


 , Jing He 1, Feng Zhang 1, Qian Yang 1, Yinyan Qi 1, Na Zhang 1, Jing Zhi 2,*
, Jing He 1, Feng Zhang 1, Qian Yang 1, Yinyan Qi 1, Na Zhang 1, Jing Zhi 2,*
1 Gynaecology Department, The Fourth Hospital of Hebei Medical University, 050011 Shijiazhuang, Hebei, China
2 Radiotherapy Department, The Fourth Hospital of Hebei Medical University, 050011 Shijiazhuang, Hebei, China
Abstract
Long-term venous access is essential for administering chemotherapy in gynecological cancers, and the use of arm ports is becoming more common due to their practical advantages. However, postoperative complications remain a significant clinical concern. Currently, investigations specifically predicting the risk of arm port-related complications in gynecological oncology patients are limited. The advances of precision medicine warrant the development of individualized risk prediction tools to optimize clinical decision-making.
This retrospective analysis enrolled 476 patients who underwent arm ports (APs) implantation in the Gynaecology Department, The Fourth Hospital of Hebei Medical University, between July 2022 and October 2024. Patients were randomly divided into a training set (n = 334) and a validation set (n = 142) using computer-generated random numbers. Univariate and multivariate logistic regression analyses were used to identify independent risk factors, and the significant variables were incorporated into a prediction model. A nomogram of the prediction model was generated. Furthermore, the prediction model was internally validated using the Bootstrap method. The model’s discriminative performance, calibration, and clinical utility were determined using the receiver operating characteristic (ROC) curve, calibration curve, and decision curve analysis (DCA), respectively.
The overall postoperative complication rate was found to be 12.18% (58/476). Multivariate logistic regression analysis identified preoperative neutrophil-to-lymphocyte ratio (NLR) (odds ratio [OR] = 1.53, 95% confidence interval [CI]: 1.20–1.96), history of ipsilateral arm surgery (OR = 5.02, 95% CI: 2.06–12.23), and planned chemotherapy cycles (OR = 1.52, 95% CI: 1.26–1.85) as independent risk factors of postoperative complications (all p < 0.05). The nomogram prediction model constructed based on these factors demonstrated superior performance, yielding an area under the curve (AUC) of 0.819 (95% CI: 0.756–0.882) in the training set and 0.869 (95% CI: 0.793–0.945) in the validation set. The calibration curve showed good agreement between predicted probabilities and the actual observed incidence of postoperative complications. DCA indicated that the model showed greater clinical benefit than either treating all or treating no patients across a moderate range of threshold probabilities.
The proposed prediction model demonstrates fair to good capability in assessing the risk of postoperative complications following AP implantation in gynecological oncology patients. It supports clinicians in identifying high-risk individuals before surgery and enabling the implementation of targeted preventive approaches.
Keywords
- gynecological neoplasms
- vascular access devices
- nomogram
Gynecological cancers, including ovarian, cervical, and endometrial cancers, represent a major global health concern for women globally. Chemotherapy is a widely used approach for treating these cancers and often requires reliable long-term venous access. Totally implantable venous access ports (TIVAPs) have provided an effective and safe option for patients requiring prolonged chemotherapy [1, 2]. TIVAPs offer significant clinical advantages such as lower infection risk, convenient maintenance, improved quality of life, and long usage duration [3, 4].
In recent years, with advances in medical technology and increasing emphasis on quality of life, arm ports (APs) have been increasingly adopted as a novel implantation approach. Compared with traditional chest wall ports, APs are considered a safer alternative that exerts lower negative impact on quality of life in patients undergoing intravenous chemotherapy [5, 6]. However, postoperative complications associated with APs remain a significant clinical concern. Frequently reported complications include infection, catheter-related thrombosis, catheter malposition, and catheter occlusion [7, 8, 9, 10, 11]. These adverse events not only increase patient suffering and financial burden but can also disrupt antitumor therapy, potentially affecting disease prognosis.
Current studies have reported several risk factors for complications associated with venous access ports; research evidence specifically emphasizing gynecological oncology cohorts, particularly regarding risk prediction models for AP-related complications, remains limited [12, 13]. This highlights a critical gap: there are no population-specific, easy-to-use predictive models for AP complications in gynecological oncology. The advances in precision medicine necessitate more individualized and nuanced clinical decision-making. Establishing a dedicated risk prediction model for AP complications in gynecological oncology could support preoperative identification of high-risk individuals, guide targeted preventive interventions, optimize healthcare resource utilization, and ultimately improve quality of care. The nomograms, as intuitive risk prediction tools, convert complex regression equations into simpler graphical scoring systems, thereby assisting clinicians in rapid risk stratification and enabling efficient doctor-patient communication [14].
Therefore, this study retrospectively evaluated clinical data from gynecological oncology patients who received APs at a single center, with the objective of systematically investigating independent risk factors for AP-related complications. Based on the findings, a population-specific risk prediction model was established, and its predictive performance and clinical utility were assessed through internal validation. The ultimate goal is to provide evidence-based guidance to support individualized management approaches and enhance complication prevention in gynecological oncology patients using APs.
