 points; and (b) individuals available to attend weekly treatment sessions for two months. Exclusion criteria were based on adverse effects associated with the use of VR headsets, as outlined by the Amelia Virtual Care software (n.d.), a platform that provides controlled virtual environments for mental health interventions. Excluded were individuals with: (a) heart disease; (b) severe respiratory illnesses; (c) vertigo syndrome; (d) schizophrenia or other active psychotic disorders; (e) epilepsy; (f) severe visual impairment or blindness; (g) deafness; and (h) pregnancy. Additionally, individuals undergoing any type of psychological treatment were excluded due to potential interference with the study. All criteria were assessed using a screening form provided alongside the PRCS-12 at recruitment.
A total of 26 participants were recruited and randomly assigned to the experimental and control conditions. Data from participants who did not attend or complete the treatment and/or failed to respond to the assessments were excluded. One participant was excluded due to outlier data linked to risk factors identified in the Clinical Outcomes in Routine Evaluation-Outcome Measure (CORE-OM; Feixas et al., 2012) and the participant form. The final sample consisted of 14 participants (7 in each group), with 9 identifying as female (64.29%) and 5 as male (35.71%). Participants ranged in age from 19 to 28 years, with a mean age of 22.6 years (SD = 2.31). A priori power analysis was conducted using G*Power (Faul et al., 2007), assuming a medium effect size of 0.30 (Cohen’s f) based on Anderson et al. (2013), an alpha level of 0.05, and a power of 0.80, indicating a required sample size of 18 participants.
Exposure sessions were conducted using “Pico G2 4K” VR headsets and the “Amelia Virtual Care” software (version 54; XRHealth, Boston, MA, USA), which provided access to five scenarios designed for exposure to public speaking. These scenarios allow the therapist to control the appearance of various specific stimuli, such as the size of the audience, questions, and audience reactions (e.g., yawns, applause, laughter), thereby offering patients a more immersive and personalized exposure environment.
To assess fear of public speaking, the study included both primary measures targeting specific symptomatology and secondary measures related to general anxiety and psychological distress. The primary measures were as follows:
2.3.2.1 Personal Report of Confidence as a Speaker-12 (PRCS-12)
The Spanish version of the 12-item questionnaire, validated in a university
population, was used (Martinez-Pecino and Durán, 2013). This
questionnaire assesses the level of confidence with which individuals face public
speaking and their fear of doing so (e.g., item 5: “Although I speak fluently
with my friends, I cannot find words to express myself on stage”). The
instrument demonstrates high internal consistency (
2.3.2.2 Self-Statements During Public Speaking (SSPS) Scale
The Mexican version was used (de la Rubia et al., 2016), composed of 10
items divided into two subscales: the positive self-statements subscale (e.g.,
item 3: “This is an uncomfortable situation, but I can handle it”) and the
negative self-statements subscale. Item 8 in the original version includes a
colloquial Mexican phrase “la voy a regar”, which was adapted to a more
commonly used expression in Chile, resulting in the item: “la voy a
embarrar”. In the english version, the item reads “I’ll probably bomb
out anyway”. The adaptation and validation of the scale for the Mexican
population show high internal consistency (
Additionally, the following secondary measures related to anxiety and general psychological distress were reported:
2.3.2.3 Clinical Outcomes in Routine Evaluation-Outcome Measure (CORE-OM)
The Spanish version by Feixas et al. (2012) was used, which has been
validated in Chile by Errázuriz et al. (2025). This instrument is
specifically designed to evaluate the therapeutic progress of patients with
various psychological problems and/or disorders, as it assesses psychological
distress. It consists of 34 items evaluating several dimensions, including
Subjective Well-being (W; e.g., item 4: “I have felt good about myself”),
Problems/Symptoms (P; e.g., item 11: “Tension and anxiety have prevented me from
doing important things”), General Functioning (F; e.g., item 21: “I have been
able to do most of the things I needed to do”), and Risk (R; e.g., item 16: “I
have made plans to end my life”). The instrument includes a measure of clinical
significance, which reflects therapeutic change. It demonstrates high internal
consistency (ranging from
2.3.2.4 Liebowitz Social Anxiety Scale
The Spanish version by Bobes et al. (1999) was used. This 24-item scale is
divided into two subscales: one related to performance anxiety (e.g., item 20:
“Giving a report to a group”) and the other to social interaction situations
(e.g., item 12: “Meeting new people”), which are commonly challenging for
individuals with social anxiety. The LSAS assesses both the degree of
fear or anxiety experienced in these situations and the level of avoidance for
each item on both subscales. It demonstrates high internal consistency (ranging
from
2.3.2.5 Subjective Units of Distress Scale (SUDS)
This one-item self-report scale, created by Wolpe (1969), was implemented through the VR headsets, as it is integrated into the Amelia Virtual Care platform. It measures the participant’s subjective experience of anxiety.
