




 , Rui Xie 2, Sile Hu 2, Yuhang Lv 2, Tianjiao Ma 3, Huricha Zhao 2, He Zhang 2, Zejian Jin 2, Hongxia Sun 4, Fei Yan 2,*
, Rui Xie 2, Sile Hu 2, Yuhang Lv 2, Tianjiao Ma 3, Huricha Zhao 2, He Zhang 2, Zejian Jin 2, Hongxia Sun 4, Fei Yan 2,*
1 Affiliated Tongliao Clinical College of Inner Mongolia Medical University, 028000 Tongliao, Inner Mongolia, China
2 Orthopedics Center, Tongliao People’s Hospital, 028000 Tongliao, Inner Mongolia, China
3 Department of Surgical Nursing, Orthopedics Center, Tongliao People’s Hospital, 028000 Tongliao, Inner Mongolia, China
4 Medical Records Department, Tongliao People’s Hospital, 028000 Tongliao, Inner Mongolia, China
Abstract
Acromioclavicular (AC) joint dislocation is associated with severe pain, functional impairment, and postoperative complications. This study aimed to compare the efficacy and safety of TightRope with hook plate fixation for Rockwood type III injuries and to develop a postoperative complication prediction model.
This retrospective study enrolled 178 patients with acute Rockwood type III AC joint dislocation who underwent surgical treatment at Tongliao People’s Hospital, China, between January 2020 and December 2023. Among them, 93 patients received arthroscopic TightRope fixation and 85 underwent conventional hook plate fixation. Perioperative parameters, radiographic outcomes, functional recovery, and complication rates were compared between the two groups. Linear regression was employed to identify factors influencing key recovery indicators, and a logistic regression model was constructed to predict complications.
The TightRope group exhibited significantly less intraoperative trauma, as indicated by reduced blood loss and shorter incision length (both p < 0.001). Postoperative infection was less frequent with TightRope (2.15% vs. 10.59%). At 6 months postoperatively, radiographic parameters—including coracoclavicular distance (CCD), acromioclavicular distance (ACD), and acromioclavicular index (ACI)—and functional outcomes (American Shoulder and Elbow Surgeons [ASES], Constant–Murley, and University of California, Los Angeles [UCLA] scores) demonstrated improvement in the TightRope group, along with lower visual analog scale (VAS) pain scores (all p < 0.05). Linear regression analysis identified operation type, intraoperative blood loss, and implant displacement as independent predictors of recovery. Logistic regression revealed TightRope as an independent protective factor for complications (odds ratio [OR] = 0.42, p = 0.028), whereas blood loss (OR = 1.86, p = 0.017) and ACD (OR = 1.34, p = 0.042) were independent risk factors. The prediction model showed good discrimination in the training set (area under the curve [AUC] = 0.84, 95% confidence interval [CI]: 0.76–0.92) and validation set (AUC = 0.76, 95% CI: 0.64–0.89), with satisfactory calibration (Hosmer–Lemeshow p = 0.177, p = 0.477) and clinical utility demonstrated by decision curve analysis.
Compared with hook plate fixation, the TightRope technique offers superior stabilization, improved functional recovery, and reduced complication rates in the management of acromioclavicular joint (ACJ) dislocations. The proposed predictive model provides a valuable tool for preoperative risk assessment and surgical decision-making.
Keywords
- acromioclavicular joint
- joint dislocations
- bone plates
- risk factors
- prognostic factors
Acromioclavicular joint (ACJ) dislocation is a common shoulder injury, particularly among young and physically active individuals, and predominantly results from sports-related trauma or a direct impact. Epidemiological data indicate that ACJ injuries account for approximately 9–12% of all shoulder injuries, occurring most frequently in young male athletes [1]. The estimated incidence is roughly 1.8 per 10,000 individuals globally, with a strong association with contact sports such as rugby and hockey [2, 3].
Radiographic and clinical assessment commonly follows the Rockwood classification system, where higher injury grades such as III, IV, V, and VI indicate increasing vertical and/or horizontal instability [4]. For Rockwood type III injuries, surgical fixation is often recommended, particularly in patients with significant instability or high functional demands, although the optimal surgical strategy for managing these injuries remains a point of debate [5]. Traditional clavicular hook plate can restore joint alignment by immediate reconstruction of the acromioclavicular relationship [6], but multiple studies report several complications, including subacromial impingement, bony changes of the distal clavicle or acromion, persistent discomfort, and a frequent need for implant removal [7, 8].
