
 , Yao Ma 1, Jiali Liu 1, Huan Liu 1,*
, Yao Ma 1, Jiali Liu 1, Huan Liu 1,*
1 Department of Anesthesiology, Tianyou Hospital Affiliated to Wuhan University of Science and Technology, 430064 Wuhan, Hubei, China
Abstract
Opioid-induced side effects present substantial perioperative challenges, thereby driving the growing clinical adoption of opioid-sparing anaesthesia (OSA) and opioid-free anaesthesia (OFA) techniques. These multimodal strategies are designed to improve patient recovery while supporting responsible opioid stewardship. This review offers a practical overview of the principles, core techniques, and contemporary evidence for implementing OSA and OFA within routine hospital anaesthesia practice. Central to OSA/OFA is the integration of multimodal analgesia, which includes regional anaesthetic blocks, alpha-2 agonists, N-methyl-D-aspartate (NMDA) receptor antagonists, and gabapentinoids. Key advantages include reduced postoperative nausea and vomiting (PONV), faster return of bowel function, and markedly decreased opioid requirements. Effective implementation requires comprehensive patient education, individualized perioperative protocols, and coordinated interdisciplinary teamwork. OSA and OFA represent safe, effective, and increasingly essential strategies for perioperative pain management. Their broader integration can improve patient recovery outcomes, reduce opioid-related complications, and contribute to institutional medication-safety initiatives.
Keywords
- opioid-free anaesthesia
- opioid-sparing anaesthesia
- perioperative period
- pain management
For decades, opioids have served as a cornerstone of perioperative analgesia, valued for their potent pain-relieving properties [1]. However, their use is associated with a broad spectrum of adverse events that compromise patient safety and delay recovery. Postoperative nausea and vomiting (PONV), one of the most frequent opioid-related complications, affects up to 80% of high-risk patients undergoing general anaesthesia, leading to delayed oral intake, prolonged hospital stays, and greater patient dissatisfaction [2]. Opioid-induced ileus, characterized by impaired gastrointestinal motility, further disrupts recovery by delaying the return of bowel function, increasing the risk of abdominal distension, and extending the need for parenteral nutrition [3]. Perhaps most concerning is opioid-induced respiratory depression (OIRD), a potentially life-threatening complication that contributes to postoperative mortality and morbidity, particularly in vulnerable populations such as the elderly, obese individuals, and patients with pre-existing respiratory disorders [4].
In addition to these acute adverse events, intraoperative opioid exposure has been linked to long-term consequences. Opioid-induced hyperalgesia (OIH), a phenomenon in which opioids paradoxically increase pain sensitivity, leads to higher postoperative analgesic requirements and an elevated risk of chronic postsurgical pain (CPSP) [5]. Additionally, perioperative opioid use is a significant risk factor for persistent postoperative opioid use (PPOU), defined as continued opioid consumption beyond 90–365 days after surgery [6]. A Danish nationwide cohort study involving nearly 70,000 patients undergoing hip fracture surgery revealed that 64.8% of preoperative opioid users remained on opioids 6–9 months postoperatively, compared with only 17.8% of opioid-naive patients [7]. These findings highlight the urgent need to re-evaluate the role of opioids in perioperative care and to explore alternative strategies that minimize opioid exposure while maintaining effective pain control.
In response to the growing recognition of opioid-related harms, opioid-sparing anaesthesia (OSA) and opioid-free anaesthesia (OFA) have emerged as viable alternatives to traditional opioid-based anaesthesia (OBA) [8]. OSA refers to techniques that reduce but do not eliminate opioid use, typically through the integration of non-opioid analgesics and regional anaesthesia [9]. OFA, in contrast, is defined as a combination of opioid-sparing strategies that avoid systemic opioid administration entirely during the perioperative period. Both approaches aim to reduce opioid exposure, thereby mitigating opioid-induced adverse events and improving patient outcomes. The development of OFA can be traced back to the 1990s, when researchers began investigating antihyperalgesic techniques to enhance postoperative pain control [10]. Early studies have demonstrated that the use of non-opioid adjuvants, such as clonidine and ketamine, reduces postoperative opioid requirements and improves overall pain management [11, 12, 13]. Since then, an expanding body of evidence has supported the efficacy and safety of OSA and OFA. A meta-analysis comparing OFA with opioid-inclusive anaesthesia reported that OFA was not associated with increased postoperative pain scores but was linked to a significant reduction in PONV [14]. Similarly, Olausson et al. [15] conducted a high-quality systematic review and meta-analysis of 26 studies, concluding that OFA resulted in reduced postoperative opioid consumption and fewer adverse events, with no evidence of compromised safety or pain management.
Despite the accumulating evidence supporting OSA and OFA, their integration into routine hospital practice remains limited. Barriers to implementation include the absence of standardized protocols, uncertainty about drug selection and dosing, and challenges related to interdisciplinary collaboration [16]. Additionally, numerous healthcare providers remain hesitant to adopt these techniques due to concerns about inadequate pain control, particularly in patients undergoing major surgical procedures. This review aimed to address these gaps by offering a practical guide for implementing OSA and OFA in hospital settings. It synthesizes current evidence on the clinical efficacy and safety of these approaches, outlines key clinical principles for their adoption, and provides strategies for overcoming implementation challenges. By emphasizing real-world applications, this review aimed to support healthcare providers in enhancing perioperative care through opioid minimization, aligning with global efforts to strengthen medication safety and optimize patient outcomes.