Participants were recruited through an open call by posting a digital flyer on the U-Cursos platform (the official platform for students and faculty at the University of Chile) as well as on social media. Individuals who met the inclusion criteria were selected. Afterward, they signed an informed consent form prior to beginning treatment, which had been approved by the Ethics Committee (CEI) of the Faculty of Social Sciences at the University of Chile (No. 26-34/2023). Both control and treatment group participants were assessed through repeated measures. While the treatment group received the intervention, the control group was monitored using the same assessments administered to the experimental group. Subsequently, control group participants received the same treatment.
The procedures were carried out by ten therapists, all of whom were either licensed psychologists or psychology graduates who were currently enrolled in or had completed the Postgraduate Certificate in CBT at the University of Chile. They received training that included detailed explanations of the therapy protocol and safety procedures, therapeutic materials, and the VR instruments to be used, in addition to biweekly supervision sessions. Before beginning the process, the therapists signed informed consent forms. Each participant was assigned to one therapist, who guided them through the entire treatment process. Additionally, a lead researcher assisted the therapist as a technical aide during the VR exposure sessions, managing the Amelia Virtual Care platform.
The treatment protocol consisted of 7 to 8 sessions distributed across four modules (Psychoeducation, Cognitive Flexibility, Exposure, and Closure), with each session lasting approximately one hour. Sessions were held at the Center for Applied Psychology (CAPs) and the Faculty of Social Sciences at the University of Chile. The protocol used was developed by Ayala (2022) and was adapted according to the improvement suggestions provided by the author, especially regarding its clinical applicability and module structure (see Table 1). Furthermore, adjustments were made to modify the delivery format to enable in-person application with participants.
| Session | Module | Objective | Activity |
| 1 | Psychoeducation | To provide psychoeducation about the fear of public speaking, Cognitive Behavioral Therapy (CBT), and techniques to cope with this fear. | Group workshop divided into groups of 5 participants. |
| 2 | Cognitive Flexibility | To help participants develop the ability to address situations that trigger emotions and respond to them adaptively. | Cognitive approach. Some worksheets from the Unified Protocol for Transdiagnostic Treatment of Emotional Disorders are used (chapter 4 and 5; Barlow et al., 2019). |
| 3 | Exposure | To assess how participants react to VR headsets. To create an anxiety hierarchy based on the level of discomfort in each scenario. To address participants’ avoidance of public speaking situations through VR exposure. | Test the VR headsets and observe participants’ reactions. Develop an anxiety hierarchy based on the different scenarios, using participants’ responses through Subjective Units of Distress Scale (SUDS). Exposure to the 1st scenario in the anxiety hierarchy through brief exercises (e.g., spelling, addition, subtraction). |
| 4 | Exposure | Address avoidance through VR exposure. Analyze irrational beliefs and alternative behaviors. | Exposure to the 2nd and 3rd scenarios in the anxiety hierarchy through brief improvisation activities (self-description and general knowledge topics). |
| Therapist’s feedback on the treatment. | |||
| 5 | Exposure | Address avoidance through VR exposure. Analyze irrational beliefs and alternative behaviors. | Exposure to the 4th scenario in the anxiety hierarchy through a prepared presentation by the participant, followed by questions from the virtual audience. |
| Therapist’s feedback. | |||
| 6 | Exposure | Address avoidance through VR exposure. Analyze irrational beliefs and alternative behaviors. | Exposure to the final scenario in the anxiety hierarchy through a longer prepared presentation, with questions from the virtual audience during the presentation. |
| 7 | Exposure (optional) | Address avoidance through VR exposure. Analyze irrational beliefs and alternative behaviors. | Same activity as the previous session, for participants who may need it. |
| 8 | Closure | End of intervention and relapse prevention. | Feedback on the treatment. |
Note: The table outlines the chronological development of the protocol and the session planning across the project. Source: Own elaboration.
