

 , Dushad Ram 2,*
, Dushad Ram 2,*
1 Department of Medicine (Family Medicine), Shaqra College of Medicine, Shaqra University, 11961 Shaqra, Saudi Arabia
2 Department of Medicine (Psychiatry), Shaqra College of Medicine, Shaqra University, 11961 Shaqra, Saudi Arabia
Abstract
Burnout among doctors in Saudi Arabia is a rising issue, affecting well-being, healthcare quality, and patient outcomes. This scoping review examines burnout among physicians in Saudi Arabia, offering a comprehensive overview of its prevalence, contributing factors, and implications.
A systematic literature search (2000–2024) was conducted across major databases (PubMed, Scopus, Web of Science, and Google Scholar) for English-language studies using validated burnout assessments among physicians in Saudi Arabia. Data were analyzed using descriptive and thematic approaches.
Burnout prevalence varied widely (17.6%–100%), with the highest rates observed among emergency medicine physicians, intensive care unit (ICU) fellows, and surgical residents. Emotional exhaustion and depersonalization were most frequently reported. Key contributing factors included younger age, marital status, heavy workloads, frequent on-call shifts, inadequate resources, and limited support for non-Saudi physicians. High burnout correlated with increased medical errors, reduced care quality, and physician attrition. Emotional intelligence, mindfulness, and physical activity provided some protection, while institutional strategies like workload redistribution and mental health support were also beneficial. Residents and non-Saudi physicians were particularly vulnerable.
Burnout is prevalent and multifactorial among physicians in Saudi Arabia, requiring targeted interventions at both systemic and individual levels. There is an urgent need for policies addressing workload, support systems, and cultural factors to mitigate burnout and improve physicians' well-being, thereby guiding research and promoting sustainable healthcare solutions aligned with national priorities.
Keywords
- professional burnout
- Saudi Arabia
- physician
- doctors
- scoping review
Doctor burnout is a global crisis affecting individual well-being, healthcare systems, and patient outcomes, characterized by emotional exhaustion, depersonalization, and low personal accomplishment. It leads to poor decision-making, medical errors, reduced care quality, workforce attrition, absenteeism, and low job satisfaction (Patel et al, 2018). Burnout rates are highest in high-stress environments like emergency rooms (ERs), intensive care units (ICUs), and surgical specialties, but vary by country, specialty, and setting. Cultural, institutional, and systemic factors influence burnout, underscoring the need for context-specific research (Patel et al, 2018).
In Saudi Arabia, the healthcare system is undergoing rapid transformation, driven by population growth and the ambitious objectives of Saudi Vision 2030, which places considerable pressure on medical professionals. Saudi Vision 2030, a national transformation initiative launched in 2016, aims to diversify the economy, enhance public services, and promote societal well-being, with healthcare as a central focus. The initiative seeks to create a vibrant society by improving quality of life, a thriving economy by fostering workforce productivity, and an ambitious nation by building sustainable systems. Unique cultural and systemic factors, such as high patient loads and societal expectations, exacerbate burnout among medical professionals (Alluhidan et al, 2020). Although research on this issue is increasing, it remains fragmented, often concentrating on specific specialties, regions, or subpopulations (Assiri, 2023; Sultan and Sultan, 2023). This scoping review synthesizes existing literature on burnout among doctors in Saudi Arabia to provide a comprehensive understanding, thereby supporting informed decision-making by policymakers and healthcare administrators. Addressing burnout aligns with Saudi Vision 2030’s emphasis on workforce sustainability, healthcare quality, and societal well-being, thereby prioritizing the well-being of medical professionals and fostering a resilient healthcare system.
This review employed the Population-Concept-Context (PCC) framework to examine
burnout (concept) among physicians (population) within Saudi healthcare
environments (context). The inclusion criteria encompassed English-language
studies conducted from 2000 to 2024, focusing on practicing physicians in Saudi
Arabia and utilizing validated burnout measures, specifically the Maslach Burnout
Inventory-Human Services Survey (MBI-HSS) or its adaptation for medical personnel
(MBI-HSS-MP). All 71 studies included in the review employed either the MBI-HSS
or MBI-HSS-MP. The MBI assesses three constructs: emotional exhaustion (EE;
characterized by feelings of being emotionally overextended by work, with scores
of
Exclusion criteria included studies on other healthcare professionals, reviews without primary data, studies outside Saudi Arabia, or where burnout was not a primary or secondary outcome. PubMed, Scopus, Web of Science, and Google Scholar were searched using keywords, Boolean operators, and Medical Subject Headings (MeSH) terms (e.g., “burnout”, “physicians”, “doctors”, “Saudi Arabia”, “emotional exhaustion”, “depersonalization”, “personal accomplishment”). Following Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) guidelines, 199 records were identified, 82 unique records remained after removing duplicates, and 71 eligible studies were included after screening by two independent reviewers (Fig. 1). Data were extracted using a standardized form (Table 1) and analyzed using a mixed-methods approach. Although no formal quality assessment was conducted, methodological rigor, sample representativeness, and tool reliability were informally evaluated. Findings are reported per PRISMA-ScR, including descriptive tables, narrative summaries, and visual representations of prevalence and themes.
