
 , Jinfeng Lyu 1, Yuhong Zhang 1, Zheng Zhang 1,*
, Jinfeng Lyu 1, Yuhong Zhang 1, Zheng Zhang 1,*
1 Department of Hemodialysis, Zibo Central Hospital, 255020 Zibo, Shandong, China
Abstract
Hemodialysis is the primary form of treatment for patients with chronic renal failure. The lengthy dialysis process and rigid treatment schedule often lead to poor patient adherence. This study aims to explore the effects of interdisciplinary collaborative nursing and routine nursing on hemodialysis compliance in patients with chronic renal failure.
This retrospective analysis included clinical data of 136 patients with chronic renal failure who underwent hemodialysis in Zibo Central Hospital from April 2021 to January 2022. The patients were divided into a control group and an observation group according to the type of nursing care given. The control group received routine nursing, whereas the observation group received nursing intervention based on an interdisciplinary collaborative nursing model. Hemodialysis compliance, anxiety, awareness of disease, and health-related quality of life among the patients were evaluated.
Compared to the control group, the observation group exhibited significantly higher levels of hemodialysis compliance and disease knowledge (p < 0.05). The anxiety level of the observation group was significantly lower than that of the control group (8.04 ± 5.06 vs. 12.49 ± 4.87; p < 0.001). In terms of quality of life, the observation group scored higher than the control group in physical, psychological, social, and environmental domains (p < 0.05).
The interdisciplinary collaborative nursing enhances hemodialysis compliance in patients with chronic renal failure, ameliorates their anxiety, and improves their health-related quality of life. This research provides a theoretical basis for the design and selection of clinical management plans in the future.
Keywords
- kidney failure
- renal dialysis
- compliance
- nursing care
- anxiety
Chronic kidney disease refers to the irreversible structural damage or impairment of kidney function [1]. Chronic kidney disease has a significant impact on the quality of life and health of patients, imposes huge burdens on their families, and has been listed as one of the top ten causes of death worldwide [2, 3]. The global prevalence of chronic kidney disease is estimated at approximately 9–13% and continues to rise each year, with China alone accounting for more than 130 million patients [4, 5]. Chronic renal failure (CRF) usually occurs in the later stages of chronic kidney disease, clinically classified as a glomerular filtration rate of less than 15 mL per minute per 1.73 m2 [6], with hemodialysis, peritoneal dialysis, and kidney transplantation being the major treatments. However, due to the limited availability of organ donors, dialysis supersedes transplantation as the most common modality of treatment, and the global records show that more than 3.5 million CRF patients are recipients of dialysis treatment [6].
Dialysis works by removing solutes and excess fluid through diffusion across a semipermeable membrane and ultrafiltration. The predominant dialysis modalities are hemodialysis, peritoneal dialysis, and hemofiltration, whereas hemodiafiltration and intestinal dialysis are less commonly used approaches [7]. Most CRF patients require lifelong dialysis, and the treatment regimen is highly rigid, marked by stringent fluid and dietary restrictions, strict medication adherence, and a time-consuming dialysis schedule of up to 3–4 hours per session, three times a week. Therefore, for CRF patients undergoing hemodialysis, strict compliance with treatment is essential. Failure in dialysis compliance would result in the accumulation of toxic substances that cannot be metabolized in the body, causing various complications and even death. Generally, patients’ compliance is affected by multiple factors, such as their understanding of the disease, levels of anxiety and apathy toward their condition, family support, and the type of nursing intervention they receive [8, 9, 10].