To assess the efficacy of the protocol, evaluations were conducted at four stages, with the aim of assessing the different modules of the therapy. In Stage 1, participants were assessed before starting treatment; in Stage 2, they were evaluated after completing the psychoeducation and cognitive flexibility modules; in Stage 3, assessment followed the exposure module; and in Stage 4, participants were assessed one week after completing the intervention. The only measure administered differently was the SUDS, which was recorded during each exposure session.
Regarding the exposure sessions, the duration of each exposure ranged between 15 and 25 minutes, becoming longer toward the final sessions. Additionally, repeated intra-session SUDS measurements were implemented every two minutes during these sessions to monitor anxiety fluctuations throughout the session and allow the therapist to take precautions or intervene in case of emotional destabilization.
To analyze the collected data, version 2.3 of the statistical software Jamovi (Sydney, New South Wales, Australia)
(The jamovi project, 2022) was used. To evaluate the efficacy of the
protocol, a 4
In the case of the CORE-OM, as described by Feixas et al. (2012), the total score is calculated as the average of the scores from all dimensions, excluding the risk dimension. Additionally, a clinical change analysis specific to the instrument is included. A clinical cutoff score of 10 is used to identify clinically significant levels of distress. To detect a reliable clinical change, the authors state that a minimum difference of 5 points between questionnaire administrations must be observed. This significance is reflected in a decrease in scores, meaning that lower scores indicate greater clinical improvement following treatment.
To assess SUDS, a one-way repeated measures ANOVA was conducted. The within-subject factor was the mean SUDS score of the experimental group for each of the four exposure sessions. For participants who requested a fifth exposure session, the data from that session were used in place of the fourth session in the exposure module. This instrument is scored on a scale from 1 (no anxiety) to 10 (intolerable anxiety), with lower scores indicating reduced anxiety.
For main effects and interactions, partial eta squared
(
The 4
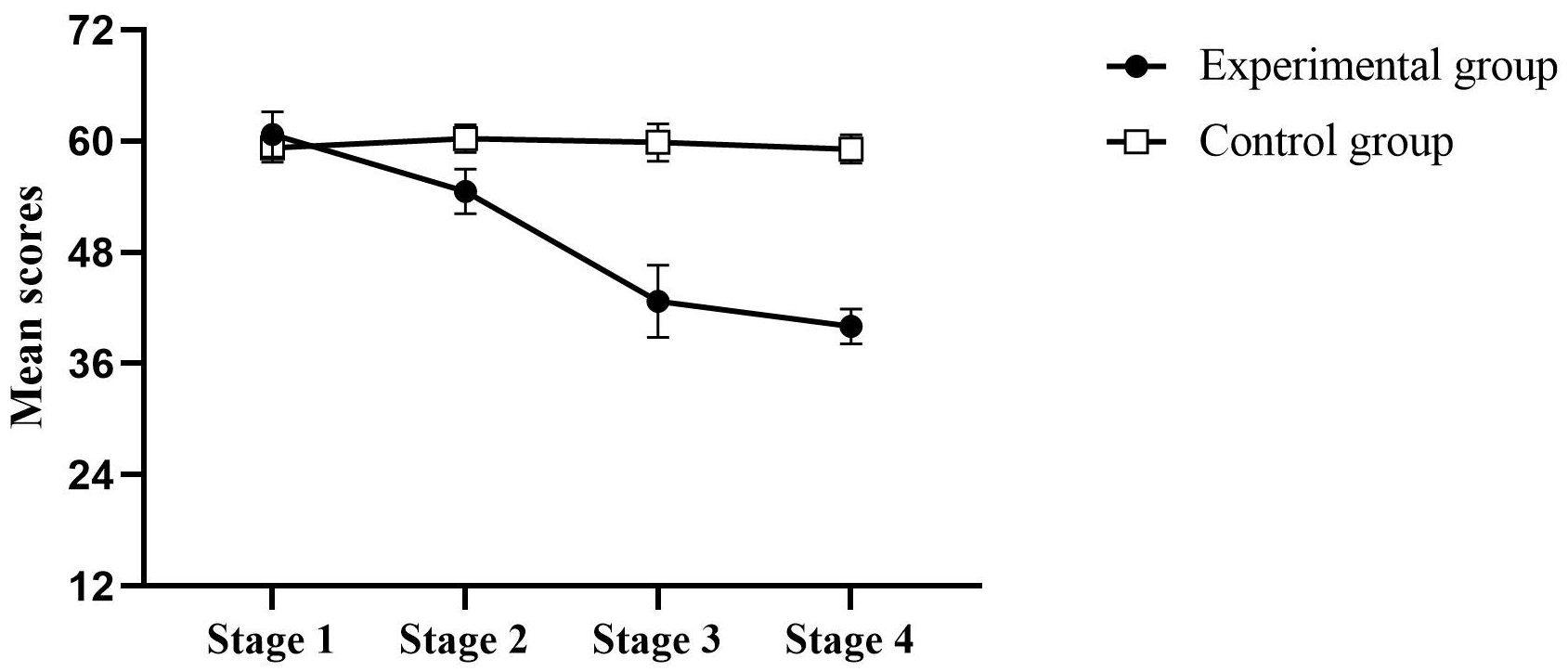 Fig. 1.
Fig. 1.
Distribution of Personal Report of Confidence as a
Speaker-12 (PRCS-12) scores. Note: The mean of each score
obtained is plotted across treatment stages, with standard error bars shown for
each group at each stage. The distribution of PRCS-12 scores shows an increase in
confidence when speaking in public throughout the stages in the experimental
group (●), compared to the control group (
Regarding the positive self-statements subscale of the SSPS, the 4
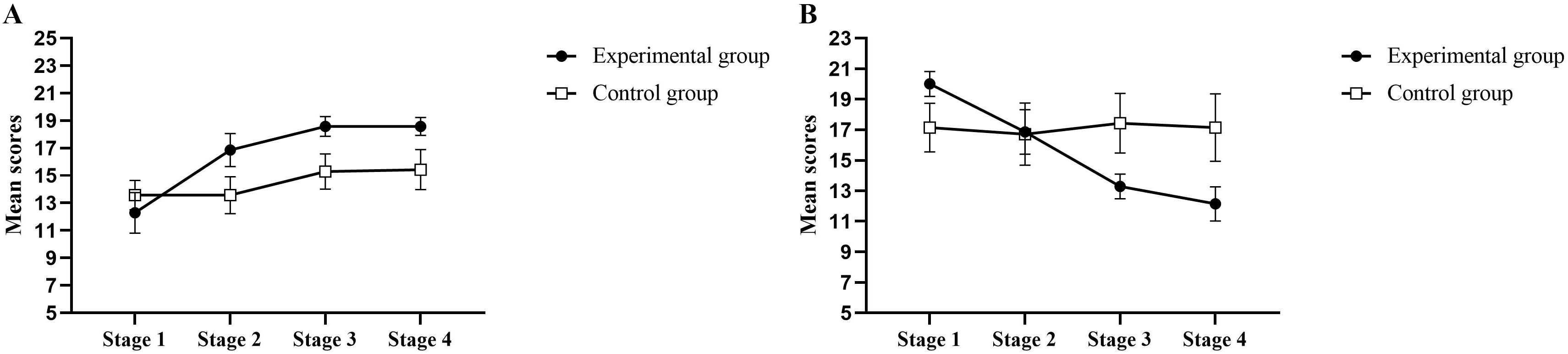 Fig. 2.
Fig. 2.
