





 , Graeme James Kevin Guthrie 2, Stuart Alistair Suttie 2
, Graeme James Kevin Guthrie 2, Stuart Alistair Suttie 21 Department of Vascular Surgery, Queen Elizabeth University Hospital, G51 4TF Glasgow, UK
2 Department of Vascular Surgery, Ninewells Hospital and Medical School, DD1 9SY Dundee, UK
Abstract
Globally and within the United Kingdom, there has been an increase in the number of people who inject drugs (PWID). PWID are at increased risk of injection site and systemic infections, which include abscesses, necrotising soft tissue infections, arterial pseudoaneurysms and infective endocarditis. Initial diagnosis and treatment of groin-related complications can be complex and frequently require emergent surgical input while ensuring adequate antimicrobial therapy. The importance of utilising a patient-centred multidisciplinary approach to promote patient engagement, while using each healthcare interaction as an opportunity to mitigate further harm, should not be underestimated. This review will examine acute presentations in PWID and provide a practical approach to diagnosing and managing groin-related complications. It is essential to maintain a high index of suspicion, promptly recognise symptoms, and initiate specific management protocols.
Keywords
- drug users
- necrotising
- injecting
- groin
- pseudoaneurysm
- thrombophlebitis
- endocarditis
The United Nations World Drug Report [1] estimates that there are over 13.9 million people who inject drugs globally. Drug use in the UK is the highest reported in any country in Western Europe [2, 3]. It is estimated that over 770,000 people aged 16 to 59 in England are frequent drug users, of whom approximately 87,000 people inject drugs [4]. When expressed as a percentage of the population, Scotland has a far higher rate of problem drug use than England (1.62% compared with 0.74%) and other European countries [5].
People who inject drugs (PWID) have significantly higher morbidity and mortality compared to the general population. Contributing factors include injecting-related harms and overdose, as well as delayed presentation to health care services that result in significantly advanced disease patterns that make management more challenging and resource-intensive [6]. A systematic review by van Boekel et al. [7] concluded that PWID frequently experience stigma from health care staff, which affects their engagement in care and leads to suboptimal outcomes. We should be mindful as we embark on discussing early diagnosis and management of the groin in this cohort of patients.
The causes of infection in this group are multifactorial. This includes non-sterile injecting techniques, contaminated diluents (saliva or toilet water), licking of needles, the sharing of injecting equipment, anatomical area of injecting, preceding contamination of the drugs in transit and higher risk injecting practices such as injecting subcutaneously or intramuscularly (“popping”), a practice particularly associated with the development of necrotising soft tissue infections (NSTI) [8, 9, 10].
Furthermore, drug solutions in the UK tend to be acidic (the commonly used brown heroin and crack cocaine need to be dissolved in acidic solutions). When this is injected subcutaneously, intramuscularly or intravenously, it can precipitate tissue and venous damage [11, 12].
But why the groin? There may be several factors for this. For some PWID, it is a last resort after other peripheral sites have been sclerosed, and for others, it is the preferred site due to its discreet location and relative ease of ensuring a “hit” with each injection [13]. Many studies in the literature depend on self-reported data and limited patient cohorts, which can result in bias and issues with reproducibility. Objective clinical assessments are essential to accurately determine the prevalence and severity of groin-related complications and their management; however, this may be difficult to obtain given the varied presentation and local differences in management strategies.
PWID may experience various groin-related complications that can be challenging to distinguish from one another. Therefore, these cases should be approached with careful consideration to minimise potential morbidity. Common presentations are described below, and having a diagnostic algorithm is beneficial (see Fig. 1). To date, no scoring system has been validated for use specifically in this patient population, and though many exist, the emphasis should be on early diagnosis and referral to the appropriate speciality as outlined.