At present, the interdisciplinary collaborative nursing mode has emerged and gradually replaced the traditional nursing mode as the primary form of nursing intervention for patients with CRF [11]. Interdisciplinary collaborative nursing entails the formation of a patient-centered nursing team comprising medical and nursing experts from different disciplines [12]. Under the traditional nursing mode, patients have poor compliance with hemodialysis due to various factors, and are prone to anxiety, depression and fear, which seriously affect their quality of life and treatment progress [13, 14]. The interdisciplinary collaborative nursing mode is expected to improve the treatment compliance of patients and their quality of life [15]. Currently, evidence on the effectiveness of interdisciplinary collaborative nursing mode in improving hemodialysis compliance and psychosocial outcomes in patients with CRF remains relatively scarce. Thus, this retrospective study aimed to analyze the impacts of different nursing modes on hemodialysis compliance, anxiety levels, disease knowledge, and health-related quality of life in patients with CRF.
A total of 136 patients with CRF undergoing hemodialysis at Zibo Central
Hospital from April 2021 to January 2022 were included in this study. The
inclusion criteria are as follows: (1) aged
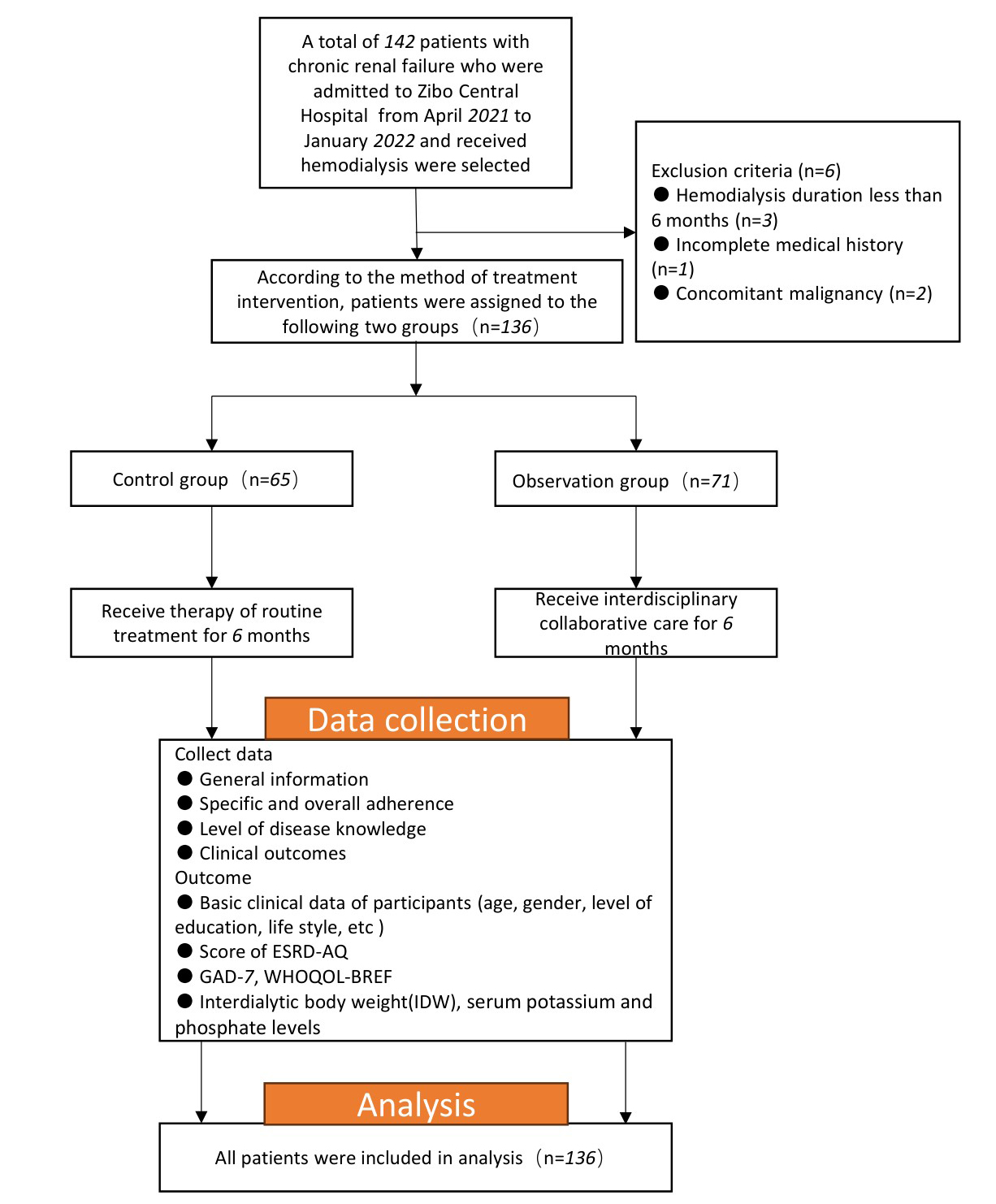
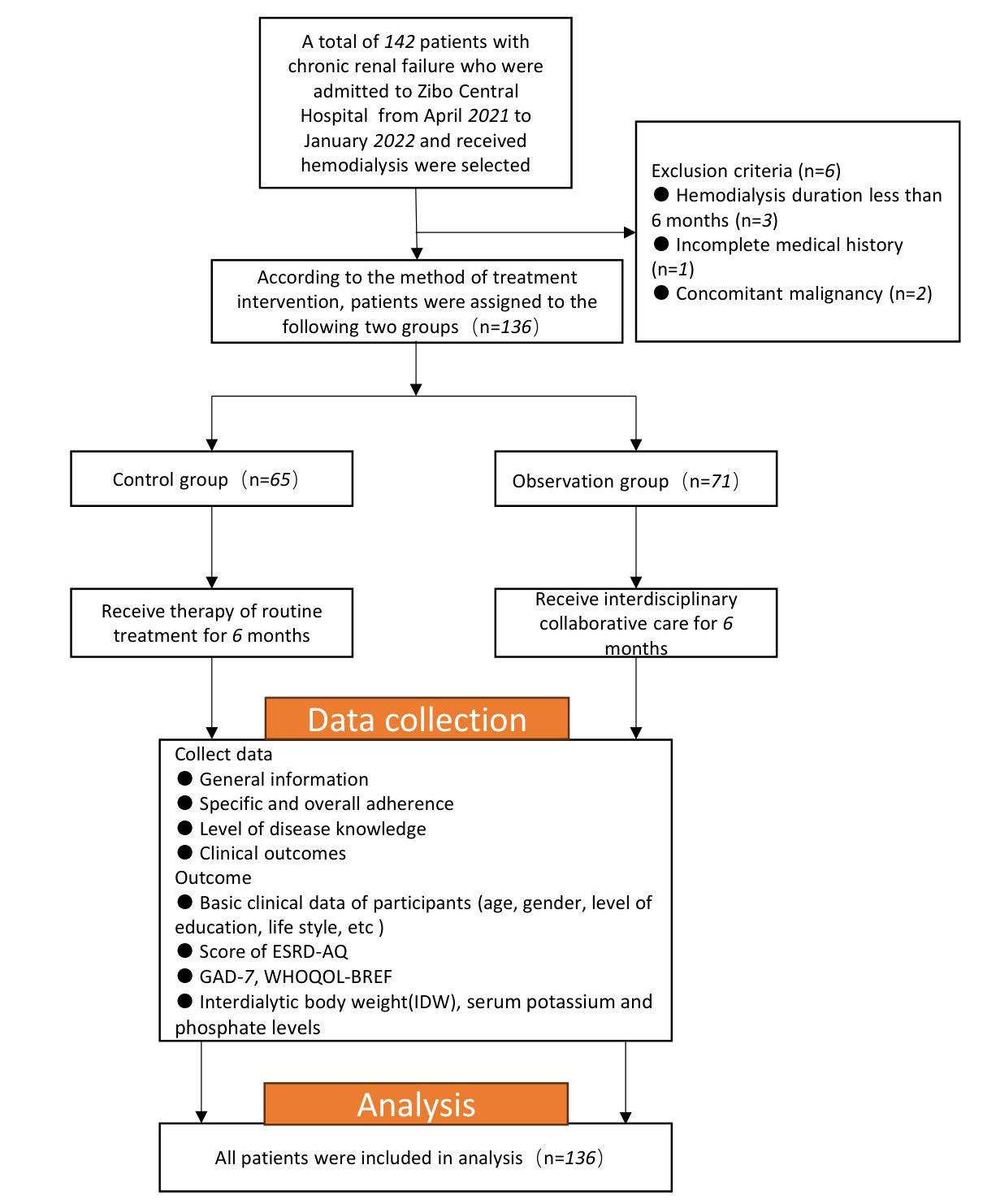 Fig. 1.