Distribution of Self-Statements during Public Speaking (SSPS)
scores according to the positive self-verbalizations subscale (A) and the
negative self-verbalizations subscale (B). Note: The mean of each score obtained
is plotted across treatment stages, with standard error bars shown for each
condition at each stage. (A) shows the distribution of scores for positive
self-verbalizations, where a slight increase can be observed across the stages in
the experimental group (●), while a smaller increase is observed in the
control group (
For the negative self-statements subscale, the 4
For the total CORE-OM score, the 4
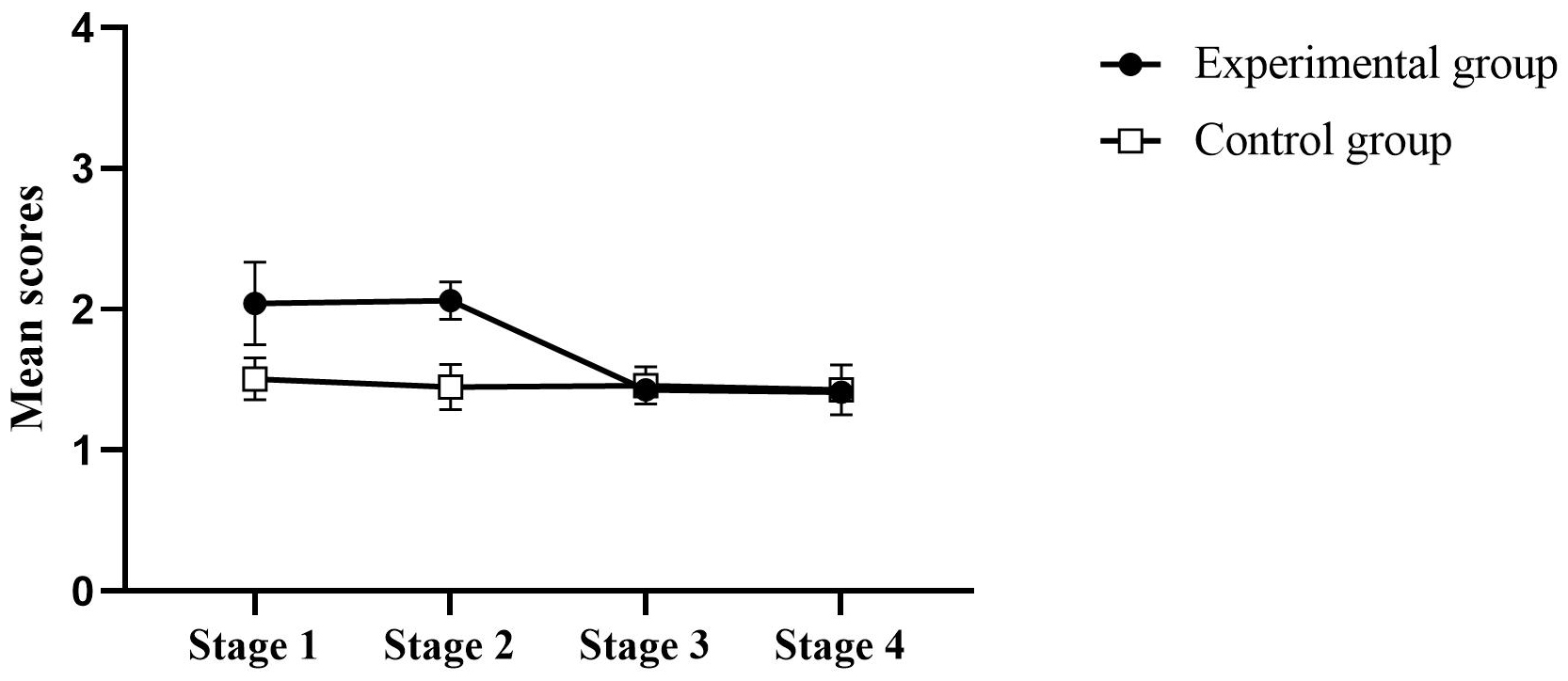 Fig. 3.
Fig. 3.