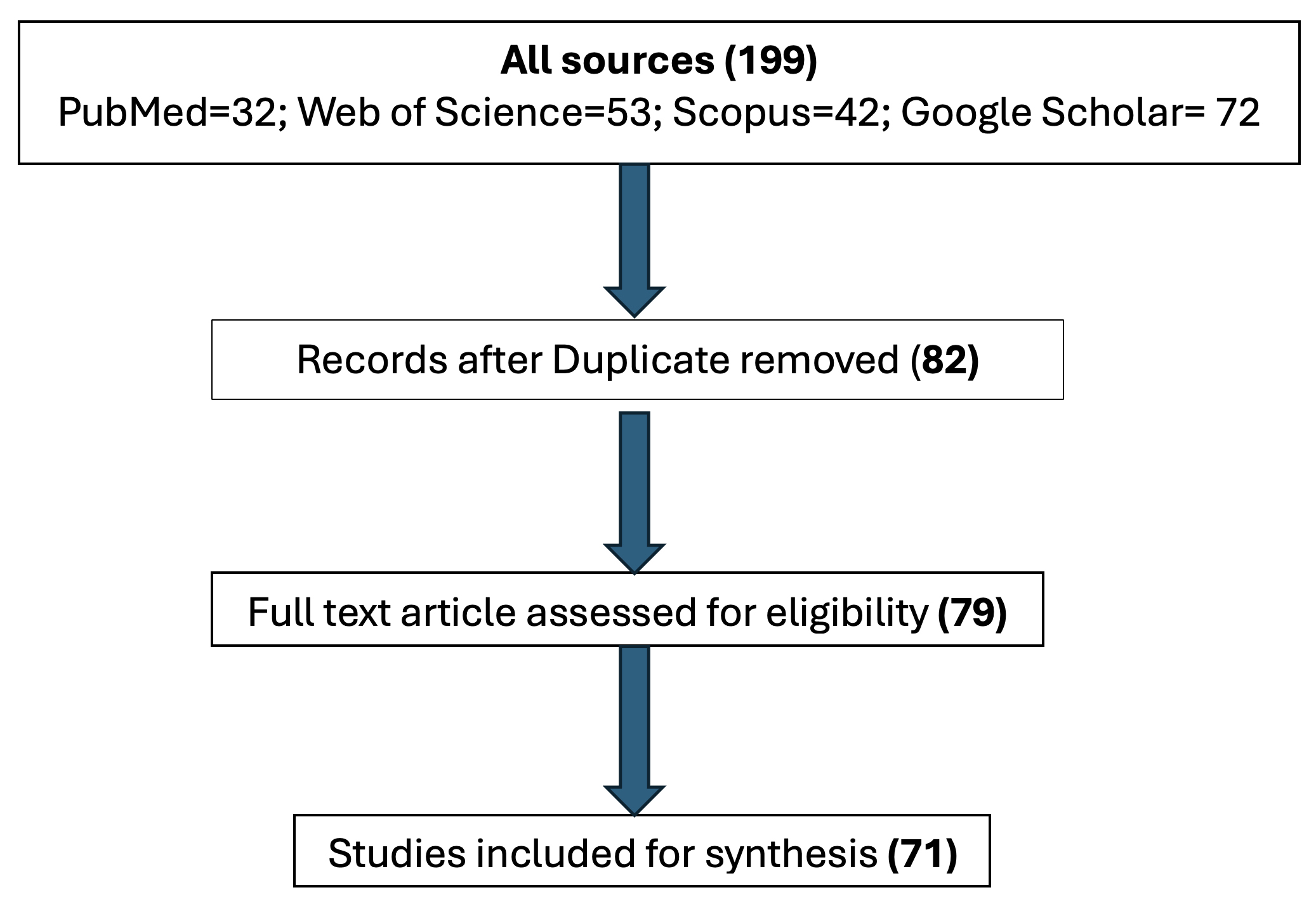 Fig. 1.
Fig. 1.
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram.
| Author(s)/Publication year/Affiliation | Study design/Sample size | Population characteristics | Study objective | Key finding | |
| 1. | Abdulaziz et al, 2009/Medicine/Riyadh | N = 205 | Residents of two TCCs | BO among Saudi residents in various subspecialties. | 70% of residents had BO. Emergency medicine residents had the highest, followed by medicine and OBGYN, while pediatricians had the least. |
| Male = 66% | |||||
| Female = 34% | |||||
| 2. | Agha et al, 2015/Emergency Medicine/Khamis Mushayt | N = 96 | Resident and Registrar of a TCC | BO among middle-grade doctors. | 88.5% of middle-grade doctors had BO syndrome. Unmarried, childless, and younger PHYs had higher depersonalization and job dissatisfaction. Nephrology and medicine were the most stressful. Housing, rotas, and transport caused the most stress. |
| Male = 67% | |||||
| Female = 33% | |||||
| 3. | Alfakeh et al, 2022/Psychiatry/Jeddah | N = 179 | Interns at a TCC | BO and depression among medical interns | 12.8% and 6.7% interns had mild and moderate depression, respectively. Most of them (19.6%) had moderate levels of anxiety and mild (6.1%) levels of stress, and 38% of participants had BO. Stress and BO were significantly positively correlated with an increase in committing medical errors, and so were the levels of BO with the levels of depression and anxiety. |
| Male = 44% | |||||
| Female = 56% | |||||
| 4. | Ali et al, 2021/Medicine/Jeddah | N = 270 | Interns at multiple public and private TCCs | prevalence of BO among interns | Half of the interns experienced high BO, primarily in personal and work-related domains. Patient-related BO was less common and linked to unethical behavior. |
| Male = 40% | |||||
| Female = 60% | |||||
| 5. | Alkhattabi et al, 2024/Pediatric/Riyadh | N = 386 | Resident and fellow at a TCC | BO among residents and fellowship trainees | 58.5% of trainees scored above the BO cut-off, with the highest score in the personal domain. BO was higher among married trainees, those with children, and seniors. Having children was a significant predictor of BO. |
| Male = 54% | |||||
| Female = 46% | |||||
| 6. | AlSayari, 2019/Surgery | N = 82 | Medical residents at a TCC | BO among Medical Residents | 41.9% experienced BO: 29% moderate, 12.9% severe. Females had twice the BO rate as males, mostly in the moderate category. BO increased from year 1 (33.3%) to year 3 (60%), but not significantly. |
| Male= 61% | |||||
| Female= 39% | |||||
| 7. | Alyamani et al, 2018/Medicine/Riyadh | N = 200 | Resident at a TCC | BO among Residents | Most work 51–70 hours weekly. 51% depersonalized, 31.5% low achievement, 12.5% emotionally exhausted. |
| Male = 60% | |||||
| Female = 40% | |||||
| 8. | ALYami et al, 2021/Community Medicine/Tabuk | N = 230 | Residents at a TCC | BO among Residents | 89.1% experienced BO, 32.2% high on all subscales. BO is linked to gender, chronic disease, training level, work-life balance dissatisfaction, work overload, and workplace stress sources. |
| Male = 61% | |||||
| Female = 39% | |||||
| 9. | Alzain et al, 2024/Public Health/Dammam | N = 177 | Residents of multiple disciplines of multiple TCCs in a city | Postgraduate trainee BO | 30.3% high EE, 24.9% high DP, and 86.3% low PA. BO varied by specialty and training, suggesting targeted interventions. |
| Male = 42% | |||||
| Female = 58% | |||||
| 10. | Ghazi et al, 2018/Family Medicine/Jeddah | N = 108 | Interns at multiple TCCs in a city | BO among medical interns | 16.7% of interns experienced BO. BO was higher among males (17.7%) than females (13.8%) and lower among those living in owned houses. BO was higher among those treated as students (27.3%) than as PHYs (11.3%), higher among those feeling overloaded (25.4%), and higher among those considering a career change (29%). |
| Male = 58% | |||||
| Female = 42% | |||||
| 11. | Hameed et al, 2018/Pediatric/Riyadh | N = 181 | Residents from two TCCs in two regions | Resident duty hours and BO | 50% of residents worked 60–79 hours, and 30% worked 80+ hours. BO prevalence was 81%. No association between work hours and BO. |
| Male = 41% | |||||
| Female = 59% | |||||
| 12. | Karim Alenezi et al, 2022/Preventive Medicine/Jeddah | N = 426 | Resident doctors at multiple TCCs in a city | BO among Saudi resident doctors | 81.22% had high BO, 18.31% high on all subscales. BO is linked to lack of exercise, training level, on-call shifts, weekend on-call, patient load, clinic frequency, work-life balance, and workplace stress. |
| Male = 54% | |||||
| Female = 46% |
BO, Burnout; EE, emotional exhaustion; PA, personal accomplishment; DP, depersonalization; OBGYN, Obstetrics and Gynecology; PHY, Physician; TCC, tertiary care center; N, number of samples.