Fig. 1.
Flowchart of patient selection and grouping. ESRD-AQ, End Stage Renal Disease-Adherence Questionnaire; GAD-7, Generalized Anxiety Disorder 7; WHOQOL-BREF, World Health Organization Quality of Life-BREF Scale.
The control group received routine nursing as follows:
(1) Pre-dialysis preparation: The nurses checked patients’ identity, evaluated dialysis equipment and vascular access before dialysis, and measured their blood pressure, heart rate, body temperature and other vital signs to ensure that they were healthy prior to dialysis initiation.
(2) Dialysis monitoring: The nurses continuously observed the patients’ blood pressure, electrocardiogram (ECG), dialysate parameters, and fluid balance during dialysis, and provided instant treatment for common complications such as hypotension, convulsions and spasms upon detection.
(3) Basic education and diet guidance: The nurses provided fundamental health education to patients during daily follow-up, including diet control (e.g., limiting potassium- and phosphate-rich foods), fluid intake control, standardized use of drugs, and the importance of maintaining dialysis compliance.
The control group received routine nursing throughout the study period, which was implemented during each dialysis session (3 times per week, 3–4 hours per session) and continued for 6 months.
Interdisciplinary collaborative nursing intervention refers to the establishment of a multidisciplinary team consisting of an attending physician, three nurses, a nutritionist, a clinical pharmacist, and a psychologist. The observation group received interdisciplinary collaborative nursing as follows:
(1) Comprehensive health education: An education manual—consisting of relevant content based on themes determined by the multidisciplinary team members through regular academic meetings—is created after strict revision. Each patient will receive a copy of the manual. The manual covers a broad spectrum of relevant health education-related content, such as dialysis compliance, timely medication use, diet and fluid control, and the interrelationship among dialysis-related symptoms, such as hyperkalemia and arrhythmia, to enhance patients’ understanding of the disease and strengthen their self-management ability. The nurses would explain and answer questions in stages during the interval of dialysis.
(2) Nutritional guidance: Nutritionists formulated a personalized diet plan tailored to each patient after assessing their nutritional status, taking into account the effects of dialysis on protein, potassium, phosphate, and electrolyte balance. They would also educate the patients on the recommended foods, cooking methods, and specific restrictions, and introduce adjustments to the plan throughout the follow-up.
(3) Drug intervention: Clinical pharmacists reviewed patients’ medication regimens, monitored for potential drug-drug interactions, and assessed the impact of dialysis on drug clearance. During their slots, they would introduce the key drugs commonly used by the patients, such as phosphate binders, antihypertensive agents, and erythropoietin, and demonstrate the proper usage to ensure patient safety and compliance.
(4) Psychological counseling: Through individual psychological counseling and group counseling regularly, psychologists offer feedback and words of advice to the patients to help them relieve anxiety and depression, so as to improve their adaptability to long-term dialysis treatment. When necessary, the psychologists will cooperate with other team members to make customized adjustments to patient’s nursing care and education plan.
The observation group received the interdisciplinary collaborative nursing intervention for 6 months. The comprehensive health education briefing was conducted weekly during dialysis session. Nutritional guidance, drug intervention and psychological intervention are carried out once a month, and these interventions can be adjusted according to the patient’s condition, when necessary.
