



 , Shi Wu 1, Feng Ying 1, Long Li 1
, Shi Wu 1, Feng Ying 1, Long Li 11 Department of Colorectal Surgery, The First People’s Hospital of Yongkang, 321300 Yongkang, Zhejiang, China
Abstract
Although laparoscopic surgery for colon cancer offers advantages over open surgery, such as minimal invasion and faster recovery, the transverse colon presents unique challenges due to its special anatomical location and complex vascular and lymphatic drainage. This study aimed to identify independent risk factors and to develop a corresponding combined predictor for perioperative complications following laparoscopic radical resection of transverse colon cancer.
Retrospective clinical data from 170 patients with transverse colon cancer who underwent laparoscopic colectomy at The First People’s Hospital of Yongkang between January 2020 and July 2025 were analyzed. According to the Clavien–Dindo classification system, patients were divided into a complication group (Clavien–Dindo grade ≥I) and a non-complication group. Baseline demographics, surgical variables, and occurrence of perioperative complications were collected. Univariate and multivariate logistic regression analyses were performed to identify independent risk factors for complications. The combination of these independent risk factors was then assessed as a composite predictor. Its predictive performance was evaluated using receiver operating characteristic (ROC) curve analysis.
Among the cohort, 43 patients experienced complications (complication group) while 127 did not (non-complication group). Univariate logistic regression analysis revealed that age, presence or absence of comorbid diabetes mellitus, type of abdominal anastomosis, and operation time were associated with perioperative complications following laparoscopic colectomy for transverse colon cancer (p < 0.05). Multivariate logistic regression analysis revealed that comorbid diabetes mellitus (odds ratio [OR] = 4.656, 95% confidence interval [CI]: 1.715–12.640, p = 0.003), extracorporeal anastomosis (OR = 5.943, 95% CI: 2.497–14.142, p < 0.001), and an operation time exceeding 3 hours (OR = 4.520, 95% CI: 1.929–10.595, p < 0.001) were independent risk factors for perioperative complications. The area under the ROC curve (AUC) for the predictor combining these three factors was 0.825 (95% CI: 0.752–0.897, p < 0.001), demonstrating superior predictive efficacy compared to any single factor alone.
Comorbid diabetes mellitus, extracorporeal anastomosis, and operation time >3 hours are independent risk factors for perioperative complications in patients undergoing laparoscopic resection of transverse colon cancer. The combination of these three risk factors shows good predictive value and holds promise for guiding targeted clinical interventions to improve patient outcomes.
Keywords
- colonic neoplasms
- laparoscopy
- postoperative complications
- risk factors
- logistic models
Colonic cancer, a malignant tumor originating in the colon, ranks as the third most common cancer globally and has become the second leading cause of cancer-related deaths worldwide, constituting a major public health burden [1]. For non-metastatic colon cancer, surgical resection remains the cornerstone of curative treatment [2]. Currently, laparoscopic colectomy is well-established, offering significant advantages over open surgery, including reduced intraoperative blood loss, faster recovery of bowel function, shorter hospital stays, comparable oncologic safety, and a decreased incidence of severe complications [3, 4, 5]. Nevertheless, according to several studies, the overall complication rate remains considerable, ranging from 20% to 30% [6, 7, 8]. Therefore, further efforts to reduce postoperative complications remain an area of research focus [9].
The transverse colon presents unique anatomical challenges due to its mid-abdominal location, where it is suspended between the hepatic and splenic flexures, as well as its complex vascular and lymphatic anatomy [10]. Laparoscopic resection of transverse colon cancer often requires specialized technical maneuvers, such as complete dissection of the middle colic vessels and mobilization of both colonic flexures. These procedures may result in distinct complication profiles compared to other colonic segments [11]. Consequently, risk factors established from studies on other colon segments may not apply to patients undergoing dedicated laparoscopic resection of transverse colon cancer.
This study aims to specifically analyze the risk of complications arising in patients with transverse colon cancer receiving laparoscopic transverse colectomy. The selection of candidate risk factors was based on a targeted review of contemporary literature on complications associated with laparoscopic colorectal surgery, with particular attention paid to pathophysiological mechanisms related to the technical characteristics of transverse colon surgery. Specifically, the analysis was structured across three dimensions: First, patient-related factors included diabetes mellitus and high body mass index (BMI), both well-established systemic risk factors associated with surgical site infections and impaired wound healing [12]. Second, technique-related factors were considered, particularly the frequent usage of extracorporeal anastomosis in transverse colon due to its mid-abdominal location. Although commonly employed, this approach may lead to greater incision exposure and mesenteric traction, and is therefore hypothesized to carry a higher risk of complications [13]. Third, surgery-related factors were evaluated, with operation time serving as an integrated indicator of procedural complexity. Transverse colon surgery is inherently more complex owing to the need to address both flexures and the middle colic vessels [14]. Additionally, age, preoperative anemia, among others, were also included due to their consistent associations with major abdominal surgery complications [15, 16]. This multidimensional screening approach was designed to comprehensively evaluate the unique risk profile of laparoscopic transverse colectomy.