Studies were mainly conducted in Riyadh and Jeddah, followed by other major cities (like Abha, Dammam, and Makkah), with most research focused on Family and General Medicine, followed by Emergency Medicine, Ear-Nose-Throat (ENT), and Community Medicine. Research peaked in 2019 and continues to be active. Earlier studies (before 2015) were smaller and more focused, while recent studies (2020–2024) covered broader populations. All studies used a cross-sectional design and validated tools, primarily the MBI. Sample sizes ranged from 29 to 520, with most studies including 150–200 participants. About 30% had fewer than 100 (specialists), half had 100–300 (broader groups like family medicine), and 20% included over 300 (multiple specialties or locations).
Most studies reported a higher proportion of male doctors, particularly in surgical and procedural specialties such as orthopedics, emergency medicine, and ENT, where 60–80% of practitioners were male. In contrast, female representation was higher in fields like pediatrics, psychiatry, and dermatology. Studies focusing on fellows generally had smaller sample sizes, whereas larger studies tended to examine broader groups, such as general physicians or primary care providers (Tables 1,2,3,4).
| Author(s)/Publication year/Affiliation | Study design/Sample size | Population characteristics | Study objective | Key finding | |
| 1. | Al-Ghamdi et al, 2021/Family Medicine/Abha | N = 133 | Family Medicine Residents of two cities | BO prevalence and predictors | 84% burned out. 29% EE, 20% DP, and 80% low PA. Men, married, anti-anxiety drugs linked to exhaustion. Long hours are linked to DP, young age, and low PA. |
| Male = 53% | |||||
| Female = 47% | |||||
| 2. | Aldrees et al, 2015/ENT/Riyadh | N = 85 | Otolaryngology residents across Saudi Arabia | Otolaryngology resident BO | Mean EE and DP were high (29.5, 10.7), and PA was low (32.33). No sex differences. Married residents had higher EE than single or divorced. |
| Male = 67% | |||||
| Female = 33% | |||||
| 3. | Aldrees et al, 2017/ENT/Riyadh | N = 38 | Residents of Plastic surgery at a TCC | Prevalence/factors associated with BO | 18% exhibited high BO, 71% had EE, and 50% had DP. The majority remained satisfied with the specialty. |
| Male = 74% | |||||
| Female = 26% | |||||
| 4. | Aldubai et al, 2019/Family Medicine/Madinah | N = 75 | Resident of Family Medicine at TCCs in a city | Prevalence and associated factors of BO | 32% of residents had BO linked to Shift work and the academic year. Examinations, workload, unfair assessments, work-life conflict, and lack of support were significant predictors of BO. |
| Male = 46% | |||||
| Female = 54% | |||||
| 5. | Alfaleh, 2017/Family Medicine/Riyadh | N = 130 | Residents’ Family and Internal Medicine at a TCC | Prevalence of BO | Family residents exhibited high DP and PA scores, with 75% of family medicine participants and 20% of internal medicine participants experiencing high levels of DP BO. |
| Male = 58% | |||||
| Female = 42% | |||||
| 6. | Aljuhayman et al, 2021/Urology/Qassim | N = 215 | Resident in Urology across Saudi Arabia | Work-related BO in urology residents | Moderate level of personal and work-related BO. 12.6% felt tired, and 19.1% EE. 14% found the work emotionally exhausting, and 18.6% felt burnt out. |
| Male = 95% | |||||
| Female = 5% | |||||
| 7. | AlNahedh et al, 2023/Family Med/Riyadh | N = 213 | Resident in Family Medicine in TCCs of a city | Resident depression and BO in Family Medicine | Moderate to high levels of BO were prevalent. 10% reported severe depression. Gender is linked to BO and depression severity. |
| Male = 53% | |||||
| Female = 47% | |||||
| 8. | Alotaibi et al, 2019/Ophthalmology/Riyadh | N = 117 | Ophthalmology Resident across Saudi Arabia | BO in Ophthalmology Resident | 41% of residents burned out. More call days are linked to BO. Work/life balance and career choice influenced BO. Southern programs had higher BO rates. |
| Male = 54% | |||||
| Female = 46% | |||||
| 9. | AlQahtani et al, 2020/Surgery/Taif | N = 303 | Surgery residents across Saudi Arabia | BO among general surgery residents | 39.3% high DP, 29.7% high EE, and 61.4% low PA. 62% intended to pull out, 80% unwilling to complete, 59% intended another program, and 66% were unsatisfied. More working days, hours, and nights on call are linked to BO. |
| Male = 72% | |||||
| Female = 28% | |||||
| 10. | Alqahtani, 2021/Medicine/Abha | N = 94 | Neurology residents across Saudi Arabia | BO prevalence and related factors among Saudi neurologists | Long hours were stressful. Consultants and residents had high BO. Consultants were more emotionally exhausted and had lower PA, while residents were more depersonalized. |