Clinical and baseline information, including age, gender, education level, disease duration, body mass index (BMI), history of smoking, marital status, presence of chronic diseases (such as diabetes or hypertension), and family history of renal failure, was collected.
The End Stage Renal Disease-Adherence Questionnaire (ESRD-AQ) was used to evaluate the adherence of patients, originally developed by Kim et al. [16] to capture multidimensional adherence behaviors in hemodialysis patients (attendance, medication, fluid, diet). The EDRD-AQ has been translated and validated in multiple languages and settings [17]. The questionnaire consists of five parts, including 46 items. The first part contains the patient’s relevant medical history, and the other four parts measure the patient’s compliance with treatment, adherence of medication use, fluid and dietary restriction during the course of hemodialysis. Questions 14, 17, 18, 26, 31, and 46 in the ESRD-AQ, which evaluate treatment compliance behavior, were translated into Chinese, and the translations were reviewed by a multidisciplinary team to ensure preservation of the intended meaning. These questions have different score ranges, with question 14 having a score range of 0–300, questions 17, 26, 31, and 46 having a score range of 0–200, and question 18 having a score range of 0–100. The higher the score, the stronger the treatment compliance in the patients.
Serum levels of phosphate and potassium, as well as body weight changes, were measured before and 6 months after dialysis to assess clinical outcomes of these patients. Serum potassium was used as a biomarker for assessing compliance of dietary restrictions, whereas serum phosphate was utilized to evaluate drug use adherence. Interdialytic weight (IDW) was calculated as the difference between patients’ pre-dialysis and post-dialysis weights. IDW, together with relevant biomarkers, was used to evaluate patients’ fluid management. Serum potassium levels remained below 6.0 mmol/L and showed a downward trend, while serum phosphate levels remained below 7.5 mg/dL and also decreased. An IDW of no more than 2.5 kg was considered indicative of a favorable clinical outcome.
Originally introduced by Spitzer et al. [18] as a quick screening tool in clinical settings, the Generalized Anxiety Disorder 7 (GAD-7) scale was used to evaluate the anxiety degree of patients in the two groups [19]. The GAD-7 has been widely validated in general and clinical populations in various languages, showing good internal consistency and diagnostic performance (in terms of sensitivity and specificity) [18]. This 7-item scale uses a 0–3 scoring range per item, resulting in a total score spanning 0–21, where higher scores indicate increased anxiety. Anxiety severity was categorized as follows: 0–4 (slight or none), 5–9 (mild), 10–14 (moderate), and 15–21 (severe).
Questions 11, 12, 22, 23, 32, 33, 41, and 42 of the ESRD-AQ assess patients’ awareness of the disease. In the original questionnaire, no explicit scoring was provided for these eight questions. After translation, each of these questions was assigned with a scoring scale of 1–5 points. A higher total score obtained indicates that the patient has a better understanding of the disease.
Health-related quality of life (HRQoL) in both groups was assessed using the World Health Organization Quality of Life-BREF Scale (WHOQOL-BREF) [20], which contains a total of 26 items. WHOQOL-BREF was developed by the World Health Organization in 1998 and has been validated across many countries marked by distinct cultural features with good psychometric properties [21, 22]. Two items are independent analysis items for the measurement of the overall quality of life. The remaining content of the scale comprises four domains: physical (7 items), psychological (6 items), social (3 items), and environmental domains (8 items). Items are rated on a 1–5 point scale, with higher scores denoting better quality of life.