Distribution of Clinical Outcomes in Routine Evaluation-Outcome
Measure (CORE-OM) total scores.Note. The mean of each score obtained
is plotted across treatment stages, with standard error bars shown for each
condition at each stage. The distribution of total CORE-OM scores shows that, in
Stage 1, the experimental group (●) had a higher mean score than the
control group (
When analyzing clinical change, the experimental group initially showed a moderate to severe level of distress (20.40 pts.). During Stage 2, this distress slightly increased (20.61 pts.), but then considerably decreased in Stage 3 (14.28 pts.) and Stage 4 (14.13 pts.), reaching a moderate distress level. This reflects a reliable clinical change with a decrease of 6.12 points between Stage 1 and Stage 3, 6.27 points between Stage 1 and Stage 4, 6.33 points between Stage 2 and Stage 3, and 6.48 points between Stage 2 and Stage 4. On the other hand, the control group started with a moderate clinical level of distress (15.05 pts.), which did not significantly decrease throughout Stages 2 (14.49 pts.), 3 (14.59 pts.), and 4 (14.29 pts.), indicating no clinically reliable change.
No statistically significant results were found in the subscales. However, reliable clinical changes were observed in all dimensions except for the risk dimension. In the well-being subscale, the experimental group initially scored 19.64 and showed a clinically significant reduction by Stage 4, scoring 12.85 (reliable change index = 6.79). In contrast, the control group started at 17.50 and maintained similar scores across all measurements, indicating no clinically reliable change.
In the symptoms/problems subscale, the experimental group initially reported clinical distress at 22.14, which decreased to 16.42 by Stage 4 (reliable clinical change index = 5.73). The control group, which started at a clinical level of 14.05 pts., did not reach a reliable clinical change in any later stage.
In the general functioning subscale, the experimental group started with a score of 18.92, which significantly decreased to 12.26 by Stage 4 (reliable clinical change index = 6.66). In contrast, the control group began with a score of 15.24, which slightly decreased to 13.81 by Stage 4, not reaching a clinically reliable change.
Performance subscale: Regarding the anxiety score on this subscale, the 4
Social Interaction Subscale: Regarding the anxiety score on this
subscale, the 4
Among participants in the experimental group, 3 requested a fifth exposure
session (42.86%). The one-way repeated measures ANOVA revealed no significant
differences across stages (F[3, 18] = 0.09, p = 0.96,
This pilot study evaluated the efficacy of a VRET protocol for fear of public speaking in adults. The results obtained from this randomized controlled pilot trial showed that the application of the VR-based treatment protocol led to significant changes in the experimental group compared to the control group, particularly in the increase in public speaking confidence, as reflected in the reduction of PRCS-12 scores and the decrease in negative self-statements on the SSPS subscale.
According to the findings, an increase in confidence when speaking in public was observed across the different treatment stages in the experimental group, while no such changes were found in the control group. In this sense, symptomatology in the treated group was reduced, especially following the exposure sessions.
These favorable results are consistent with findings from Anderson et al. (2013), who also observed an increase in public speaking confidence in a group that received VR exposure therapy for public speaking anxiety, compared to a waitlist control group. The consistency between these findings and those of Anderson et al. (2013) supports the hypothesis that the VRET protocol is effective in increasing confidence in public speaking situations.
Additionally, these results support the PRCS as a reliable tool for detecting post-treatment changes (Comeche et al., 1995; Leary, 1990). The sensitivity of this instrument has been demonstrated in various studies (García-López et al., 2002; Olivares et al., 2002; Anderson et al., 2013; Piñeiro, 2015; Bartholomay, 2015; Ayala, 2022), which validates its use as a primary measure for evaluating treatments targeting fear of public speaking.
Regarding the SSPS, the reduction in negative self-statements also provides evidence in favor of the protocol’s efficacy. This finding is particularly relevant given that negative self-talk is a central component of social anxiety, as described by the APA (2013). It aligns with a previous study indicating that exposure to feared situations can help reduce the negative and catastrophic thoughts associated with social anxiety (Hofmann et al., 2012). Therefore, the reduction in negative self-statements may be a key mediator of the therapeutic effect observed in the reduction of public speaking fear.
