









 , Fatemeh Habibi Nameghi 2, Federico Giacobbe 3, Mehdi Eskandari 1,2, Alexandros Papachristidis 1,2, Kevin O’Gallagher 1,2, Philip MacCarthy 1,2, Jonathan Byrne 1,2, Max Baghai 4
, Fatemeh Habibi Nameghi 2, Federico Giacobbe 3, Mehdi Eskandari 1,2, Alexandros Papachristidis 1,2, Kevin O’Gallagher 1,2, Philip MacCarthy 1,2, Jonathan Byrne 1,2, Max Baghai 41 Department of Cardiology, King’s College Hospital, SE5 9RS London, UK
2 School of Cardiovascular and Metabolic Medicine & Sciences, King’s College London, SE5 9RS London, UK
3 Department of Cardiology, Royal Brompton Hospital, SW3 6NP London, UK
4 Department of Cardiothoracic Surgery, King’s College Hospital, SE5 9RS London, UK
Abstract
Valvular heart disease (VHD) affects millions worldwide and remains a major cause of morbidity and mortality, placing a substantial and growing burden on healthcare systems. Over the past two decades, transcatheter therapies have emerged to meet this challenge, transforming the management of aortic, mitral, and tricuspid valve disease. Initially developed for inoperable or high-risk surgical patients, procedures such as transcatheter aortic valve implantation (TAVI) and mitral transcatheter edge-to-edge repair (M-TEER) are now routinely offered across a broader risk spectrum. More recently, tricuspid therapies, including tricuspid transcatheter edge-to-edge repair (T-TEER) and transcatheter valve replacement (TTVR), have emerged to address a significant unmet clinical need. With transcatheter interventions becoming more widely available, clinicians across general and acute medical specialities are increasingly likely to encounter patients before and after these procedures. Familiarity with these therapies will support better decision-making and coordinated care. This review summarises the evolution of transcatheter valve therapy, its role alongside surgery, and the evidence supporting its use. Surgery remains the gold standard for younger or low-risk patients, particularly where long-term durability is essential. Transcatheter therapies now offer safe and effective treatment for older patients, including those with frailty or significant comorbidity, supported by landmark trials, which have demonstrated favourable clinical outcomes in carefully selected populations and underpinned guideline endorsement across risk categories. The importance of the multidisciplinary Heart Team is emphasised, ensuring treatment decisions reflect individual anatomy, comorbidity burden, life expectancy, and procedural risk. As device technology, imaging, and procedural expertise continue to advance, the integration of surgical and transcatheter approaches will support more individualised care and broaden access to definitive treatment for patients across the clinical spectrum.
Keywords
- heart valve diseases
- transcatheter aortic valve replacement
- mitral valve insufficiency
- tricuspid valve insufficiency
- cardiac surgical procedures
- heart valve prosthesis implantation
Transcatheter valve interventions have fundamentally transformed the management of valvular heart disease (VHD), emerging as a viable alternative to surgery for many patients requiring intervention [1]. These therapies were initially developed for individuals considered unsuitable for surgery. Transcatheter aortic valve implantation (TAVI) was the first major transcatheter therapy to be adopted at scale and is now the first-line treatment for many patients, including older individuals and those at intermediate or higher surgical risk. In well-resourced healthcare systems, transcatheter approaches have expanded treatment eligibility, increased procedural volumes, and enabled intervention in older, frailer patients with complex medical needs [2]. Without such therapies, many would remain limited to symptom control, as no pharmacological treatments exist to halt or reverse valve disease progression [3].
The rise of transcatheter therapies follows decades of surgical innovation. The introduction of cardiopulmonary bypass in the mid-20th century revolutionised cardiac surgery, enabling open-heart procedures for rheumatic valve disease, then the dominant pathology [4]. Surgical valve repair and replacement became standard care, supported by the development of mechanical and later bioprosthetic valves [5]. With improved living conditions and widespread access to antibiotics, rheumatic disease declined sharply in high-income countries [6]. Degenerative valve disease, driven by ageing populations, has since become the leading indication for intervention, followed increasingly by functional regurgitation secondary to left or right ventricular remodelling [7].
In present-day clinical practice, patients with VHD are often older, frailer, and affected by multiple comorbidities. These factors increase operative risk and frequently result in patients being deemed unsuitable for surgical intervention, even when the potential benefit could be lifesaving [2]. This treatment gap has encouraged the development of less invasive options, particularly catheter-based therapies, alongside advances in minimally invasive and robotic-assisted surgical techniques.
The success of TAVI in treating aortic stenosis (AS) has helped to catalyse transcatheter interventions for the other cardiac valves. Building on this platform, transcatheter edge-to-edge repair (TEER) has emerged as a leading therapy for mitral and tricuspid regurgitation, supported by advances in imaging, device technology, and procedural technique. Early success in high-risk populations has driven expansion into broader cohorts, with a growing body of evidence supporting safety and efficacy [8, 9, 10].
Today, transcatheter therapies are a core component of cardiovascular care. They are well established for patients deemed too high risk for surgery and are increasingly used in selected patients for whom surgery remains an option but who prefer a less invasive approach. This evolution reflects not only technical progress but also a broader reconsideration of how valvular heart disease may be managed across the surgical risk spectrum. Nonetheless, important uncertainties remain, including long-term device durability, optimal patient selection, and equitable access to treatment. Moreover, transcatheter approaches are less well developed for patients requiring multi-valve intervention or concomitant revascularisation, in which surgery continues to play a central role.
This review summarises the evolution of transcatheter valve therapy and its current role alongside surgery, drawing on evidence from landmark trials across aortic, mitral, and tricuspid valve disease. It highlights the central role of the multidisciplinary Heart Team, considers global trends in access, and looks ahead to the future of personalised valve care.
The mid-20th century marked a turning point in catheter-based cardiovascular care. In 1953, Dr Sven-Ivar Seldinger introduced the needle-guidewire technique, a breakthrough he attributed to a “severe attack of common sense”, which eliminated the need for surgical cutdowns and transformed vascular access [11].
Coronary angiography and ventriculography became routine during the 1960s and 1970s. In 1964, Dr Charles Dotter pioneered transluminal angioplasty, and over a decade later, Dr Andreas Grüntzig adapted the technique to the coronary arteries, performing the first successful percutaneous coronary intervention (PCI) [12, 13]. These advances formed the foundation of interventional cardiology.
While PCI transformed coronary care, no equivalent percutaneous option existed for structural heart disease, which continued to rely on surgery. For many high-risk patients, surgical intervention was either too hazardous or not feasible, highlighting the need for less invasive alternatives. Over time, the same technologies that enabled PCI, including catheter design, balloon-expandable devices, imaging, and vascular access, formed the technical base for transcatheter valve therapies.
Key early milestones followed in the 1980s. In 1982, Dr Kanji Inoue performed the first percutaneous balloon mitral valvuloplasty (PBMV) to treat rheumatic mitral stenosis, demonstrating for the first time that structural valve disease could be treated with catheter-based techniques [14] (Fig. 1). Remarkably, PBMV remains recommended in current guidelines for the treatment of rheumatic mitral stenosis in selected cases. In 1985, Dr Alain Cribier adapted this technique, performing the first balloon aortic valvuloplasty (BAV) for severe AS [15]. While limited by high rates of restenosis and aortic regurgitation, BAV offered a lifeline to patients too unwell for surgery and demonstrated that percutaneous treatment of the aortic valve was feasible. This landmark proof-of-concept laid the groundwork for TAVI and remains in use today as a bridge to definitive intervention in critically unwell patients [16].
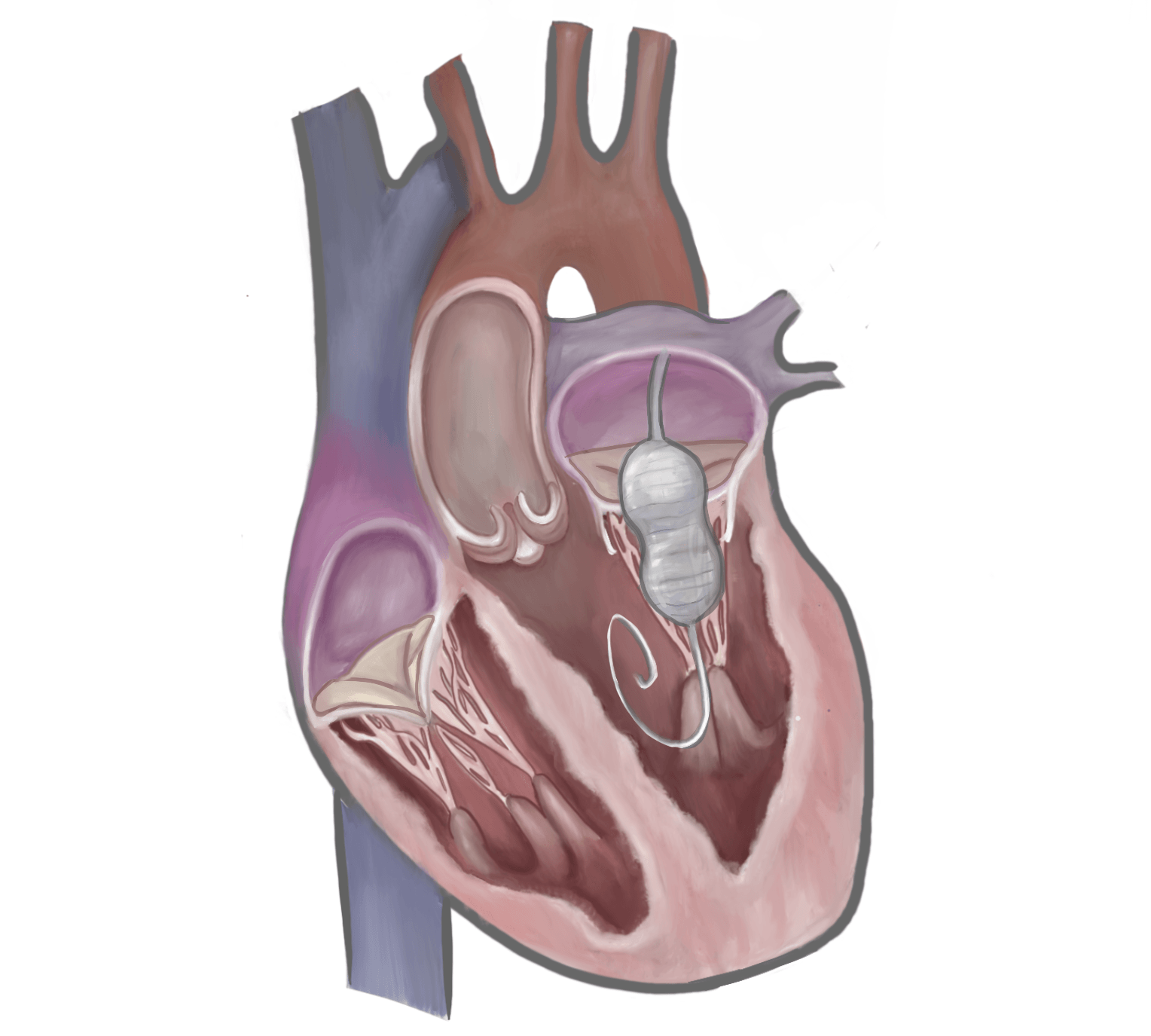 Fig. 1.