The data were processed and analyzed using SPSS 22.0 statistical software (IBM
Corp., Armonk, NY, USA). Normality and homogeneity of variance of continuous data
were evaluated. Normally distributed data are presented as mean
A total of 136 patients with CRF undergoing hemodialysis in Zibo Central
Hospital from April 2021 to January 2022 were included in this study and divided
into two groups according to the nursing mode applied. Among them, 65 patients in
the control group received routine nursing care, and 71 patients in the
observation group received interdisciplinary collaborative nursing care. No
statistically significant intergroup differences were observed in
sociodemographic variables (p
| Variables | Control group (n = 65) | Observation group (n = 71) | Statistic | p | |
| Age (years) | 53.98 |
55.86 |
t = −1.66 | 0.099 | |
| Disease duration (months) | 25.52 |
26.93 |
t = −1.72 | 0.087 | |
| BMI (kg/m2) | 23.70 |
24.25 |
t = −1.16 | 0.250 | |
| Smoking history | 0.333 | ||||
| No | 53 (81.54) | 53 (74.65) | |||
| Yes | 12 (18.46) | 18 (25.35) | |||
| Family history of kidney failure | 0.920 | ||||
| No | 62 (95.38) | 69 (97.18) | |||
| Yes | 3 (4.62) | 2 (2.82) | |||
| Gender | 0.541 | ||||
| Male | 36 (55.38) | 43 (60.56) | |||
| Female | 29 (44.62) | 28 (39.44) | |||
| Marital status | 0.981 | ||||
| Divorced or widowed | 23 (35.38) | 24 (33.80) | |||
| Married | 24 (36.92) | 27 (38.03) | |||
| Unmarried | 18 (27.69) | 20 (28.17) | |||
| With chronic conditions | |||||
| Hypertension | 18 (27.69) | 26 (36.62) | 0.266 | ||
| Hyperglycemia | 6 (9.23) | 5 (7.04) | 0.640 | ||
| Level of education | 0.057 | ||||
| High school and below | 46 (70.77) | 39 (54.93) | |||
| College and above | 19 (29.23) | 32 (45.07) | |||
Abbreviation: BMI, body mass index.
In this study, the ESRD-AQ scale was used as a tool to evaluate patients’
compliance. There was no significant difference in individual scores between the
two groups before implementation of the nursing intervention (p
| Item | Adherence | Control group (n = 65) | Observation group (n = 71) | Statistic | p |
| Before nursing intervention | |||||
| 14 | Number of dialysis sessions | 245.72 |
250.45 |
t = −0.96 | 0.341 |
| 17 | Whether to shorten dialysis | 152.75 |
150.89 |
t = 0.87 | 0.387 |
| 18 | Reduced duration of dialysis | 66.23 |
65.86 |
t = 0.18 | 0.860 |
| 26 | Medication use adherence | 169.06 |
167.21 |
t = 0.94 | 0.351 |
| 31 | Fluid restriction compliance | 122.23 |
121.54 |
t = 0.51 | 0.614 |
| 46 | Dietary restriction compliance | 133.20 |
131.44 |
t = 1.05 | 0.297 |
| After nursing intervention | |||||
| 14 | Number of dialysis sessions | 271.72 |
277.17 |
t = −2.06 | 0.041* |
| 17 | Whether to shorten dialysis | 165.30 |
170.58 |
t = −2.44 | 0.016* |
| 18 | Reduced duration of dialysis | 78.91 |
80.80 |
t = −2.90 | 0.004* |
| 26 | Medication use adherence | 173.54 |
175.76 |
t = −2.46 | 0.016* |
| 31 | Fluid restriction compliance | 134.09 |
137.99 |
t = −3.38 | |
| 46 | Dietary restriction compliance | 144.62 |
150.23 |
t = −5.26 | |
* p
Serum potassium, phosphate and IDW were measured before and 6 months after dialysis as clinical outcomes.