Arthroscopic TightRope fixation, a minimally invasive approach, has emerged as a promising option due to its preservation of acromial anatomy and lack of routine implant removal [9]. Compared with hook plate fixation, TightRope approach demonstrates shorter incision, less intraoperative blood loss, and alleviated postoperative pain assessed through visual analog scale (VAS), with postoperative functional outcomes by American Shoulder and Elbow Surgeons (ASES), Constant–Murley, and University of California, Los Angeles (UCLA) scores that are comparable or often better, whereas overall complication rates, such as infection and reoperation, are considerably lower [10, 11, 12]. A meta-analysis indicates that while differences in VAS, Constant–Murley scores, and coracoclavicular distance (CCD) restoration are often small, the TightRope approach effectively reduces the likelihood of reoperations and subacromial bony changes [10].
Despite extensive advances in surgical approach-related investigations, integrated assessments examining radiographic reduction quality, functional recovery, and risk factors for postoperative complications remain limited. To our knowledge, there is limited evidence on combining clinical and imaging variables to develop predictive models for individualized risk assessment before surgery.
Therefore, this study compares the efficacy and safety of arthroscopic TightRope with conventional hook plate fixation, identifies independent risk factors that shape postoperative complications and functional outcomes, and develops a complication-prediction model integrating clinical variables with radiographic indices. The study aims to provide practical, evidence-based guidance for surgical decision-making and perioperative management in patients with Rockwood III acromioclavicular (AC) dislocations.
This single-center retrospective cohort study enrolled 178 patients with acute Rockwood type III ACJ dislocation who received surgical interventions at Tongliao People’s Hospital, China, between January 2020 and December 2023. Initially, 185 patients were screened according to predetermined inclusion-exclusion criteria; 178 patients who met the eligibility criteria were included in the final analysis.
Based on the surgical approach, patients were divided into two groups: arthroscopic TightRope fixation (n = 93) and conventional open hook plate fixation (n = 85) (Fig. 1). In this non-randomized, observational study, the selection of an appropriate surgical procedure was a joint decision of the surgeon and patient after assessing the severity of the dislocation, patient preferences, and the surgeon’s expertise in surgical indications.
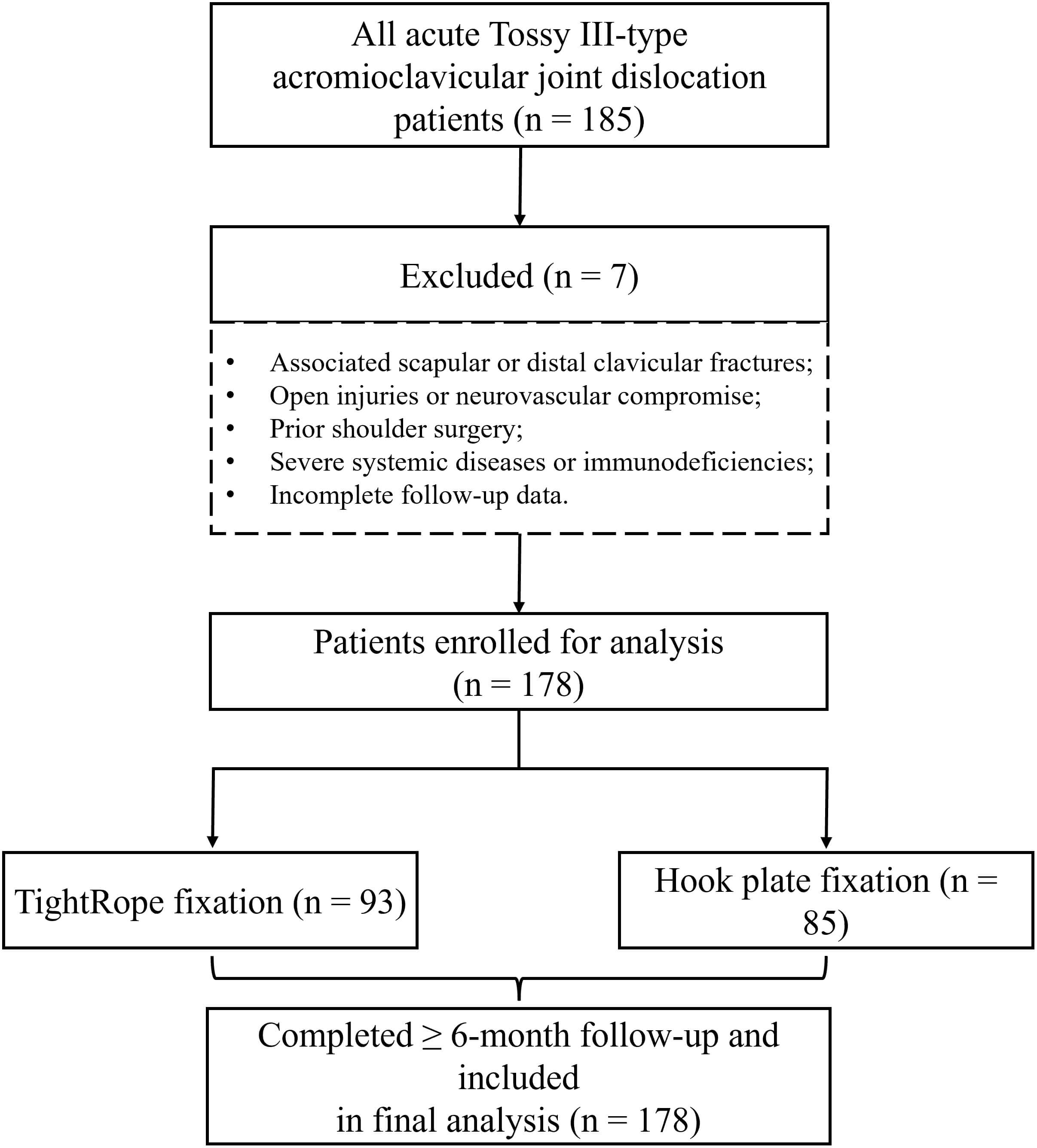 Fig. 1.
Fig. 1.
A flow chart of patient selection and study design. Fig. 1 was created using BioRender (https://biorender.com), an online platform for scientific illustration. The authors declare that they have no financial, commercial, or personal relationship with BioRender. The use of this software is solely for figure creation and does not imply any endorsement by the authors or by the platform.