| Male = 60% | |||||
| Female = 40% | |||||
| 11. | Alsheikh et al, 2019/Orthopedics/Jeddah | N = 301 | Orthopedic surgery residents of multiple TCCs in a city | BO syndrome among orthopedic residents | 56.3% had BO. 68.3% are dissatisfied with work-life balance. 21.8% wouldn’t choose ortho again, 43% wouldn’t choose medicine. |
| Male = 90% | |||||
| Female = 10% | |||||
| 12. | Basheikh, 2021/Medicine/Riyadh | N = 40 | Internal Medicine residency directors across Saudi Arabia | BO among Internal Medicine residency directors | 85% of program directors were stressed. 27.5% lacked administrative support, 30% had uncooperative colleagues, and 82.5% received no financial benefit. |
| 13. | Binsaeed et al, 2022/Preventive Medicine | N = 104 | Preventive medicine residents in a region. | BO among preventive medicine residents | Half of the residents had physical and EE, and 40% felt weak. BO was higher among younger residents. |
| Male = 75% | |||||
| Female = 25% | |||||
| 14. | Bu Bshait et al, 2024/Surgery/Hofuf | N = 258 | ER and surgery residents at multiple TCCs across KSA | BO among ER and surgery residents | 63% experienced BO, with high EE (55%) and DP (28%). Resilience varied. BO is linked to gender, marital status, children, specialty, experience, and postgraduate enrolment. |
| Male = 72% | |||||
| Female = 28% | |||||
| 15. | Dahmash et al, 2019/Medicine/Riyadh | N = 29 | Plastic surgery residents at a TCC | Emotional intelligence and BO in plastic surgery residents | 37.9% had high BO: 72.4% high EE, 41% high DP, and 41% low PA. EI negatively correlated with EE, and DP positively correlated with PA. Dissatisfaction with career, income. |
| Male = 55% | |||||
| Female = 45% | |||||
| 16. | Dahmash et al, 2020/Medicine/Riyadh | N = 108 | Radiology residents across Saudi Arabia. | BO in radiology residents | 24.1% high BO, 56.5% high EE, 31.5% high DP, and 64.8% low PA. Predictors: work/life balance, exercise. Married, dissatisfied with the appreciation linked to low PA. |
| Male = 54% | |||||
| Female = 46% | |||||
| 17. | Dahmash et al, 2020/Pediatric/Riyadh | N = 264 | Pediatric residents across Saudi Arabia | BO and risk factors in pediatric residents | 14% unsatisfactory work-life balance, and 62% satisfied with pediatrics. 15.9% high BO, 63.6% high EE, 27.7% high DP, and 48.5% low PA.BO is linked to on-call and low salary. |
| Male = 53% | |||||
| Female = 47% | |||||
| 18. | Jamjoom and Park, 2018/Pediatric/Jeddah | N = 50 | Pediatric residents at a TCC in a city | BO among Jeddah pediatric residents | 70%+ residents are severely burned out. 43% EE, 71.8% DP, and 40.6% low PA. |
| Male = 6% | |||||
| Female = 94% | |||||
| 19. | Jan FM and Jan MM, 2015/Pediatric/Jeddah | N = 60 | Pediatric residents at multiple TCCs in a city | BO among Jeddah pediatric residents | 82% had abnormal BO, 32% severe. Males had more severe BO than females. University hospitals and junior residents had more severe BO. |
| Male = 33% | |||||
| Female = 67% | |||||
| 20. | Shadid et al., 2022/Dermatology/Riyadh | N = 51 | Dermatology resident at multiple TCCs in a city | BO in dermatology residents | 7.8% had high BO. 41.2% had high EE, 45.1% had low PA, and 13.7% had high Depersonalisation, and career satisfaction and sleep hours linked to it. |
| Male = 33% | |||||
| Female = 67% | |||||
| 21. | Shadid et al, 2023/Dermatology/Riyadh | N = 70 | Dermatology resident at multiple TCCs in a city | BO in dermatology residents | 21.4% burned out. 47.1% were emotionally exhausted, 65.7% had low PA, and 24.3% were depersonalized. Men and work-life balance reduced exhaustion. More patients experienced increased exhaustion. More study hours and career satisfaction reduced low PA. Exercise and work-life balance reduced overall BO. |
| Male = 50% | |||||
| Female = 50% | |||||
| 22. | Sharaf et al, 2022/Otorhinolaryngology/Riyadh | N = 51 | ENT residents from multiple TCCs across Saudi Arabia | Emotion intelligence and BO in ENT residents | 17.6% high BO risk, 39.2% EE, 29.4% DP, and 43.1% low PA. Higher Emotional Intelligence scores are associated with lower EE and DP. |
| Male = 65% | |||||
| Female = 35% | |||||
| 23. | Almalky et al, 2024/Emergency Medicine/Riyadh | N = 133 | Emergency medicine residents of multiple TCCs across Saudi Arabia | BO among emergency medicine residents | 57.9% took sick leave, 74.9% took short meals, 41.4% exercised regularly, and 71.6% had sleep disturbances. BO is related to age, region, and marital status. |
| Male = 0% | |||||
| Female = 100% |
ENT, Ear-Nose-Throat.