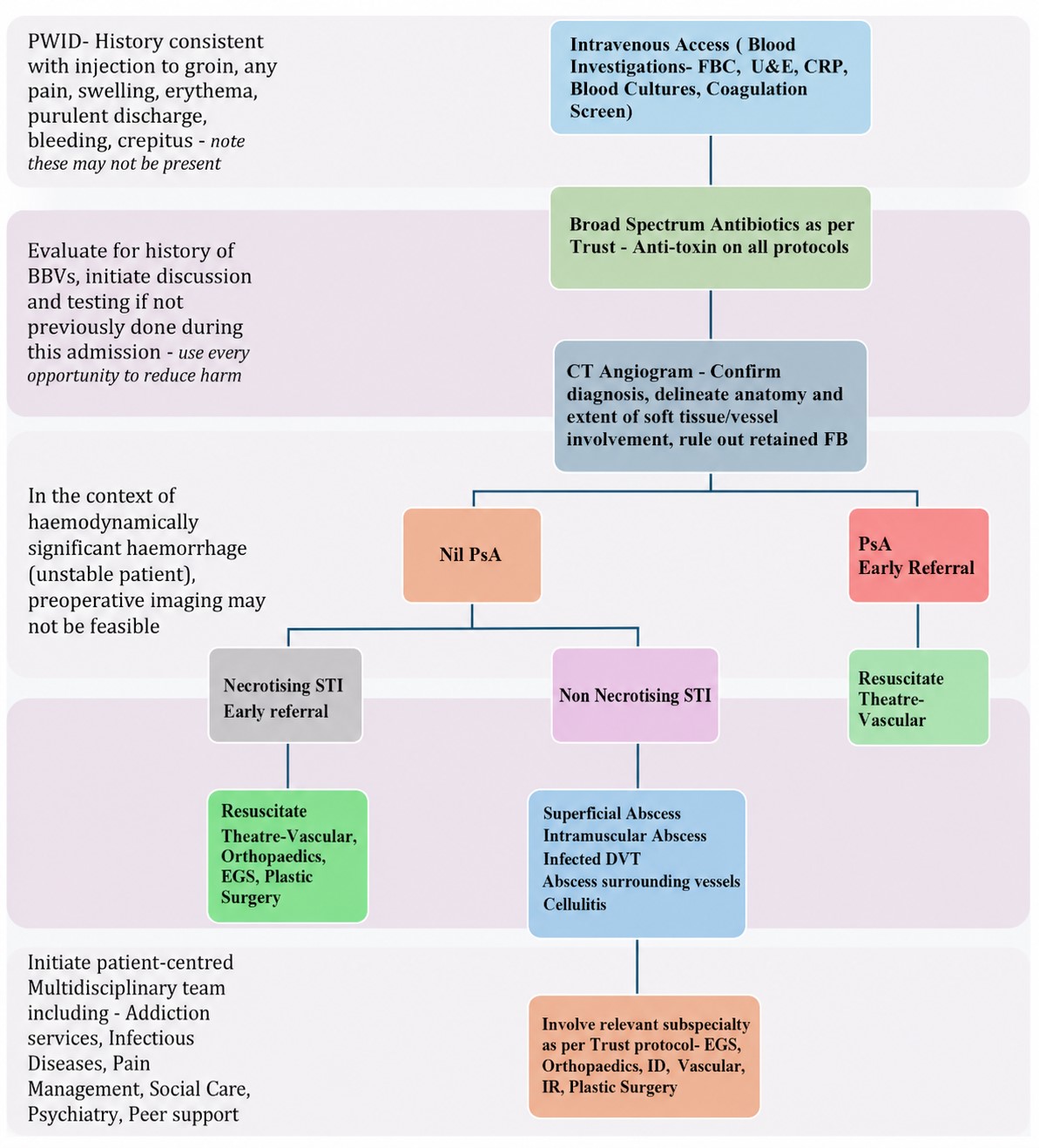 Fig. 1.
Fig. 1.
Diagnostic algorithm. PWID, people who inject drugs; FBC, full blood count; U&E, urea and electrolytes; CRP, C-reactive protein; FB, foreign body; PsA, pseudoaneurysm; STI, soft tissue infection; EGS, emergency general surgery; DVT, deep venous thrombosis; ID, infectious diseases; IR, interventional radiology; CT, computed tomography; BBVs, blood-borne viruses.