The primary objective of this retrospective clinical study is to identify independent risk factors of perioperative complications among patients undergoing laparoscopic colectomy for transverse colon cancer. Our findings hold potential to be translated into a valuable preoperative risk assessment tool for facilitating personalized patient counseling and guiding targeted preventive strategies, with an ultimate goal of improving patient outcomes.
This study retrospectively included 170 patients with primary transverse colon cancer who underwent laparoscopic colectomy at The First People’s Hospital of Yongkang between January 2020 and July 2025. The study was approved by the Ethics Review Committee of The First People’s Hospital of Yongkang (approval number: 2025-LW-035) and conducted in adherence to the Declaration of Helsinki. Informed consent was obtained from all included patients.
The inclusion criteria of this study were as follows: (1) patients with histologically confirmed primary adenocarcinoma of the transverse colon based on postoperative pathology, with tumor location anatomically defined as within the transverse mesocolon, situated between the hepatic flexure and splenic flexure [International Statistical Classification of Diseases and Related Health Problems, 10th Revision (ICD-10) Code: C18.4)]; (2) patients who underwent elective laparoscopic-assisted or totally laparoscopic colectomy (including extended right hemicolectomy, transverse colectomy, or left hemicolectomy) with achievement of radical (R0) resection of the primary tumor; and (3) patients with complete medical records allowing for retrospective extraction of all predefined study variables related to demographics, surgical procedures, and perioperative outcomes.
The exclusion criteria were as follows: (1) patients who underwent emergent surgery due to acute conditions such as obstruction, perforation, or hemorrhage, or those with a preoperative assessment indicating palliative resection due to confirmed unresectable distant metastases; (2) patients with recurrent transverse colon cancer; (3) patients who had received any form of neoadjuvant chemotherapy or targeted therapy prior to surgery; (4) patients with a history of major abdominal surgery; (5) patients with concurrent intra-abdominal malignancy requiring synchronous resection, or with non-adenocarcinoma histology (e.g., lymphoma, gastrointestinal stromal tumor, neuroendocrine neoplasm); (6) patients requiring multivisceral resection required due to tumor invasion of other organs (e.g., partial hepatectomy, distal pancreatectomy, partial gastrectomy); and (7) cases that were converted to open surgery for any reason.