| Author(s)/Publication year/Affiliation | Study design/Sample size | Population characteristics | Study objective | Key finding | |
| 1. | Bany Hamdan et al, 2019/Oncology/Riyadh | N = 55 | Doctors at a cancer care center | BO among the Saudi Cancer Center staff | 44% of PHYs had BO. |
| Male = 40% | |||||
| Female = 60% | |||||
| 2. | AlAteeq et al, 2023/Family Medicine/Riyadh | N = 86 | PHYs from TCCs of Emergency Departments from multiple tertiaries | Estimate BO among ICU PHYs and nurses | Fellows had the highest BO (100%), followed by senior registrars (80%) and training residents (73%). Consultants and service residents had lower rates (39% and 40%). Fellows had the highest DP. PHYs and nurses had similar BO. |
| 3. | Al-Haddad et al, 2020/Family Medicine/Ahsha | N = 226 | PHY of PHC in a region | Prevalence of BO and its risk factors among primary care PHYs | 47% exhausted, 50% depersonalized, and 60% low PA. 24% highly burned out. Exhaustion is highest in 35–45-year-old Saudi rotators. DP is highest in Saudi family PHY rotators. Low PA is highest in dissatisfied PHYs and rotators. |
| Male = 68% | |||||
| Female = 32% | |||||
| 4. | Al-Omari et al, 2020/Public Administration/Riyadh | N = 115 | Doctors of Private hospitals | Assess BO among Saudi and UAE healthcare providers | Nurses were most emotionally exhausted compared to PHYs, therapists, and others. |
| 5. | Alanazi et al, 2022/Family Medicine/Arar | N = 303 | PHYs at multiple healthcare centers in a city | Assess PHY BO and related factors | BO was up to 17.8%, and 23.4% planned to quit their job. |
| Male = 51% | |||||
| Female = 49% | |||||
| 6. | Aldrees et al, 2013/ENT/Riyadh | N = 348 | PHY at a TCC | level and factors associated with BO | 70% of residents and consultants experienced BO. Back pain, sleep deprivation, residency status, and negative work-life balance predicted BO. |
| Male = 72% | |||||
| Female = 28% | |||||
| 7. | Almostadi et al, 2019/Family Medicine/Jeddah | N = 183 | PHYs at PHC in a region. | Link of BO and sleep quality among PHYs | 37.2% of PHYs had high BO, 89.1% had DP, and 67.2% had EE. Sleep disturbance was a risk factor, as was the residency status, administrative tasks, limited resources, poor working relationships, and high patient loads. |
| Male = 69% | |||||
| Female = 31% | |||||
| 8. | AlHadi et al, 2022/Psychiatry/Riyadh | N = 198 | Psychiatrists across Saudi Arabia | Prevalence/help-seeking for depression, anxiety, and BO | 42.7% had BO, 21% had depression, and 19% had anxiety. Psychiatrists and social workers experienced higher BO. Psychiatrists were more likely to self-medicate. Most MHPs preferred disclosing mental illness to family and friends. |
| 9. | Alharbi et al, 2023/Medicine/Makkah | N = 520 | PHYs in a region | CF, BO, and compassion satisfaction among PHYs | F affected 18.5% of PHYs, particularly middle-aged/older PHYs, and was reduced by prayer/meditation. BO affected 15.6%, with lower rates in females, younger PHYs, preventive medicine, and consultant roles. CS affected 18%, higher in males, those with social activities, prayer/meditation, and family medicine practice; lower in primary care, and preventive medicine. |
| Male = 51% | |||||
| Female = 49% | |||||
| 10. | Almadani et al, 2023/Psychiatry/Riyadh | N = 441 | Doctors across Saudi Arabia | BO and CF Among Healthcare Workers | PHYs had higher BO. Higher age had higher compassion satisfaction, while those with more experience had lower satisfaction. Work support and job satisfaction were positively correlated with compassion satisfaction and negatively correlated with BO and secondary traumatic stress. |
| 11. | Almeneessier and Azer, 2023/Medicine/Riyadh | N = 126 | Doctors at multiple TCCs | BO and emotional intelligence (EI) among clinicians and faculty. | BO ranged from moderate to severe, while EI was slightly above average. Younger, non-Saudi physicians experienced more BO. Age is negatively linked with BO. Saudi physicians reported more EE and less DP. EI reduced BO. |
| Male = 52% | |||||
| Female = 48% | |||||
| 12. | Alshreem et al, 2022/Family Medicine/Qassim | N = 150 | PHYs of PHC in multiple cities | BO and its impact on PHC PHY | 21.3% had EE, 38% DP, and 27.3% low PA. Staff PHYs had high EE, and residents had high DP and low PA. Long years in practice, long hours, and ER shifts increased BO risk. High BO negatively impacted patient care. |
| Male = 47% | |||||
| Female = 53% | |||||
| 13. | Alyaemni, 2019/Hospital Administration/Riyadh | N = 48 | PHYs of multiple TCCs in a city | BO among healthcare workers. | One-third to one-half of PHYs and nurses had moderate BO. PHYs used adaptive coping less. Nationality increased PHY EE, and marital status increased perceived low PA. |
| 14. | Baghdadi et al, 2020/Community Medicine/Riyadh | N = 136 | PHYs of multiple TCCs in a city | PHY satisfaction, ethics, and BO. | No gender difference in job satisfaction. High BO among PHYs, especially those willing to change specialty. Dissatisfaction with salary is linked to lower ethics scores. Females are better at resolving ethical dilemmas. |
| Male = 69% | |||||
| Female = 31% | |||||
| 15. | Bany Hamdan et al, 2019/Onco/Riyadh | N = 55 | PHY at a cancer center | BO among cancer center staff. | PHYs had the highest BO (44%), followed by nurses (29%) and others (27%). |
| 16. | Bawakid et al, 2017/Public Health/Jeddah | N = 246 | PHY of PHC in a region. | PHY BO in primary care. | 25.2% had moderate-high BO, and 69.5% had EE. Patient pressure/violence, unorganized patient flow, more paperwork, and less cooperative colleagues predicted high EE. Patient pressure/violence predicted overall BO. |
| Male = 43% | |||||
| Female = 57% | |||||
| 17. | Jarrar et al, 2023/Medical Education/Khobar | N = 249 | Residents, Teaching, and primary care PHYs | BO’s, work conditions and perceived patient safety, adverse events. | Leadership support and PHY engagement reduced adverse events while workload increased them. BO mediated the relationship between leadership support, work engagement, workload, and adverse events. |
| Male = 56% | |||||
| Female = 44% | |||||
| 18. | Marzouki et al, 2019/Medicine/Jeddah | N = 77 | PHY of a TCC | BO and job satisfaction among Saudi doctors. | Having children, training time, and daily work hours predicted BO. BO rates were 35.1%–66.2% for different domains. |
| 19. | Mohamed et al, 2021/OBG/Riyadh | N = 147 | PHYs at a TCC | BO among Hospital PHYs | 14.2% had BO. Exercise, shift duty, workload, quality of life, and work/specialty satisfaction affected EE. Shift duty, workload, quality of life, and specialty affected DP. BO is prevalent. |
| Male = 78% | |||||
| Female = 22% | |||||
| 20. | Selaihem, 2013/Medicine/Riyadh | N = 144 | PHY multiple PHC in a city | BO among primary care doctors at a TCC | 53.5% EE, 38.9% DP, 28.5% PA, 2.78% high in all. 25% low in all. High BO is linked to low job satisfaction, job change intention, tobacco/psychotropic use, younger age, recent graduation, marriage, and board qualification. |
| Male = 61% | |||||
| Female = 39% | |||||
| 21. | Wajid, 2017/Pharmacy/Dammam | N = 140 | Doctors from multiple public TCCs in a city | BO among doctors. | Despite 90.5% viewing work positively, 46% experienced BO, and 46.3% lacked energy for leisure. Most tolerated pressure, managed workload, and disagreed with overtime disconnection/negative work talk. |
| Male = 62% | |||||
| Female = 38% |
CF, compassion fatigue; PHC, primary health care; UAE, United Arab Emirates.