Fig. 1.
Percutaneous balloon mitral valvuloplasty. The procedure begins with catheter insertion via the femoral vein, advancing into the right atrium. Through the transseptal puncture, a guidewire and catheter are advanced into the left atrium. The balloon is then positioned across the mitral valve and inflated, splitting the fused commissures and relieving the stenosis. Original illustration created using Procreate version 5.4 for iPad (Savage Interactive Pty Ltd., Hobart, TAS, Australia).
Although transcatheter valve therapy is most commonly associated with the aortic position, the first human transcatheter valve implantation was performed in the right ventricular outflow tract. In 2000, Dr Philipp Bonhoeffer [17] implanted a transcatheter pulmonary valve (the Melody valve) to treat a dysfunctional right ventricle–to–pulmonary artery conduit. This was followed in 2002 by Dr Alain Cribier [18], who performed the first successful transcatheter aortic valve implantation in a patient with severe calcific aortic stenosis, a milestone that catalysed the modern era of structural heart intervention (Fig. 2).
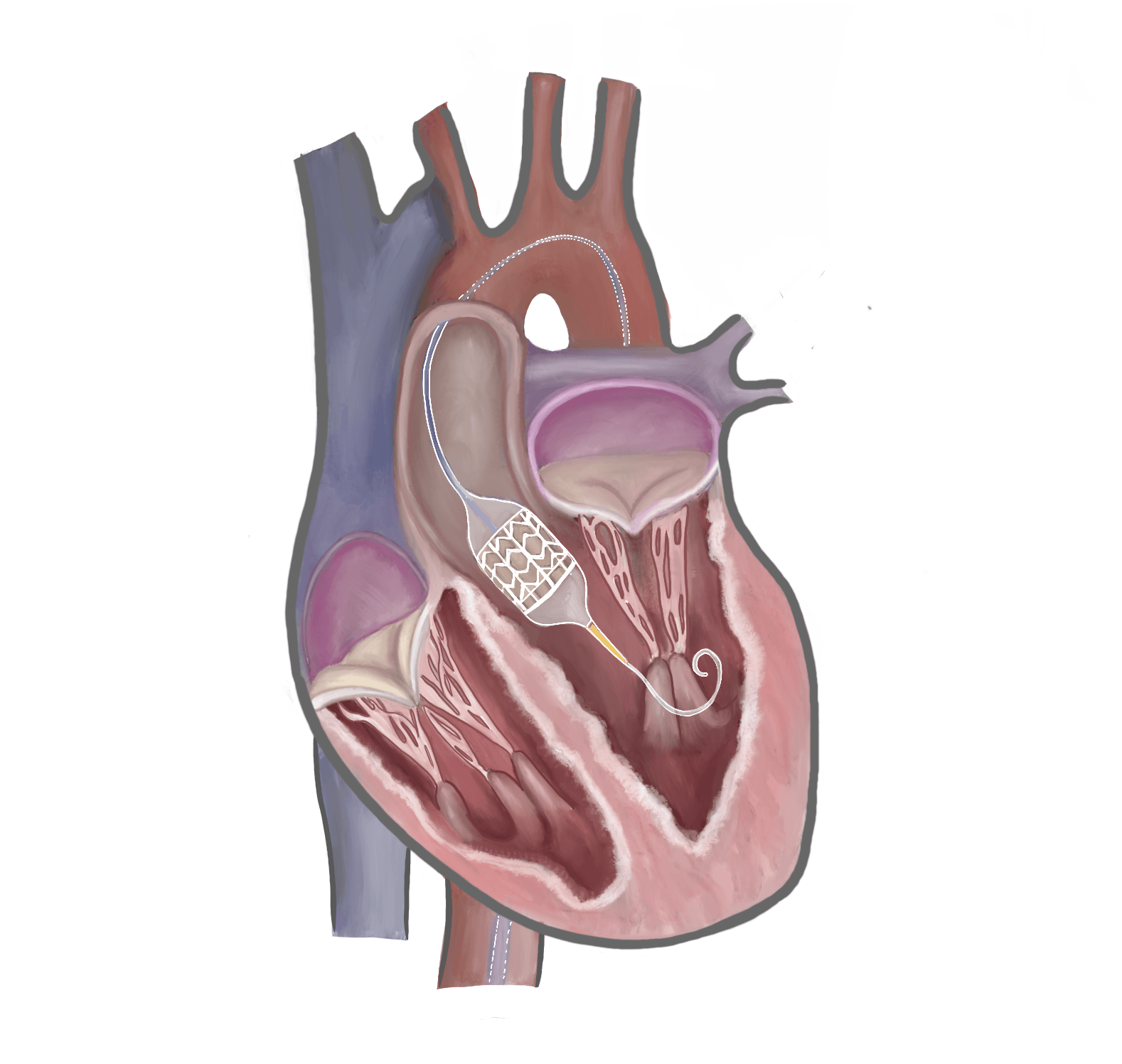 Fig. 2.
Fig. 2.
Transcatheter aortic valve implantation (TAVI). A transcatheter aortic valve prosthesis is shown deployed within the native aortic valve via a retrograde femoral arterial approach. This minimally invasive technique allows valve replacement without open-heart surgery. Original illustration created using Procreate version 5.4 for iPad (Savage Interactive Pty Ltd., Hobart, TAS, Australia).
AS became a natural entry point for transcatheter approaches due to its high prevalence in older populations, its relatively straightforward anatomy for catheter-based intervention, and the poor prognosis of untreated disease. Severe symptomatic AS leads to progressive left ventricular dysfunction, heart failure, and death, often within months if left untreated. One-year survival is estimated at around 50–60%, with five-year survival as low as 20%, a prognosis worse than many common cancers and comparable to severe left ventricular systolic dysfunction [19].
Historically, a substantial proportion of elderly patients with symptomatic severe AS were deemed unsuitable for surgical intervention because of advanced age, frailty, or comorbidity. The Euro Heart Survey demonstrated that approximately one-third of patients fell into this category and were consequently denied definitive valve treatment [20].
Transcatheter aortic valve implantation (TAVI) was developed in direct response to this unmet need and has markedly expanded treatment eligibility. Contemporary UK modelling suggests that approximately 62% of patients previously considered unsuitable for conventional surgery would now be eligible for transcatheter intervention [21].
However, expanded eligibility has not translated into universal treatment. Contemporary US data indicate that only 61% of patients with severe AS undergo valve intervention within four years of diagnosis, despite clear guideline indications [22]. As populations age and multimorbidity increases, this persistent gap between eligibility and delivery represents a central challenge for modern valve services [23].
Nonetheless, following Dr Alain Cribier’s landmark 2002 procedure, TAVI has become the most performed intervention for AS in well-developed health systems, supported by strong guideline recommendations and extensive evidence (Fig. 3, Ref. [24, 25, 26, 27]).
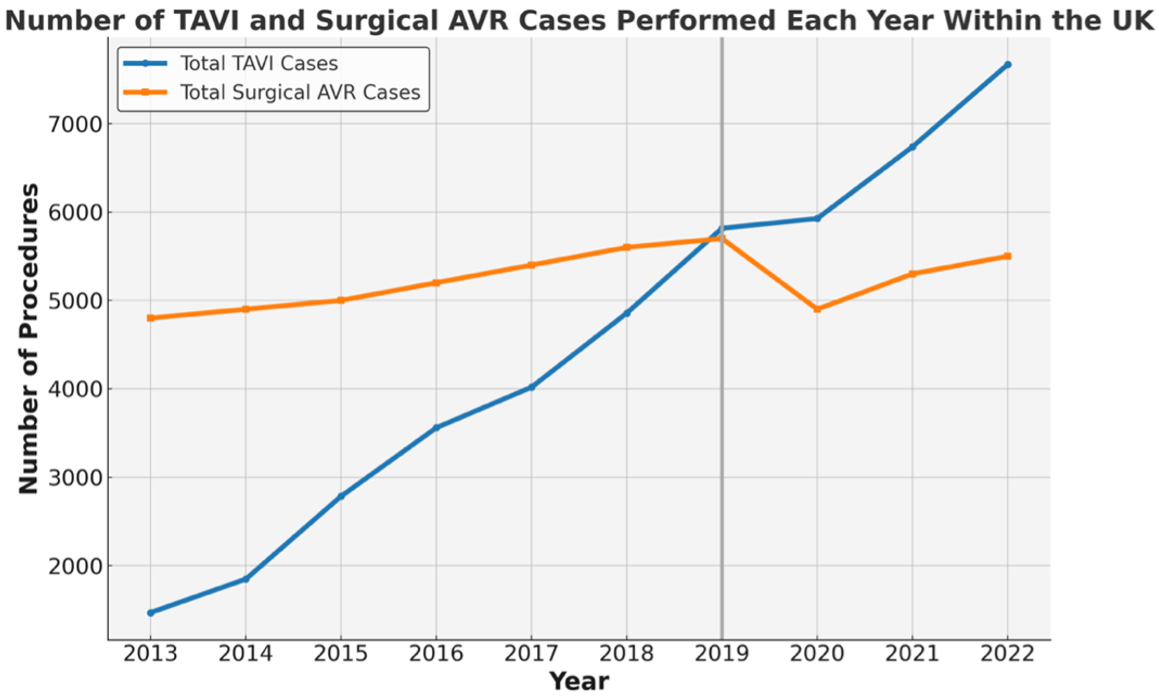 Fig. 3.
Fig. 3.
Annual transcatheter aortic valve implantation (TAVI) and surgical aortic valve replacement (SAVR) procedures in the UK (2013–2022). Data derived from the National Institute for Cardiovascular Outcomes Research (NICOR) [24, 25, 26, 27]. Chart created using Microsoft Excel for Mac version 16.103.3 (Microsoft Corporation, Redmond, WA, USA).
Modern TAVI is typically performed via transfemoral access under local anaesthesia and conscious sedation. This avoids the need for sternotomy, cardiopulmonary bypass and general anaesthesia, significantly reducing procedural invasiveness. Pre-procedural computed tomography (CT) imaging allows accurate valve sizing, vascular planning, and assessment of the coronary arteries to evaluate the risk of coronary obstruction. Procedural guidance is primarily fluoroscopic, often supplemented by transthoracic echocardiography (TTE). A wide range of transcatheter valves is now available, including balloon-expandable and self-expanding systems, with designs that incorporate features such as outer skirts and repositionability to reduce paravalvular leak. Advances in lower-profile delivery systems, ultrasound-guided femoral access, and percutaneous closure devices have significantly reduced vascular complications. In early series using first-generation devices, major vascular complication rates of 12–20% were reported [28]. With these improvements and greater operator experience, contemporary rates have fallen to 4–6% in recent trials and below 2% at high-volume centres using optimised closure protocols [29].