This retrospective cohort study was conducted at The Fourth Hospital of Hebei Medical University, China, including 476 eligible patients who received AP implantation in the Gynecological Department between July 2022 and October 2024. Inclusion criteria for patient were: (1) pathologically confirmed gynecological malignancy; (2) first-time AP implantation; and (3) availability of complete clinical data. Patients were excluded if they had (1) concurrent major surgery (defined as any non-port-related surgical procedure under general anesthesia within 30 days before port implantation); (2) severe coagulation dysfunction; (3) preexisting venous thrombosis or active infection in the implantation arm; and (4) follow-up duration less than 3 months.
This study was approved by the Ethics Committee of The Fourth Hospital of Hebei Medical University (approval number: 2023KS164). Written informed consent was obtained from all participants, and all procedures were conducted in accordance with the principles outlined in the Declaration of Helsinki.
Complications were defined as adverse events associated with the port occurring within 3 months after implantation. These events included infection (local or systemic manifestations requiring antibiotic therapy), catheter-related thrombosis (symptomatic thrombosis confirmed by Doppler ultrasound), port flip (rotation or displacement of the port chamber requiring repositioning), catheter occlusion (inability to flush or aspirate through the catheter), and other port-related adverse events. Study participants (n = 476) were randomly divided into a training set and a validation set at a 7:3 ratio using computer-generated random numbers, resulting in 334 individuals in the training set and 142 in the validation set.
Furthermore, patients were categorized into a complication group and a non-complication group based on the occurrence of complications. Collected clinical variables included: age, body mass index (BMI), history of diabetes, neutrophil-to-lymphocyte ratio (NLR), history of ipsilateral arm surgery (defined by any prior surgical procedure on the same arm as the port implantation, including but not limited to fracture fixation, lymph node dissection, or vascular access procedure, irrespective of the time since surgery), and the planned number of chemotherapy cycles. Age, BMI, NLR, and planned chemotherapy cycles were included as continuous variables. All patients received the same type of totally implantable venous access port (Model 61.635.07.070V3, PFM Medical, Cologne, Germany) with a 4.8 Fr catheter (inner/outer diameter: 1.0/1.6 mm).
Statistical analysis was conducted using R (version 4.2.1, R Foundation for
Statistical Computing, Vienna, Austria). Normality of continuous variables was
assessed using the Shapiro-Wilk test. Normally distributed variables are
presented as mean
Out of the 476 patients, 334 were assigned to the training set and 142 to the
validation set. No statistically significant differences were observed between
the two sets regarding age, BMI, diabetes history, preoperative NLR, history of
ipsilateral arm surgery, planned chemotherapy cycles, or complication rate (all
p
| Variable | Level | Training set (n = 334) | Validation set (n = 142) | Statistic | p-value |
| Age (years), (mean |
51.55 |
51.16 |
t = 0.392 | 0.695 | |
| BMI (kg/m2), median (Q1, Q3) | 24.60 (21.53, 26.28) | 25.00 (22.33, 26.50) | Z = –1.320 | 0.187 | |
| Diabetes, n (%) | No | 284 (85.03) | 129 (90.85) | 0.087 | |
| Yes | 50 (14.97) | 13 (9.15) | |||
| Previous surgery, n (%) | No | 299 (89.52) | 128 (90.14) | 0.839 | |
| Yes | 35 (10.48) | 14 (9.86) | |||
| NLR, median (Q1, Q3) | 3.28 (2.10, 4.15) | 3.19 (2.27, 4.27) | Z = –0.787 | 0.431 | |
| Chemo-cycles, median (Q1, Q3) | 4.00 (2.00, 6.00) | 5.00 (2.00, 7.00) | Z = –0.814 | 0.416 | |
| Complication, n (%) | No | 293 (87.72) | 125 (88.03) | 0.926 | |
| Yes | 41 (12.28) | 17 (11.97) |
Note: BMI, body mass index; NLR, neutrophil-to-lymphocyte ratio.
Among the 476 patients, 58 (12.18%) experienced postoperative complications, including 22 cases of infection (4.62%), 18 cases of symptomatic catheter-related thrombosis (3.78%), 5 cases of port flip (1.05%), 8 cases of catheter occlusion (1.68%), and 5 cases of other complications (1.05%). Incidence of complications is summarized in Table 2.
| Complication | Infection | Thrombosis | Port flip | Catheter occlusion | Other |
| Number of cases | 22 (4.62%) | 18 (3.78%) | 5 (1.05%) | 8 (1.68%) | 5 (1.05%) |
As shown in Table 3, univariate logistic regression analysis demonstrated that
preoperative NLR, a history of ipsilateral arm surgery, and the planned
chemotherapy cycles were significantly associated with the occurrence of
complications (p
| Predictor | SE | Wald | p-value | OR (95% CI) | |
| Age | 0.02 | 0.02 | 1.00 | 0.302 | 1.02 (0.98–1.05) |
| BMI | –0.05 | 0.05 | 1.00 | 0.259 | 0.95 (0.87–1.04) |
| Diabetes | 0.71 | 0.40 | 3.15 | 0.076 | 2.04 (0.93–4.48) |
| NLR | 0.51 | 0.12 | 18.06 | 1.66 (1.31–2.10) | |
| Previous surgery | 1.74 | 0.40 | 18.92 | 5.72 (2.60–12.58) | |
| Chemo-cycles | 0.41 | 0.09 | 20.75 | 1.50 (1.26–1.78) |
Note: OR, odds ratio; CI, confidence interval; SE, standard error; BMI, body mass index; NLR, neutrophil-to-lymphocyte ratio.