As previously reported [11, 13], a clinically meaningful difference in
functional scores between procedures is generally 3–5 points, with an expected
standard deviation of approximately 10. Using a two-sided
All surgical procedures were performed by a specialized trauma team of four board-certified orthopedic surgeons. Standardized operative protocols were used for all cases. Regular training sessions and case discussions were performed to maintain consistency in the procedures and reduce bias. Complete clinical records, including imaging, surgical procedure data, and validated functional scores, were obtained for all patients, and the patients were followed up for 6 months after the procedure.
Patients’ inclusion criteria included adults aged 18 to 65 years with a confirmed Rockwood type III ACJ dislocation who underwent arthroscopic TightRope or open hook plate fixation, volunteered for a minimum 6-month follow-up assessment, and had complete imaging, surgical, and functional assessment data available. However, patients were excluded from the study cohort if they had associated scapular or distal clavicular fractures, open injuries or neurovascular compromise, a history of shoulder surgery, severe systemic disease or immunodeficiency, or incomplete follow-up data.
Under general anesthesia, patients in the TightRope group were placed in the beach-chair position. Standard arthroscopic portals were established to access the glenohumeral joint and determine any intra-articular integrity, such as superior labrum anterior and posterior (SLAP) lesions or rotator cuff pathology. After exposing the coracoid under arthroscopy, a small clavicle incision was made to establish an auxiliary tunnel. A guidewire was used to create a transosseous channel, after which the TightRope device was inserted. Once the appropriate positioning of subcoracoid and subclavicular buttons was confirmed, the fixation was secured by tensioning the sutures. Intraoperative fluoroscopy was used throughout to confirm appropriate ACJ reduction. Finally, the joint was irrigated, soft tissues were closed in layers, and a sterile compression dressing was applied.
In the hook plate group, patients underwent general anesthesia and were placed in the beach-chair position. A longitudinal incision of approximately 8 cm was made over the ACJ to expose the distal clavicle and acromion. An appropriately contoured hook plate was selected, with the hook inserted posterior and inferior to the acromion, and the plate shaped to fit the clavicle. Fixation was achieved with locking screws. Intraoperative fluoroscopy was used to assess joint reduction and range of motion to ensure there was no acromion impingement. After thorough lavage, the wound was closed in layers, and a compression dressing was applied.