The flowchart for subject screening based on the inclusion and exclusion criteria is shown in Fig. 1.
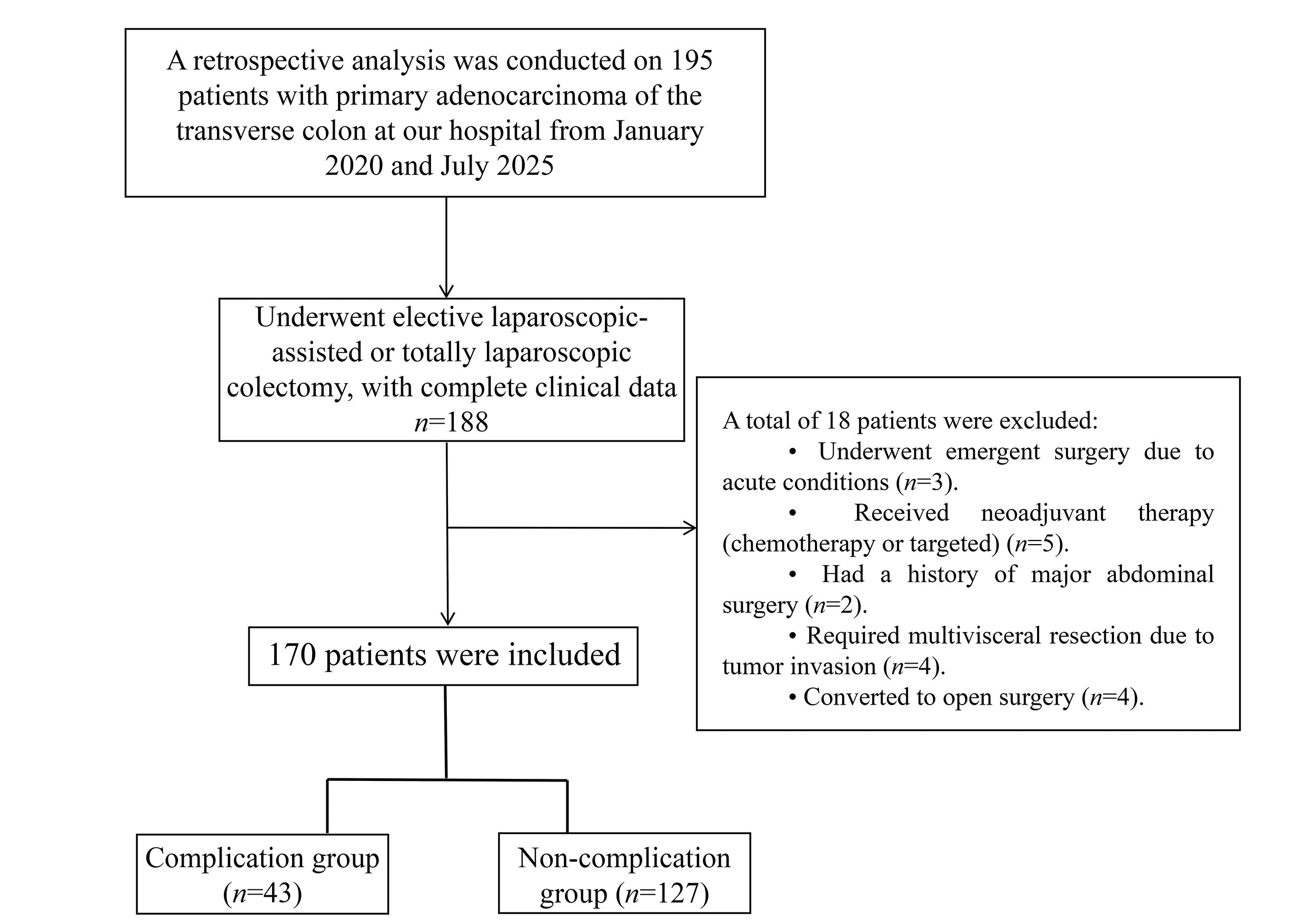 Fig. 1.
Fig. 1.
Flowchart depicting patient selection in this study.
The variables collected were selected based on their confirmed or hypothesized associations with postoperative complications of laparoscopic colorectal surgery. Data, including sex, age, body mass index (BMI), smoking status, alcohol consumption status, presence or absence of diabetes mellitus, hypertension, cardiovascular disease, preoperative serum albumin level, preoperative anemia status, tumor node metastasis (TNM) stage, tumor differentiation grade, American Society of Anesthesiologists (ASA) physical status classification, operation time, and type of abdominal anastomosis, were extracted from electronic medical records.
Perioperative complications were monitored across all patients. All adverse
events occurring within 30 perioperative days were recorded and graded according
to the Clavien–Dindo classification system [17]. Commonly observed complications
included, but were not limited to, ileus, anastomotic leakage, and surgical site
infection. The Clavien–Dindo grading criteria were as follows: (1) Grade I: No
life-threatening complications requiring only supportive care (e.g., antiemetics,
antipyretics, analgesics, electrolyte replacement therapy, or physical measures);
(2) Grade II: Requiring management beyond Grade I medications, such as blood
transfusion or parenteral nutrition; (3) Grade IIIa: Requiring intervention
without general anesthesia (e.g., radiological/endoscopic procedures); (4) Grade
IIIb: Requiring intervention under general anesthesia (e.g., surgery and interventional radiology); (5) Grade IV: Presented with
life-threatening complications demanding intensive care unit (ICU) admission; and (6) Grade V: Death of the patient. In
this study, only patients classified as Clavien–Dindo grade
All statistical analyses in this study were performed using SPSS version 25.0 software (IBM Corporation, Armonk, NY, USA). For ease of clinical interpretation and consistency with prior studies, some continuous variables were dichotomized using clinically relevant cutoff values (Table 1). All categorical variables were expressed as frequencies with percentages [n (%)], with intergroup comparisons performed using the chi-square test. Key continuous variables were dichotomized using widely accepted clinical thresholds to identify applicable predictors: BMI at 24.0 kg/m2 [18], age at 60 years [19], preoperative serum albumin at 35.0 g/L [20], and operation time at 180 minutes [21].