Before dialysis, the serum potassium levels and the number of patients meeting
the serum potassium criteria were comparable between the two groups (p
| Variables | Control group (n = 65) | Observation group (n = 71) | Statistic | p | |
| Pre-dialysis level (mmol/L) | 5.22 (4.93, 5.80) | 5.26 (5.07, 5.83) | Z = 0.75 | 0.455 | |
| Post-dialysis level (mmol/L) | 4.61 (4.30, 4.99)# | 4.00 (3.57, 4.38)# | Z = 6.82 | ||
| Number of eligible people before dialysis, n (%) | 0.982 | ||||
| Not qualified | 12 (18.46) | 13 (18.31) | |||
| Qualified | 53 (81.54) | 58 (81.69) | |||
| Number of eligible people after dialysis, n (%) | 0.018* | ||||
| Not qualified | 9 (13.85) | 2 (2.82) | |||
| Qualified | 56 (86.15) | 69 (97.18) | |||
* p
Before dialysis, there were no significant differences in serum phosphate levels
and the number of patients meeting the serum phosphate standard between the two
groups (p
| Variables | Control group (n = 65) | Observation group (n = 71) | Statistic | p | |
| Pre-dialysis level (mg/dL) | 6.65 (6.00, 7.33) | 6.77 (6.03, 7.26) | Z = 0.31 | 0.757 | |
| Post-dialysis level (mg/dL) | 5.88 (5.50, 6.09)# | 4.50 (3.99, 4.90)# | Z = 8.69 | ||
| Qualified before dialysis, n (%) | 0.697 | ||||
| Not qualified | 12 (18.46) | 15 (21.13) | |||
| Qualified | 53 (81.54) | 56 (78.87) | |||
| Qualified after dialysis, n (%) | 0.048* | ||||
| Not qualified | 9 (13.85) | 3 (4.23) | |||
| Qualified | 56 (86.15) | 68 (95.77) | |||
| IDW, n (%) | |||||
| Not qualified | 42 (64.62) | 18 (25.35) | |||
| Qualified | 23 (35.38) | 53 (74.65) | |||
* p
Individual scores did not differ significantly between the two groups prior to
the nursing intervention (p
| Variables | Control group (n = 65) | Observation group (n = 71) | Statistic | p | |
| Pre-intervention scores | 16.55 |
16.66 |
t = −0.33 | 0.743 | |
| Post-intervention scores | 12.49 |
8.04 |
t = 5.22 | ||
| Pre-intervention anxiety level, n (%) | 0.479 | ||||
| Moderate | 10 (15.38) | 8 (11.27) | |||
| Severe | 55 (84.62) | 63 (88.73) | |||
| Post-intervention anxiety level, n (%) | |||||
| Severe | 24 (36.92) | 11 (15.49) | |||
| Moderate | 20 (30.77) | 15 (21.13) | |||
| Mild | 19 (29.23) | 25 (35.21) | |||
| Slight or none | 2 (3.08) | 20 (28.17) | |||
* p
Both control and observation groups showed comparable levels in disease
understanding prior to the implementation of nursing intervention (p
| Variables | Control group (n = 65) | Observation group (n = 71) | Statistic | p |
| Pre-intervention | 20.94 |
22.10 |
t = −1.84 | 0.068 |
| Post-intervention | 30.15 |
32.04 |
t = −2.41 | 0.019* |
| Statistic | t = −12.65 | t = −14.11 | ||
| p |
* p
Before nursing interventions were implemented, the individual domain scores of
the health-related quality of life were not significantly different between the
control and observation groups (p
| Variables | Control group (n = 65) | Observation group (n = 71) | Statistic | p |
| Before nursing intervention | ||||
| Physical domain | 19.48 |
19.38 |
t = 0.10 | 0.921 |
| Psychological domain | 18.98 |
18.58 |
t = 0.95 | 0.344 |
| Social domain | 5.68 |
5.54 |
t = 0.37 | 0.713 |
| Environmental domain | 23.06 |
23.06 |
t = 0.01 | 0.991 |
| After nursing intervention | ||||
| Physical domain | 24.68 |
29.39 |
t = –8.09 | |
| Psychological domain | 22.52 |
24.23 |
t = –4.19 | |
| Social domain | 8.42 |
10.03 |
t = –4.12 | |
| Environmental domain | 29.46 |
31.37 |
t = –2.51 | 0.013* |
* p
According to global epidemiological studies, chronic kidney disease (CKD) is a major contributor to mortality worldwide, with approximately 1.48 million deaths in 2023, making it one of the top ten causes of death globally and underscoring the expanding health burden of CKD and its related complications [23], highlighting CRF as a life-threatening condition. Hemodialysis is the primary treatment modality for patients with CRF [24], but the lengthy dialysis process and frequent schedules are among its notable drawbacks [25, 26].