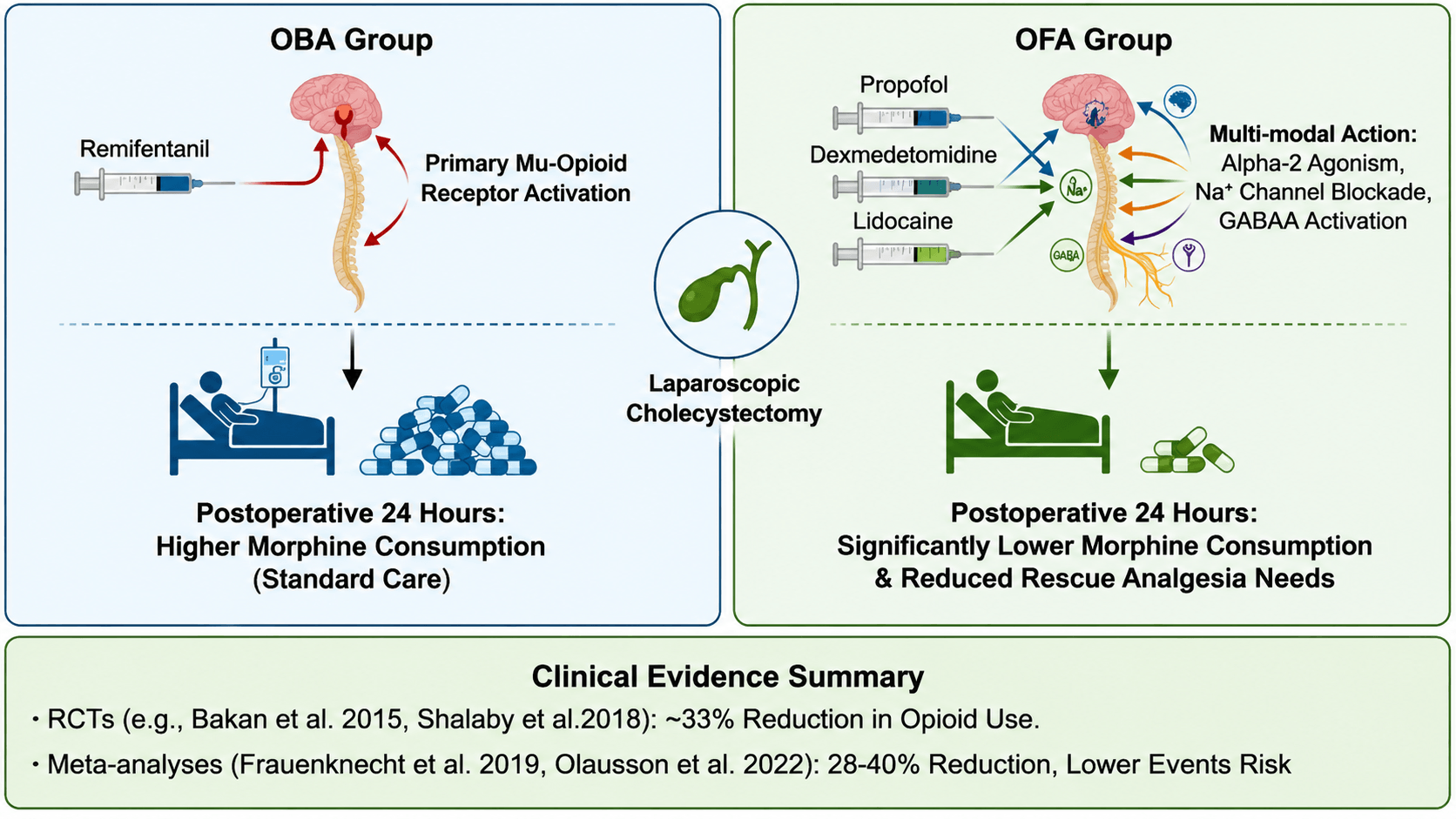
A central objective of OSA and OFA is to minimize opioid use throughout the perioperative period, and numerous studies have demonstrated their effectiveness in achieving this goal. In a randomized controlled trial (RCT) by Bakan et al. [17], patients undergoing laparoscopic cholecystectomy were assigned to either an OFA group (receiving propofol, dexmedetomidine, and lidocaine) or an OBA group (receiving remifentanil). The OFA group showed significantly lower postoperative morphine consumption at 24 hours and a reduced need for rescue analgesia. Similarly, Shalaby et al. [18] conducted an RCT in patients undergoing laparoscopic cholecystectomy and reported a 33% reduction in postoperative opioid consumption in the OFA group compared with the OBA group.
Meta-analyses have further confirmed these findings. Frauenknecht et al. [19] analyzed 23 studies comparing OFA with OBA (Fig. 1, Ref. [15, 17, 18, 19]) and reported that OFA was associated with a 28% reduction in postoperative opioid use. Olausson et al. [15] conducted a more recent meta-analysis of 26 studies and identified an even greater reduction, with OFA resulting in a 40% decrease in postoperative opioid use. These reductions are clinically significant, as they correspond to a lower risk of opioid-induced adverse events and a reduced likelihood of persistent postoperative opioid use (PPOU).
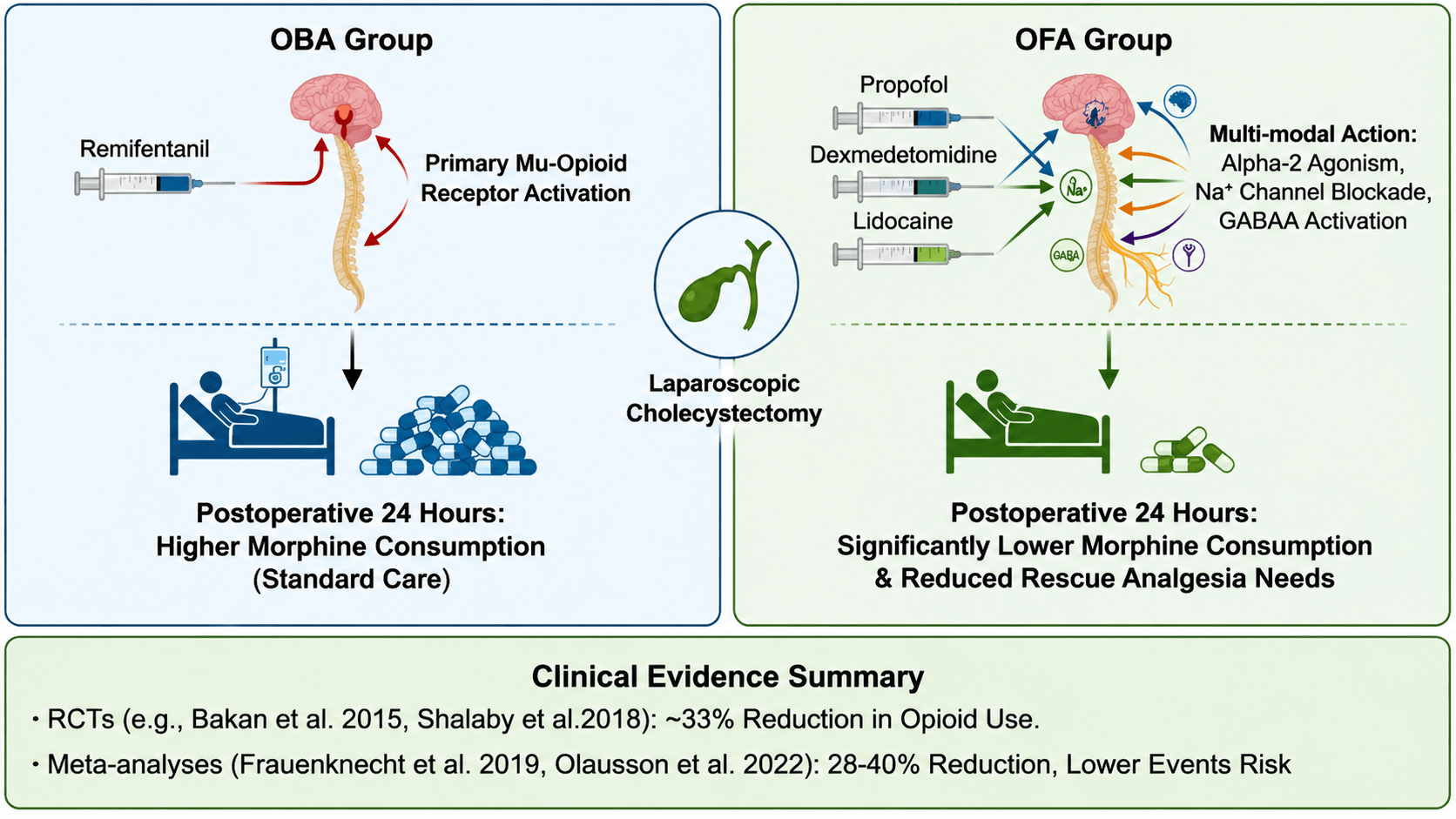 Fig. 1.