All patients received standardized perioperative care, including 1–2 days of prophylactic antibiotics, pain management with nonsteroidal anti-inflammatory drugs (NSAIDs) or adjusted analgesia as needed, local cold therapy, and routine wound care. Shoulders were immobilized in an abduction brace for 6 weeks, with restriction of active upper limb motion. Only passive flexion (not exceeding 90°) and abduction exercises were allowed to reduce the risk of superior humeral head impingement or implant displacement. After 6 weeks, patients gradually resumed active range-of-motion exercises, including flexion, abduction, and rotation, while avoiding weight-bearing activities for the first 12 weeks. From 3 months onward, patients progressed to resistance-based shoulder strengthening, such as elastic-band work and scapular stabilization training.
Follow-up radiographs were obtained immediately after surgery and then at 1-, 3-, and 6-month time points to monitor implant position and joint alignment. However, preoperative and 6-month postoperative imaging measures were included in data analysis. Rehabilitation was guided by a standardized, phase-based protocol, with adjustments in intensity and progression for older patients or those with reduced muscle strength. All rehabilitation sessions were supervised by certified therapists in the hospital’s sports rehabilitation center to ensure standardization while enabling individualized care.
Baseline characteristics included age, sex, body mass index (BMI), injured side (left or right), and the time from injury to surgery (days). Preoperative and 6-month postoperative imaging data were recorded using standard anteroposterior radiographs or computed tomography (CT) scans.
The study assessed four radiographic and biomechanical parameters. The coracoclavicular distance (CCD) was determined as the vertical distance between the coracoid tip and the inferior cortex of the clavicle on the injured side, serving as an indicator of vertical ACJ stability. The acromioclavicular distance (ACD) was defined as the horizontal distance between the acromion and the distal clavicle, reflecting horizontal stability of the joint. Furthermore, the acromioclavicular index (ACI) was calculated as the ratio of the CCD on the affected side to the CCD on the contralateral, unaffected side (ACI = CCDaffected/CCDunaffected). The index was calculated both preoperatively and at 6 months postoperatively to assess anatomic restoration of the acromioclavicular joint. Finally, implant shift was determined as the maximum displacement (in millimeters) of the fixation device from its initial intraoperative position, assessed from serial radiographs obtained immediately after surgery and 1, 3, and 6 months.
Functional outcomes were extracted from patient medical records. Two orthopedic surgeons specializing in shoulder and elbow surgery, each with more than five years of clinical experience, independently assessed the patients at baseline (preoperatively and at the 6-month follow-up).
Shoulder function was assessed using the ASES Standardized Shoulder Assessment
questionnaire, specifically the patient self-report section, which evaluates pain
and activities of daily living (ADL). Pain was measured on a 0–10 VAS, with 0
representing no pain and 10 the worst pain imaginable. The pain subscore was
calculated as follows: Pain subscore = 5
Additional measurements included the Constant–Murley score [16, 17] (maximum score: 100), including pain (15 points), activities of daily living (20 points), range of motion (40 points), and strength (25 points).
The UCLA score [18, 19] (maximum 35 points) incorporating pain, function, active forward flexion, strength, and patient satisfaction used to evaluate short- to mid-term postoperative outcomes; and the VAS for pain on 0 to 10 scale using standard instruments, where 0 indicates no pain and 10 represents worst imaginable pain [20].
Operative and perioperative variables were extracted from standardized surgical and anesthesia records to ensure data consistency. Variables included operative time (minutes) (the time measured from skin incision to final suture closure), incision length (cm) (maximum length of the surgical incision reflecting surgical invasiveness), and intraoperative blood loss (mL) (estimated blood loss estimated from suction canister volumes and gauze counts, serving as an indirect measure of surgical trauma).
Postoperative complications within 6 months included implant loosening or breakage (TightRope or hook plate), surgical site infection, recurrent or residual dislocation, subacromial impingement syndrome (specific to the hook plate group), heterotopic ossification of the ACJ, and nerve compression symptoms in the operative field. Two members of the research team, along with the treating orthopedic surgeon, assessed and confirmed complications using follow-up notes, surgical records, and radiological evidence. For statistical analysis, complications were coded as a binary outcome (Yes = 1, No = 0), defined by the occurrence of any listed complication.
Clinical and imaging data were obtained from the hospital electronic medical record (EMR) system and the Picture Archiving and Communication System (PACS). Surgical parameters, including operative time, blood loss, and incision length, were uniformly extracted from intraoperative anesthesia and surgical records to minimize retrospective bias. All variables were manually entered by two independent researchers and cross-checked; any discrepancies were resolved by a third reviewer to ensure data accuracy and consistency.