Many centres now use simplified protocols with early mobilisation and discharge, enabling return to normal activities within one to two weeks. Most patients are mobilised within hours, with up to 75% discharged within 24 hours [30]. Same-day discharge has also been shown to be feasible and safe in carefully selected low-risk patients [31]. These streamlined pathways reduce the risk of hospital-acquired complications such as infection, delirium or deconditioning, which are especially relevant in older or frail individuals [31].
Pivotal trials including Placement of Aortic Transcatheter Valves (PARTNER) I, II and III, Surgical Replacement and Transcatheter Aortic Valve Implantation (SURTAVI), and Evolut Low Risk have shown that, in carefully selected patients, TAVI is non-inferior to surgical aortic valve replacement (SAVR) at short- to mid-term follow-up. However, this evidence should not be extrapolated to younger, fit patients with long life expectancy, in whom long-term durability remains uncertain and SAVR therefore remains preferred in current guidelines. An important exception includes younger patients with significant multimorbidity or limited physiological reserve, in whom transcatheter approaches may still offer a more appropriate risk–benefit profile [2, 28, 29, 32, 33, 34].
The strength of this evidence has driven a progressive expansion of regulatory approvals. TAVI was first approved in Europe in 2007 and in the USA in 2011, initially for patients at high surgical risk. As evidence from PARTNER II and SURTAVI accumulated, indications extended to intermediate-risk patients in 2016. By 2019, following the landmark PARTNER III and Evolut Low Risk trials, approval expanded to selected low-risk populations in both Europe and the USA. Procedural volumes have increased significantly since, with TAVI now performed more frequently than SAVR in many developed health systems.
This evidence has also shaped contemporary guideline recommendations. The 2021 European Society of Cardiology/European Association for Cardio-Thoracic Surgery (ESC/EACTS) guidelines recommend TAVI for symptomatic patients aged 75 and older or those at elevated surgical risk, while SAVR remains preferred for patients under 75, particularly where mechanical valves or long-term durability are priorities [1]. The 2020 American College of Cardiology/American Heart Association (ACC/AHA) guidelines similarly advise TAVI in patients aged 65 and older or those with limited life expectancy, and favour SAVR in younger individuals, especially those expected to live beyond 20 years [3]. For patients in the intermediate age range, treatment selection is individualised. European guidance defines this group as those aged 70–75 years, while US guidelines recommend shared decision-making for patients aged 65–80 years. In both frameworks, the choice between TAVI and SAVR should be guided by Heart Team assessment and patient-specific factors, including anatomy, comorbidity burden, life expectancy, and procedural feasibility.
Rather than displacing surgery, the expansion of TAVI has increased the total number of patients receiving treatment for severe aortic stenosis (Fig. 3). TAVI volumes have risen steadily, surpassing SAVR for the first time in 2019, while surgical volumes have, overall, remained stable, with a transient decline during the Coronavirus Disease 2019 (COVID-19) pandemic [24, 25]. Patient selection is increasingly nuanced and relies on multidisciplinary Heart Team assessment of anatomy, valve morphology, long-term reintervention strategy and patient preference.
Despite its minimally invasive nature, TAVI is not without complications. These include paravalvular leak, stroke, and conduction abnormalities requiring permanent pacemaker implantation [35]. Pacemaker rates vary by valve type, with self-expanding systems associated with higher rates (15–25%) than balloon-expandable devices (6–10%), though overall rates have declined with newer-generation valves and refined implantation techniques [36]. This remains an important consideration, particularly in younger patients. Nevertheless, complication rates overall have declined over time due to better patient selection, improved operator experience, and iterative device enhancements [35].
BAV retains a limited role in contemporary practice, primarily as a bridge to definitive intervention in haemodynamically unstable patients requiring urgent stabilisation before TAVI or surgery [37].
While TAVI is now well established for the treatment of calcific AS, several challenges remain in expanding its use to other aortic valve pathologies. Pure aortic regurgitation (AR) is one such challenge, where the absence of annular calcification and larger annular dimensions make valve anchoring more difficult, increasing the risk of device migration or paravalvular leak [38]. Surgical valve replacement remains the standard of care for severe AR [1]. However, as with AS, many patients are unsuitable for surgery due to advanced age, frailty, or comorbidities. Newer transcatheter devices, such as the Trilogy Transcatheter Heart Valve System (JenaValve Technology, Irvine, CA, USA) and the J-Valve transfemoral transcatheter aortic valve replacement system (Genesis MedTech / Suzhou Jiecheng Medical Technology Co., Ltd., Suzhou, China), have been specifically designed to overcome these challenges [39]. These devices have recently gained regulatory approval for use in patients unsuitable for surgery, with the ALIGN-AR pivotal trial demonstrating promising technical success and acceptable early safety outcomes with the JenaValve Trilogy system [40]. Further data from ongoing trials will inform broader adoption of this approach.
Bicuspid aortic valve disease poses additional anatomical challenges, including elliptical annuli, asymmetric leaflet calcification, and associated aortopathy. These factors can impede uniform expansion and sealing of transcatheter valves, leading to increased risk of paravalvular regurgitation or device malposition [41]. SAVR remains the preferred option for many patients with bicuspid morphology, particularly the young. However, in older or high-risk individuals with favourable anatomy, TAVI is increasingly being considered. Outcomes with newer-generation valves are encouraging, though long-term durability data remain limited in this subgroup [42].
Valve-in-valve (ViV) TAVI is now a widely adopted option for patients with structural degeneration of bioprosthetic valves, whether surgical and transcatheter. By implanting a new transcatheter valve within the failing prosthesis, ViV procedures offer a less invasive alternative to redo sternotomy. This approach is particularly useful in high-risk patients but comes with important technical considerations, including valve sizing, risk of coronary obstruction, and potential for elevated gradients. Notably, if the initial prosthesis is small or implanted too high, future reinterventions may become more difficult or impossible [43].
These challenges have brought increasing attention to the concept of lifetime valve management. In patients with longer life expectancy, it is essential to plan not just for the initial valve procedure, but also for the likely need for future intervention. For many patients, this will involve a future transcatheter implantation rather than surgery, making it critical to optimise the first intervention. Careful attention to valve type, size, positioning, and coronary access can preserve future treatment options and minimise procedural risk. As early TAVI and SAVR recipients begin to outlive their original bioprosthesis, forward planning is becoming central to long-term success [44].
Surgical techniques have advanced in parallel with transcatheter therapies, following separate but complementary paths. Minimally invasive SAVR, typically via partial upper sternotomy or right anterior thoracotomy, has become increasingly common. Although cardiopulmonary bypass is still required, these approaches are associated with reduced bleeding, shorter hospital stays, and faster recovery compared to full sternotomy [45]. They are best suited to patients with favourable anatomy and those opting for bioprosthetic valves, although mechanical valves can also be implanted using these techniques.
There has been a growing shift towards bioprosthetic valves in surgical practice, driven by an ageing patient population and the possibility of future valve-in-valve TAVI. However, mechanical valves remain preferred in younger patients who can tolerate long-term anticoagulation. Unlike bioprosthetic valves, mechanical valves cannot be treated with valve-in-valve TAVI but offer superior long-term durability, making them the valve of choice when longevity is the priority.
Alongside these trends, the proportion of patients undergoing complex surgery has increased. More than 40% of contemporary SAVR procedures now involve complex surgery, including reoperations, multi-valve intervention, or concomitant coronary artery bypass graft (CABG), up from less than 30% a decade ago [46]. This evolution is reflected in national registry data (Fig. 4, Ref. [25, 26, 27, 47]), which shows rising complexity and declining mechanical valve use.
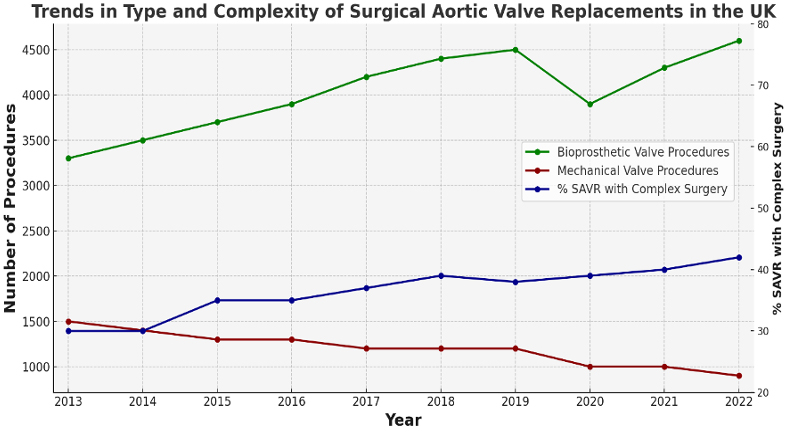 Fig. 4.
Fig. 4.
Trends in type and complexity of surgical aortic valve replacements (SAVR) in the UK (2013–2022). Bioprosthetic valve use has increased overall, while mechanical valve procedures have declined. The proportion of SAVR cases involving complex surgery has also risen over time, now accounting for over 40% of cases. Data from [25, 26, 27, 47]. Chart created using Microsoft Excel for Mac version 16.103.3 (Microsoft Corporation, Redmond, WA, USA).
Surgery offers unique advantages, including the ability to excise the native valve, perform annular enlargement, implant mechanical prostheses, and address multiple valves or concomitant revascularisation in a single procedure. It also avoids the risk of limiting future coronary access, which can occur with some transcatheter valves. These features are particularly valuable in younger patients or those with complex anatomy.
Emergency conversion from TAVI to open-heart surgery is rare, occurring in approximately 1.3% of cases [47, 48]. This may be required for complications such as annular rupture, severe aortic regurgitation, coronary obstruction, or device embolisation. It remains one of the most technically demanding scenarios in structural heart intervention and reinforces the need for close collaboration between interventional and surgical teams. As TAVI volumes continue to rise, surgical intervention for late complications is also becoming more common. When transcatheter options such as valve-in-valve TAVI are not feasible, SAVR may be required to manage structural valve deterioration or severe paravalvular regurgitation. Surgery is also indicated for infective endocarditis, where transcatheter approaches have no established role. Although still relatively uncommon, TAVI valve explantation is technically challenging, with reported in-hospital mortality ranging from 10–15% in contemporary series [49].