| Author(s)/Publication year/Affiliation | Study design/Sample size | Population characteristics | Study objective | Key finding | |
| 1. | Al-Sareai et al, 2013/Family Medicine/Abha | N = 370 | PHC PHY in a region | BO prevalence/associated factors in primary care PHYs | 29% were EE, 16% DP, and 20% had low PA. Younger, low-income Saudis were more EE. Longer vacations reduced exhaustion. Older, high-income Saudis were more PD. Younger, non-Saudi, and longer-vacationers had lower PAs. |
| Male = 82% | |||||
| Female = 18% | |||||
| 2. | Al-Youbi and Jan, 2013/Pediatric/Jeddah | N = 130 | Pediatricians in a region | Evaluate BO in pediatricians | 82% of participants experienced BO, with 34% experiencing severe BO. Male academic pediatricians/consultants were more likely to experience severe BO. |
| Male = 45% | |||||
| Female = 55% | |||||
| 3. | Alghamdi, 2014/Anasthesis/Riyadh | N = 152 | Anaesthesiologist of Multiple TCC | Prevalence of BO among anaesthesiologists’ | Anesthetists reported high rates of depression (45%), stress (35.1%), anxiety (51%), and BO (64.9%). |
| Male = 78% | |||||
| Female = 22% | |||||
| 4. | Almalky et al, 2024/Emergency Medicine/Riyadh | N = 430 | Emergency Medicine PHY Across Saudi Arabia | BO in emergency medicine PHY | 57.9% of residents took sick leave, 74.9% had short meals, and 41.4% exercised regularly. 71.6% experienced sleep disturbances. BO was associated with age, region, and marital status. Gender, nationality, emergency healthcare provider status, and residency duration were not significant factors. |
| Male = 58% | |||||
| Female = 42% | |||||
| 5. | Alqahtani et al, 2019/Family Medicine/Abha | N = 187 | PHYs of Emergency Medicine at multiple TCCs | BO among emergency PHYs | Nurses had higher EE and lower PA than PHYs. Half of those with 4 weeks’ vacation had low PA, compared to 20% with 5 weeks. |
| Male = 29% | |||||
| Female = 71% | |||||
| 6. | Alqhtany et al, 2023/Medicine/Makkah | N = 57 | Forensic medicine PHYs of multiple TCCs across Saudi Arabia | BO syndrome among forensic PHYs | 56.1% experienced high BO, 26.3% medium, and 17.5% low. Increased caseload and work hours predicted high BO. Vacation was the preferred coping strategy. |
| Male = 65% | |||||
| Female = 35% | |||||
| 7. | Alsaawi et al, 2014/Emergency Medicine/Riyadh | N = 53 | Emergency PHYs at a TCC | BO among emergency PHYs | There was a moderate to high level of EE and DP, as well as low to moderate feelings of PA. |
| Male = 85% | |||||
| Female = 15% | |||||
| 8. | Alsaawi et al, 2019/Emergency Medicine/Riyadh | N = 265 | Emergency PHYs across Saudi Arabia | BO among Emergency PHYs | 56.3% were high-risk. BO was not linked to gender, age, job, or experience, but older participants had lower Depersonalisation scores. |
| Male = 74% | |||||
| Female = 26% | |||||
| 9. | Alshahrani et al, 2022/Hospital Administration/Dammam | N = 67 | Emergency PHYs at multiple TCCs in a city | BO among Emergency PHYs | 76% of PHYs had BO, and there was no significant difference between them and nurses. |
| 10. | Babiker et al, 2021/Occupational PHY/Jubail | N = 51 | PHY at a TCC | BO among family PHYs | Overall, there was severe EE and moderate DP. 29.4% high in all three. High EE is linked to bachelor’s degree, family medicine, patient load, years of practice, and job dissatisfaction. High DP is linked to dental specialty, patient load, and job dissatisfaction. High PA is linked to short practice, salary dissatisfaction, job dissatisfaction, and non-clinical tasks. |
| 11. | Ghazwani, 2022/Family Medicine/Najran | N = 44 | Palliative care clinicians across Saudi Arabia. | BO among palliative care clinicians | 18.2% EE, 25% DP/detachment. Job title, admin support, and pain relief meds impact BO. No significant difference based on other PHY characteristics. |
| Male = 59% | |||||
| Female = 41% | |||||
| 12. | Khalaf et al, 2023/Ophthalmology/Riyadh | N = 160 | Ophthalmologists in multiple tertiary care settings in a city | Mental health of ophthalmologists | 40% no depression, 17.5% mild, 23.8% moderate, and 18.8% severe depression. 31.9% no anxiety, 10.6% mild, 21.9% moderate, and 35.6% severe anxiety. 15% mild, 14.4% moderate, and 10% severe stress. 43.8% low DP, 17.5% moderate, 38.8% high. 32.5% BO, 67.5% no BO. BO is higher among 6–10-year ophthalmologists. On-call duty had no significant impact. |
| Male = 56% | |||||
| Female = 44% | |||||
| 13. | Rahimaldeen et al, 2021/Public Health/Makkah | N = 251 | Pediatricians from multiple public and private TCCs in a region | BO, mental health, and care quality in pediatricians | Pediatricians had high BO (80.5%), depression (66.5%), anxiety (71.3%), and stress (55%). 21.6%, 41.1%, and 16.7% had severe/extremely severe depression, anxiety, or stress. Females, juniors, and younger doctors had higher levels. 45.8%–48.6% believed adverse conditions led to lost workdays and reduced quality. |
| Male = 71% | |||||
| Female = 29% | |||||
| 14. | Sadat-Ali et al, 2005/Orthopedic/Khobar | N = 69 | Orthopedic surgeons of multiple TCC | BO among orthopedic surgeons | 50.7% emotionally exhausted, 59.4% depersonalized, and 17% low PA. Government doctors fared better than private-sector doctors. |
| Male = 71% | |||||
| Female = 39% | |||||
| 15. | Shaher Al-Otaibi et al, 2020/Surgery/Abha | N = 107 | Orthopedic surgeons of multiple TCCs in a region | BO among orthopedic surgeons | Surgeons had 35.1% EE, 30.7% DP, and 39.6% PA. |
| Male = 94% | |||||
| Female = 6% |
Burnout prevalence among doctors in Saudi Arabia ranged from 17.6% to 100%, varying by specialty, career stage, and setting (Tables 1,2,3,4). The highest prevalence was observed in ICU (80–100%) (AlAteeq et al, 2023), Emergency Medicine (88.5%) (Alshahrani et al, 2022), and Pediatrics (82%) (Al-Youbi and Jan, 2013; Jamjoom and Park, 2018). Moderate prevalence rates were reported in Orthopedics (56.3%) (Sadat-Ali et al, 2005), Psychiatry (42.7%) (AlHadi et al, 2022), Plastic Surgery (37.9%) (Dahmash et al, 2019), Ophthalmology (32%) (Alotaibi et al, 2019), and Radiology (24.1%) (Dahmash et al, 2020). Lower prevalence was found in Dermatology (21.4%) (Shadid et al, 2023) and ENT (17.6%) (Sharaf et al, 2022) (Tables 1,2,3,4).