Imaging measurements were conducted independently by two investigators who were
blinded to treatment group allocation—a radiology attending and a sports
medicine specialist. If measurements differed by more than a predefined threshold
(greater than 5% or
Statistical analyses were performed in R software (version 4.3.0, R Foundation for Statistical Computing, Vienna, Austria), using the tidyverse, car, rms, receiver operating characteristic curve package (pROC), ResourceSelection, caret, ggplot2, and MASS packages.
Normality of continuous variables was assessed using the Shapiro-Wilk test.
Normally distributed variables were expressed as mean
To identify key determinants associated with radiographic and functional
outcomes, multivariate linear regression models were constructed using the
6-month postoperative CCD and Constant–Murley shoulder score as dependent
variables. Variables included operation type, implant shift, incision length,
intraoperative blood loss, ACI, surgical delay, BMI, operation time, and injured
side. Before model construction, multicollinearity was assessed using variance
inflation factors (VIFs), and variables with severe collinearity (VIFs
Postoperative complications were analyzed as a binary outcome (yes = 1, no = 0)
using a logistic regression analysis. The entire data set was randomly split at
7:3 into training (n = 124) and validation (n = 54) sets. In the training set,
univariate logistic regression identified candidate predictors (p
Model performance was evaluated using the receiver operating characteristic (ROC) curve and area under the curve (AUC) with the pROC package. Calibration was assessed using calibration plots constructed with the rms package, and model goodness-of-fit was tested using the Hosmer–Lemeshow (HL) test. Furthermore, clinical usefulness was evaluated using decision curve analysis (DCA) performed with the ggDCA package. Additionally, we determined accuracy, sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) from confusion matrix-derived metrics; the classification threshold was selected by the maximum Youden index (sensitivity + specificity – 1). Finally, the trained model was then applied to the validation set, and the same performance metrics were reassessed to evaluate model robustness and generalizability.
This analysis enrolled 178 patients, with 93 (52.25%) treated with TightRope
and 85 (47.75%) with a hook plate. There were no statistically significant
differences between the two groups in terms of age, BMI, time from injury to
surgery, sex distribution, or side of injury (all p
| Variable | Hook plate group (n = 85) | TightRope group (n = 93) | Statistic | p-value | |
| Age (years), mean |
39.35 |
37.33 |
t = 1.47 | 0.144 | |
| BMI (kg/m2), mean |
25.09 |
24.91 |
t = 0.39 | 0.698 | |
| Surgery delay (days), mean |
5.62 |
5.15 |
t = 1.54 | 0.125 | |
| Sex, n (%) | 0.830 | ||||
| Female | 25 (29.41) | 26 (27.96) | |||
| Male | 60 (70.59) | 67 (72.04) | |||
| Injury, n (%) | 0.151 | ||||
| Right | 42 (49.41) | 36 (38.71) | |||
| Left | 43 (50.59) | 57 (61.29) | |||
t, independent samples t-test;
There were significant differences in perioperative outcomes between the two
groups. The TightRope group had a slightly longer operative time (56.78
| Variable | Hook plate group (n = 85) | TightRope group (n = 93) | Statistic | p-value |
| Operation time (min) | 53.50 |
56.78 |
t = –4.76 | |
| Incision length (cm) | 8.14 |
3.95 |
t = 43.45 | |
| Blood loss (mL) | 71.04 |
45.31 |
t = 7.15 |
Within 6 months postoperatively, the overall complication rate was substantially
lower in the TightRope group than the hook plate group (5.38% vs. 40.0%;
| Variable | Hook plate group (n = 85) | TightRope group (n = 93) | Statistic | p-value |
| Loose broken implant, n (%) | 6 (7.06) | 1 (1.08) | Fisher’s exact test | 0.096 |
| Infection, n (%) | 9 (10.59) | 2 (2.15) | 0.020 | |
| Redislocation, n (%) | 4 (4.71) | / | - | - |
| Impingement, n (%) | 7 (8.24) | / | - | - |
| Heterotopic ossification, n (%) | 5 (5.88) | 2 (2.15) | Fisher’s exact test | 0.372 |
| Nerve compression, n (%) | 3 (3.53) | / | - | - |
| Overall complication | 34 (40.00) | 5 (5.38) |
Note:
Baseline radiographic parameters (CCD, ACD, and ACI) did not differ between the
two groups (all p
| Variable | Hook plate group (n = 85) | TightRope group (n = 93) | Statistic | p-value |
| CCD Pre (mm) | 15.52 |
15.61 |
t = –0.24 | 0.809 |
| CCD Post (mm) | 8.00 |
6.96 |
t = 4.22 | |
| ACD Pre (mm) | 7.52 |
7.78 |
t = –0.97 | 0.334 |
| ACD Post (mm) | 4.34 |
3.94 |
t = 2.50 | 0.013 |
| ACI Pre | 2.12 |
2.11 |
t = 0.26 | 0.795 |
| ACI Post | 1.17 |
1.09 |
t = 2.86 | 0.005 |
| Implant shift (mm) [Median (Q1, Q3)] | 1.17 (0.59, 1.59) | 0.49 (0.30, 0.67) | Z = –5.53 |
t, independent samples t-test; Z, Mann–Whitney U test; Q1, 1st Quartile;
Q3, 3st Quartile; CCD, coracoclavicular distance; ACD, acromioclavicular
distance; ACI, acromioclavicular index. ACI (Pre) and ACI (Post) were calculated
as CCDaffected/CCDunaffected before and after surgery, respectively.