Non-necrotising soft tissue infections (non-NSTIs) are the most common presentation, which includes cellulitis and superficial abscesses. In a review of PWID in urban areas in England by Hope and colleagues [14] 48% of patients reported erythema, tenderness and swelling at injection sites, while a systematic review [15] found that abscess formation is more commonly seen in women, in those with greater frequency of injecting, and in PWID who inject into tissues rather than veins (“popping”) [10].
Necrotising soft tissue infections (NSTI) are a clinically aggressive group of infections characterised by rapidly progressive soft tissue destruction resulting in necrosis of subcutaneous tissue, fascia or muscle with high rates of morbidity and mortality [16]. In a recent retrospective cohort study by MacLeod et al. [6], it was noted that significantly more NSTI patients required both high dependency and intensive care unit admissions than non-NSTI patients, which gives an indication of the systemic inflammatory burden associated with this diagnosis.
NSTI in PWID remains somewhat difficult to diagnose, as early symptoms can appear similar to non-NSTI. Key indicators include pain disproportionate to other symptoms, indistinct infection margins, rapid progression (necessitating serial examinations), and tenderness of seemingly unaffected skin [17]. The early identification, imaging, and timely surgical debridement have been correlated with enhanced survival rates [18].
Though NSTI is a clinical diagnosis, the relative ease of access to cross-sectional imaging in the form of a contrast-enhanced computed tomography (CT) should be utilised as an adjunct when faced with the PWID groin. CT features associated with NSTI include asymmetrical fascial involvement, non-enhancement of fascia after contrast injection (which is the most specific finding), oedema extending across fascial planes and into muscle, as well as fluid and gas collections [19] (see Figs. 2,3).
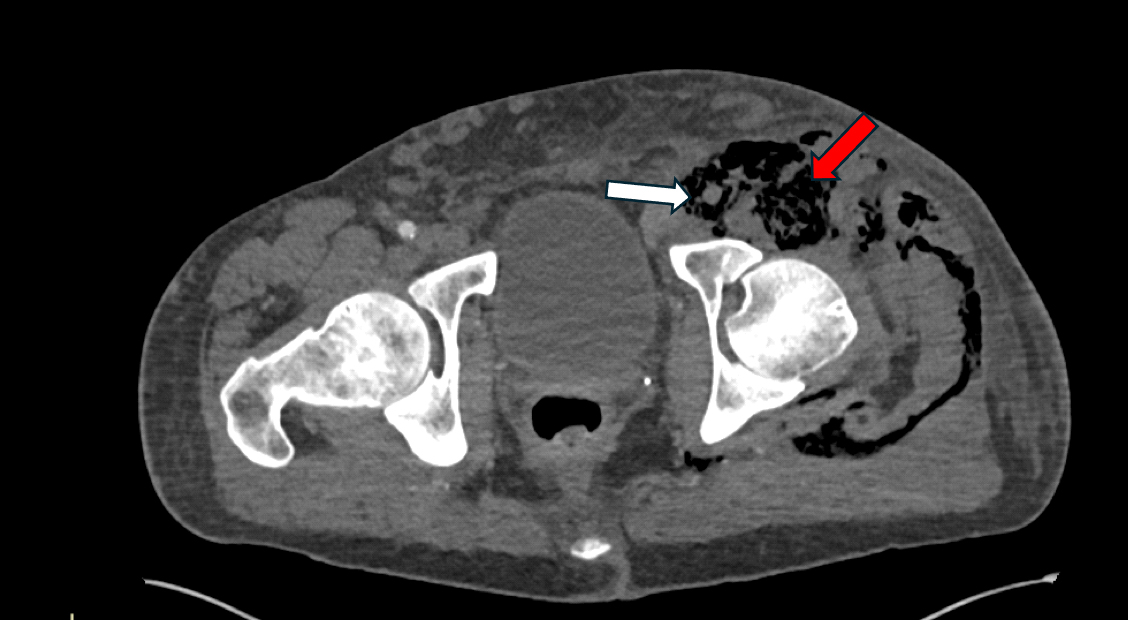 Fig. 2.