Residents showed high emotional exhaustion (EE; 54%–75.5%) and depersonalization (DP; 35%–41.2%) due to training demands and on-call shifts (Alsaawi et al, 2019). Consultants, showed lower burnout rates (17.6%–68.8%), with experience reducing EE but not low personal accomplishment (PA), particularly among senior consultants (Aldrees et al, 2013). Junior doctors faced stressors like lack of mentorship and unclear career pathways, exacerbating burnout (Dahmash et al, 2020).
Work environment factors, including workload, resource availability, and
workplace support, significantly influence burnout. High patient loads (
Individual factors like gender, age, and marital status were associated with
burnout. Female physicians showed higher EE and DP compared to males, due to
societal expectations and work-life conflict (Alghamdi, 2014; Bahmaid et al, 2023). Younger physicians (
Organizational factors, including leadership style, administrative burden, and reward systems, influence burnout. Lack of empathetic leadership and inadequate recognition were linked to higher burnout, particularly in high-stress specialties (Jarrar et al, 2023). Administrative tasks like documentation and scheduling contributed to EE, with physicians spending up to 20% of time on non-clinical work (e.g., Al-Youbi and Jan, 2013). Organizations offering career advancement and financial incentives reported lower burnout rates (Bawakid et al, 2017). The absence of wellness programs was noted as a gap (e.g., Alamri et al, 2023).
Cultural and personal factors in the Saudi context influence burnout. Societal expectations, including emphasis on physicians’ self-sacrifice, increased EE and DP (e.g., Alwhaibi et al, 2022). Mental health stigma prevented doctors from seeking support, worsening burnout (e.g., Dahmash et al, 2020). Personal resilience and coping mechanisms like mindfulness and peer support were protective but underutilized (e.g., AlAteeq et al, 2023). Work-life imbalance, especially among female physicians with family duties, contributed to burnout (e.g., Alghamdi, 2014).
Burnout among doctors in Saudi Arabia has become a growing concern over the past decade, significantly influenced by career stage, specialty, and work environment. Most studies on this issue have been conducted in urban centers. This scoping review highlights substantial variation in burnout prevalence, ranging from 17.6% to 100%, which aligns with previous reports (Ziena, 2022). The findings emphasize the complex interplay between individual factors, such as resilience, and systemic factors, including workload, resource availability, and cultural expectations (Rotenstein et al, 2018).
High-prevalence specialties such as ICU, Emergency Medicine, and Pediatrics face intense care demands, leading to high levels of emotional exhaustion. In contrast, moderate-prevalence specialties like Plastic Surgery and Radiology experience stress related to repetitive tasks and high patient expectations despite operating in more structured environments. Lower-prevalence specialties, including ENT and Dermatology, generally have fewer emergencies, more predictable schedules, and better work-life balance. Additionally, younger, early-career doctors tend to have higher burnout due to increased responsibilities and long working hours (Peisah et al, 2009).
Several factors contribute to burnout among physicians. Early-career physicians are more susceptible to emotional exhaustion and depersonalization due to their inexperience, career uncertainty, and underdeveloped coping skills. In contrast, older, high-income Saudi physicians may experience higher levels of depersonalization as a long-term response to sustained job-related stress. Female doctors are more prone to experience emotional exhaustion, possibly due to work pressures of balancing work and family responsibilities (Lyubarova et al, 2023), whereas male doctors may be more prone to depersonalization using depersonalization as a coping mechanism (Hoff and Lee, 2021; Lyubarova et al, 2023). Family life also plays an important role in burnout, with married doctors and parents facing higher burnout levels due to competing personal and professional demands. Unmarried doctors potentially experience lower personal accomplishment, potentially due to weaker social support systems (Hoff and Lee, 2021; Lyubarova et al, 2023).
The demanding nature of medicine, particularly in high-workload, irregular-hour, high-stakes specialties, is a significant contributor to burnout. Many residents report working 60–79 hours per week, with some exceeding 80 hours, leading to physical and mental exhaustion (Rodrigues et al, 2018). On-call shifts, weekend duties, and the pressures of acute care settings, such as ERs and ICUs, increase stress due to the need for constant vigilance and rapid decision-making (Zhang et al, 2020). Internal medicine physicians face additional stressors such as limited administrative support, unfair assessments, and workplace politics (Abid and Salzman, 2021). The continuous shift between diverse medical challenges in specialties like internal medicine requires high adaptability and focus, further increasing burnout risk (Gopal et al, 2005).
Psychosocial and cultural factors further exacerbate burnout (Walsh, 2013). Work-life imbalance is a major contributor to stress, particularly for radiology residents and those working long, irregular hours, as it negatively affects personal recovery. The emotional demands of patient care, particularly in pediatrics, can be deeply draining. Cultural and societal expectations place additional pressure on female doctors, who often struggle to balance family and career responsibilities (Rao and Shailashri, 2021). Younger non-Saudi doctors experience higher burnout levels due to challenges related to cultural adjustment, limited support systems, and potential workplace discrimination (Peisah et al, 2009). Additionally, poor leadership and weak team dynamics have been identified as key drivers of burnout among family physicians (Abid and Salzman, 2021).