On the other hand, a significant increase in positive self-statements was observed across stages, regardless of group condition. It is important to note that the SSPS is not commonly used as a primary measure, unlike the PRCS, as shown in various meta-analyses of exposure treatments for public speaking fear (Chesham et al., 2018; Chard and van Zalk, 2022; Krijn et al., 2004; Reeves et al., 2022). Nevertheless, the SSPS has demonstrated sensitivity to therapeutic change in both of its subscales (Gallego et al., 2010). This is consistent with findings by Zacarin et al. (2019), who reported significant differences in both SSPS subscales following treatment. In that study, the treatment placed greater emphasis on cognitive and affective exploration, as well as functional analysis of the public speaking situation. Additionally, the treatment duration was longer, 13 or 15 sessions depending on the group. These prior findings are important for contextualizing the present pilot study, where the treatment emphasis was placed on the exposure module rather than cognitive flexibility, and the number of sessions was lower. Future studies could incorporate a greater number of sessions focused on cognitive aspects in this protocol to examine whether changes occur in the SSPS positive self-statements subscale.
In terms of the secondary measures, the experimental group showed a decrease in symptoms in the total CORE-OM score. However, in the statistical analyses, the Condition variable did not show a significant difference, which may be due to the control group starting with lower scores than the experimental group, making it difficult to attribute changes directly to the treatment. In terms of reliable clinical change, the experimental group showed improvement, whereas the control group did not. Based on the results obtained, there appears to be a trend toward clinically significant improvement, with reliable clinical change particularly evident after the exposure sessions, indicating that the greatest reduction in distress occurred during those sessions. This offers modest evidence in favor of the treatment; however, this difference could be more robust with a longer treatment duration, specifically within the exposure module.
Regarding the LSAS, results did not show significant differences between the experimental and control groups, meaning that the changes cannot be attributed to the treatment. Similar results have been found in a previous study, such as Harris et al. (2002), where a 4-session VR exposure treatment for public speaking anxiety was compared to a waitlist control group. The authors hypothesized that anxiety reduction may require a longer treatment duration. Therefore, future studies could assess the impact of a more prolonged intervention on LSAS scores.
Finally, regarding the results in the SUDS, the analyses showed no significant changes across the exposure module, with the overall session average being 5.2 points. In another study, most patients showed an increase in subjective distress scores on this scale when there were changes in the VR scenario (Zacarin et al., 2019) or when task complexity increased during sessions (Harris et al., 2002). In Takac et al. (2019), researchers sought to support the fear habituation model using SUDS during VR exposure sessions for public speaking fear; however, they also found no significant differences within each session, and only a few between-session differences. These findings are relevant for contrasting with the present study’s results. For example, exposure sessions here also involved scenario changes and a gradual increase in task complexity. Thus, a reduction in subjective distress may not reflect the success of an exposure protocol. This may explain the findings of the present study, or alternatively, it may be necessary to maintain a high level of subjective distress for the treatment to be effective (Craske et al., 2014). This could be because eliciting an emotional and behavioral reaction in the patient is essential to explore dysfunctional beliefs and promote the formation of new, adaptive learning through therapy (Beck and Haigh, 2014).
One of the main limitations of this pilot study was the small sample size (14 participants, 7 in each group). This reduced number limits the generalizability of the results and decreases the statistical power of the analyses. While the design allowed for the exploration of preliminary differences between groups, future studies should consider larger samples to validate and extend the findings.
Another important limitation to consider is that the data may be influenced by the sample’s homogeneity, as it predominantly consisted of individuals with higher education levels. This can be explained by the fact that fear of public speaking is one of the most common problems among university students, as the ability to communicate effectively before an audience is a key factor in many professions (Piñeiro, 2015). Although the number of individuals who meet clinical criteria is low, this fear is still impactful enough that 76% of people avoid at least one public speaking situation each year, and 45% experience significant or extreme difficulty when facing such situations, with university students being the most affected (Piñeiro, 2015). Therefore, to improve the external validity and overall applicability of future research, it is recommended to include a more diverse sample in terms of educational background. This approach will allow for a more comprehensive and nuanced understanding of the phenomenon and the ability to more robustly extrapolate results to the general population.