TAVI has transformed the treatment of AS, while SAVR remains essential for younger patients, those requiring mechanical valves and complex cases. Current guidelines support an age- and risk-based approach to intervention (Table 1, Ref. [1, 3]), with final treatment decisions guided by life expectancy, procedural feasibility, anatomical suitability, and Heart Team input.
| Clinical scenario | ESC/EACTS 2021 | ACC/AHA 2020 |
| TAVI vs SAVR: Age and risk | TAVI: |
TAVI: |
| Bicuspid AS | SAVR preferred; TAVI off-label, but may be considered in selected older patients or those at high surgical risk | SAVR preferred; TAVI off-label, but may be considered in high surgical risk cases |
| Asymptomatic severe AS | Intervention indicated (TAVI or SAVR) if LVEF |
Intervention indicated (TAVI or SAVR) if LVEF |
| Prosthesis (SAVR) | Individualised; mechanical valve if younger | Mechanical valve preferred if |
| Aortic regurgitation (AR) | SAVR preferred if symptomatic or if LV dysfunction is present. TAVI off-label, but may be considered in high-risk or inoperable patients | Similar to ESC/EACTS; TAVI off-label, considered mainly in trial settings or selected high-risk patients |
Abbreviations: ACC, American College of Cardiology; AHA, American Heart Association; AS, aortic stenosis; ESC, European Society of Cardiology; EACTS, European Association for Cardio-Thoracic Surgery; LV, left ventricle; LVEF, left ventricular ejection fraction; SAVR, surgical aortic valve replacement; TAVI, transcatheter aortic valve implantation.
As TAVI expands into lower-risk populations, where patients may outlive their first valve intervention, lifetime valve management has become a central consideration. Initial treatment decisions must take into consideration durability, reintervention options, and coronary access. Innovations in valve design, imaging, and procedural planning, combined with equitable access and multidisciplinary care, will shape the next era of aortic valve therapy.
Mitral regurgitation (MR) is the most common form of valvular heart disease in developed countries, particularly among older adults [20]. Unlike the relatively static semilunar valves of the aortic and pulmonary positions, the mitral and tricuspid valves are dynamic atrioventricular valves whose function depends on the geometry and contractility of the chambers they separate.
In the mitral position, close coupling to the left ventricle and, to a lesser extent, the left atrium means that structural or functional changes in either chamber can disturb valve function. Ventricular remodelling may tether the leaflets or restrict their motion, while atrial enlargement can cause annular dilatation and loss of coaptation. These mechanisms, alone or in combination, can lead to regurgitation. This anatomical dependence makes the mitral valve susceptible to a wider range of pathologies than the aortic valve and adds to the technical challenges of repair or replacement.
Surgical mitral valve repair remains the standard of care for severe symptomatic primary MR, offering excellent long-term outcomes in experienced centres. In 1960, Nina Starr Braunwald performed the first successful mitral valve replacement, marking a landmark in cardiac surgery and highlighting the role of women in the speciality [50].
In the 1970s and 1980s, Alain Carpentier pioneered repair techniques centred on leaflet preservation and restoration of normal anatomy [51]. These advances established repair, rather than replacement, as the preferred strategy in suitable patients. However, many patients are elderly or have comorbidities that preclude open-heart surgery, creating a clear role for transcatheter approaches.
The dominant transcatheter approach to MR is mitral transcatheter edge-to-edge repair (M-TEER), an adaptation of the surgical Alfieri stitch first described in the 1990s by Ottavio Alfieri. In its original form, the technique approximated the anterior and posterior leaflets with a central suture to create a double orifice and improve coaptation [52] (Fig. 5).
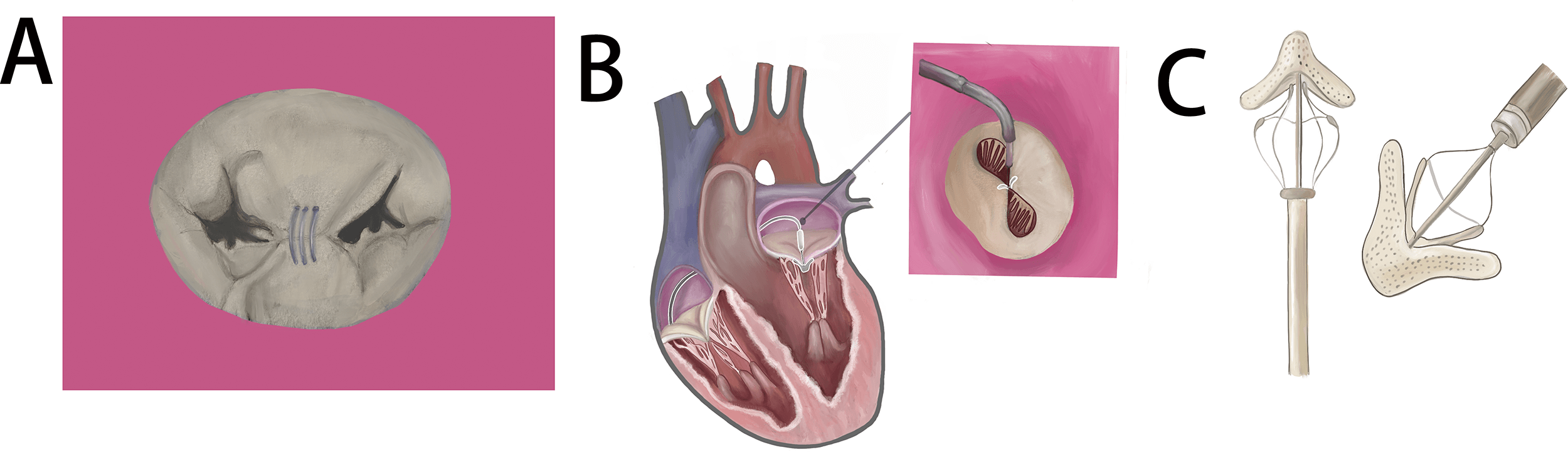 Fig. 5.
Fig. 5.
Mitral transcatheter edge-to-edge repair: from surgical concept to percutaneous technique. (A) Schematic of the surgical Alfieri stitch, which approximates the anterior and posterior mitral leaflets with a central suture. (B) Mitral transcatheter edge-to-edge repair (M-TEER) using a clip-like device to create a similar double-orifice valve configuration. (C) Example of an edge-to-edge device used for both mitral and tricuspid valve procedures. Original illustration created using Procreate version 5.4 for iPad (Savage Interactive Pty Ltd., Hobart, TAS, Australia).
M-TEER devices include the MitraClip G4/G5 system (Abbott Vascular, Santa Clara, CA, USA) and the PASCAL Precision system (Edwards Lifesciences LLC, Irvine, CA, USA). These devices replicate the surgical Alfieri stitch using a clip-based mechanism delivered via transfemoral venous access with transseptal puncture. The first human M-TEER procedure was performed in 2003, and the safety and efficacy of the MitraClip system were subsequently evaluated in the Endovascular Valve Edge-to-Edge Repair Study (EVEREST) I and II trials [53, 54, 55]. These studies demonstrated that M-TEER was feasible in both primary and secondary MR, with lower rates of periprocedural complications than surgery. However, M-TEER was less effective at eliminating MR, and reintervention rates were higher, largely because of residual or recurrent regurgitation. These findings formed the basis for regulatory approval in high-risk patients.
Evidence has since expanded in both primary and secondary MR. In secondary MR, the Cardiovascular Outcomes Assessment of the MitraClip Percutaneous Therapy for Heart Failure Patients with Functional Mitral Regurgitation (COAPT) trial demonstrated substantial reductions in heart failure hospitalisations and improved survival in carefully selected patients, whereas the Percutaneous Repair with the MitraClip Device for Severe Functional/Secondary Mitral Regurgitation (MITRA-FR) trial, which used broader enrolment criteria, showed no significant benefit [56, 57]. These contrasting findings highlight the importance of patient selection, particularly the severity of MR relative to the degree of left ventricular dilatation. More recent studies, including the Percutaneous Repair of Moderate-to-Severe or Severe Functional Mitral Regurgitation in Symptomatic Heart Failure Patients (RESHAPE-HF2) trial and the A Multicenter, Randomized, Controlled Study to Assess Mitral Valve Reconstruction for Advanced Insufficiency of Functional or Ischemic Origin (MATTERHORN) trial, have broadly supported the benefits observed in COAPT, although longer-term durability data are still needed [58, 59].
Procedural success depends on favourable anatomy, including adequate leaflet length for device grasping, minimal calcification, and limited annular dilation. Most M-TEER procedures are performed under general anaesthesia with combined fluoroscopic and transoesophageal echocardiographic (TOE) guidance to ensure accurate device positioning. Procedures typically last 1.5 to 2 hours, and recovery is usually rapid, with many patients discharged the following day.
M-TEER is generally safe and well-tolerated. Major complications occur in fewer than 5% of cases and include device embolisation, single leaflet device attachment (SLDA), and iatrogenic mitral stenosis from excessive leaflet restriction [60]. Vascular and transseptal-related complications are uncommon. Importantly, contemporary devices are fully retrievable until final deployment, allowing repositioning or removal if initial placement is suboptimal. If M-TEER is unsuccessful or SLDA occurs, surgical repair or replacement remains feasible, either with the device in situ or following retrieval. This safety profile, combined with rapid recovery and short hospital stays, has supported the broader adoption of M-TEER in clinical practice.
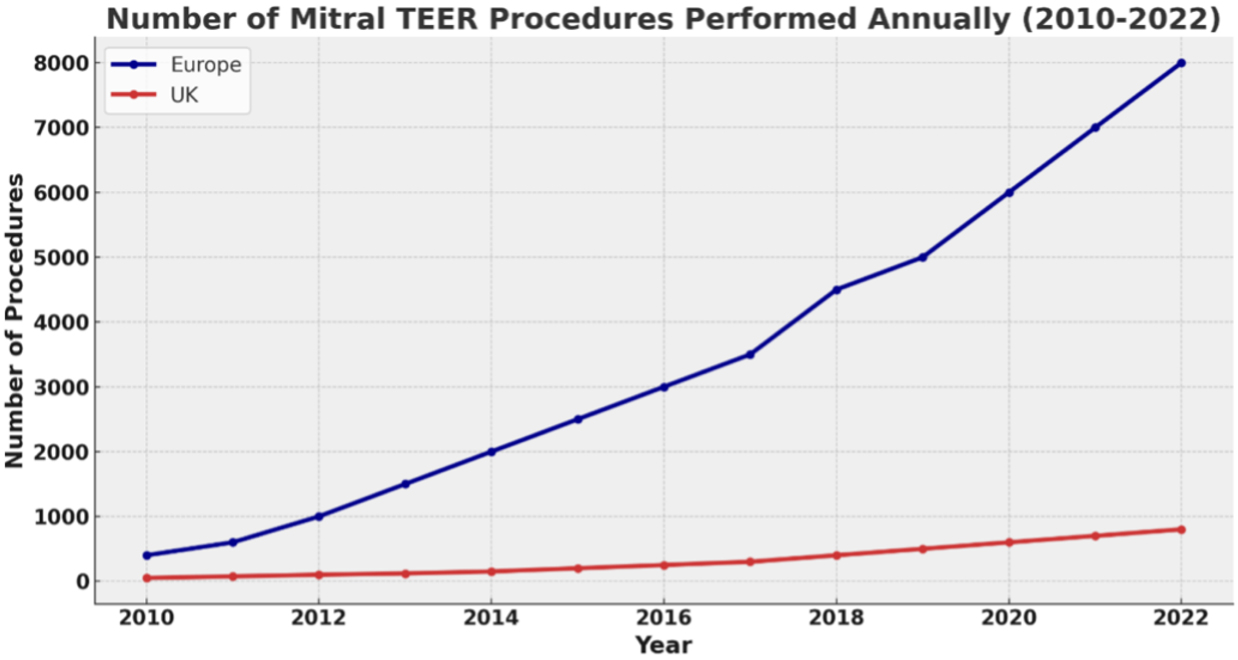
Access to M-TEER has expanded significantly across Europe, driven by guideline endorsement and growing operator experience. Procedure volumes have risen sharply over the past decade, with particularly high adoption in Germany, the Netherlands, and Switzerland. The USA is also performing a large and growing number of procedures following US Food and Drug Administration (FDA) approval in 2013. In the UK, uptake was historically constrained by delayed commissioning, and rates remain substantially lower than in many comparable countries, though they continue to increase (Fig. 6, Ref. [61, 62]). These patterns reflect both the growing evidence base and the gradual integration of M-TEER into routine clinical pathways for appropriately selected patients.