| Variable | Assignment |
| Sex | Female = 0; Male = 1 |
| Age | |
| BMI | |
| Smoking | No = 0; Yes = 1 |
| Drinking | No = 0; Yes = 1 |
| ASA physical status classification | Stage I–II = 0; Stage III–IV = 1 |
| Comorbid diabetes mellitus | No = 0; Yes = 1 |
| Comorbid hypertension | No = 0; Yes = 1 |
| Comorbid cardiovascular disease | No = 0; Yes = 1 |
| Preoperative serum albumin level | |
| Preoperative anemia status | No = 0; Yes = 1 |
| TNM stage | Stage I–II = 0; Stage III–IV = 1 |
| Tumor differentiation grade | High/Intermediate grade = 0; Low grade = 1 |
| Abdominal anastomosis method | Intracorporeal anastomosis = 0; Extracorporeal anastomosis = 1 |
| Operation time |
Abbreviations: ASA, American Society of Anesthesiologists; BMI, body mass index; TNM, tumor node metastasis.
Univariate logistic regression analysis was initially conducted to identify
factors associated with the occurrence of complications. A p-value threshold of
This study included a total of 170 patients, comprising 43 cases in the
complication group and 127 cases in the non-complication group. There were
significant differences between the two groups in age, diabetes mellitus
comorbidity, type of abdominal anastomosis, and operation time (p
| Factor | Complication group (n = 43) | Non-complication group (n = 127) | p | ||
| Sex | 0.189 | 0.664 | |||
| Female | 29 (67.44) | 81 (63.78) | |||
| Male | 14 (32.56) | 46 (36.22) | |||
| Age (years) | 6.627 | 0.010 | |||
| 16 (37.21) | 76 (59.84) | ||||
| 27 (62.79) | 51 (40.16) | ||||
| BMI (kg/m2) | 0.722 | 0.396 | |||
| 25 (58.14) | 83 (65.35) | ||||
| 18 (41.86) | 44 (34.65) | ||||
| Smoking | 0.635 | 0.426 | |||
| No | 29 (67.44) | 77 (60.63) | |||
| Yes | 14 (32.56) | 50 (39.37) | |||
| Drinking | 0.654 | 0.419 | |||
| No | 28 (65.12) | 91 (71.65) | |||
| Yes | 15 (34.88) | 36 (28.35) | |||
| ASA physical status classification | 0.281 | 0.596 | |||
| Stage I–II | 13 (30.23) | 44 (34.65) | |||
| Stage III–IV | 30 (69.77) | 83 (65.35) | |||
| Comorbid diabetes mellitus | 19.596 | ||||
| No | 27 (62.79) | 116 (91.34) | |||
| Yes | 16 (37.21) | 11 (8.66) | |||
| Comorbid hypertension | 0.139 | 0.710 | |||
| No | 24 (55.81) | 75 (59.06) | |||
| Yes | 19 (44.19) | 52 (40.94) | |||
| Comorbid cardiovascular disease | 0.224 | 0.636 | |||
| No | 25 (58.14) | 79 (62.20) | |||
| Yes | 18 (41.86) | 48 (37.80) | |||
| Preoperative serum albumin level (g/L) | 0.397 | 0.528 | |||
| 21 (48.84) | 55 (43.31) | ||||
| 22 (51.16) | 72 (56.69) | ||||
| Preoperative anemia | 0.435 | 0.509 | |||
| No | 25 (58.14) | 81 (63.78) | |||
| Yes | 18 (41.86) | 46 (36.22) | |||
| TNM stage | 0.501 | 0.479 | |||
| Stage I–II | 23 (53.49) | 60 (47.24) | |||
| Stage III–IV | 20 (46.51) | 67 (52.76) | |||
| Tumor differentiation grade | 0.680 | 0.410 | |||
| High/Intermediate grade | 11 (25.58) | 41 (32.28) | |||
| Low grade | 32 (74.42) | 86 (67.72) | |||
| Abdominal anastomosis method | 20.323 | ||||
| Intracorporeal anastomosis | 13 (30.23) | 88 (69.29) | |||
| Extracorporeal anastomosis | 30 (69.77) | 39 (30.71) | |||
| Operation time (h) | 15.502 | ||||
| 16 (37.21) | 90 (70.87) | ||||
| 27 (62.79) | 37 (29.13) | ||||
Note: Data are expressed as n (%).
Abbreviations: ASA, American Society of Anesthesiologists; BMI, body mass index.