Fig. 1.
Perioperative opioid-sparing strategies: OBA vs. OFA mechanisms
and clinical outcomes [15, 17, 18, 19]. This figure is an original schematic created
by the authors for this review. The figure was created using BioRender (Toronto, ON, Canada; https://www.biorender.com). OBA, opioid-based anaesthesia; OFA, opioid-free
anaesthesia; GABAA,
The reduction in opioid consumption associated with OSA and OFA has a positive impact on multiple postoperative recovery outcomes. One of the most notable benefits is the improvement in gastrointestinal function. Opioid-induced ileus is a major contributor to delayed recovery and prolonged hospital stays, and evidence shows that OSA and OFA can accelerate the return of bowel function. In an RCT by Elsaye et al. [20], patients undergoing laparoscopic surgery who received OFA experienced a significantly shorter time to first flatus and first bowel movement compared with those in the OBA group. Similarly, a systematic review by de Boer et al. [21] reported that OSA techniques reduced the incidence of postoperative ileus by 35% and shortened the time to bowel function resumption by an average of 12 hours.
OSA and OFA also have a favorable impact on the length of hospital stay (LOS). In a retrospective cohort study by Ljungqvist et al. [22], the implementation of an enhanced recovery after surgery (ERAS) protocol incorporating OSA was associated with a 20% reduction in LOS among patients undergoing major abdominal surgery. Similarly, an RCT by Hontoir et al. [23] found that patients undergoing breast cancer surgery who received OFA had a 1.5-day shorter LOS compared with those in the OBA group. These reductions in LOS improve patient satisfaction and carry significant cost implications for healthcare systems.
A key concern regarding the adoption of OSA and OFA is the potential for inadequate pain control. However, current evidence indicates that these techniques provide comparable or even superior analgesia relative to OBA. In a systematic review by Suandika et al. [24], four of seven studies reported that the OFA group had lower mean resting pain scores at the first postoperative assessment and at 24 hours postoperatively compared with the OBA group. Similarly, a meta-analysis by Liu et al. [25] reported no significant difference in postoperative pain scores between the OFA and OBA groups, indicating that OFA does not compromise pain management.
In terms of safety, OSA and OFA are associated with a significantly reduced incidence of opioid-induced adverse events. PONV is among the most consistently observed clinical benefits. For instance, an adaptive randomized controlled trial (aRCT) by Choi et al. [26] demonstrated that patients undergoing thyroidectomy who received OFA had a PONV incidence of 17.5%, compared with 70.0% in the OBA group. Furthermore, a comprehensive meta-analysis by Olausson et al. [15] corroborated these findings, reporting that OFA was associated with a substantial reduction in the risk of both nausea (Odds Ratio [OR] 0.27) and vomiting (OR 0.22), along with a commensurate decrease in the requirement for rescue antiemetic medication.
Respiratory depression, a potentially life-threatening opioid-related complication, is also less common among patients receiving OSA or OFA. Nagappa et al. [27] conducted a systematic review of opioid-related respiratory adverse events and reported that OSA techniques reduced the risk of respiratory depression by 30% compared with OBA. This finding is especially relevant in high-risk populations, such as obese individuals and patients with obstructive sleep apnea, who face substantially increased vulnerability to OIRD.
CPSP and PPOU are long-term consequences of perioperative opioid use that carry significant implications for patient quality of life and healthcare resource utilization. Emerging evidence suggests that OSA and OFA may reduce the risk of these outcomes. Van Gulik et al. [28] conducted a prospective cohort study in patients undergoing cardiac surgery and found that the use of high-dose remifentanil was associated with a 2.5-fold increased risk of CPSP at one year postoperatively. In contrast, a study by Lavand’homme et al. [29] reported that patients undergoing major digestive surgery who received an OFA technique incorporating epidural analgesia and ketamine had a 40% lower incidence of CPSP at six months postoperatively compared with those in the OBA group.
Regarding PPOU, few studies have directly evaluated the impact of OSA and OFA, yet indirect evidence suggests a beneficial effect. Crucially, a study by Travaglini et al. [30] identified preoperative opioid use as a major risk factor for PPOU; by reducing intraoperative and postoperative opioid exposure, OSA and OFA may help interrupt the progression toward opioid dependence.
In terms of PPOU, few studies have directly evaluated the impact of OSA and OFA, but indirect evidence suggests a beneficial effect. Verla and Iqbal [31] conducted a narrative review and noted that strategies to minimize perioperative opioid use, including OSA and OFA, are associated with a reduced risk of PPOU. A study by Travaglini et al. [30] identified preoperative opioid use as a major risk factor for PPOU, and by reducing intraoperative and postoperative opioid exposure, OSA and OFA may help interrupt the progression toward opioid dependence. Future studies with long-term follow-up are warranted to clarify the relationship between OSA/OFA and PPOU.
Multimodal analgesia, defined as the use of multiple analgesic agents or techniques that act through different mechanisms to achieve effective pain control, is the foundation of OSA and OFA [32]. By targeting various pathways within the pain signaling cascade, multimodal analgesia enables the use of lower doses of individual drugs, thereby reducing the risk of adverse events while maintaining or enhancing analgesic efficacy. Key components of multimodal analgesia for OSA and OFA include non-opioid analgesics, regional anaesthesia, and adjuvant medications [33].
Non-opioid analgesics play a central role in OSA and OFA because they provide effective pain control without the adverse effects associated with opioids. Acetaminophen, a non-steroidal anti-inflammatory drug (NSAID)-like analgesic, is widely used in the perioperative period due to its favorable safety profile and potential to reduce opioid requirements [34]. A meta-analysis by Martinez et al. [35] reported that perioperative acetaminophen reduced postoperative opioid consumption by 15% and improved pain scores at 24 hours.
NSAIDs, such as ketorolac and ibuprofen, are also effective non-opioid analgesics, though the risk of gastrointestinal bleeding and renal dysfunction may limit their use. A systematic review by Doleman et al. [36] found that pre-emptive NSAID administration reduced postoperative pain scores by 20% and opioid consumption by 25% in patients undergoing various surgical procedures.