Moreover, the treatment was administered by different therapists, which could have influenced the outcomes. Individual differences in therapeutic style, clinical experience, or communication skills may affect the effectiveness of the treatment, even when using a standardized protocol. In this regard, the therapist can represent a significant source of variability in psychotherapy outcomes (Johns et al., 2019; Lutz and Barkham, 2015; Mahon et al., 2024), highlighting the importance of considering this factor in future studies.
Lastly, this study only compared the effectiveness of the treatment against a no-treatment condition. Therefore, future research should ideally compare the efficacy of this protocol with other types of treatments, as well as with in vivo exposure therapy. Several studies have indicated that VR demonstrates comparable efficacy to in vivo exposure therapy (Anderson et al., 2013; Chesham et al., 2018; Reeves et al., 2021). Additionally, it would be important to include follow-up assessments to evaluate long-term effects and determine whether the efficacy of the protocol is sustained over time (Hill et al., 2016).
Ultimately, although these findings should be interpreted with caution due to the exploratory nature of the study design and the small sample size, the results reveal promising implications for the field of mental health, as effects suggesting the efficacy of the protocol in treating public speaking anxiety were observed. In this way, the study contributes to the development and refinement of treatments in clinical settings.
One potential advantage of VRET for SAD is its ability to reduce treatment dropout rates, since exposure to social situations takes place in a virtual environment rather than in real-life situations, as occurs with in vivo exposure (Emmelkamp et al., 2020).
Another implication of this pilot study is its contribution to the development of treatments that incorporate new technologies. The well-documented technological gap in Latin America, evidenced by access barriers and lack of digital skills (Economic Commission for Latin America and the Caribbean, 2021) makes this especially relevant. This is particularly important considering the WHO (2023) has stated that diverse technological innovations should be adopted to positively impact public health and improve people’s quality of life. Given this context, it is essential to promote access to treatment and raise awareness of these issues in the region to support and encourage help-seeking among those in need.
In summary, while this is a pilot study and results should be interpreted with caution, considering the absence of effective VR-based protocols in Chile, the findings of this research represent a relevant starting point for the development, evaluation, and implementation of VR interventions aimed at various anxiety disorders in the region.
The results of this pilot study suggest that the VR exposure protocol for fear of public speaking is effective in reducing associated symptomatology and increasing confidence when speaking in front of an audience, as evidenced by the reduction in PRCS-12 scores and in negative self-statements on the SSPS in the experimental group. These findings, although preliminary, are consistent with previous literature and support the use of VR exposure as a promising therapeutic alternative for the treatment of fear of public speaking.
Study data are under the custody of the responsible investigators, who have ensured their appropriate handling and protection as encrypted data in a database for a period of 5 years, after which they will be deleted. Due to ethical, confidentiality, and legal considerations, these data are not available to be shared with third parties.
SE, CS, GV, MS, GA, GMi, ML, and VQ conceived and designed the study. VQ participated in and supervised all stages of the research, providing intellectual leadership and overseeing the scientific and formative aspects of the work. SE, CS, GV, and MS were responsible for data collection and performed the data analysis. SE, CS, GV, MS, GMu, and FV contributed to the interpretation of the results. SE, CS, GV, MS, and FV drafted the first version of the manuscript. MS, SE, CS, GV, GA, FV, GMu, GMi, ML, and VQ critically revised the manuscript for important intellectual content. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
The study was conducted in accordance with the guidelines of the Declaration of Helsinki and was reviewed and approved by the Ethics Committee (CEI) of the Faculty of Social Sciences, University of Chile (No. 26-34/2023). All participants provided written informed consent.
We sincerely thank the therapists Cecilia Cordero-Ruz, Catalina Landa, Jonathan Badilla, Paulina Pino, Catalina Aguilar, Javiera Buzeta, Viviana Saez, Francisca Ayala and Sebastián Ibacache, whose contribution was essential to this study.
This work was funded by the National Agency for Research and Development of Chile through Fondecyt 1251388 (V.E. Quezada-Scholz) and Fondecyt 1220797 (G. Miguez).
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.