Fig. 2.
Axial computed tomography (CT). White arrow—Thrombosed left common femoral artery, red arrow—Gas and fluid collection.
 Fig. 3.
Fig. 3.
Coronal CT. Red arrows indicate extensive gas within the tissues.
A pseudoaneurysm occurs when blood leaking from an injured vessel collects within the surrounding soft tissues, as opposed to a true aneurysm, which contains all layers of the vessel wall.
In PWID, accidental arterial injection of illicit substances leads to peri-arterial extravasation and haematoma formation. Contamination of this haematoma may lead to erosion and eventual rupture of the vessel wall, resulting in pseudoaneurysm formation [20]. Pain, swelling and a pulsatile mass (see Fig. 4) may be present in a few; however, historical reports of misdiagnoses leading to major haemorrhage when attempting to drain an “abscess” serve as a reminder that each case should be evaluated with a high index of suspicion [21].
 Fig. 4.
Fig. 4.
Left groin painful pulsatile indurated swelling. Note central threatened skin due to soft tissue sepsis and pressure effect of underlying pseudoaneurysm.
As always, patient history is important. A history of bleeding or a herald bleed may often precede life-threatening haemorrhage [22]. Arterial duplex imaging was previously the imaging modality of choice in many centres as it gave a dynamic view of the pseudoaneurysm but in this patient cohort when faced with diagnostic uncertainty CT angiography not only adequately characterises the aneurysm but gives information on the proximal and distal extent of soft tissue sepsis as well as other local factors which are important for periprocedural planning [21, 22].
One such local factor is the presence of foreign bodies (FBs) in the groin, as retained broken needle segments are unfortunately very common in this patient population. In a review by Norfolk and Gray [23], up to 20% of PWID reported breaking needles while injecting; this undoubtedly poses a risk to the operating team. It is noteworthy that the incidental finding of a FB on imaging performed during diagnostic workup for other conditions is typically managed conservatively. Intervention and FB removal are usually reserved for cases involving sepsis or vascular involvement.
Surgical intervention is a key component of treatment in these cases, and clinical equipoise still exists. Generally, two strategies are employed: either ligation of the involved vessels and debridement of soft tissue infection without revascularisation or debridement with vascular reconstruction/revascularisation. From the discussion above, it can be observed that the PWID groin presents challenges due to extensive soft tissue involvement and the potential unavailability of autologous vein for use as a revascularisation conduit, often because of thrombosis or disease resulting from injection practices. In a meta-analysis by Singh and colleagues [24] comparing the outcomes of patients treated by ligation and debridement alone vs debridement and revascularisation found no difference in amputation (8.89% vs. 8.03%, odds ratio (OR): 0.74, 95% confidence interval (CI): 0.35–1.56, p = 0.42, 11 studies) or chronic limb threatening ischemia (21.5% vs. 12.4%, OR: 1.24, 95% CI: 0.35–4.38, p = 0.74, 9 studies) after ligation and debridement compared with excision and revascularization. There was, however a higher incidence of reintervention (24.7% vs. 10.6%, OR: 0.31, 95% CI: 0.16–0.62, p = 0.0009, 13 studies) and rebleeding (7.1% vs. 1.6%, OR: 0.61, 95% CI: 0.16–2.38, p = 0.48, 5 studies) after excision and revascularization compared with ligation alone. They concluded that debridement and ligation are a safe initial intervention strategy, though more robust data sets are needed in this cohort of patients.
PWID may present with pain and swelling to the limb as well as symptoms and
signs of systemic upset. The formation of deep venous thrombosis (DVT) in this
cohort is likely attributable to recurrent punctures of the femoral vein,
accompanied by the injection of irritant substances. This process induces
endothelial damage and activates local tissue factors [25].