Lidocaine, a local anesthetic, is another essential non-opioid analgesic incorporated into OSA and OFA protocols. Intravenous lidocaine infusion has been shown to reduce postoperative pain scores and opioid consumption, particularly in patients undergoing abdominal surgery. Beaussier et al. [37] performed a systematic review of perioperative intravenous lidocaine and reported that it reduced postoperative pain scores at 24 hours and decreased opioid consumption by 30%. Its mechanism of action is thought to involve inhibition of voltage-gated sodium channels, thereby reducing nociceptive input and limiting central sensitization.
Regional anaesthesia techniques, including peripheral nerve blocks (PNBs) and epidural analgesia, are integral components of OSA and OFA because they provide targeted analgesia with minimal systemic adverse effects. PNBs, including femoral, sciatic, and brachial plexus blocks, are frequently used in patients undergoing orthopedic, vascular, and plastic surgery procedures [38].
Epidural analgesia remains particularly effective in individuals undergoing major abdominal, thoracic, or orthopedic surgery. Sun et al. [39] found that epidural analgesia combined with ketamine reduced the incidence of chronic postsurgical pain (CPSP) by approximately 40% in patients undergoing major digestive surgery. The addition of adjuvants, such as clonidine or dexmedetomidine, to epidural local anesthetics can further enhance analgesic potency and extend block duration. Sanchez Munoz et al. [40] performed a systematic review of clonidine in epidural analgesia and found that it prolonged the duration of analgesia by approximately 2 hours and decreased postoperative opioid requirements by 25%.
Adjuvant medications are administered alongside non-opioid analgesics and regional anaesthesia to enhance analgesia and reduce opioid use. Alpha-2 adrenergic agonists, such as clonidine and dexmedetomidine, are widely used adjuvants in OSA and OFA. These agents act by activating alpha-2 receptors in the spinal cord and brainstem, thereby inhibiting nociceptive signaling and promoting sedation and anxiolysis [41]. Blaudszun et al. [42] conducted a meta-analysis of perioperative alpha-2 agonists and reported a 20% reduction in postoperative morphine consumption and lower pain scores at 24 hours. Dexmedetomidine, which exhibits greater alpha-2 selectivity than clonidine, offers additional advantages, including improved hemodynamic stability and reduced postoperative shivering.
Ketamine, an N-methyl-D-aspartate (NMDA) receptor antagonist, is another valuable adjuvant in OSA and OFA. It functions by inhibiting NMDA receptors within the spinal cord and brain, thereby mitigating central sensitization and OIH. Brinck et al. [43] conducted a systematic review of perioperative ketamine and found that it reduced postoperative pain scores at 24 hours and decreased opioid consumption by 25%. Ketamine is particularly useful in patients with a history of opioid use or those undergoing major surgery, where the risk of OIH is heightened. Karabayirli et al. [44] conducted an RCT in patients undergoing endoscopic sinus surgery and reported that the intraoperative administration of dexmedetomidine reduced postoperative pain scores and decreased analgesic requirements compared with the control group.
Magnesium sulfate, a calcium channel antagonist, has also been examined as an adjuvant in OSA and OFA. It reduces nociceptive transmission by inhibiting NMDA receptors and decreasing calcium influx into pain-sensing neurons. Albrecht et al. [45] conducted a meta-analysis of perioperative magnesium sulfate and observed reductions in postoperative pain scores at 24 hours and opioid use by 20%. However, evidence for magnesium sulfate remains less consistent than for other adjuvants, and its application is typically reserved for patients who cannot tolerate alternative non-opioid analgesics.
The successful implementation of OSA and OFA requires careful patient selection and comprehensive assessment. Although these techniques can be applied across a broad range of patients, several factors must be considered to optimize clinical outcomes. Patient-specific factors must be considered to optimize clinical outcomes. Patient-specific variables, such as age, comorbidities, and prior opioid exposure, play a key role in determining the suitability of OSA and OFA [46].
Elderly patients are particularly vulnerable to opioid-induced adverse events, including respiratory depression and cognitive impairment, which make them ideal candidates for OSA and OFA. However, older adults often exhibit reduced organ function, potentially altering the pharmacokinetics and pharmacodynamics of non-opioid analgesics [47].
Patients with comorbidities such as chronic obstructive pulmonary disease (COPD), sleep apnea, and renal or hepatic dysfunction are also at heightened risk for opioid-related complications and may benefit from OSA and OFA strategies. Individuals with COPD have an elevated risk of OIRD, and opioid administration may exacerbate respiratory depression and increase the risk of postoperative pulmonary complications [48]. In these patients, regional anaesthesia techniques, including PNBs, should be prioritized to minimize systemic drug exposure. Patients with renal dysfunction may experience reduced clearance of non-opioid analgesics, such as NSAIDs and lidocaine, necessitating dose adjustments to prevent accumulation and toxicity.
Patients with a history of opioid use, including individuals with chronic pain or a history of substance abuse, are at increased risk of OIH, tolerance, and PPOU. These patients often require higher opioid doses to achieve adequate analgesia, thereby increasing their risk of adverse events. OSA and OFA are particularly advantageous in this population by reducing opioid exposure and limiting further tolerance and OIH. Meyer-Frießem et al. [49] conducted a systematic review of perioperative ketamine in patients with preoperative opioid use and noted a 30% reduction in postoperative pain scores and a 35% decrease in opioid consumption by 35%. However, patients with established opioid dependence may develop withdrawal symptoms during OFA, necessitating careful monitoring and appropriate perioperative management.
The type of surgical procedure also significantly influences the choice of OSA and OFA techniques. Minor surgical procedures, such as laparoscopic cholecystectomy and hernia repair, are well-suited for OFA because they are associated with moderate pain intensity and a low risk of severe postoperative complications [50]. Conversely, major surgical procedures, including cardiac, thoracic, and major abdominal operations, may require a combination of OSA and regional anaesthesia to achieve effective analgesia [51]. The expected duration of surgery is another essential consideration, as prolonged procedures may require more frequent dosing or continuous infusion of non-opioid analgesics to maintain effective pain control [52].
The selection of drugs for OSA and OFA depends on patient characteristics, the type of surgical procedure, and the desired clinical outcomes. The overarching goal is to choose a combination of agents that provides effective pain control with minimal adverse events [53]. Below is a summary of the principal drugs used in OSA and OFA, along with their recommended dosing strategies and monitoring parameters.
Clonidine and dexmedetomidine are the most frequently used alpha-2 adrenergic agonists in OSA and OFA. Clonidine is typically administered as a preoperative oral dose of 0.2 mg, followed by a continuous intravenous infusion of 1–2 mcg/kg/h during surgery [54]. Dexmedetomidine is administered as a loading dose of 0.5–1 mcg/kg over 10–15 minutes, followed by a continuous infusion of 0.2–0.7 mcg/kg/h [55]. The infusion rate should be titrated according to hemodynamic responses, with a target heart rate of 50–70 beats per minute and a mean arterial pressure of 60–80 mmHg. Vigilant monitoring for bradycardia and hypotension is essential, particularly in elderly individuals and those with pre-existing cardiac conditions [56].