Table 3 summarizes the perioperative complications observed in the patients included in this study. The most common complication was superficial surgical site infection, occurring in 6 cases (13.95%). Prolonged postoperative ileus, fever, and anastomotic leakage each occurred in 5 cases (11.63%). Wound erythema and edema, intestinal obstruction, and anastomotic bleeding were documented in 4 cases each (9.30%). Intra-abdominal abscess was diagnosed in 3 cases (6.98%). Stoma necrosis, intra-abdominal hemorrhage, and acute renal failure were noted in 2 cases each (4.65%). One case (2.33%) developed sepsis.
| Complication | n (%) |
| Wound erythema and edema | 4 (9.30) |
| Fever | 5 (11.63) |
| Anastomotic bleeding | 4 (9.30) |
| Prolonged postoperative ileus | 5 (11.63) |
| Superficial surgical site infection | 6 (13.95) |
| Anastomotic leakage | 5 (11.63) |
| Intra-abdominal abscess | 3 (6.98) |
| Intestinal obstruction | 4 (9.30) |
| Stoma necrosis | 2 (4.65) |
| Intra-abdominal hemorrhage | 2 (4.65) |
| Sepsis | 1 (2.33) |
| Acute renal failure | 2 (4.65) |
As shown in Table 4, univariate logistic regression analysis revealed that age,
presence or absence of comorbid diabetes mellitus, type of abdominal
anastomosis, and operation time were associated with perioperative complications
following laparoscopic colectomy for transverse colon cancer (p
| Factor | SE | Wald |
OR | 95% CI | p | ||
| Sex | |||||||
| Female | 1.000 | Reference | |||||
| Male | −0.162 | 0.374 | 0.188 | 0.850 | 0.408–1.770 | 0.664 | |
| Age (years) | |||||||
| 1.000 | Reference | ||||||
| 0.922 | 0.364 | 6.427 | 2.515 | 1.233–5.130 | 0.011 | ||
| BMI (kg/m2) | |||||||
| 1.000 | Reference | ||||||
| 0.306 | 0.361 | 0.719 | 1.358 | 0.669–2.756 | 0.396 | ||
| Smoking | |||||||
| No | 1.000 | Reference | |||||
| Yes | −0.296 | 0.373 | 0.633 | 0.743 | 0.358–1.543 | 0.426 | |
| Drinking | |||||||
| No | 1.000 | Reference | |||||
| Yes | 0.303 | 0.376 | 0.651 | 1.354 | 0.648–2.828 | 0.420 | |
| ASA physical status classification | |||||||
| Stage I–II | 1.000 | Reference | |||||
| Stage III–IV | 0.202 | 0.381 | 0.280 | 1.223 | 0.580–2.581 | 0.597 | |
| Comorbid diabetes mellitus | |||||||
| No | 1.000 | Reference | |||||
| Yes | 1.832 | 0.446 | 16.868 | 6.249 | 2.606–14.983 | ||
| Comorbid hypertension | |||||||
| No | 1.000 | Reference | |||||
| Yes | 0.133 | 0.356 | 0.139 | 1.142 | 0.568–2.295 | 0.710 | |
| Comorbid cardiovascular disease | |||||||
| No | 1.000 | Reference | |||||
| Yes | 0.170 | 0.359 | 0.223 | 1.185 | 0.586–2.396 | 0.637 | |
| Preoperative serum albumin level (g/L) | |||||||
| 1.000 | Reference | ||||||
| −0.223 | 0.354 | 0.397 | 0.800 | 0.400–1.601 | 0.529 | ||
| Preoperative anemia | |||||||
| No | 1.000 | Reference | |||||
| Yes | 0.237 | 0.360 | 0.434 | 1.268 | 0.626–2.568 | 0.510 | |
| TNM stage | |||||||
| Stage I–II | 1.000 | Reference | |||||
| Stage III–IV | −0.250 | 0.354 | 0.500 | 0.779 | 0.389–1.557 | 0.479 | |
| Tumor differentiation grade | |||||||
| High/Intermediate grade | 1.000 | Reference | |||||
| Low grade | 0.327 | 0.398 | 0.676 | 1.387 | 0.636–3.024 | 0.411 | |
| Abdominal anastomosis method | |||||||
| Intracorporeal anastomosis | 1.000 | Reference | |||||
| Extracorporeal anastomosis | 1.650 | 0.384 | 18.488 | 5.207 | 2.454–11.047 | ||
| Operation time (h) | |||||||
| 1.000 | Reference | ||||||
| 1.412 | 0.371 | 14.484 | 4.105 | 1.984–8.494 | |||
Abbreviations: ASA, American Society of Anesthesiologists; BMI, body mass index; CI, confidence interval; OR, odds ratio.