*** p
Preoperative ASES, Constant–Murley, UCLA, or VAS scores did not differ between
the two groups (all p
| Variable | Hook plate group (n = 85) | TightRope group (n = 93) | Statistic | p-value |
| ASES Pre | 32.92 |
31.23 |
t = 1.53 | 0.128 |
| ASES Post | 84.20 |
89.27 |
t = –4.71 | |
| Constant–Murley Pre | 42.69 |
41.06 |
t = 1.29 | 0.199 |
| Constant–Murley Post | 83.70 |
87.98 |
t = –4.25 | |
| UCLA Pre | 16.89 |
16.92 |
t = –0.04 | 0.966 |
| UCLA Post | 28.66 |
31.46 |
t = –6.18 | |
| VAS Pre | 5.58 |
5.87 |
t = –1.56 | 0.121 |
| VAS Post | 2.03 |
1.35 |
t = 4.17 |
*** p
To identify key predictors of postoperative recovery, we constructed two
multivariable linear regression models with 6 months of CCD and Constant–Murley
score as dependent variables (Fig. 2A,B). Model performance was evaluated through
residual diagnostics (Fig. 2C,D). Before model construction, multicollinearity
among candidate predictors was assessed. Variables with VIF
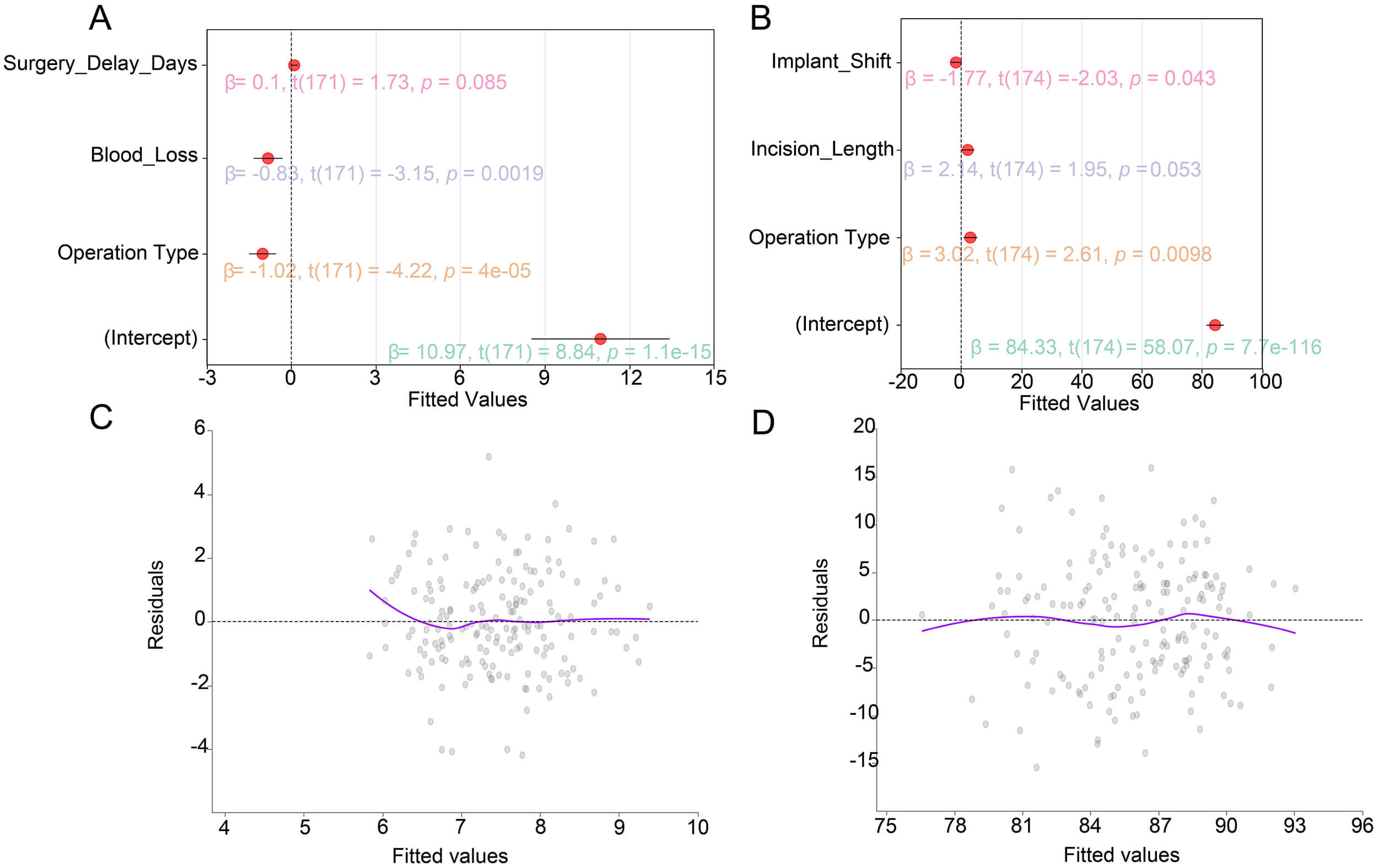 Fig. 2.
Fig. 2.
Multivariable linear regression models for key postoperative
outcomes. (A) Regression coefficients for postoperative coracoclavicular
distance (CCD).
In the CCD model, minimally invasive TightRope fixation was significantly
associated with better vertical stability. Specifically, TightRope fixation
reduced CCD by an additional 1.02 mm compared to hook plate fixation (
In the Constant–Murley score model, operation type remained the strongest
predictor. TightRope fixation was associated with a mean 3.02-point higher score
compared with hook plate fixation (
Before developing the model, baseline clinical characteristics were compared
between the training set (n = 124) and the validation set (n = 54). No
significant differences were observed between the two groups (all p