Ketamine is administered as a bolus dose of 0.2–0.5 mg/kg at induction, followed by a continuous infusion of 0.1–0.5 mg/kg/h during surgery [57]. Higher doses may be required in patients with a history of opioid use or those undergoing major surgery [58]. Ketamine use may be associated with hallucinations, nightmares, and hypertension, and premedication with a benzodiazepine can help mitigate these effects [59]. Monitoring for the emergence of delirium is important, particularly among pediatric patients and young adults.
Intravenous lidocaine is administered as a bolus dose of 1–2 mg/kg at induction, followed by a continuous infusion of 1–3 mg/kg/h during surgery [60]. The infusion should be discontinued 30–60 minutes before the conclusion of surgery to prevent prolonged local anesthetic toxicity. Monitoring for signs of lidocaine toxicity, including tinnitus, perioral numbness, and seizures, is essential [61]. Patients with renal or hepatic dysfunction may require dose adjustments to avoid drug accumulation [62, 63].
Acetaminophen is administered as a preoperative oral dose of 1000 mg, followed by intravenous doses of 1000 mg every 6 hours during the postoperative period [64]. The maximum daily dose should not exceed 4000 mg to prevent hepatotoxicity. In patients with hepatic dysfunction, the total daily dose should be reduced to 3000 mg/day or less [65].
Ketorolac is the most commonly used NSAID in the perioperative period, administered as an intravenous dose of 15–30 mg every 6 hours [66]. The maximum duration of administration should not exceed 5 days to reduce the risk of gastrointestinal bleeding and renal dysfunction. Ibuprofen is also used, given as an oral dose of 400–600 mg every 6 hours [67]. NSAIDs should be avoided in patients with a history of gastrointestinal ulcers, renal dysfunction, or bleeding disorders [68].
The successful implementation of opioid-sparing anaesthesia (OSA) and opioid-free anaesthesia (OFA) depends on establishing standardized, actionable protocols that align with real-world clinical workflows, along with clear mechanisms for interdisciplinary collaboration.
The implementation of OSA and OFA requires the development of standardized protocols that clearly outline patient selection, drug choice and dosing, monitoring parameters, and the management of adverse events [69]. These protocols should be evidence-based, adapted to the specific needs of the institution, and regularly reviewed and updated based on emerging evidence and clinical experience [70]. To facilitate this process, the following template (Table 1, Ref. [15, 22, 31, 37, 42, 48, 49, 59, 61, 71]) incorporates the essential components, with practical examples grounded in the clinical evidence presented earlier. This template aims to ensure that each protocol element is not only evidence-informed but also actionable and directly applicable to daily clinical practice.
| Protocol component | Key content & operational details | Evidence-based rationale |
| Patient assessment criteria | Inclusion Criteria: Elective surgeries (e.g., laparoscopic cholecystectomy, thyroidectomy, total hip arthroplasty); high-risk populations including elderly adults ( |
Supports the identification of patients most likely to benefit from OSA/OFA, while preventing protocol use in individuals with clear contraindications to minimize the risk of adverse events [48, 49]. |
| Exclusion Criteria: Severe bradycardia (baseline HR |
||
| Drug selection/dosing matrix | Non-opioid Analgesics: Acetaminophen (1000 mg PO preoperatively; 1000 mg IV q6h postoperatively; max 4000 mg/day or 3000 mg/day in hepatic dysfunction); IV lidocaine (1–2 mg/kg bolus at induction; 1–3 mg/kg/h infusion discontinued 30–60 min before end of surgery); NSAIDs such as ketorolac (15–30 mg IV q6h, max 5 days, avoided in renal dysfunction). | Dosing aligns with meta-analyses demonstrating efficacy, such as lidocaine reducing opioid use by approximately 30% [37] and dexmedetomidine improving hemodynamic stability while enhancing analgesia [42], ensuring optimal pain control without excessive opioid exposure. |
| Adjuvants: Dexmedetomidine (0.5–1 mcg/kg loading over 10–15 min; 0.2–0.7 mcg/kg/h infusion titrated to HR 50–70 bpm and MAP 60–80 mmHg); ketamine (0.2–0.5 mg/kg bolus at induction; 0.1–0.5 mg/kg/h infusion; 0.5–1 mg/kg/h for opioid-tolerant patients). | ||
| Regional anaesthesia: Femoral nerve block (20–30 mL of 0.25% bupivacaine for total knee arthroplasty); epidural analgesia (0.125% ropivacaine + clonidine 1 mcg/mL at 5–10 mL/h for major abdominal surgery). | ||
| Intraoperative monitoring parameters | Vital Signs: HR and MAP measured every 5 minutes; continuous SpO2 and ETCO2 monitoring. | Ensures the early identification of adverse events (e.g., lidocaine toxicity [61], and ketamine-induced delirium [59]), while maintaining adequate intraoperative analgesia [15]. |
| Neurological: Sedation assessed using the Ramsay Scale (target 2–4); emergence delirium screening for patients receiving ketamine. | ||
| Toxicity Surveillance: Lidocaine (monitor for perioral numbness, tinnitus; target serum level |
||
| Pain Assessment: Nociception monitoring (e.g., NOL index |
||
| Handover checkpoints | Intraoperative-to-PACU Handover: Standardized checklist covering protocol used (OSA/OFA), drug doses and infusion duration, hemodynamic trends, pain score (0–10), and intraoperative adverse events. | Improves continuity of care throughout perioperative transitions, reducing errors in analgesic management and ensuring that all providers have consistent, critical information [71]. |
| PACU-to-Ward Handover: Details of postoperative analgesia plan (e.g., acetaminophen + ketorolac schedule), regional block duration, and rescue analgesic (e.g., oxycodone 5 mg PO for pain score |
||
| Ward-to-Discharge Handover: Discharge education and follow-up plan (e.g., 72-hour postoperative call to assess pain and opioid use). | ||
| Postoperative analgesia transition plan | 0–24 h: IV non-opioids (acetaminophen, ketorolac) with regional block support; rescue oxycodone 5–10 mg PO q4h PRN for pain score |
Aligns with enhanced recovery after surgery (ERAS) principles by minimizing opioid exposure [22] and reducing the risk of persistent postoperative opioid use (PPOU) [31] while maintaining effective pain control during recovery. |
| 24–48 h: Transition to oral non-opioids (acetaminophen 1000 mg PO q6h + ibuprofen 400–600 mg PO q6h); discontinue IV adjuvants (e.g., dexmedetomidine). | ||
| Discharge: Prescribe opioids only if pain score |
OSA, opioid-sparing anaesthesia; BMI, body mass index; COPD, chronic obstructive pulmonary disease; ASA, American Society of Anesthesiologists; PACU, post-anaesthesia care unit; ASA physical status I–V, American Society of Anesthesiologists physical status I–V (I = A normal healthy patient; II = A patient with mild systemic disease; III = A patient with severe systemic disease; IV = A patient with severe systemic disease that is a constant threat to life; V = A moribund patient who is not expected to survive without the operation); eGFR, estimated glomerular filtration rate; PRN, pro re nata (as needed); PO, per os (orally); NOL, nociception level; MAP, mean arterial pressure; ETCO2, end-tidal carbon dioxide; HR, heart rate; SpO2, peripheral capillary oxygen saturation.