In this study, we investigated the effects of different nursing modes on patients’ compliance, anxiety, disease understanding, and health-related quality of life. Both the control and observation groups tested exhibited comparable baseline demographics. Patients receiving interdisciplinary care demonstrated significantly superior adherence to treatment regimens, medication protocols, fluid control, and dietary restrictions, compared to the controls. Due to the subjectiveness of the questionnaire used, we also adopted IDW, serum levels of potassium and phosphate of the patients as clinical indicators to evaluate their degree of treatment compliance. The observation group achieved significantly improved IDW compliance, serum levels of potassium and phosphate, relative to the controls. High overall adherence correlated with enhanced treatment efficacy. The observation results validate the effectiveness of the interdisciplinary collaboration nursing mode, demonstrating a higher degree of treatment compliance among the patients using this nursing mode.
Subjects in the observation group had significantly greater understanding of
the disease than those in the control group (32.04
Several limitations of this study need to be acknowledged. First, the adoption of a single-center, retrospective study design and a relatively small sample size in this research may affect the generalizability of the results. Second, although there were no statistically significant differences in baseline sociodemographic and clinical characteristics between the two groups of patients, the lack of randomization, which is inherent in the retrospective study design, may impact the results, probably due to the presence of unmeasured or unrecorded confounding factors. Furthermore, key indicators, including anxiety levels and quality of life, were primarily assessed via questionnaires, which are inherently subjective. Future research should expand the sample size, adopt a multicenter prospective design, and introduce more objective physiological or behavioral parameters to control for potential confounding factors and further validate the conclusions of this study.
This study demonstrates that the interdisciplinary collaborative nursing intervention significantly improves hemodialysis compliance, expands disease understanding, reduces anxiety levels, and enhances clinical outcomes as well as health-related quality of life in patients with CRF. These multidimensional improvements may elevate survival rates and reduce complications in hemodialysis-dependent CRF patients, aligning with the core nursing principles for this patient population. Future research should assess intervention sustainability, monitor complication incidence, and optimize therapeutic efficacy in this population.
• This study examines the effects of interdisciplinary collaborative nursing versus traditional nursing on hemodialysis compliance in patients with CRF.
• Interdisciplinary collaborative nursing mode significantly enhances patients’ hemodialysis compliance, improves clinical indicators such as serum potassium and phosphate, and reduces interdialytic weight.
• Compared with the traditional nursing mode, the interdisciplinary approach effectively reduces patients’ anxiety, expands their disease understanding, and strengthens their self-management ability.
• Regarding health-related quality of life, patients in the observation group experienced significant improvements across four domains: physical, psychological, social, and environmental.
• Therefore, the interdisciplinary collaborative nursing mode demonstrates significant clinical value in the management of patients with CRF undergoing hemodialysis, offering a solid foundation for the development and implementation of subsequent care strategies.
The data that support the findings of this study are available from the corresponding author upon reasonable request.
HW and JFL designed the research study. YHZ and ZZ performed the research. HW and ZZ analyzed the data. ZZ drafted the manuscript. All authors contributed to the important editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
This study has been approved by the Ethics Committee of Zibo Central Hospital (Ethics No. 202104022). The study protocol was designed in accordance with the Declaration of Helsinki, and the enrolled patients signed a written informed consent.
Not applicable.
This research received no external funding.
The authors declare no conflicts of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.