The VIF for the four factors identified in the univariate analysis—age (VIF =
1.035), presence or absence of diabetes mellitus (VIF = 1.061), type of
anastomosis method (VIF = 1.026), and operation time (VIF = 1.031)—were all
below 5, indicating the absence of multicollinearity. These factors were
therefore included in the multivariate logistic regression model. Results
demonstrated that comorbid diabetes mellitus (OR = 4.656; 95% CI: 1.715–12.640;
p = 0.003), extracorporeal anastomosis (OR = 5.943; 95% CI:
2.497–14.142; p
| Factor | SE | Wald |
p | OR | 95% CI | |
| Comorbid diabetes mellitus | 1.538 | 0.510 | 9.113 | 0.003 | 4.656 | 1.715–12.640 |
| Extracorporeal anastomosis | 1.782 | 0.442 | 16.232 | 5.943 | 2.497–14.142 | |
| Operation time |
1.509 | 0.435 | 12.052 | 4.520 | 1.929–10.595 | |
| Age |
0.664 | 0.425 | 2.436 | 0.119 | 1.943 | 0.844–4.472 |
Abbreviations: CI, confidence interval; OR, odds ratio; SE, standard error.
ROC curves were constructed to evaluate the predictive performance of individual
risk factors and their combination. The area under the ROC curve (AUC) for
predicting perioperative complications based on comorbid diabetes mellitus,
extracorporeal anastomosis, and operation time
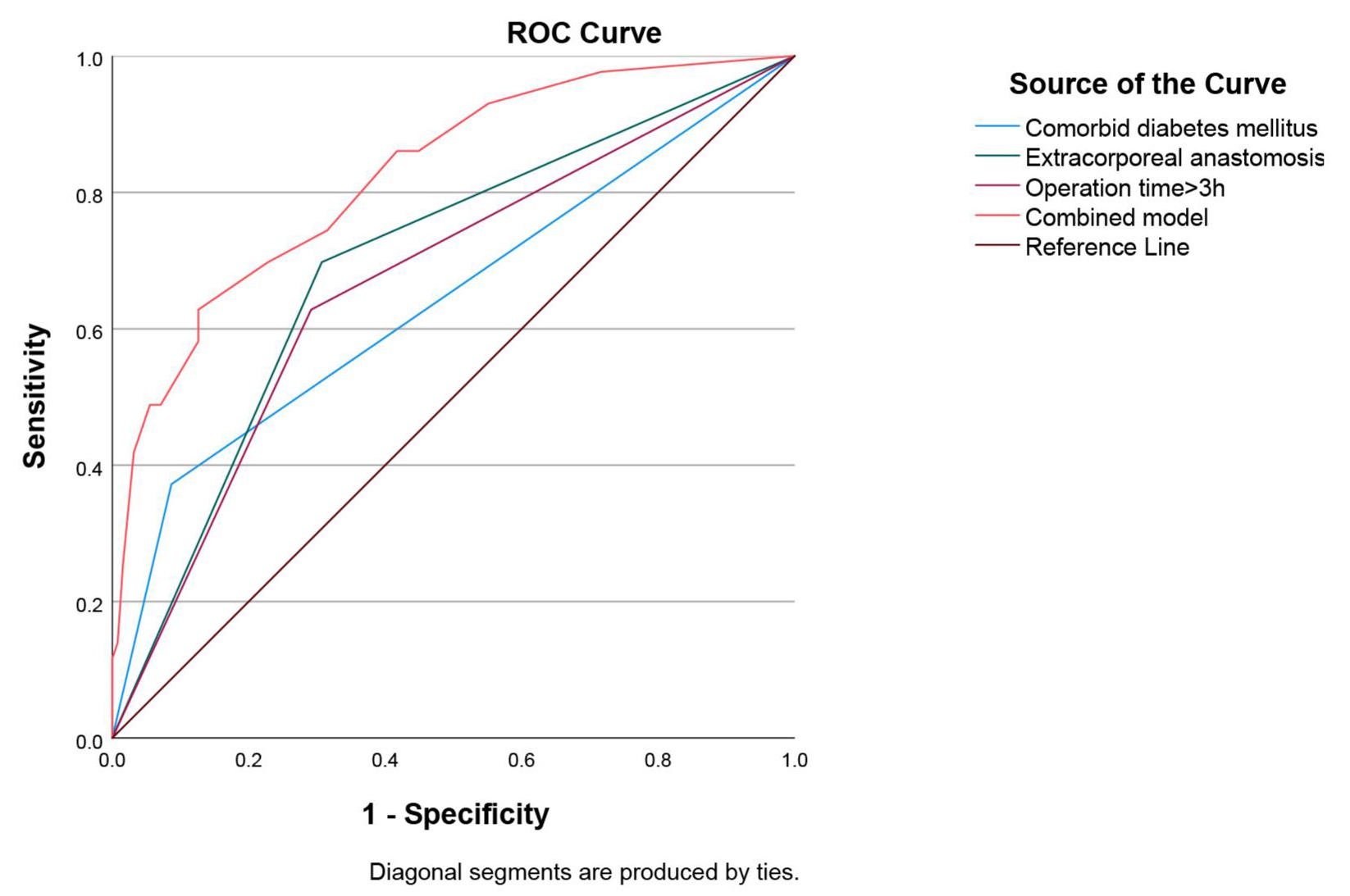 Fig. 2.