| Variable | Training set (n = 124) | Validation set (n = 54) | Statistic | p-value | |
| Age (years), mean |
38.54 |
37.73 |
t = –0.54 | 0.588 | |
| BMI (kg/m2), mean |
24.96 |
25.07 |
t = 0.23 | 0.822 | |
| Surgery delay (days), mean |
5.33 |
5.46 |
t = 0.37 | 0.712 | |
| Operation time (min), mean |
55.57 |
54.40 |
t = –1.47 | 0.144 | |
| Incision length (cm), mean |
5.84 |
6.21 |
t = 1.01 | 0.313 | |
| Blood loss (mL), mean |
59.41 |
53.45 |
t = –1.36 | 0.174 | |
| CCD Pre (mm), mean |
15.58 |
15.54 |
t = –0.09 | 0.927 | |
| ACD Pre (mm), mean |
7.53 |
7.94 |
t = 1.64 | 0.103 | |
| ACI Post, mean |
1.13 |
1.12 |
t = –0.36 | 0.719 | |
| Operation type, n (%) | 0.470 | ||||
| Hook plate | 57 (45.97) | 28 (51.85) | |||
| TightRope | 67 (54.03) | 26 (48.15) | |||
| Sex, n (%) | 0.596 | ||||
| Female | 37 (29.84) | 14 (25.93) | |||
| Male | 87 (70.16) | 40 (74.07) | |||
| Injury, n (%) | 0.229 | ||||
| Right | 58 (46.77) | 20 (37.04) | |||
| Left | 66 (53.23) | 34 (62.96) | |||
To identify potential risk factors for postoperative complications, univariate and multivariate logistic regression analyses were conducted using the training set. In the univariate analysis, the TightRope operation type was associated with a significantly reduced risk of complication (odds ratio [OR] = 0.36, 95% CI: 0.17–0.79; p = 0.014). Factors associated with higher risk included longer incision length (OR = 1.65, 95% CI: 1.14 – 2.40; p = 0.009), greater intraoperative blood loss (OR = 1.02, 95% CI: 1.01–1.04; p = 0.007), larger immediate postoperative ACD (OR = 1.28, 95% CI: 1.03–1.60; p = 0.025), and elevated postoperative ACI (OR = 4.31, 95% CI: 1.27–14.62; p = 0.019). Shorter operative time was linked to a protective effect (OR = 0.89, 95% CI: 0.80–0.99; p = 0.026) (Table 7).