Factors with a p-value
| Predictor | SE | Wald | p-value | OR (95% CI) | |
| NLR | 0.43 | 0.13 | 10.94 | 1.53 (1.20–1.96) | |
| Previous surgery | 1.61 | 0.45 | 12.80 | 5.02 (2.06–12.23) | |
| Chemo-cycles | 0.42 | 0.10 | 17.64 | 1.52 (1.26–1.85) |
Note: NLR, neutrophil-to-lymphocyte ratio.
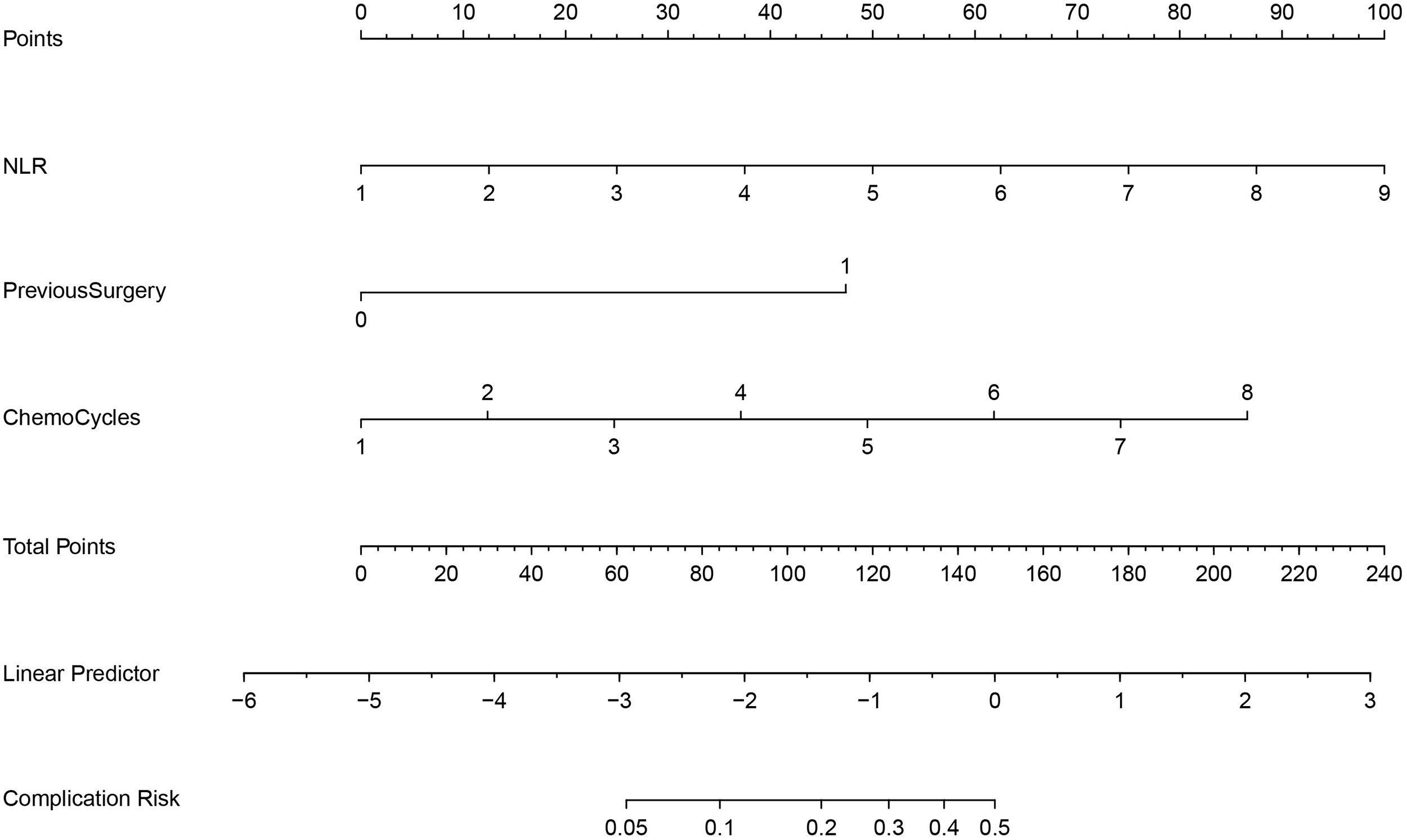
A nomogram prediction model was then constructed using the three independent risk factors identified (NLR, history of ipsilateral arm surgery, and planned chemotherapy cycles), based on the training set of 334 individuals (Fig. 1).