The development of OSA and OFA protocols should involve a multidisciplinary team including anesthesiologists, surgeons, nurses, pharmacists, and pain management specialists. The team should begin by conducting a formal needs assessment to identify the target patient population, common surgical procedures, and current challenges in opioid management. This assessment may include a review of hospital data on opioid consumption, postoperative adverse events, and LOS [71]. To ensure that every phase of care, from preoperative preparation to postoperative discharge, is comprehensively addressed, a clear delineation of role-specific responsibilities is crucial. The following framework (Table 2) outlines the core responsibilities for key members of the perioperative team in the context of OSA/OFA implementation.
| Team member | Preoperative responsibilities | Intraoperative responsibilities | Postoperative responsibilities |
| Anesthesiologist | Conduct patient assessment to evaluate inclusion and exclusion criteria, provide patient education on OSA/OFA (e.g., describing how these approaches reduce nausea and facilitate faster recovery), and formulate an individualized analgesia plan (e.g., selecting regional blocks for orthopedic procedures). | Lead protocol execution, including drug administration and continuous monitoring; adjust medications in response to hemodynamic fluctuations (e.g., reducing dexmedetomidine for bradycardia), and perform regional blocks if applicable. | Provide structured handover to PACU personnel, monitor patients for adverse events (e.g., OIRD, lidocaine toxicity), and optimize the analgesic regimen (e.g., discontinuing ketamine if delirium develops). |
| Surgeon | Confirm the surgical procedure type (e.g., laparoscopic vs. open cholecystectomy) to support protocol selection and collaborate with the anesthesiologist in patient screening (e.g., excluding individuals with severe coagulopathy from epidural analgesia). | Communicate the intensity of surgical stimuli (e.g., “retraction of the liver”) to help adjust analgesia and avoid unnecessary surgical trauma to reduce nociception. | Assess surgical site pain, verify that recovery milestones (e.g., return of bowel function) are achieved. |
| Operating room nurse | Prepare protocol-specific medications (e.g., pre-mixing lidocaine infusions), assist with regional block setup (e.g., sterile preparation for femoral nerve blocks), and document drug administration times and doses. | Monitor vital signs and promptly alert the anesthesiologist to abnormalities (e.g., MAP |
Transfer patients to the PACU with a complete handover checklist and educate patients on postoperative pain scoring systems (e.g., “0 = no pain, 10 = worst pain”). |
| PACU nurse | Receive handover from operating room staff, verify protocol elements, monitor pain scores every 15 minutes for the first hour and every 30 minutes thereafter, and administer rescue analgesics as per protocol. | N/A (intraoperative responsibilities are limited to operating room personnel). | Assess for postoperative nausea and vomiting (PONV) at 30-minute intervals and administer antiemetics (e.g., ondansetron 4 mg IV); transition patients to oral analgesics once alert; and coordinate handover with ward nursing staff. |
| Pharmacist | Review protocol medications for potential interactions (e.g., avoiding NSAIDs in patients on warfarin), ensure availability of protocol-specific drugs in operating room and PACU (e.g., dexmedetomidine), and provide dosing guidance (e.g., adjusting lidocaine for renal dysfunction). | N/A (intraoperative responsibilities are limited to medication preparation). | Review postoperative medication lists to avoid duplication (e.g., overlapping acetaminophen doses) and counsel patients on discharge medications (e.g., “Take ibuprofen with food to minimize stomach upset”). |
OIRD, opioid-induced respiratory depression; N/A, not applicable.
The team should review the current evidence on OSA and OFA to identify the most effective drugs and techniques for the target population [72]. This review should include RCTs, systematic reviews, and meta-analyses, as well as clinical practice guidelines from professional bodies such as the American Society of Anesthesiologists (ASA) and the European Society of Anesthesiology and Intensive Care (ESAIC).
Based on the needs assessment and evidence review, the team should develop draft protocols outlining patient selection criteria, drug selection and dosing for OSA and OFA, monitoring parameters, management of adverse events, and postoperative pain management plans. The draft protocols should then be pilot-tested in a small group of patients to evaluate feasibility and effectiveness [73]. Feedback from healthcare providers and patients should be collected and used to refine the protocols before full implementation.
To evaluate the effectiveness of OSA and OFA implementation, hospitals should track both clinical and operational KPIs, comparing baseline data with post-implementation outcomes to identify areas for improvement and validate the added value of these techniques. These metrics provide objective indicators of success, supporting ongoing adoption and institutional commitment.
Clinical KPIs include postoperative opioid consumption (reported in oral
morphine equivalents [OME] at 24 and 48 hours post-operation, targeting at least
a 30% reduction from baseline [19]); incidence of PONV (aiming for
Operational KPIs include length of hospital stay (LOS), with a target of
Data for these KPIs can be extracted from electronic health records (EHRs) for opioid consumption and LOS, nursing documentation for pain scores and PONV, and post-discharge surveys for patient satisfaction, ensuring a comprehensive evaluation of implementation success.
One of the main barriers to the implementation of OSA and OFA is the concern among healthcare providers that these techniques may not provide adequate pain control. This concern is often rooted in limited experience with non-opioid analgesics and regional anaesthesia, as well as misconceptions about the effectiveness of these approaches [74]. To address this barrier, healthcare providers should be educated on the latest evidence supporting the efficacy of OSA and OFA and given opportunities to gain hands-on experience with these techniques [75].
Healthcare providers should receive structured education on the current evidence supporting the analgesic efficacy of OSA and OFA. This education may include reviews of meta-analyses and RCTs that demonstrate that OSA and OFA provide comparable or superior pain control relative to OBA [76]. Olausson et al. [15] reported no significant difference in postoperative pain scores between OFA and OBA groups, while Frauenknecht et al. [19] showed that OFA was associated with a reduction in PONV without compromising analgesia.
Hands-on training is essential for building confidence in the use of OSA and OFA. This may include shadowing experienced anesthesiologists who routinely apply these techniques, participating in workshops on regional anaesthesia, and practicing drug dosing and monitoring in simulation settings. Simulation training is particularly useful for rehearsing the management of adverse events, such as lidocaine toxicity and bradycardia, that may occur infrequently in routine clinical practice [77].
Pilot projects can also be employed to demonstrate the effectiveness of OSA and OFA in a controlled cohort, thereby increasing provider confidence before full-scale implementation. For example, a pilot project could be conducted in patients undergoing laparoscopic cholecystectomy, comparing outcomes between a small OFA group and a control group receiving OBA [78]. The results of such pilots should be shared with the interdisciplinary team as evidence of the clinical benefits of OSA and OFA.