In a retrospective study of over two hundred episodes of DVT presenting to a
tertiary hospital, Syed and Beeching [26] highlighted that in patients
Septic thrombophlebitis more commonly affects the large proximal veins in long-term frequent intravenous injectors. They are commonly diagnosed by CT (gas within the thrombus/venous wall enhancement) or duplex ultrasonography. Severe symptoms can include fever, chills, rigours, and a draining sinus, with potential complications such as septic pulmonary embolism, right-sided infective endocarditis, and local haemorrhage [27]. Despite the complex and often polymicrobial nature of these infections, a retrospective series by McCaughan and colleagues [28] reported an over 80% cure rate, which was independent of the duration of antimicrobial regimens.
PWID are at higher risk of other infectious processes, and respiratory symptoms resulting in presentation to the hospital are common. Septic pulmonary embolism (SPE) occurs when thrombi containing microorganisms enter the pulmonary vasculature, resulting in infarction and abscess formation. Common symptoms include fever, chest pain, and dyspnoea. Plain chest X-ray and CT scans show characteristic findings, including nodules, patchy infiltrates, cavities, and pleural effusion. Most cases exhibit two of these imaging manifestations simultaneously [29].
SPE is usually considered to originate from the right ventricular system. In keeping with this, previous work with PWID echocardiography showed that 87% of the vegetations in the SPE patients were tricuspid vegetations [29, 30]. Historically, infective endocarditis (IE) in this cohort of patients has special characteristics, namely, it affects younger patients, is usually community-acquired, right-sided native valve endocarditis that mostly involves the tricuspid valve, is most often caused by Staphylococcus aureus and is associated with high rates of human immunodeficiency virus (HIV) and hepatitis C coinfection [31, 32]. However, left-sided heart involvement does occur, with a multicentre prospective cohort study demonstrating left-sided valvular involvement in 53% of episodes, with 34% of these being solely left-sided IE [31].
It is well-established that PWID face considerable stigma from healthcare professionals, which significantly impacts their involvement in care [7]. In one series by Biancarelli et al. [33], experiences of dehumanisation in healthcare settings were common, with many participants perceiving that they had been treated unfairly or discriminated against due to their injection drug use. Empathy-based training for health professionals, through online modules or workshops, can reduce discriminatory attitudes. Others suggest that organisational support, such as role support, supervision, and the opportunity for early consultation with an expert, may enhance willingness and satisfaction when working with this patient group [34].
As healthcare professionals, we should aim to adequately engage this cohort of patients at each encounter in a move to limit missed opportunities and morbidity. A detailed non-judgmental history should be obtained from patients presenting with complaints in and around the groin. As aforementioned, a high index of suspicion is needed when a history of intravenous injection is obtained with pain, swelling, erythema or purulent/serosanguinous discharge.
On examination, there may be swelling to the groin, erythema to the injection site, a groin sinus (a sign of repeated injection to the groin), and the hip on the affected side may be held in flexion, a sign of psoas irritation and retroperitoneal extension of the infective/inflammatory component [22]. There may also be very few visual cues or findings on physical examination as to the severity of the underlying problem.
In every patient encounter with PWID and an antecedent history as described above, a full blood count, renal function and liver function tests, C-reactive protein, coagulation screen, and two sets of blood cultures should be regarded as baseline.
The opportunity should be taken at the initial blood draw or later during the in-hospital episode to discuss investigation for blood-borne viruses. PWID have higher rates of sexually transmissible infections, viral hepatitis, HIV infection, and tuberculosis compared to non-PWID [35].
Early cross-sectional imaging in the form of a contrast-enhanced CT angiogram should be obtained in PWID presenting with injection site pain, swelling, discharge or erythema. This will aid in an early and accurate diagnosis or exclusion of disease processes that require emergent surgical input [6]. NSTI, infected pseudoaneurysms and deep-seated abscesses can be adequately characterised within the groin and the surrounding tissues (retroperitoneal extension, presence of retained FB), which aids in preoperative planning [22].
Further imaging may be warranted, including chest X-ray, CT Pulmonary Angiogram/High-Resolution CT Thorax, to discern primary pulmonary infection and SPE. In patients with evidence of SPE, a new murmur or bacteraemia (esp. Staphylococcus aureus), a pragmatic approach may be to perform trans thoracic echocardiography (TTE) in the first instance. PWID tend to have right-sided infective endocarditis. A thorough assessment of the tricuspid valve can be conducted using TTE, given the anterior positioning of the valve and the substantial vegetations commonly found in right-sided infective endocarditis (IE). In the event of an inconclusive TTE, then a trans oesophageal echocardiogram may be warranted [36].