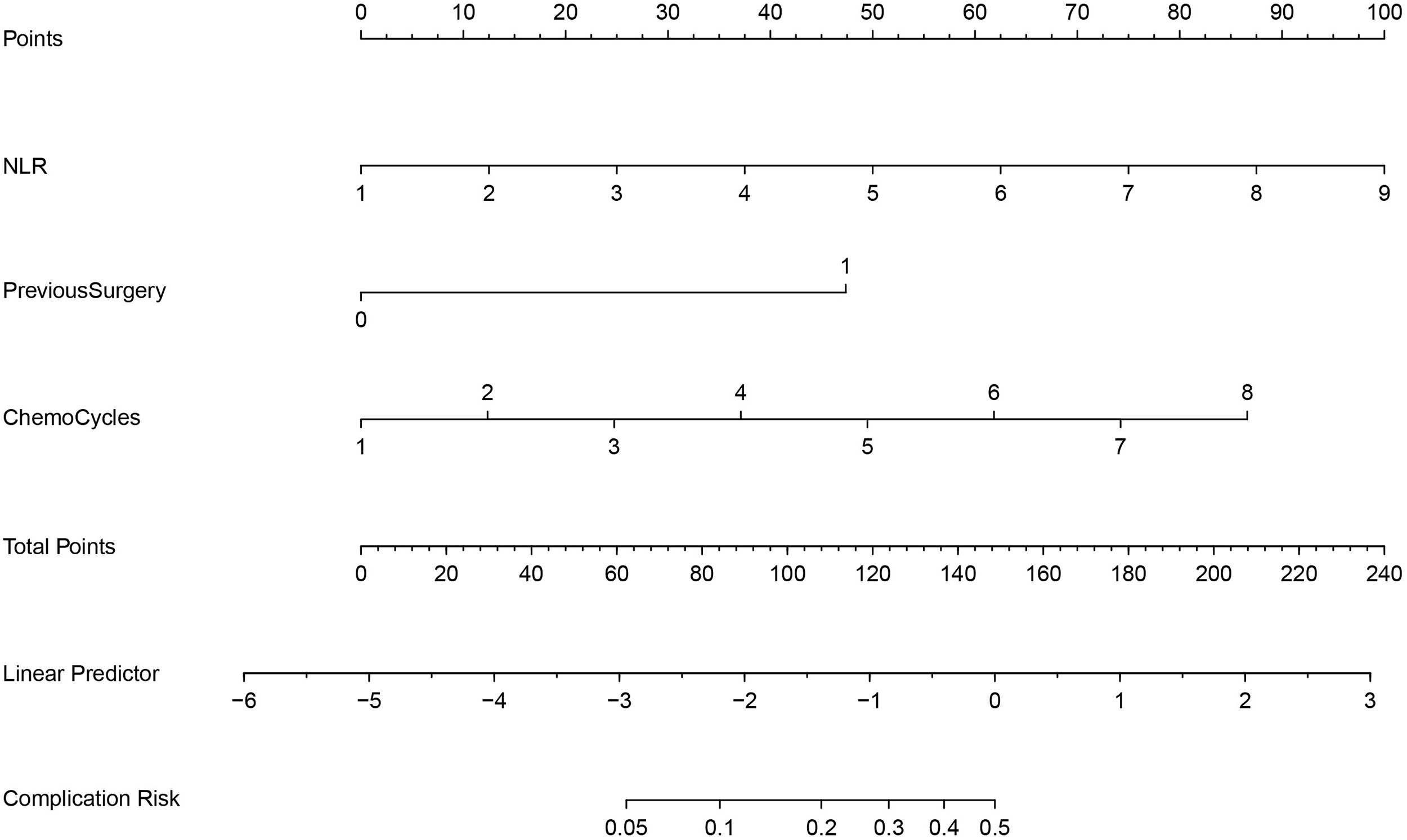 Fig. 1.
Fig. 1.
A nomogram prediction model for postoperative complications.
Receiver operating characteristic (ROC) curve analysis showed strong discriminative performance, with an area under the curve (AUC) of 0.819 (95% confidence interval [CI]: 0.756–0.882) in the training set and 0.869 (95% CI: 0.793–0.945) in the validation set (Fig. 2, n = 334 for training, n = 142 for validation).
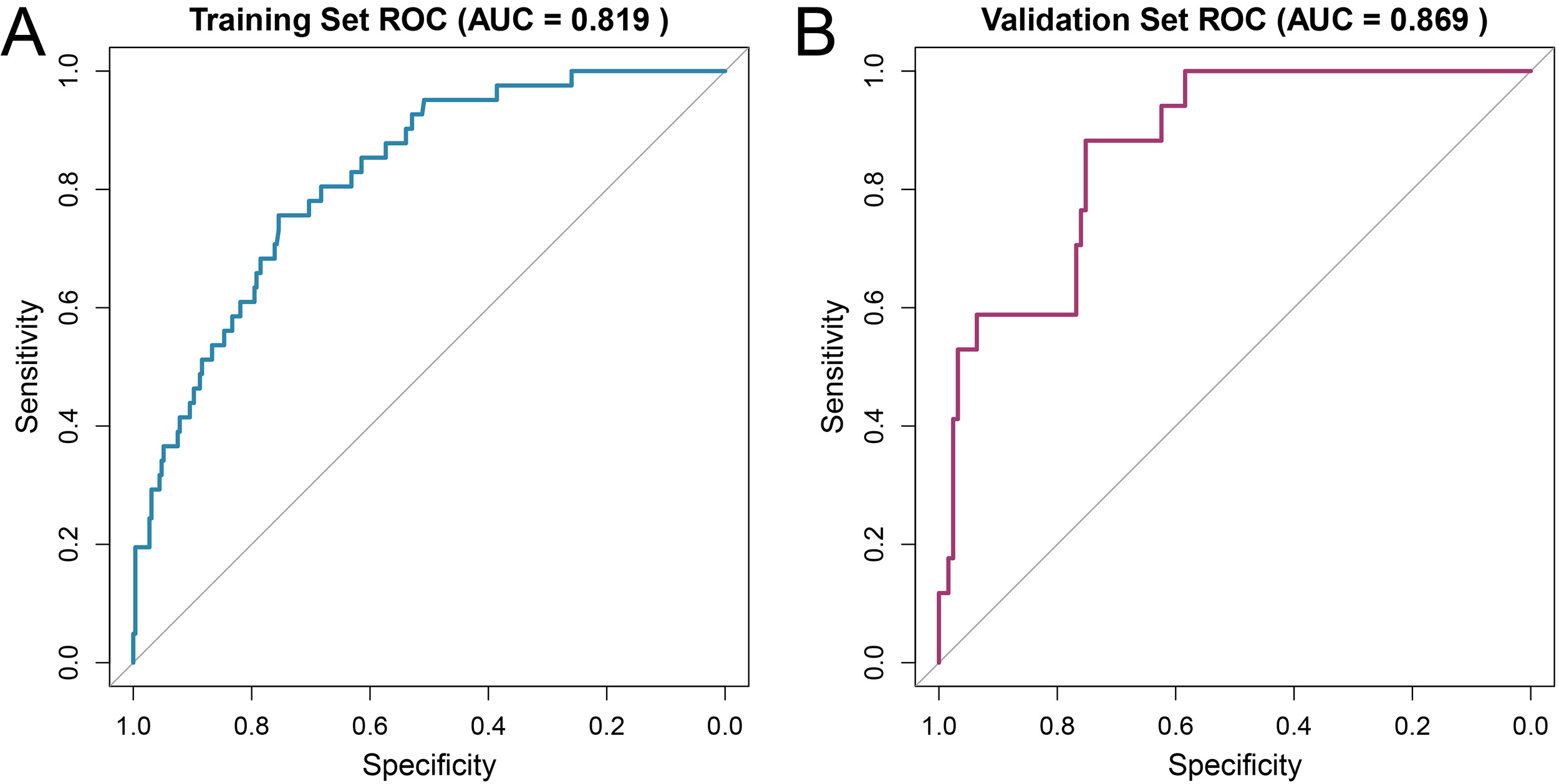 Fig. 2.
Fig. 2.