Burnout is a multifaceted condition characterized by the complex interplay of emotional exhaustion, depersonalization, and low personal accomplishment, influenced by patient care intensity, career stage, and sociocultural factors. Emotional exhaustion is the most prevalent dimension, particularly in high-intensity specialties, where cultural emphasis on altruism may further intensify its effects.
Depersonalization, often a potential coping mechanism, is more common among younger, unmarried doctors working in high-pressure environments such as the ICU and pediatrics. This is likely due to their limited experience, fewer coping strategies, and demanding workloads (Peisah et al, 2009). In contrast, consultants tend to experience less depersonalization, benefiting from greater autonomy and experience.
Low personal accomplishment is a major concern for younger doctors and those working in resource-limited settings (Gluschkoff et al, 2022). This may be exacerbated by a lack of recognition, and, in certain specialties such as radiology, less direct patient interaction (Gluschkoff et al, 2022). These dimensions often reinforce each other (Taris et al, 2005).
Several coping mechanisms and protective factors can help mitigate burnout. Emotional intelligence (EI) plays a key role in managing emotional demands, reducing both exhaustion and detachment (Kumar, 2016). Regular exercise enhances overall well-being, while wellness practices such as mindfulness and spiritual activities enhance resilience (Clough et al, 2017).
Institutional support, including collaborative workplaces with strong teamwork and empathetic leadership, enhances job satisfaction (Abid and Salzman, 2021). Flexible schedules, extended vacations, and mentorship programs provide essential recovery and support (Kumar, 2016). Additionally, adequate resource allocation, proper staffing, and a reduction in administrative burdens help alleviate stress (Kumar, 2016). Public recognition also serves as a motivator, reinforcing professional commitment and engagement.
Burnout among physicians in Saudi Arabia has emerged as an increasing concern over the past decade, influenced by factors such as career stage, specialty, and work environment. The majority of studies on this issue have been conducted in urban centers. This scoping review highlights the variation in burnout prevalence, ranging from 17.6% to 100%, consistent with previous reports. The findings underscore the interaction between individual factors, such as resilience, and systemic factors, including workload, resources, and cultural expectations. Addressing burnout aligns with the objectives of Saudi Vision 2030 to cultivate a vibrant society, a thriving economy, and an ambitious nation. Through targeted interventions such as workload management and mental health support, healthcare systems can enhance physician well-being, contributing to a society where professionals flourish. Improved physician well-being leads to enhanced patient care, reduces medical errors, and improves healthcare outcomes, thereby supporting economic growth by increasing workforce productivity and reducing costs associated with physician turnover. Furthermore, addressing burnout fosters an ambitious nation by developing a sustainable healthcare workforce capable of meeting the demands of a growing population, in alignment with Vision 2030’s goal of a resilient healthcare system. These efforts ensure that physicians can deliver optimal care, reinforcing the commitment to health and societal progress.
The primary limitation of this review is that the majority of studies were
conducted as cross-sectional surveys, predominantly lacking a control group, and
capturing data at a single point in time, which does not reflect longitudinal
progress. Most of the primary studies reported 95% CIs, resulting in greater
uncertainty in smaller studies (n
In summary, burnout in Saudi doctors varies by career stage, specialty, and environment. Early-career physicians in high-stress specialties face increased vulnerability due to demanding transitions, long hours, and limited support (Chemali et al, 2019). While senior physicians experience burnout, their experience often mitigates its impact (Peisah et al, 2009). Specialty-specific stressors exist: Emergency and ICU doctors contend with emotional strain and sleep disturbances, while primary care and pediatrics face resource and financial pressures. Surgeons struggle with work-life balance (Zhang et al, 2020). Urban-rural disparities also influence burnout (Bethea et al, 2020). Ultimately, workload-resource imbalances compromise patient care, workforce sustainability, and healthcare costs (Alfakeh et al, 2022).
In conclusion, burnout is a significant issue among Saudi doctors, particularly in high-stress specialties, arising from systemic pressures, cultural factors, and individual challenges. Burnout has serious consequences for healthcare, contributing to increased medical errors, reduced quality of patient care, and workforce attrition. Prioritizing physician well-being through evidence-based and culturally sensitive solutions is crucial for building a resilient healthcare system in alignment with Saudi Vision 2030. Based on the findings of this review and supported by existing literature, we propose the following recommendations:
(1) Workload management through flexible scheduling, time off, and team-based care to reduce the impact of long hours and on-call duties (Al-Ghamdi et al, 2021; Hameed et al, 2018).
(2) Enhanced emotional support via peer networks, accessible counseling, and destigmatizing mental health, as emotional exhaustion was prevalent in high-intensity specialties (AlAteeq et al, 2023; AlHadi et al, 2022).
(3) Professional development and mentorship with structured guidance, clear career pathways, and recognition to address low personal accomplishment, particularly among younger doctors (Dahmash et al, 2020; Kumar, 2016).
(4) Streamlined administrative support using digital solutions and AI-driven tools to optimize staff scheduling, operating room scheduling, and documentation, reducing administrative burdens (Bhuyan et al, 2025; Misurac et al, 2025; West et al, 2018).
(5) Improved work-life balance through wellness practices, flexible work schedules, and telehealth (Clough et al, 2017; Shadid et al, 2023).
(6) Optimized resource allocation with better staffing in high-risk specialties and access to necessary resources (Abid and Salzman, 2021; Bawakid et al, 2017).
(7) Empathetic leadership that fosters recognition and rewards, as leadership support was found to reduce burnout and adverse events (Gopal et al, 2005; Jarrar et al, 2023).
All data generated or analysed during this study are included in this published article.
MA and DR had equal contribution in Conceptualization, Investigation, Writing—Original Draft, Writing—Review and Editing. Supervision, MA. Both authors read and approved the final manuscript. Both authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
Not applicable.
We would like to thank the deanship of scientific research at Shaqra University for supporting this work.
This research received no external funding.
The authors declare no conflict of interest.
During the preparation of this work, the authors used Grammarly in order to check spelling and grammar. After using this tool, the authors reviewed and edited the content as needed and take full responsibility for the content of the publication.
Supplementary material associated with this article can be found, in the online version, at https://doi.org/10.31083/BP42895.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.