NSTIs in PWID are often polymicrobial [6], commonly implicated pathogens include Staphylococcus aureus, Streptococcus pyogenes, anaerobes (including Clostridia and Bacteroides) and Gram-negative aerobes.
Monomicrobial NSTIs are predominantly caused by Streptococcus pyogenes, Staphylococcus aureus, and Clostridium species, with the latter often linked to myonecrosis.
As such, the initial empirical antibiotic regimen chosen should provide activity against the above microflora and toxins. Most regions/hospitals have guidelines based on their local bacterial ecology; thus, an extensive list of antimicrobials lacks value (see Table 1, Ref. [37]). However, standard empiric therapy may include use of broad-spectrum beta-lactams (e.g., piperacillin tazobactam), aminoglycosides (e.g., gentamicin) and anti-Methicillin-Resistant Staphylococcus aureus (anti-MRSA) agents (e.g., vancomycin/daptomycin). High-dose Clindamycin has been shown to suppress toxin production by Streptococcus pyogenes and Staphylococcus aureus, and Clostridium spp. through inhibition of bacterial protein synthesis while also modulating cytokine (e.g., tumour necrosis factor [TNF]) production and thus should also be utilised empirically [38].
| Options for Therapy* | ||
| Source | MRSA unlikely | MRSA suspected |
| Uncomplicated skin and soft tissue infection (cellulitis or abscess), septic arthritis, or osteomyelitis†‡ | • Flucloxacillin/nafcillin 1–2 g 6 hourly IV or | • Vancomycin 15–20 mg/kg 12 hourly IV (adjust based on therapeutic monitoring) or |
| • Cefazolin 1–2 g 8 hourly IV or | ||
| • Ceftriaxone 2 g daily IV | • Daptomycin 6 mg/kg daily IV or | |
| Severe penicillin allergy: | • Linezolid 600 mg 12 hourly IV | |
| • Clindamycin 600 mg 8 hourly IV | When oral appropriate: | |
| When oral appropriate: | • Trimethoprim-sulfamethoxazole 960–1920 mg 12 hourly PO or | |
| • Flucloxacillin 1 g 6 hourly PO§ or | ||
| • Trimethoprim-sulfamethoxazole 960–1920 mg 12 hourly PO or | • Doxycycline 100 mg 12 hourly PO or | |
| • Doxycycline 100 mg 12 hourly PO or | • Linezolid 600 mg 12 hourly PO | |
| • Clindamycin 450 mg 8 hourly PO | ||
| Endovascular infection (endocarditis, septic thrombophlebitis or infected pseudoaneurysm)‡ | • Flucloxacillin/nafcillin 2 g 4–6 hourly IV | • Vancomycin 15–20 mg/kg 12 hourly IV (adjust based on therapeutic monitoring) and gentamicin 3 mg/kg daily IV or |
| Severe penicillin allergy: | ||
| • As per MRSA suspected | • Daptomycin 6–10 mg/kg daily IV | |
| Severely ill patient without obvious source or necrotising soft tissue infection (NSTI) | • Piperacillin-tazobactam 4.5 g 6 hourly IV or | As per non-MRSA but add: |
| • Meropenem 1–2 g 8 hourly IV or | • Vancomycin 15–20 mg/kg 12 hourly IV (adjust based on therapeutic monitoring) or • Daptomycin 6–10 mg/kg daily IV or • Linezolid 600 mg 12 hourly IV | |
| • Flucloxacillin/nafcillin 2 g 4–6 hourly IV, gentamicin 5–7 mg/kg IV (dosing based on therapeutic monitoring), and metronidazole 500 mg 8 hourly IV | ||
| • If NSTI add Clindamycin 900 mg 8 hourly IV to above | ||
| Severe penicillin allergy: | ||
| • Clindamycin 900 mg 8 hourly IV and either: | ||
| – Gentamicin 5–7 mg/kg IV (dosing based on therapeutic monitoring) or | ||
| – Ciprofloxacin 400 mg 8–12 hourly IV | ||
Note: * Empirical regimen should be based on local resistance patterns.