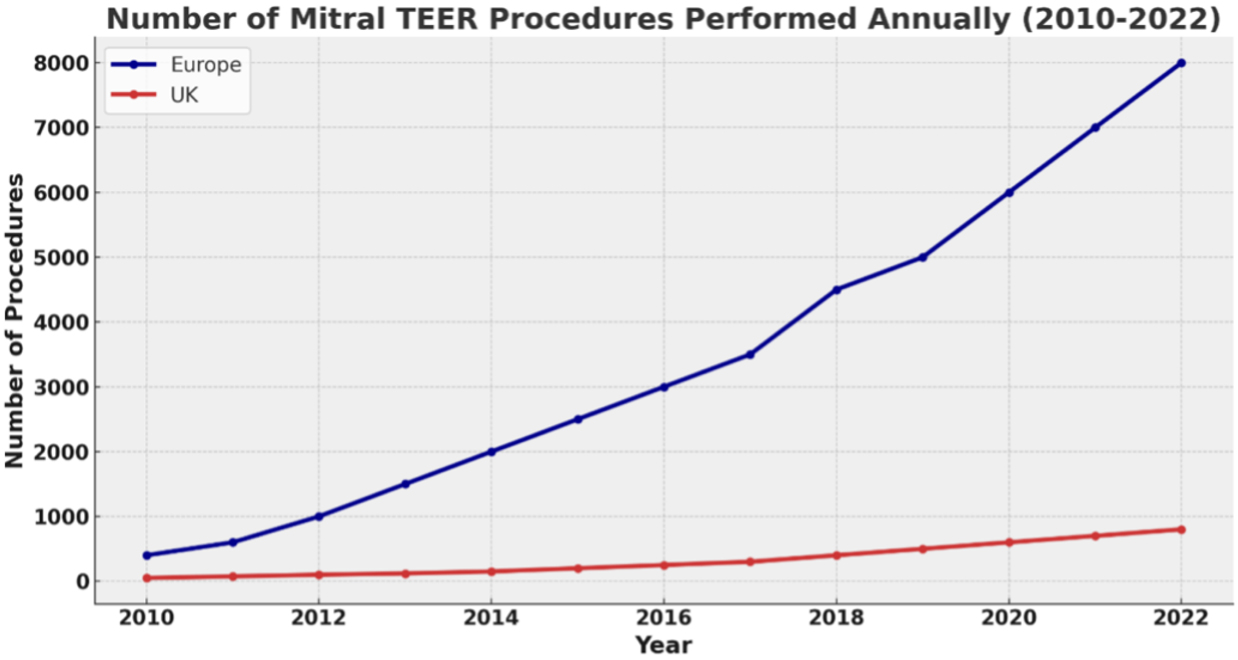 Fig. 6.
Fig. 6.
Number of mitral TEER procedures performed annually in Europe and the UK (2010–2022). The adoption of transcatheter edge-to-edge repair (TEER) for mitral regurgitation has increased markedly across Europe over the past decade, with more modest but steady growth observed in the UK. Data from [61, 62]. Chart created using Microsoft Excel for Mac version 16.103.3 (Microsoft Corporation, Redmond, WA, USA).
TMVR is a transcatheter procedure that offers a potential solution for patients with severe MR who are unsuitable for surgery or M-TEER. It is most often considered when repair is unlikely to achieve a durable result, such as in cases with extensive leaflet pathology, severe annular calcification, large coaptation gaps, or recurrent MR after previous surgical intervention. In these settings, complete valve replacement offers the prospect of eliminating regurgitation, whereas M-TEER would be technically challenging or predictably ineffective.
Unlike M-TEER, which preserves the native valve, TMVR involves complete replacement with a bioprosthetic device, aiming for definitive elimination of MR. However, the procedure is technically demanding due to the mitral valve’s large orifice, D-shaped annulus, and proximity to the left ventricular outflow tract (LVOT), which increases the risk of obstruction. Anatomical incompatibility remains the main barrier, with 60–80% of screened patients excluded because of unfavourable annular dimensions, LVOT obstruction risk, or limitations in vascular access [63].
In the UK, TMVR is currently reserved for highly selected high-risk patients, usually within clinical trials or under compassionate-use approval, and overall experience remains limited. The Tendyne Transcatheter Mitral Valve System (Abbott, Santa Clara, CA, USA), delivered via a transapical approach and repositionable before release, has generated the greatest UK experience to date, with early studies demonstrating high procedural success and symptomatic improvement [64]. The SAPIEN M3 Transcatheter Mitral Valve Replacement System (Edwards Lifesciences LLC, Irvine, CA, USA) and the Cardiovalve transfemoral mitral valve replacement system (Venus Medtech IL, Or Yehuda, Israel), both fully percutaneous transfemoral platforms, are at an earlier stage of evaluation in the UK, with only a small number of cases performed. While transfemoral delivery has the potential to shorten recovery compared with transapical access, clinical experience remains relatively early and limited to selected centres, and the absence of long-term durability data continues to constrain wider adoption.
Other transcatheter repair strategies are also emerging. The NeoChord DS1000 Artificial Chordae Delivery System (NeoChord, Inc., Maple Grove, MN, USA) is a beating-heart transcatheter procedure performed via a transapical approach, in which artificial chordae are implanted to restore leaflet coaptation without the need for cardiopulmonary bypass [65]. It is generally reserved for degenerative MR with isolated leaflet prolapse and is not yet widely available in the UK. Observational series, including the NeoChord International Registry, have reported promising early outcomes, although long-term results and comparative trial data are still awaited.
Early feasibility studies of TMVR have shown encouraging rates of acute MR elimination, but important challenges remain. These include large delivery systems, vascular access constraints, the risk of LVOT obstruction, high anatomical screening failure rates, the potential for acute left ventricular dysfunction, and the lack of long-term durability data. Ongoing trials will help define its role relative to surgery and M-TEER, particularly in determining whether its use can be expanded to intermediate-risk populations.
MS is now relatively uncommon in higher-income countries due to the decline in rheumatic fever. In suitable patients, particularly younger individuals with pliable, non-calcified valves, percutaneous balloon mitral valvuloplasty (PBMV) remains the preferred first-line treatment [1]. For most others who are unsuitable for PBMV, surgery is almost always required, typically valve replacement rather than repair, as repair is rarely feasible in the presence of extensive calcification and advanced pathological changes.
M-TEER has no role in MS, as it is designed to treat regurgitation rather than stenosis and would further impede valve opening. TMVR is technically possible but has only a very limited role due to the high rate of anatomical incompatibility. In MS, this is further compounded by heavy calcification, complex subvalvular disease, and frequent multi-valve involvement, meaning the procedure is feasible only in highly exceptional cases. Current guideline recommendations for mitral valve disease are summarised in Table 2 (Ref. [1, 3]).
| Clinical scenario | ESC/EACTS 2021 | ACC/AHA 2020 |
| Primary MR: Surgery vs TEER | Surgery preferred; M-TEER in high-risk patients | Surgery preferred; M-TEER reasonable in high-risk patients |
| Secondary MR: Surgery vs TEER | M-TEER recommended if suitable anatomy; surgery if concomitant cardiac surgery required | M-TEER recommended if suitable anatomy; surgery if concomitant cardiac surgery required |
| Surgical risk | M-TEER if high surgical risk | M-TEER if high surgical risk |
| Asymptomatic severe MR | Surgery if LVEF |
Surgery if LVEF 30–60%, LVESD |
| Mitral stenosis | PBMV preferred if suitable; surgery if not | PBMV preferred if suitable; surgery if not |
| Prosthesis (Mitral) | Individualised; mechanical in younger patients | Mechanical preferred |
Abbreviations: ACC, American College of Cardiology; AHA, American Heart Association; AF, atrial fibrillation; ESC, European Society of Cardiology; EACTS, European Association for Cardio-Thoracic Surgery; LVESD, left ventricular end-systolic diameter; LVEF, left ventricular ejection fraction; M-TEER, mitral transcatheter edge-to-edge repair; MR, mitral regurgitation; PBMV, percutaneous balloon mitral valvuloplasty.
While transcatheter innovations continue to advance, conventional mitral surgery, particularly valve repair, remains the preferred treatment for operable patients with primary MR because of its superior durability and long-term outcomes. In secondary MR, where durable repair is less achievable and outcomes depend more on ventricular function, M-TEER offers a mortality benefit in carefully selected patients. Surgery in this setting is generally reserved for those who also require concomitant procedures such as coronary revascularisation. The key challenge is to determine how transcatheter interventions can best complement surgical options to ensure each patient receives the most appropriate and effective treatment.
As the field evolves, transcatheter therapies are likely to expand treatment access for patients ineligible for surgery and may provide a bridge to recovery in acute heart failure. Ongoing trials are assessing the use of M-TEER and TMVR in intermediate-risk populations to explore whether these less invasive approaches can be applied safely and effectively to a wider range of patients. Experience gained from mitral interventions is also informing the development of transcatheter strategies for tricuspid valve disease, which presents similar anatomical and procedural challenges. At the same time, advances in surgical techniques, discussed later in this paper, continue to raise the standard for long-term outcomes across all valve positions.
The tricuspid valve, often referred to as “the forgotten valve”, has historically received less clinical attention than its left-sided counterparts [66]. Tricuspid stenosis is exceedingly rare, but tricuspid regurgitation (TR) is both common and frequently underestimated. Many patients with significant TR have been managed conservatively despite substantial symptoms, progressive functional decline, and poor long-term outcomes.
TR is increasingly recognised as a progressive disease, independently associated with right-sided heart failure, systemic congestion, reduced quality of life, and increased mortality [66, 67]. Unlike the mitral valve, the tricuspid valve is more compliant and prone to marked annular dilation, particularly in the setting of chronic right ventricular (RV) volume or pressure overload. Its function depends on the complex interaction between the leaflets, annulus, RV geometry, and right atrial pressures. In functional TR, which is the most common form, leaflet motion is usually normal, but coaptation is impaired due to annular dilation and leaflet tethering from RV remodelling. Up to 30% of patients have four or more leaflets, adding complexity to both surgical and transcatheter repair strategies [68].