ROC analysis of the prediction model. (A) Training set; (B) validation set. ROC, receiver operating characteristic; AUC, area under the curve.
The calibration curve showed that the predicted risks closely followed the ideal
diagonal line (45-degree line), indicating good agreement between predicted and
observed probabilities (Fig. 3, n = 334 for training, n = 142 for validation).
Internal validation using the bootstrap method, along with the Hosmer-Lemeshow
test (training set:
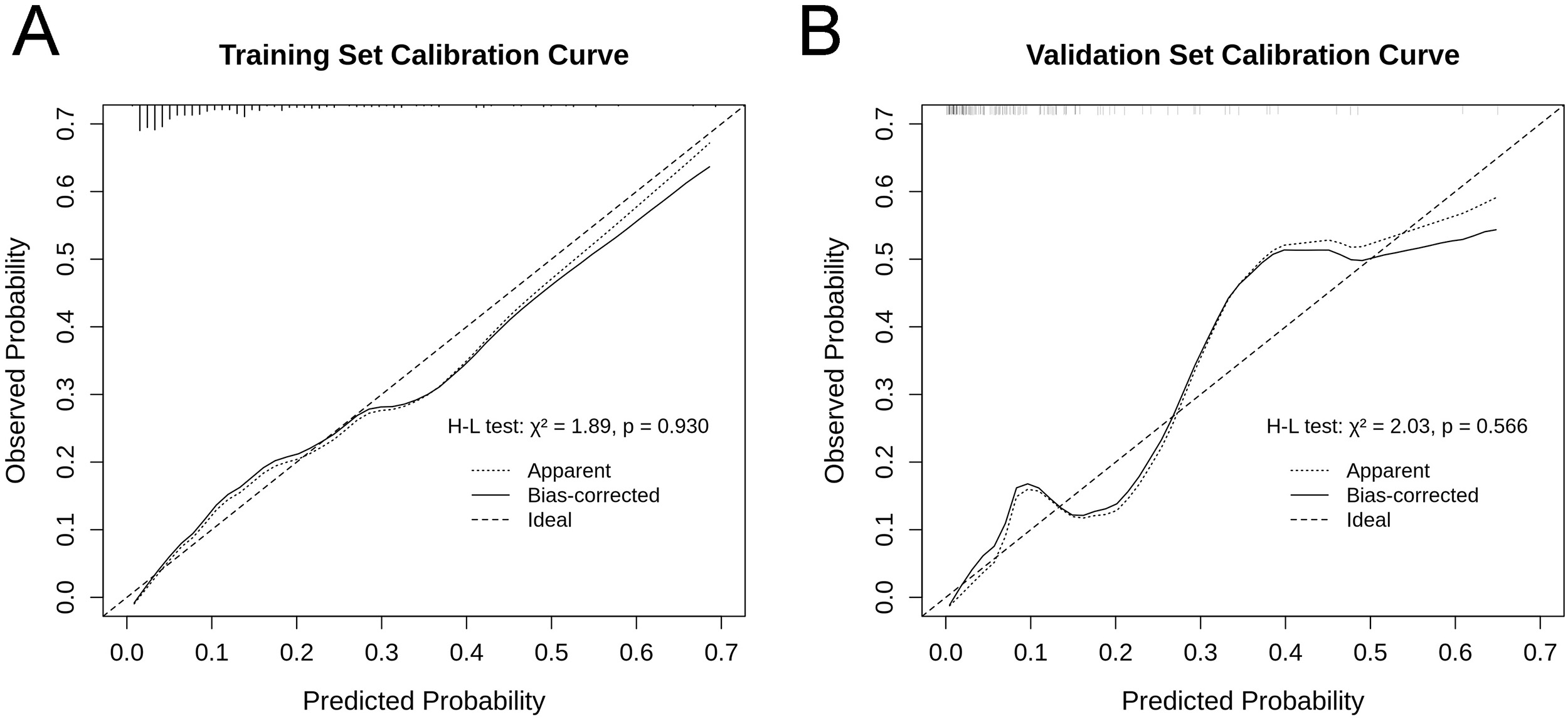 Fig. 3.