† Consider adding metronidazole if risk factors for anaerobic infection.
‡ If severely ill or deterioration despite initial empirical therapy, consider broadening therapy to ensure cover for MRSA, Gram-negatives and anaerobes (such as addition of vancomycin and either aminoglycoside, quinolone, or third/fourth generation cephalosporin with metronidazole).
§ Oral penicillins are not preferred for bone and joint infection as bone penetration is poor.
Reprinted with the permission from Stevenson et al. [37]. MRSA, Methicillin-Resistant Staphylococcus aureus; PO, per os (by mouth).
Antibiotics can be tailored based on pus and tissue samples obtained at the time of debridement, blood cultures and clinical progress of the patient.
For patients with complicated Staphylococcus aureus bacteraemia, a transition to oral antibiotics in those who have completed at least 10 days of effective IV antibiotic therapy with outpatient support is a potential alternative strategy [39]. The involvement of local microbiology and infectious diseases teams is essential, as each patient requires an individualised approach.
The diversity of infectious processes in PWID and their management can be complex due to various medical and social factors. The role of the multidisciplinary team cannot be understated, these teams may include surgical staff (vascular, general surgery, orthopaedics, plastic surgery), medical staff (infectious diseases, anaesthetics, psychiatry, general medicine), addictions liaison, pain management, social work and community care, tissue viability, nursing and peer support as well as the patient themselves to ensure an individualised approach and plan can be made. The list provided is not comprehensive, and their role will depend on patient needs and local hospital policies.
Each hospital admission should be viewed as an opportunity for the prevention of further morbidity in PWID.
Compared to the general population, PWID are at increased risk for acquiring and transmitting infectious diseases via bloodborne exposure, and they are at increased risk for sexual exposure to HIV and sexually transmitted diseases (STDs) [35]. In some series, concomitant infectious diseases are well documented.
Admission provides the ability to engage in appropriate counselling and screening, as these patients may have little contact with healthcare previously.
Upon obtaining positive results, patients should receive counselling regarding the advantages of promptly commencing therapy, particularly for hepatitis C and HIV infections.
There should be discussions surrounding safer injection techniques, such as injection site preparation and use of filters and sterile water, where possible, and use of sterile needles and syringes, including not reusing needles [35].
PWID may experience reduced stigma and judgment if the above discussions are addressed by appropriate members of the multidisciplinary team. The goal is to improve engagement with their current care and decrease the risk of future admissions due to injecting-related infections [40].
Groin presentations secondary to injecting drugs may present a diagnostic challenge to healthcare professionals. Clinician education surrounding presentation of PWID, having a high index of suspicion and early cross-sectional imaging will prevent delays in diagnosis and decrease morbidity and mortality. There, however, remains insufficient research in certain aspects of management in the PWID population. Current evidence relies heavily on retrospective studies. Prospective trials are needed to determine the best treatment for invasive infections in PWID. Moreover, further research incorporating patient observations and perceptions is necessary to examine the potential impacts of stigma.
• Globally, 13.9 million individuals inject drugs, with the United Kingdom, particularly Scotland, experiencing a notably high rate of drug use.
• People who inject drugs (PWID) have higher morbidity and mortality as compared to the general population.
• Groin presentations are common, frequently misdiagnosed and require a high index of suspicion to minimise morbidity.
• PWID experience stigma from healthcare staff, which may lead to suboptimal outcomes.
• A multidisciplinary team approach is required in the management of this patient group.
Not applicable.
JJ, SS and GG designed the work. JJ, SS and GG drafted the manuscript. All authors contributed to the important editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
Written consent obtained for anonymised clinical photography. The research was conducted in strict accordance with the ethical principles outlined in the Declaration of Helsinki.
Not applicable.
This research received no external funding.
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.