For many years, surgery was the only definitive treatment for severe TR. Isolated tricuspid valve surgery carries an operative mortality of 8–10%, considerably higher than for other cardiac surgical procedures [69]. This elevated risk reflects late referral, advanced right ventricular dysfunction, and limited surgical experience with isolated TR [66, 69]. As a result, surgery is generally reserved for patients already undergoing left-sided valve surgery or CABG who also have severe TR. When intervention is undertaken, current guidelines recommend repair rather than replacement whenever feasible.
4.2.1.1 Tricuspid Transcatheter Edge-to-Edge Repair (T-TEER)
The development of transcatheter therapies is transforming the treatment landscape for patients with severe TR who are unsuitable for surgery. T-TEER uses the same approach as M-TEER, attaching a clip-like device to the leaflet tips to bring them together and reduce regurgitation (Fig. 7). The larger and more variable tricuspid annulus, more complex leaflet anatomy, and the need for detailed right heart imaging make these procedures technically challenging.
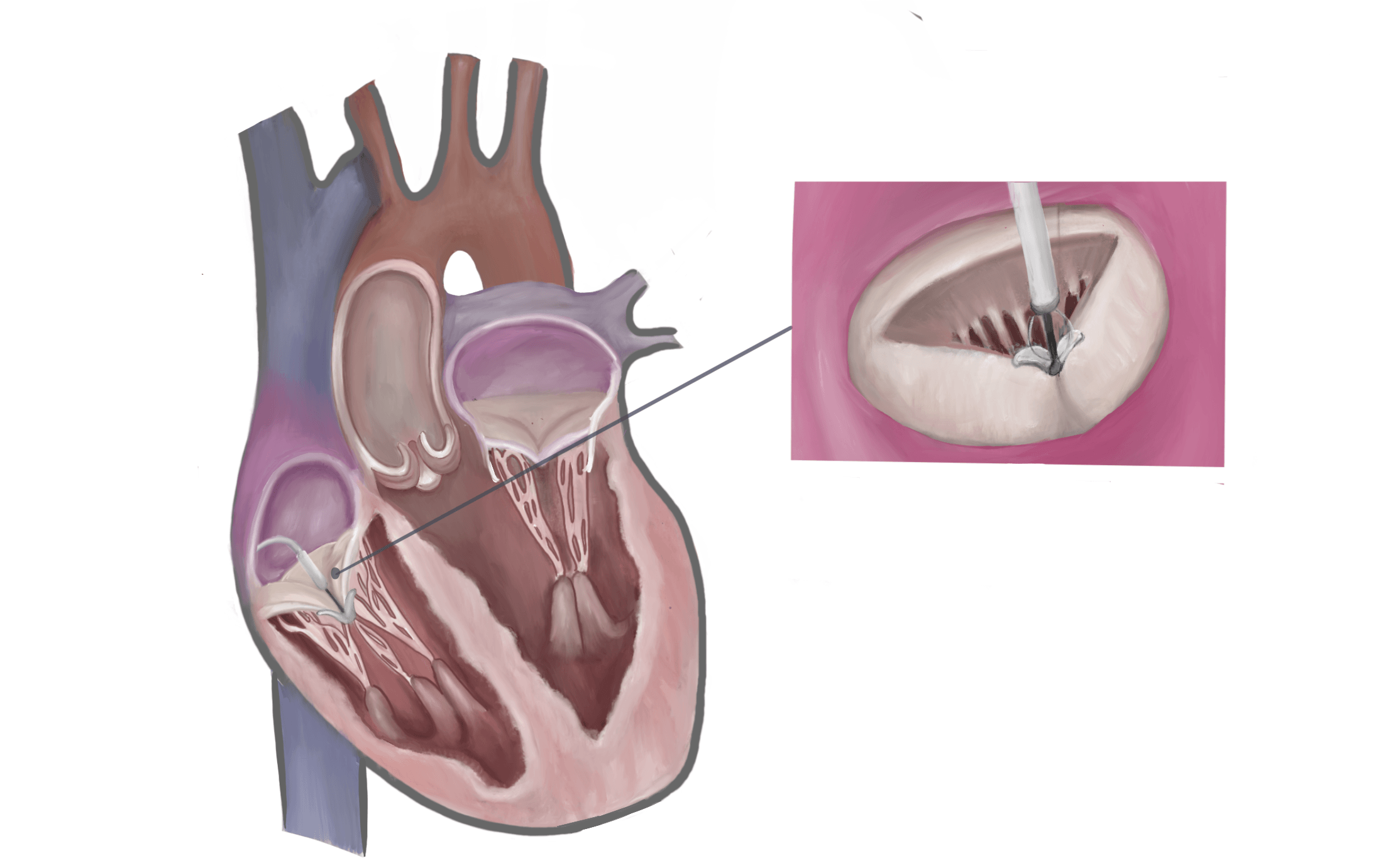 Fig. 7.
Fig. 7.
Tricuspid transcatheter edge-to-edge repair (T-TEER). A clip-like device is shown grasping the tricuspid valve leaflets to reduce regurgitation. Original illustration created using Procreate version 5.4 for iPad (Savage Interactive Pty Ltd., Hobart, TAS, Australia).
In the TRILUMINATE Pivotal Trial, using the TriClip transcatheter tricuspid valve repair system (Abbott Vascular, Santa Clara, CA, USA), T-TEER achieved high procedural success with the majority of treated patients experiencing meaningful reductions in TR severity and improvements in symptoms and quality of life [70]. Randomised evidence for the PASCAL Precision transcatheter valve repair system (Edwards Lifesciences LLC, Irvine, CA, USA) is being evaluated in the ongoing CLASP II TR Trial, with final outcomes awaited [71].
To date, randomised data have demonstrated consistent improvements in symptoms, exercise capacity, and quality of life following T-TEER, although no significant reduction in mortality or heart failure hospitalisation has yet been shown compared with medical therapy alone. This emphasises that symptom relief remains the principal aim of intervention at present. Across Europe, adoption of T-TEER has grown steadily, though procedural rates vary widely between countries. In the UK, uptake remains slower than in many other nations due to commissioning restrictions, although procedure numbers are increasing. Both T-TEER and transcatheter tricuspid valve replacement (TTVR) are not yet formally commissioned in the UK, which continues to limit access despite growing clinical demand (Fig. 8, Ref. [61, 62]).
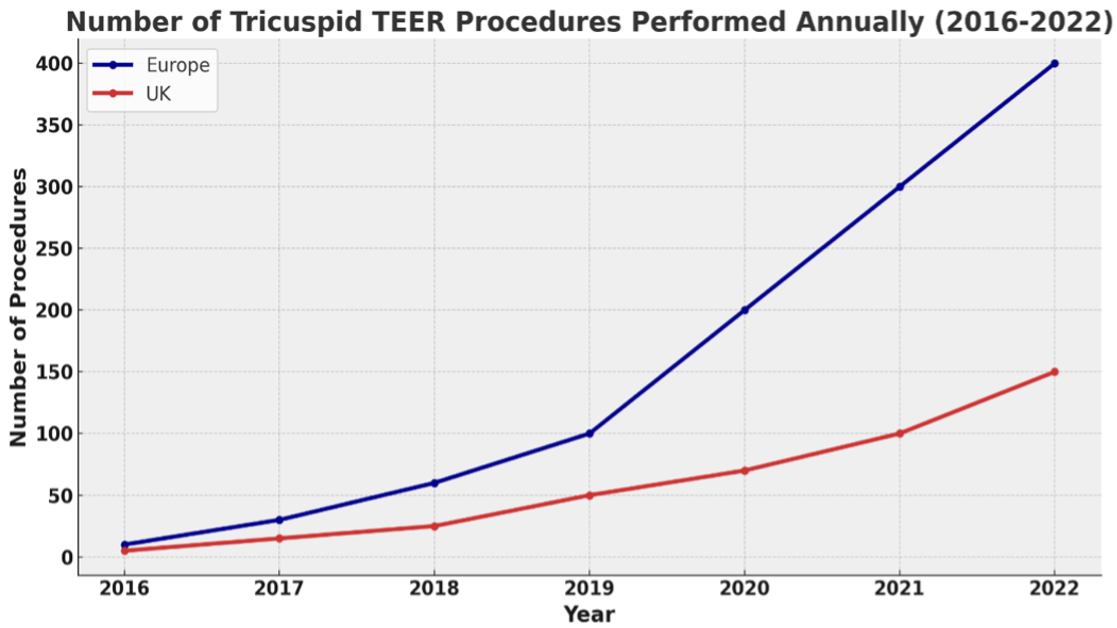 Fig. 8.
Fig. 8.
Number of tricuspid TEER procedures performed annually in Europe and the UK (2016–2022). The adoption of transcatheter edge-to-edge repair (TEER) for tricuspid regurgitation has increased markedly across Europe over recent years, with more modest but steady growth observed in the UK. Data from [61, 62]. Chart created using Microsoft Excel for Mac version 16.103.3 (Microsoft Corporation, Redmond, WA, USA).
4.2.1.2 Transcatheter Tricuspid Valve Replacement (TTVR)
TTVR has emerged as an option for patients in whom surgery is unsuitable and transcatheter repair is unlikely to succeed, such as those with large coaptation gaps, severe leaflet tethering, or a previous failed T-TEER procedure (Fig. 9).