Resource constraints, including limited access to regional anaesthesia equipment and personnel, can also pose significant barriers to OSA and OFA implementation. To address these limitations, hospitals should prioritize resource allocation to support these techniques and explore innovative strategies to overcome operational constraints.
Hospitals should allocate adequate resources to support the adoption of OSA and OFA, including the procurement of regional anaesthesia equipment and the recruitment of additional personnel such as nurse anesthetists and pain management specialists. Additionally, institutions should consider investing in EHR systems that can be used to collect and analyze OSA/OFA outcome data, thereby supporting quality improvement efforts.
Innovative solutions can further help mitigate resource constraints. Telemedicine can provide remote support to anesthesiologists in rural or underserved areas who may have limited experience with regional anaesthesia. Additionally, nurse-led pain management teams can be established to support postoperative management for patients receiving OSA and OFA, thereby reducing the workload placed on anesthesiologists.
Changing organizational culture is another significant barrier to the implementation of OSA and OFA. This requires shifting from a culture that relies heavily on opioids for pain control to one that prioritizes opioid minimization and multimodal analgesia [79]. To achieve this shift, hospital leadership should be actively involved in supporting the implementation of OSA and OFA and should communicate the importance of these techniques to all healthcare providers. Hospital leadership should provide visible support for implementation of OSA and OFA, including allocating resources, approving changes to policies and procedures, and recognizing the efforts of healthcare providers who adopt these techniques [80]. Leadership should also communicate the goals of OSA and OFA across the institution, emphasizing the benefits for patients, healthcare providers, and the hospital as a whole.
Interdisciplinary teams should be established to guide the implementation of OSA and OFA and to promote collaboration and communication among healthcare providers [81]. These teams should meet regularly to review outcome data, address challenges, and share best practices. By working together, healthcare providers can develop a shared vision for opioid minimization and collectively work toward achieving common goals. Recognition and incentives may also be used to encourage healthcare providers to adopt OSA and OFA practices.
Sharing real-world success stories can help overcome skepticism and offer a practical roadmap for implementation. For example, a tertiary academic center in Belgium [29] successfully implemented an opioid-sparing protocol combining ketamine and epidural analgesia for patients undergoing major digestive surgery. This institutional approach not only optimized acute pain control but also resulted in a 40% lower incidence of CPSP at six months post-operation. Furthermore, comprehensive evidence from recent meta-analyses [15] reinforces that the systematic institutional integration of multimodal agents, such as dexmedetomidine, can reliably reduce postoperative opioid consumption and decrease the incidence of acute adverse events like PONV, facilitating a shorter LOS.
A U.S. community hospital focused on OSA for total knee arthroplasty, incorporating acetaminophen, lidocaine, and femoral nerve blocks. This approach reduced PONV by 60%, shortened PACU stay by 20%, and achieved 90% patient satisfaction, supported by nurse-led pain teams and targeted equipment investment.
A Canadian rural hospital [78] simplified OFA protocols for laparoscopic surgery (using propofol and dexmedetomidine) and leveraged telemedicine for regional anaesthesia support, resulting in 33% lower opioid use, no increase in pain scores, and zero cases of OIRD, demonstrating that OSA/OFA can be successfully implemented even in resource-limited settings. These cases collectively demonstrate that with appropriate strategies, barriers to OSA and OFA adoption can be effectively overcome, leading to improved patient outcomes and reduced opioid-related harm.
A critical premise for the clinical application of opioid-free anaesthesia (OFA) is to clarify that its primary goal is opioid minimization rather than rigid adherence to absolute opioid avoidance. This distinction reflects the need to balance the benefits of opioid reduction with the fundamental requirement for adequate perioperative pain control. In clinical practice, certain scenarios, such as major complex surgeries (e.g., extensive thoracic or abdominal resections) involving intense nociceptive stimulation, or patients with pre-existing severe chronic pain and opioid tolerance, may render non-opioid analgesic regimens insufficient to control acute pain. In such cases, short-term, low-dose opioid administration (e.g., a small bolus of remifentanil during peak surgical stimulation) is not only clinically justifiable but necessary to prevent the adverse consequences of uncontrolled pain, including excessive sympathetic activation, intraoperative hemodynamic instability, and an increased risk of chronic postsurgical pain (CPSP) mediated through central sensitization. This goal-oriented approach ensures that OFA does not become a dogmatic protocol but remains a flexible strategy tailored to individual patient needs.
The selection of OFA requires a rigorous assessment of patient-specific factors
and the pharmacological characteristics of non-opioid alternatives, as several
conditions represent clear contraindications to the implementation of OFA. First,
contraindications related to key non-opioid analgesics are essential to consider.
For
For ketamine, relative contraindications include a history of schizophrenia, bipolar disorder, or severe anxiety disorders, as its dissociative effects may trigger acute exacerbation of psychotic symptoms or emergence of delirium. Patients with active substance use disorders involving dissociative agents (e.g., phencyclidine) are also at heightened risk of adverse psychological reactions to ketamine, warranting heightened caution. For intravenous lidocaine, severe hepatic dysfunction (e.g., Child-Pugh Class C cirrhosis) or a history of lidocaine-induced seizures constitutes an absolute contraindication, due to impaired hepatic metabolism that may lead to drug accumulation and increased risk of central nervous system (CNS) toxicity (e.g., tinnitus, perioral numbness, or generalized seizures). Second, patient-specific physiological states further limit the applicability of OFA. Pregnant patients in the third trimester are generally excluded from ketamine-based OFA, as ketamine crosses the placental barrier and may transiently influence fetal CNS development. Patients with severe chronic obstructive pulmonary disease (COPD) in acute exacerbation may also be unsuitable for high-dose dexmedetomidine, as even mild sedation can reduce respiratory drive and worsen hypercapnia.
The non-opioid analgesics central to OFA regimens are associated with distinct
safety risks, which may be amplified in high-risk patient populations and
therefore require targeted monitoring and management. Dexmedetomidine-associated
bradycardia and hypotension are particularly concerning in elderly patients
(
Ketamine’s psychotomimetic effects, including hallucinations, vivid dreams, and disorientation, are more common in young adults (18–30 years) and in patients with a history of anxiety disorders. These manifestations typically occur during emergence from anaesthesia. Although premedication with a low-dose benzodiazepine (e.g., midazolam 0.5–1 mg) can attenuate these effects, high-risk patients may require extended post-anaesthesia care unit (PACU) observation to ensure resolution of psychological symptoms. Additionally, ketamine’s sympathomimetic activity (e.g., increased blood pressure and heart rate) may present risks in patients with uncontrolled hypertension or coronary artery disease, as transient elevations in myocardial oxygen demand could precipitate myocardial ischemia.