Fig. 2.
ROC curves for comorbid diabetes mellitus, extracorporeal anastomosis,
operation time
| Items | AUC | p | 95% CI | Sensitivity | Specificity | Youden index |
| Comorbid diabetes mellitus | 0.643 | 0.005 | 0.539–0.746 | 0.372 | 0.913 | 0.285 |
| Extracorporeal anastomosis | 0.695 | 0.603–0.787 | 0.698 | 0.693 | 0.391 | |
| Operation time |
0.668 | 0.001 | 0.573–0.764 | 0.628 | 0.709 | 0.337 |
| Combined model | 0.825 | 0.752–0.897 | 0.628 | 0.874 | 0.502 |
Abbreviations: AUC, area under the ROC curve; CI, confidence interval.
This retrospective analysis identified three independent risk factors for perioperative complications following laparoscopic colectomy in patients with transverse colon cancer: comorbid diabetes mellitus, extracorporeal anastomosis, and an operation time exceeding 3 h. These findings provide crucial evidence for identifying high-risk patients and optimizing perioperative management strategies. Below, we discuss the underlying mechanisms and clinical implications of these risk factors in light of existing literature.
Our study demonstrated that comorbid diabetes mellitus is an independent risk factor for increased perioperative complications after laparoscopic colectomy for transverse colon cancer. This finding aligns with conclusions from multiple studies on colonic cancer surgery. A Finnish population-based study reported significantly elevated complication rates after laparoscopic resection in stages I–III colon cancer patients with diabetes [24]. Furthermore, post hoc analysis of a prospective multicenter randomized controlled trial confirmed diabetes as an independent risk factor for surgical site infections following laparoscopic right hemicolectomy [6]. The increased risk of adverse outcomes after colorectal surgery in diabetic patients has well-established pathophysiological bases. Primarily, impaired immune function plays a central role: chronic hyperglycemia substantially compromises neutrophil chemotaxis, phagocytosis, and bactericidal activity, leading to diminished cellular immunity and heightened susceptibility to both local wound infections and systemic sepsis [25]. Secondarily, impaired tissue repair constitutes another critical factor: diabetes-associated microangiopathy disrupts tissue perfusion and oxygenation, delaying healing at surgical incision sites and anastomoses while markedly increasing the risk of anastomotic leakage [26]. Additionally, reduced organ reserve capacity should not be overlooked: diabetic patients often exhibit subclinical organ dysfunction, diminishing their overall tolerance to surgical trauma and anesthetic stress [27]. Given these mechanisms, rigorous perioperative glycemic control is imperative for diabetic patients undergoing transverse colectomy and should be prioritized equally with surgical technique. Evidence indicates that elevated postoperative infection risks correlate strongly with hyperglycemic states, while appropriate insulin therapy demonstrates a dose-response relationship in mitigating this risk [27]. Therefore, implementing targeted protocols such as insulin pump therapy to maintain perioperative blood glucose within an optimal range represents a key modifiable intervention for reducing complication rates in this patient population.
In this study, extracorporeal anastomosis was identified as the only risk factor of perioperative complications from among the technique-related factors screened. This finding strongly aligns with evolving trends in laparoscopic colonic surgery and existing evidence. With advancements in minimally invasive techniques, intracorporeal anastomosis has emerged as a preferred alternative to extracorporeal anastomosis. Technologically, intracorporeal anastomosis enables complete reconstruction of the gastrointestinal tract entirely within the abdominal cavity, typically requiring only a small accessory incision for specimen extraction—eliminating the need to exteriorize both ends of the colonic segment required by extracorporeal anastomosis [28]. This fundamental difference yields multiple clinical advantages: intracorporeal anastomosis significantly reduces abdominal wall incision size, minimizes traction and torsion on the colon and its mesentery, facilitates earlier postoperative bowel function recovery, shortens hospital stays, and lowers overall complication rates after laparoscopic left/right hemicolectomy [29, 30]. A systematic review and meta-analysis further substantiated that compared to extracorporeal anastomosis, intracorporeal anastomosis accelerates patient recovery and substantially reduces infections and total complications following right hemicolectomy [31].