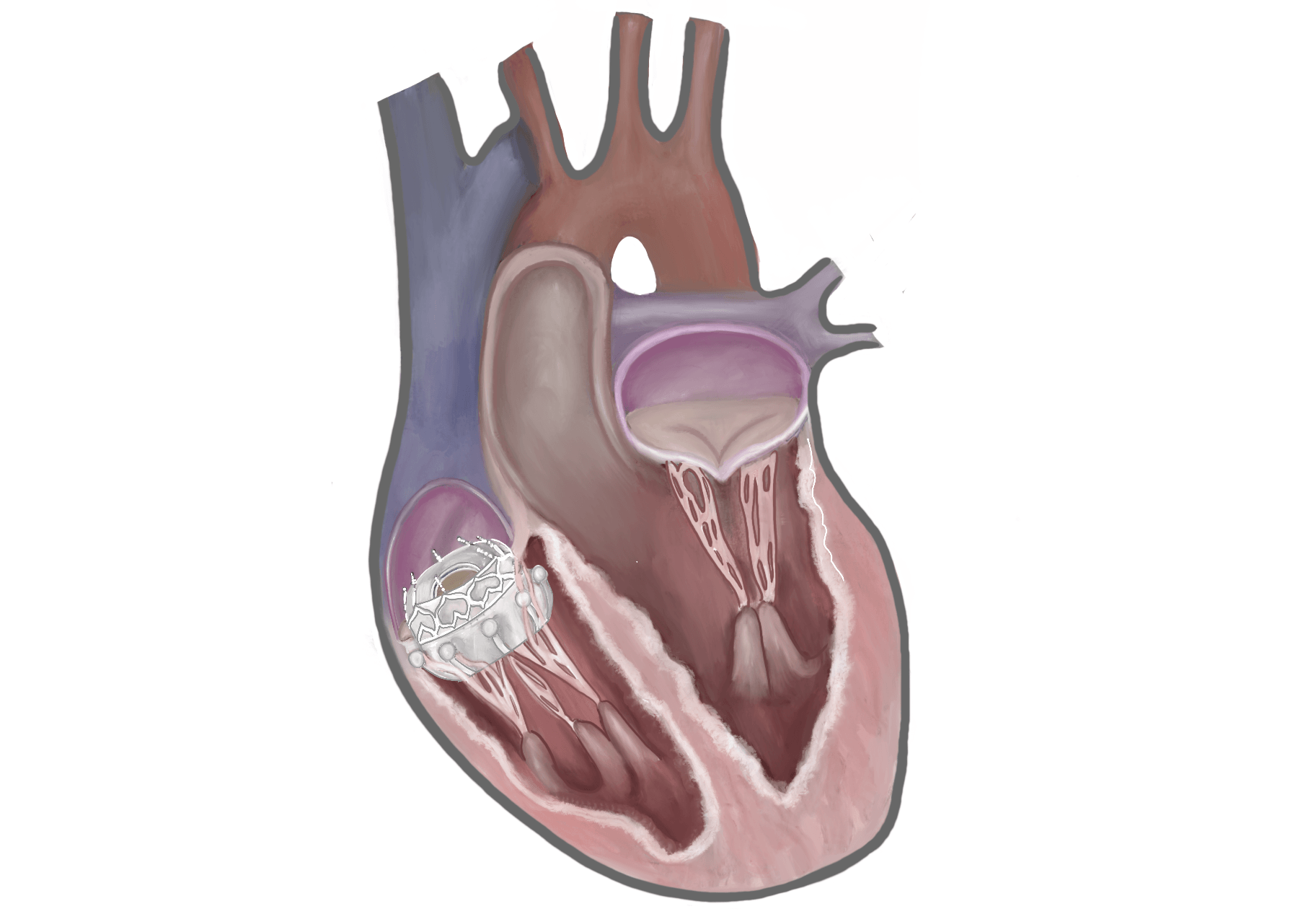 Fig. 9.
Fig. 9.
Tricuspid transcatheter valve replacement (TTVR). A transcatheter valve prosthesis is shown deployed within the tricuspid annulus. Original illustration created using Procreate version 5.4 for iPad (Savage Interactive Pty Ltd., Hobart, TAS, Australia).
The EVOQUE Tricuspid Valve Replacement System (Edwards Lifesciences LLC, Irvine, CA, USA) is the first TTVR device to receive Conformité Européenne (CE) marking, based on the TRISCEND II trial, which compared TTVR plus medical therapy with medical therapy alone [72, 73]. Procedural success was high at 97.6%, with 72.6% achieving TR reduction to mild or less at one year. Marked improvements in symptoms, exercise capacity, and quality of life were observed. At one-year, all-cause mortality was 12.6% with TTVR vs 15.2% with medical therapy, and heart failure hospitalisation was 20.9% vs 26.1%, but neither difference reached statistical significance. Longer-term data are awaited, although crossover from medical therapy to TTVR following commercial availability may limit ongoing comparison.
Other systems, including the Cardiovalve transfemoral tricuspid valve replacement system (Venus Medtech IL, Or Yehuda, Israel) and the LuX-Valve Plus transvascular tricuspid valve replacement system (Jenscare Scientific Co., Ltd., Ningbo, China), are being evaluated, although comparative and long-term durability data are still awaited. LuX-Valve Plus has progressed beyond early feasibility work and has accumulated substantial clinical experience, predominantly in China, where several hundred cases have now been performed. International use remains limited to feasibility or special-access programmes.
While complication rates may vary between devices, TTVR carries inherent risks regardless of the system used. These include vascular and bleeding complications from large-bore venous access, conduction disturbances requiring permanent pacemaker implantation, and valve thrombosis necessitating ongoing anticoagulation [72]. In the UK, access to TTVR remains restricted to research trials or exceptional-use cases.
Current guideline recommendations for tricuspid valve disease are summarised in Table 3 (Ref. [1, 3]). Notably, the ESC/EACTS 2021 guidelines do not formally endorse transcatheter therapies due to limited long-term data, whereas the ACC/AHA 2020 guidelines acknowledge them as promising for patients unsuitable for surgery.
| Clinical scenario | ESC/EACTS 2021 | ACC/AHA 2020 |
| Tricuspid Surgery During Left-Sided Surgery | Recommended (Class I) | Recommended (Class I) |
| Isolated Tricuspid Surgery | Considered in selected symptomatic cases (Class IIb) | Reasonable in severe symptomatic TR with progressive RV dilatation/dysfunction (Class IIa–IIb) |
| Transcatheter therapies (TTVI) | Acknowledged but not formally endorsed due to limited long-term data | Promising for patients unsuitable for surgery; consider under heart team-based, individualised decision-making |
Abbreviations: ACC, American College of Cardiology; AHA, American Heart Association; ESC, European Society of Cardiology; EACTS, European Association for Cardio-Thoracic Surgery; RV, right ventricular; TR, tricuspid regurgitation; TTVI, transcatheter tricuspid valve intervention.
Transcatheter tricuspid interventions are evolving rapidly. T-TEER is now established as an effective therapy for symptom relief in many patients with severe TR, while TTVR offers hope for those unsuitable for repair. As with mitral and aortic valve disease, early referral and Heart Team evaluation are essential. Advances in imaging and procedural expertise now offer real treatment options to patients who previously had none.
Cardiac surgery has progressed in step with transcatheter therapies. Advances in surgical technique, valve design, and perioperative care have improved outcomes, even as case complexity has increased. The proportion of complex surgical cases, including multi-valve procedures, re-do operations, and SAVR combined with CABG, has risen from approximately 30% to over 40% over the past two decades [25, 26, 27]. Despite this, outcomes have continued to improve. SAVR in-hospital mortality has declined from 5.6% to 3.4% overall, and to 1–2% in low-risk patients at high-volume centres [25, 26, 27, 74].
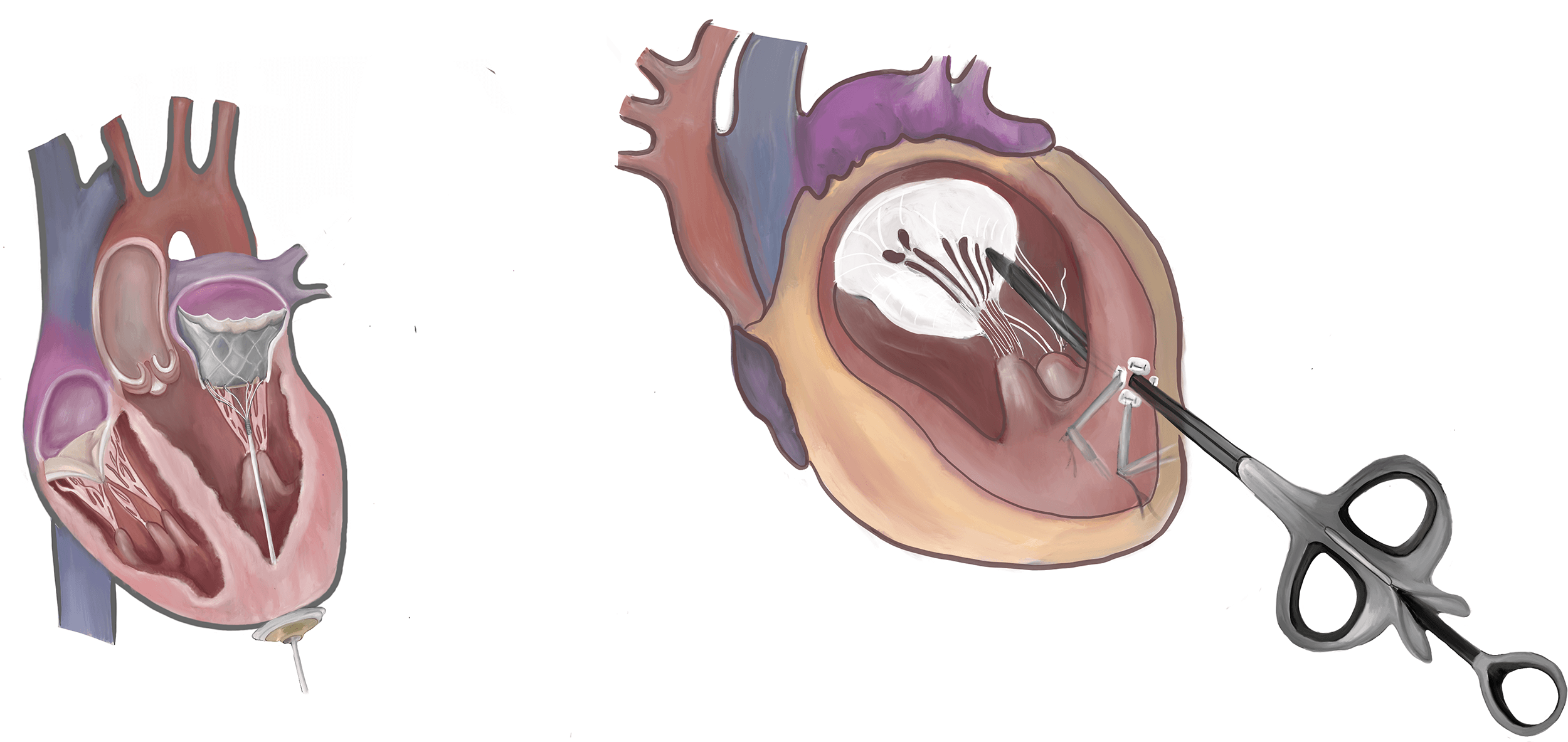
Minimally invasive and hybrid approaches continue to advance. Fully endoscopic and robotic-assisted valve surgery can reduce pain, infection risk, and recovery time, although broader adoption is limited by the specialised expertise required, steep learning curves, and substantial capital investment [75]. Hybrid procedures, such as transapical TMVR using the Tendyne system and transapical mitral repair with NeoChord, bridge surgical and transcatheter strategies by combining surgical access with catheter-based delivery [76, 77] (Fig. 10). These approaches remain under active investigation and may offer alternatives for patients unsuitable for conventional surgery or fully percutaneous intervention.