Fig. 3.
Calibration curves for the prediction model. (A) Training set; (B) validation set. The dotted line represents the apparent performance, the solid line represents the bias-corrected performance after bootstrap validation, and the dashed line represents the ideal reference line.
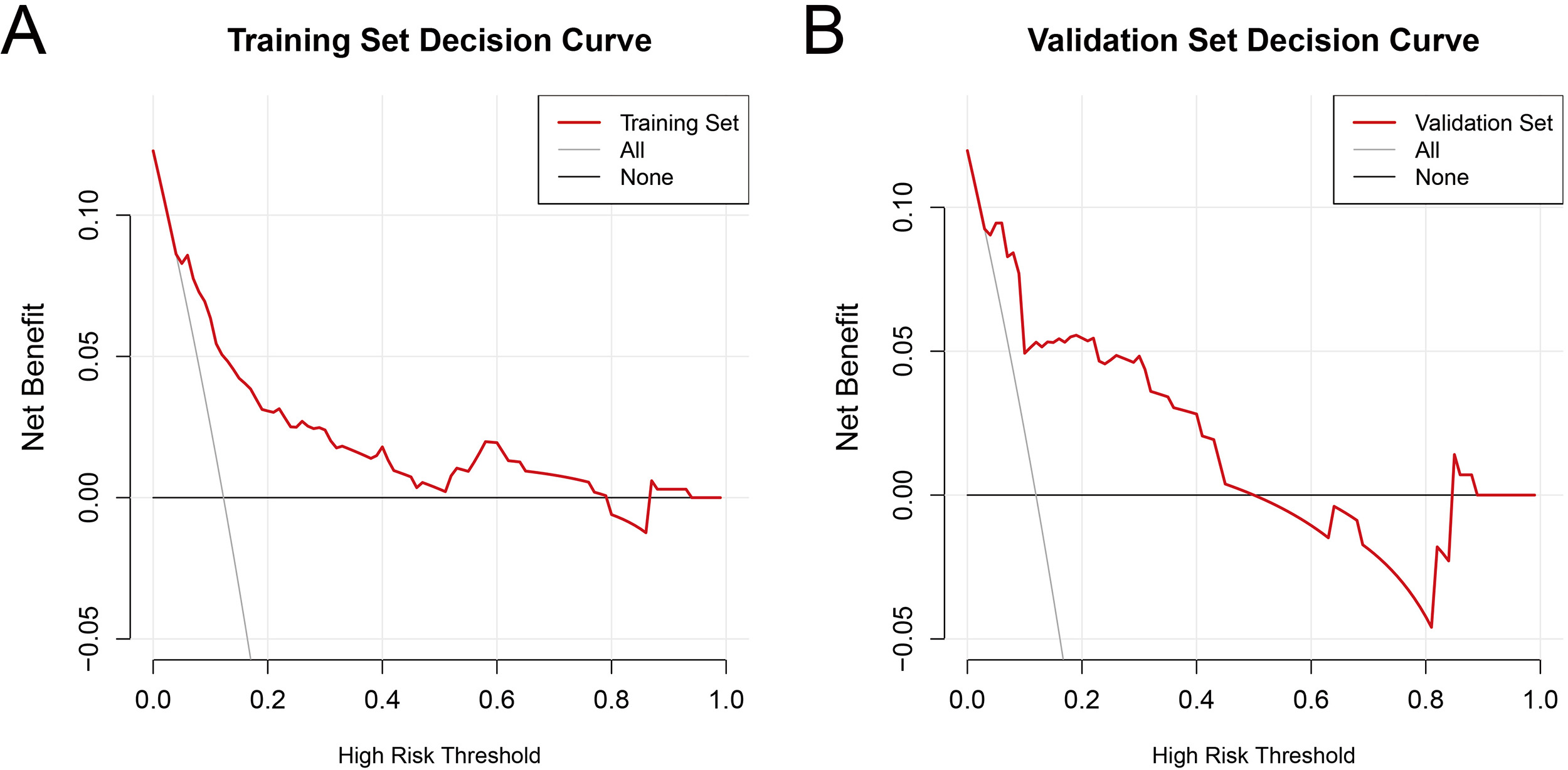
The decision curve analysis (DCA, Fig. 4, n = 334 for training, n = 142 for validation) demonstrated that, in the training set, using the prediction model for clinical decision-making yielded a higher net benefit compared to the “intervene-all/treat all” and “intervene-none/treat-non” strategies across a threshold probability range of approximately 10% to 80%. In the validation set, the model achieved greater net benefit within a threshold range of about 10% to 45%. The ‘All’ strategy represents intervening in all patients, whereas the ‘None’ strategy represents no intervention. The DCA indicates that the clinical utility of the model is primarily confined to a moderate range of threshold probabilities, which nonetheless covers a meaningful and relevant decision-making spectrum in clinical practice.