Lidocaine toxicity remains a significant safety concern, especially in patients
with renal dysfunction or those receiving medications that impair lidocaine
metabolism (e.g., propranolol, a cytochrome P450 inhibitor). Even within
recommended infusion ranges (1–3 mg/kg/h), patients with end-stage renal disease
(ESRD) may experience delayed clearance and progressive accumulation, manifesting
initially as mild CNS symptoms (e.g., dizziness) and potentially advancing to
severe toxicity such as tonic-clonic seizures. Intraoperative monitoring of
lidocaine plasma concentrations (target
The advantages of OSA and OFA in the perioperative domain have been demonstrated across multiple dimensions through growing clinical evidence. Their core value lies not only in reducing opioid-related adverse reactions but also in their positive impact on long-term outcomes. This includes an approximately 40% reduction in the risk of chronic postsurgical pain (CPSP) and a decreased likelihood of persistent postoperative opioid use (PPOU). At the same time, these strategies reduce healthcare resource utilization by shortening the length of hospital stay (LOS). The beneficial impact of OSA and OFA spans the entire perioperative continuum. Preoperatively, they lower patients’ tolerance and dependence on opioids by minimizing exposure, especially in high-risk populations such as the elderly, obese individuals, and patients with chronic obstructive pulmonary disease (COPD), significantly reducing the risk of severe opioid-related adverse effects such as respiratory depression. Intraoperatively, precise multimodal analgesia reduces hemodynamic fluctuations and enhances anaesthetic safety. Postoperatively, they accelerate gastrointestinal recovery and reduce the incidence of PONV, improving early mobilization and oral intake, thereby shortening the rehabilitation cycle and improving patient satisfaction.
From a clinical perspective, patients undergoing laparoscopic cholecystectomy with OFA have demonstrated a 33%–40% reduction in postoperative 24-hour morphine consumption compared with those receiving traditional opioid-based anaesthesia (OBA), with no significant difference in pain scores. This highlights that such protocols can effectively improve postoperative experience while maintaining analgesia.
Future research should prioritize addressing existing evidence gaps. Longitudinal studies examining long-term outcomes should extend follow-up to 1–3 years to better clarify the sustained value of OSA/OFA in chronic pain management. Additionally, individualized regimens tailored to special populations (e.g., children, pregnant women, patients with end-stage renal disease) warrant further investigation. Based on the pharmacokinetic characteristics of these populations, optimized dosing and administration strategies for non-opioid analgesics are needed to address current limitations in clinical guidelines. Furthermore, integration of digital technologies may enable precise, automated, and adaptive medication regimens for OSA/OFA, thereby improving efficiency and safety.
At the same time, existing studies still have several limitations: most clinical trials emphasize short-term outcomes (e.g., pain scores at 24–48 hours postoperatively, length of hospital stay), with insufficient investigation into their long-term impact on physiological functions (e.g., cognitive function, immune function). The study populations are predominantly patients undergoing elective procedures, resulting in limited evidence on the applicability of these techniques in emergency surgeries and complex major operations. Additionally, a study has small sample sizes and geographical limitations, which restrict the generalizability of its findings.
To address these limitations, improvement strategies should be implemented from both research design and clinical translation perspectives. Meanwhile, doctor-patient communication and education should be enhanced. Through popular science materials, preoperative interviews, and related approaches, patients should be informed about the advantages and safety profiles of OSA/OFA to alleviate their concerns about “opioid-free” approaches, enhance patient acceptance and cooperation, and facilitate the transition of these techniques from academic research to routine clinical practice, ultimately advancing innovation and optimization of the perioperative pain management model.
Opioid-sparing anaesthesia (OSA) and opioid-free anaesthesia (OFA) represent important advances in perioperative care, providing safer and more patient-centered alternatives to traditional opioid-based anaesthesia. Current evidence demonstrates that these techniques reduce opioid consumption, enhance postoperative recovery outcomes, and decrease opioid-related harms, without compromising analgesic effectiveness. However, their integration into routine hospital practice remains limited due to concerns about inadequate pain control, resource constraints, and challenges in interdisciplinary collaboration. Current research consistently shows that both OSA and OFA significantly reduce perioperative opioid use and opioid-induced adverse events while maintaining comparable or improved pain control relative to conventional opioid-based anaesthesia. Furthermore, multimodal analgesia, which combines non-opioid analgesics, regional anaesthesia, and adjuvant agents, serves as the irreplaceable foundation for OSA/OFA, with individualized drug selection and dosing further optimizing clinical outcomes.
Importantly, successful implementation relies on standardized, evidence-based protocols and coordinated interdisciplinary collaboration, although practical barriers, including provider unfamiliarity with non-opioid strategies and limited access to regional anaesthesia resources, continue to hinder widespread adoption. These observations underscore the need for targeted interventions: hospitals should prioritize structured training programs to strengthen provider confidence in OSA/OFA and allocate resources to expand access to essential equipment and personnel. At the same time, limitations in current research must be acknowledged. Most studies emphasize short-term outcomes (e.g., 24–48-hour pain scores, length of hospital stay) rather than long-term endpoints, such as PPOU or CPSP, in diverse patient populations, leaving gaps in understanding how best to tailor OSA/OFA for high-risk or understudied patient groups.
This review provides a practical guide for applying OSA and OFA in hospital settings, with a focus on multimodal analgesia, interdisciplinary collaboration, and real-world implementation considerations. It has summarized key clinical principles for OSA/OFA use, including patient selection, drug choice and dosing, and monitoring parameters. It has also outlined strategies for addressing implementation challenges, such as establishing standardized protocols, enhancing interdisciplinary training and patient education, and engaging in continuous quality improvement and monitoring. By adopting the strategies described, healthcare providers can successfully integrate OSA and OFA into routine practice, advancing perioperative care through opioid minimization. This not only improves patient outcomes but also aligns with global initiatives aimed at addressing the opioid epidemic and optimizing medication safety.
Future research should prioritize long-term outcomes, such as the influence of OSA and OFA on PPOU and CPSP, and identify the most effective implementation strategies across diverse healthcare settings. Through sustained investigation and innovation, OSA and OFA have strong potential to transform perioperative practice, offering safer and more effective pain management and facilitating faster postoperative recovery.
• A practical guide for hospital implementation of OSA and OFA, outlining principles, techniques, and evidence in the context of opioid-induced perioperative side effects.
• Multimodal analgesia is central to OSA/OFA, with evidence showing reduced opioid use, lower incidence of PONV, and improved bowel recovery without compromising pain control.
• Successful OSA/OFA requires careful patient selection, evidence-based drug administration, standardized protocols, and interdisciplinary collaboration to achieve optimal outcomes.
• This study examines the barriers and solutions to OSA/OFA implementation, with a focus on education, training, and leadership support to enhance opioid safety.
Not applicable.
QSZ and HL conceived the review manuscript, carried out the literature searches and wrote the first draft. YM and JLL made contributions to the conception and design of the study. All authors reviewed and critically revised the manuscript for important intellectual content, approved the final manuscript, and agreed to be accountable for all aspects of the work.
Not applicable.
Not applicable.
This research received no external funding.
The authors declare no conflicts of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.