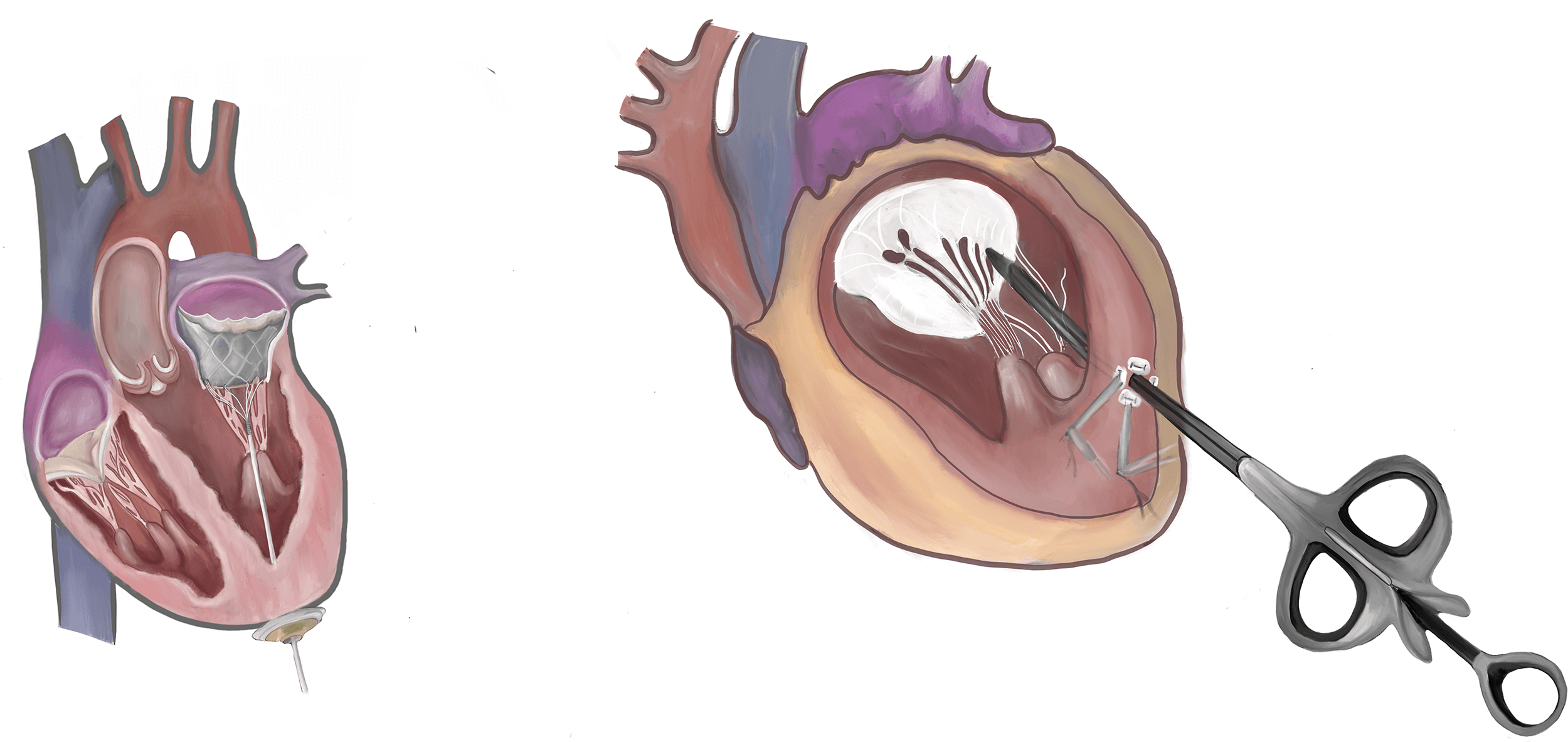 Fig. 10.
Fig. 10.
Emerging transcatheter mitral valve technologies. (Left) Tendyne transcatheter mitral valve replacement system. (Right) NeoChord artificial chordae delivery system for mitral valve repair, which allows implantation of artificial chordae tendineae without the need for cardiopulmonary bypass. Original illustration created using Procreate version 5.4 for iPad (Savage Interactive Pty Ltd., Hobart, TAS, Australia).
Surgical and transcatheter options are complementary rather than competing, with each approach offering distinct advantages depending on patient age, anatomy, and comorbidities (Table 4).
| Domain | Transcatheter Approach | Surgical Approach |
| Access to Therapy | Enables treatment in patients previously deemed inoperable or high surgical risk | Minimally invasive and robotic techniques extend surgical options to patients unable to tolerate full sternotomy |
| Recovery & Morbidity | Reduced perioperative risk, often performed under local anaesthesia and sedation; shorter hospital stays | Minimally invasive approaches associated with less pain, lower infection risk, and faster recovery |
| Multi-valve & Complex Disease | Sequential transcatheter interventions are possible, but simultaneous multi-valve procedures remain challenging and lack a robust evidence base | Surgical approach remains preferred for multi-valve, re-do, or combined CABG cases, with the ability to address multiple pathologies in one procedure |
| Reintervention Planning | Valve-in-valve techniques allow for staged management of structural valve deterioration | Bioprosthetic valve preference facilitates future valve-in-valve TAVI; mechanical valves offer long-term durability for younger patients |
| Durability in Younger Patients | TAVI durability encouraging (10–15 years), but long-term outcomes for mitral and tricuspid devices remain under investigation | Surgical repair/replacement remains gold standard for durability; mechanical valves preferred where anticoagulation is acceptable |
| Anatomical Versatility | Increasingly sophisticated imaging and device iterations are improving applicability | Surgical expertise allows correction of complex or borderline anatomy that remains off label for transcatheter devices |
| Specialised Expertise & Infrastructure | Rapid expansion of Heart Teams integrating imaging, interventional, and surgical input | Minimally invasive and robotic surgery requires specialist expertise, a steep learning curve, and significant investment in infrastructure and technology |
Abbreviations: CABG, coronary artery bypass grafting; TAVI, transcatheter aortic valve implantation.
The contemporary management of valvular heart disease encompasses a spectrum of interventions, from traditional open surgery through minimally invasive and robotic approaches to fully percutaneous transcatheter techniques. Rather than competing strategies, these options are complementary, with the optimal choice determined by patient-specific factors including age, anatomy, comorbidity burden, and the need for concomitant procedures. As detailed in the preceding sections, transcatheter therapies have extended treatment to patients previously deemed inoperable, while advances in minimally invasive surgery have reduced the morbidity of surgical intervention for those who remain operative candidates. Navigating this increasingly complex landscape requires the integration of multiple subspecialty perspectives, a theme explored further in the following section on the multidisciplinary Heart Team. Table 4 summarises the key considerations informing this decision-making process.
As cardiac interventions have grown in complexity, multidisciplinary collaboration through the Heart Team has become standard practice. Once reserved for high-risk cases, this approach is now embedded in routine care at leading centres.
Valve-specific teams typically include interventional cardiologists, cardiac surgeons, imaging specialists, anaesthetists, and heart failure experts. Together, they guide patient selection and procedural planning, weighing frailty, anatomical suitability, and procedural risk to deliver individualised care across the full spectrum of disease severity.
Both ESC/EACTS and ACC/AHA guidelines recommend Heart Team involvement, particularly for TAVI, complex mitral procedures, and reoperations [1, 3].
The adoption of transcatheter valve interventions varies considerably worldwide. Western Europe and North America rapidly embraced TAVI and are now expanding into mitral and tricuspid therapies, while uptake in other regions has been slower. Even within Europe, procedural volumes differ markedly, shaped by commissioning policies, resource availability, and access to specialist training.
Beyond Europe and the US, TAVI programmes are growing but at different rates. In China, annual cases rose from fewer than 300 in 2017 to over 7000 in 2021, though this still represents a small proportion of the eligible population [78]. In India, TAVI use is increasing, but SAVR remains more common because TAVI is significantly more expensive and insurance coverage is limited [79]. In Africa, adoption is very limited. South Africa has introduced TAVI in a small number of centres, but volumes remain low. Across most of the continent, economic and infrastructural barriers mean that many patients with severe valvular disease lack access to either TAVI or complex surgical intervention [80].
Transcatheter valve therapies are now firmly established in clinical practice and continue to evolve rapidly. Following the success of TAVI for AS, mitral and tricuspid transcatheter interventions are expanding. Edge-to-edge repair already benefits many high-risk patients, and ongoing trials may support broader use. Transcatheter valve replacement is progressing, with tricuspid replacement under large-scale investigation, while TMVR development has been slower due to anatomical and technical challenges.
Challenges remain. Global uptake is uneven, limited in some regions by resource constraints and access to specialist training. International collaboration, including proctorship, mentorship, and digital case-sharing, is helping to bridge these gaps.
Future advances in valve durability, delivery systems, and imaging will make procedures safer and more precise. Patient-specific planning using 3D imaging and computational modelling will refine selection and strategy. The future of valve care will be defined by integration, guided by multidisciplinary Heart Teams to ensure each patient receives the most appropriate, evidence-based treatment.
The management of VHD has advanced dramatically over the past century, from early surgical commissurotomies to the introduction of cardiopulmonary bypass, mechanical prostheses, and transcatheter techniques. Each innovation has built on the last, supported by pioneering clinicians and patients willing to embrace new approaches.
Transcatheter therapies have transformed outcomes for patients who were previously untreatable or faced prohibitive surgical risk. TAVI is now the dominant treatment for AS in older patients, while M-TEER offers a mortality benefit in carefully selected patients with secondary mitral regurgitation. Tricuspid interventions, though at an earlier stage, are providing symptom relief for patients with severe TR who have no surgical option.
Surgery remains essential for younger patients, those requiring mechanical valves, and complex cases involving multiple valves or concomitant revascularisation. The focus is no longer on whether transcatheter therapies will replace surgery, but on how best to integrate both to serve the needs of each individual patient. Guided by multidisciplinary Heart Teams, the future of valve care lies in personalised, evidence-based treatment selection.
• TAVI has transformed the treatment landscape by expanding access to older and frailer patients and is now being offered to lower-risk individuals thanks to excellent outcomes and a faster and less intensive recovery process.
• AS is now frequently managed with TAVI, which has become the standard of care across a wide spectrum of patients and is firmly embedded in international guidelines.
• Transcatheter options for mitral and tricuspid valve disease are gaining ground, but in parallel, innovations in minimally invasive surgery and hybrid techniques are renewing interest in surgical solutions for carefully selected patients.
• Surgical valve replacement continues to offer unmatched durability and remains the preferred option for younger, lower-risk patients, particularly when mechanical valves are indicated.
• Surgical and transcatheter therapies are no longer viewed in opposition, but are increasingly used together to tailor treatment, expand access, and optimise patient outcomes.
• Truly optimal care now depends on multidisciplinary collaboration, with Heart Teams bringing together expertise to guide nuanced, patient-specific decisions about timing, technique, and long-term strategy.
Not applicable.
SRP, MB, and KOG conceived the article and contributed to its design and overall structure. SRP conducted the literature review, synthesised and interpreted the literature, wrote the original draft, and created all graphs and tables. FHN created all original illustrations and contributed to the presentation and interpretation of visual content. FG, ME, AP, JB, PMC, MB, and KOG made substantial contributions to the conception and design of the article and to the interpretation of the literature and clinical content. All authors contributed to critical revision of the manuscript for important intellectual content, reviewed and approved the final version, and agreed to be accountable for all aspects of the work.
Not applicable.
The authors gratefully acknowledge the Cardiology and Cardiothoracic Surgery teams at King’s College Hospital, London, for their dedication to multidisciplinary valve care and their support in the preparation of this work.
This research received no external funding.
The authors declare no conflicts of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.