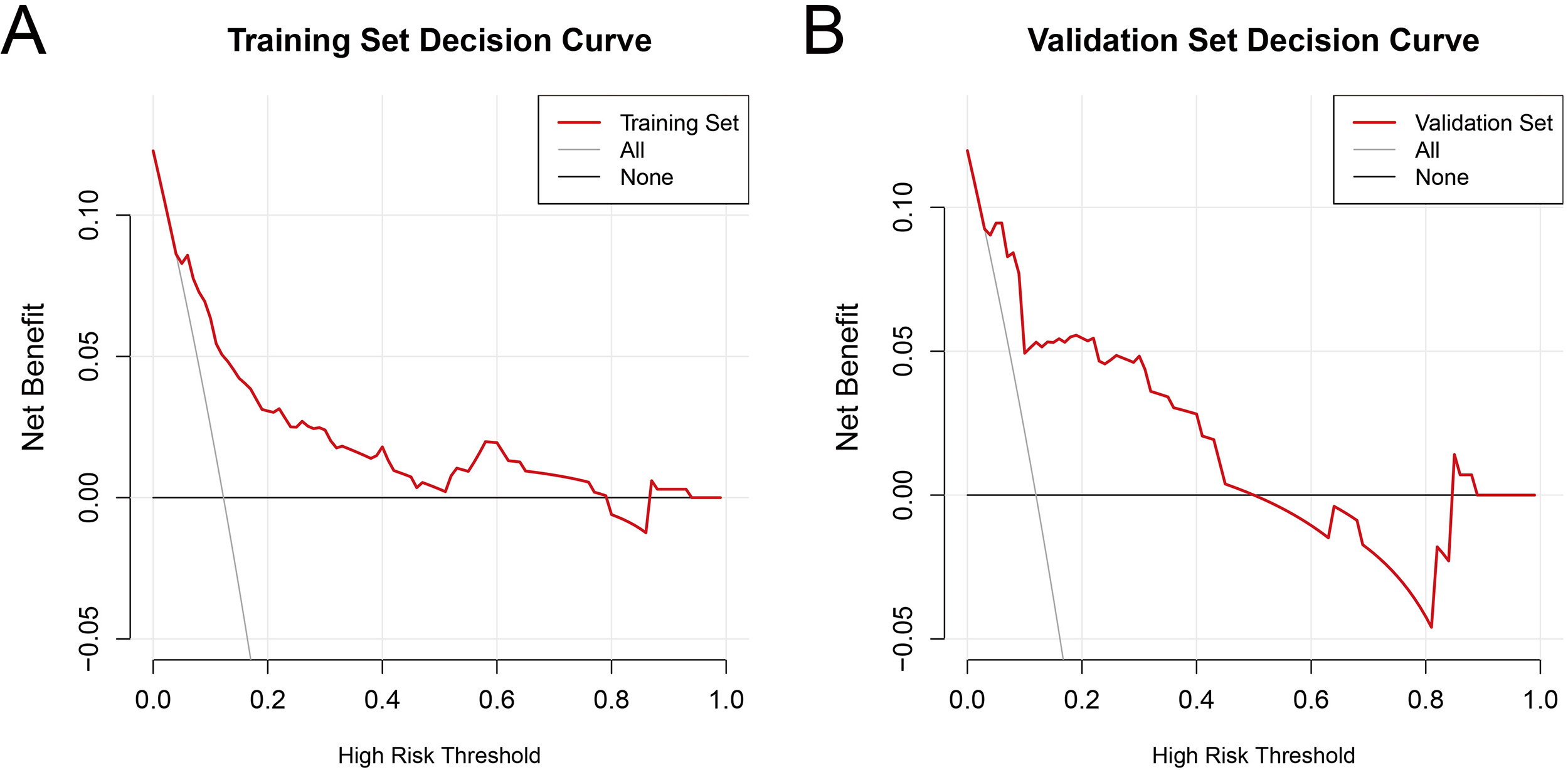 Fig. 4.
Fig. 4.
Decision curve analysis for the prediction model. (A) Training set; (B) validation set. The “All” line represents the strategy of intervening on all patients, while the “None” line represents the strategy of withholding intervention from all patients. The red solid line represents the net benefit of applying this prediction model for clinical decision-making.
This retrospective analysis of 476 gynecological oncology patients with APs constructed a risk prediction model, specifically targeting postoperative complications following AP implantation in this patient cohort. Preoperative NLR, history of ipsilateral arm surgery, and planned chemotherapy cycles were identified as independent risk predictors of complications. These variables were incorporated into an intuitive nomogram, enabling clinicians to conduct rapid, individualized risk assessment. The model demonstrated superior predictive performance and clinical utility, providing a valuable tool to guide tailored approaches for complication prevention and management.
The NLR is a reliable marker of systemic inflammatory response and has been
widely validated as a prognostic predictor for various clinical outcomes in
cancer patients [15, 16, 17, 18]. This study is the first to indicate a specific
association between NLR and AP-related complications, with a significant odds
ratio (OR = 1.53), suggesting that managing preoperative inflammatory status may
contribute to reducing complication risk. Mechanistically, NLR indicates more
than a simple risk indicator and is closely associated with the
“inflammation-coagulation-immunity” axis. Elevated NLR, indicative of an
inflammatory state, promotes the release of neutrophil extracellular traps
(NETs), upregulates the expression of tissue factors, and enhances platelet
activation, collectively enhancing a potent prothrombotic environment that
significantly increases the risk of catheter-related thrombosis [19, 20]. On the
other hand, persistent inflammation, mediated by pro-inflammatory cytokines such
as tumor necrosis factor-alpha (TNF-
A history of ipsilateral surgery was identified as the strongest predictor of
complications (OR = 5.02), and its impact is driven by multiple mechanisms.