Anatomically, the broad and mobile nature of the transverse mesocolon poses
unique challenges for extracorporeal anastomosis. When anastomosis was performed
extracorporeally, limited working space may necessitate increased manipulation of
the intestinal loops, potentially compromising perfusion at the anastomotic site.
Conversely, under magnified laparoscopic visualization, intracorporeal
anastomosis allows surgeons to achieve precise tension-free sutures while
preserving optimal blood supply—two critical pillars for preventing anastomotic
leakage [32, 33]. A Study demonstrated superior perioperative outcomes with
intracorporeal anastomosis in transverse colon cancer patients, including a
higher likelihood of achieving adequate surgical margins (
This study confirmed that an operation time exceeding 3 hours constitutes
another significant independent risk factor for perioperative complications
following laparoscopic resection in transverse colon cancer patients. Consistent
with recent evidence, post hoc analysis of the Radical Extent of
lymphadenectomy—D2 dissection versus complete mesocolic excision of
LAparoscopic Right Colectomy for right-sided colon cancer (RELARC) trial
identified procedures lasting over 180 minutes as an independent predictor of
complications in laparoscopic right hemicolectomy [6]. Similarly, a retrospective
analysis based on the Minimally-invasivE surgery for oncologic Right ColectomY
(MERCY) study group database demonstrated a significant association between
operation time
In this study, we demonstrated that a combined model incorporating the three
validated risk factors is essentially more effective in perioperative
complication prediction. The model achieved an AUC value of 0.825, demonstrating
significantly improved discriminative ability compared to any individual risk
factor (diabetes: AUC = 0.643; extracorporeal anastomosis: AUC =
0.695; prolonged operation time: AUC = 0.668). There are three theoretical bases
for integrating diabetic comorbidities, extracorporeal anastomosis, and prolonged
surgical duration (
It should be noted that in the present cohort, the complication group had a relatively high proportion of patients with ASA grade III–IV (69.77%) and poorly differentiated tumors (74.42%). Although these figures appear higher than those reported in some previous studies, they are not necessarily erroneous. One possible explanation is that our institution serves as a referral center for complex colorectal cancer cases, leading to an over-representation of patients with poorer general condition and more aggressive tumor biology. Additionally, the retrospective design and specific inclusion/exclusion criteria (e.g., exclusion of patients with incomplete records) may have introduced selection bias. Importantly, the data were carefully rechecked and confirmed to be accurate. Thus, these findings reflect the real-world situation of our study population and may remain valid, provided the interpretation is approached with caution.
This study has several limitations. First, the single-center retrospective design may introduce selection and information biases. Second, the relatively small sample size may reduce the statistical power for specialized analysis of certain rare yet serious complications, such as anastomotic leakage. Additionally, intraoperative variables, including estimated blood loss, intraoperative transfusion status, and fluctuations in hemodynamic or temperature, were not included in the study. Although these factors are known to influence surgical outcomes, they were excluded due to non-standardized recording to avoid introducing bias. Consequently, the current predictive model primarily reflects preoperative risk stratification and surgical strategy choices. Furthermore, dichotomizing continuous variables (such as operation time) facilitates clinical interpretation but results in a loss of statistical power and prevents the exploration of potential dose-response relationships with complication risks. Future prospective, multicenter studies with standardized perioperative data collection and the use of continuous variable modeling methods are necessary to further expand the model by integrating more validated intraoperative factors.
In summary, this retrospective study demonstrates that comorbid diabetes
mellitus, use of extracorporeal anastomosis, and prolonged operation time (
• This retrospective study identified comorbid diabetes mellitus,
extracorporeal anastomosis, and operation time
• The combined model incorporating these factors showed excellent predictive performance, with an AUC of 0.825, providing a practical tool for preoperative risk stratification.
• The study specifically addresses the unique anatomical and technical challenges of transverse colon cancer surgery, offering targeted evidence for this surgical context.
• These findings may directly inform clinical practice by optimizing patient selection, perioperative planning, and targeted interventions aimed at reducing postoperative morbidity.
The data used to support the findings of this study are available from the corresponding author upon request.
STJ and SW designed the research study. STJ drafted the manuscript. STJ and FY performed the research. STJ and LL analyzed the data. All authors contributed to the important editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
The study has been approved by the Ethics Review Committee of The First People’s Hospital of Yongkang (Approval number: 2025-LW-035) and strictly adheres to the principles outlined in the Declaration of Helsinki. The patients included in the study have signed the informed consent form.
Not applicable.
This research received no external funding.
The authors declare no conflicts of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.