Disruption of the local lymphatic network during previous surgery can lead to
chronic lymphatic stasis and interstitial fluid accumulation [23]. Additionally,
surgical scarring compromises the local microvascular architecture and reduces
tissue perfusion, which impairs oxygen and nutrient delivery, severely affects
tissue repair capacity, and is directly linked to increased infection risk
[24, 25, 26]. Furthermore, the chronically hypoxic microenvironment within scar tissue
can further exacerbate local inflammation through upregulation of factors such as
hypoxia-inducible factor 1-alpha (HIF-1
The positive association between the planned number of chemotherapy cycles and complication risk (OR = 1.52) primarily reflects the cumulative effect of treatment intensity and extended catheter exposure. Mechanistically, each chemotherapy infusion imposes chemical and mechanical injury on the vascular endothelium. Recurrent endothelial damage and repair over time promote a prothrombotic state and increase the risk of catheter-related thrombosis [29]. Simultaneously, frequent catheter access increases the cumulative probability of micro-damage to the catheter lumen and facilitates bacterial biofilm formation. Once established, biofilms can shield pathogens from host immune responses and antimicrobial agents, leading to persistent and difficult-to-treat infections [30, 31, 32].
The proposed prediction model offers a practical tool for individualized AP management in gynecological oncology. For example, a patient with an NLR of 4.5 (approximately 40 points), a history of ipsilateral arm surgery (approximately 50 points), and 6 planned chemotherapy cycles (approximately 60 points) would yield a total score of about 150 points, corresponding to a complication risk of about 50%. For such high-risk patients, intensified monitoring and consideration of prophylactic interventions, such as anticoagulation, may be needed. The model demonstrated robust predictive performance, consistent with contemporary prediction models for complications of totally implantable venous access ports in adult oncology cohorts, which typically report validation AUCs around 0.80. For instance, a recent nomogram for predicting port-related infections in adult tumor patients reported an AUC of 0.835 [33]. These findings support clinical application while leaving room for future refinement.
Incorporating this model into preoperative assessment can help identify high-risk patients and guide targeted preventive approaches, including enhanced blood glucose management, optimized surgical planning, and individualized anticoagulation strategies. For patients stratified as very high-risk, alternative venous access options or more intensified postoperative monitoring may be considered. The model can also guide patient counseling by elucidating individual risk profiles and emphasizing preventive behaviors, which include adherence and management. Furthermore, the model provides a standardized tool for risk stratification in future clinical investigations, facilitating patient selection, subgroup analysis, and comparison of outcomes across different interventions.
This study has several limitations. First, as a single-center retrospective study, it is subject to potential selection bias related to the characteristics of the specific patient population and the clinical practices at our center, which may limit the generalizability of these findings to other healthcare settings with different demographics or treatment protocols. Second, despite the overall sample size, the number of patients was still limited, and it remained insufficient for detailed subgroup analyses of less frequent complication types. Third, the model has not undergone external validation, and its performance with broader or more diverse populations remains to be established.
Another key limitation is the use of a composite endpoint that combines complications with potentially different pathophysiological mechanisms. While this approach improves statistical power, it may mask specific risk factors that are specific to individual complication subtypes. Future investigations should focus on multi-center prospective designs for external validation, assessment of whether incorporating novel biomarkers, such as inflammatory cytokines and coagulation parameters, can enhance predictive performance, and the development of dynamic, potentially artificial intelligence-based prediction tools to enable real-time risk assessment and early detection of complications.
Overall, this study developed a prediction model specifically designed to estimate the risk of postoperative complications following AP implantation in patients with gynecological oncology. The model demonstrates good predictive performance and clinical utility, supporting preoperative identification of high-risk individuals and guided targeted preventive approaches. This model has the potential to lower complication rate, improve patient outcomes, and contribute to more effective clinical management.
• This study developed a nomogram for the first time to predict arm port complications in gynecological oncology patients.
• Preoperative NLR, history of ipsilateral arm surgery, and planned chemotherapy cycles were identified as independent risk factors.
• The model demonstrates good discriminative performance and calibration in both the training and validation sets.
• Decision curve analysis confirmed the clinical utility of the model across a moderate range of threshold probabilities.
• This tool may aid in preoperative risk stratification and guide personalized preventive strategies for high-risk patients.
The data that support the findings of this study are available from the corresponding author upon reasonable request.
YLS, JH, JZ and FZ designed the research study. QY, YYQ and NZ performed the research. YLS and JZ analyzed the data. JZ drafted the manuscript. All authors contributed to the important editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
The study was approved by the Ethics Committee of The Fourth Hospital of Hebei Medical University (approval number: 2023KS164). Written informed consent was obtained from all participants, and all procedures were conducted in accordance with the principles outlined in the Declaration of Helsinki.
Not applicable.
This research was supported by Hebei Province Medical Science Research Project Plan, Grant No. 20230830.
The authors declare no conflicts of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.