| Variable | SE | Z | p-value | OR (95% CI) | ||
| Operation type | ||||||
| Hook plate | 1.00 (Reference) | |||||
| TightRope | –1.01 | 0.41 | –2.46 | 0.014 | 0.36 (0.17–0.79) | |
| Sex | ||||||
| Female | 1.00 (Reference) | |||||
| Male | –0.42 | 0.46 | –0.91 | 0.364 | 0.66 (0.27–1.61) | |
| Injury | ||||||
| Right | 1.00 (Reference) | |||||
| Left | 0.06 | 0.44 | 0.14 | 0.888 | 1.06 (0.45–2.51) | |
| Age (years) | –0.01 | 0.02 | –0.47 | 0.638 | 0.99 (0.94–1.04) | |
| BMI (kg/m2) | –0.05 | 0.07 | –0.67 | 0.505 | 0.95 (0.82–1.10) | |
| Surgery delay (days) | –0.09 | 0.10 | –0.89 | 0.374 | 0.91 (0.75–1.10) | |
| Operation time (min) | –0.11 | 0.05 | –2.23 | 0.026 | 0.89 (0.80–0.99) | |
| Incision length (cm) | 0.50 | 0.19 | 2.63 | 0.009 | 1.65 (1.14–2.40) | |
| Blood loss (per 50 mL) | 0.02 | 0.01 | 2.69 | 0.007 | 1.02 (1.01–1.04) | |
| Immediate postoperative CCD (mm) | 0.14 | 0.08 | 1.81 | 0.069 | 1.15 (0.99–1.33) | |
| Immediate postoperative ACD (mm) | 0.25 | 0.11 | 2.25 | 0.025 | 1.28 (1.03–1.60) | |
| Immediate postoperative ACI | 1.46 | 0.62 | 2.35 | 0.019 | 4.31 (1.27–14.62) | |
Variables with p
TightRope fixation remained an independent protective factor against
postoperative complications (OR = 0.42, 95% CI: 0.19–0.91; p = 0.028).
Conversely, greater intraoperative blood loss (OR = 1.86, 95% CI: 1.12–3.09;
p = 0.017) and larger immediate postoperative acromioclavicular distance
(ACD) (OR = 1.34, 95% CI: 1.01–1.80; p = 0.042) were identified as
independent risk factors. Incision length, operation time, and immediate
postoperative acromioclavicular index (ACI) were not statistically significant
(p
Overall, these findings indicate that the choice of Operation type, the extent of surgical invasiveness, and immediate postoperative radiographic alignment were the key determinants of postoperative complications (Table 8).
| Variable | SE | Z | p-value | OR (95% CI) | VIF | ||
| Operation type | |||||||
| Hook plate | 1.00 (Reference) | ||||||
| TightRope | –0.87 | 0.39 | –2.2 | 0.028 | 0.42 (0.19–0.91) | 1.88 | |
| Incision length (cm) | 0.17 | 0.17 | 0.99 | 0.322 | 1.19 (0.84–1.68) | 1.95 | |
| Operation time (min) | –0.08 | 0.05 | –1.65 | 0.099 | 0.92 (0.83–1.02) | 1.76 | |
| Blood loss (per 50 mL) | 0.62 | 0.26 | 2.40 | 0.017 | 1.86 (1.12–3.09) | 1.81 | |
| Immediate postoperative ACD (per mm) | 0.29 | 0.14 | 2.03 | 0.042 | 1.34 (1.01–1.80) | 2.31 | |
| Immediate postoperative ACI | 1.12 | 0.65 | 1.74 | 0.081 | 3.05 (0.86–10.78) | 4.18 | |
VIF, variance inflation factor.
After developing the model in the training set, its discriminative performance and generalizability were assessed and subsequently validated in the independent validation set. In the training dataset, the model demonstrated excellent discriminatory capacity with an area under the curve (AUC) of 0.84 (95% CI: 0.76–0.92). Performance remained robust in the validation set, with an AUC of 0.76 (95% CI: 0.64–0.89), indicating good external consistency. Overlaid ROC curves from both sets showed stable classification performance across datasets (Fig. 3A–C).
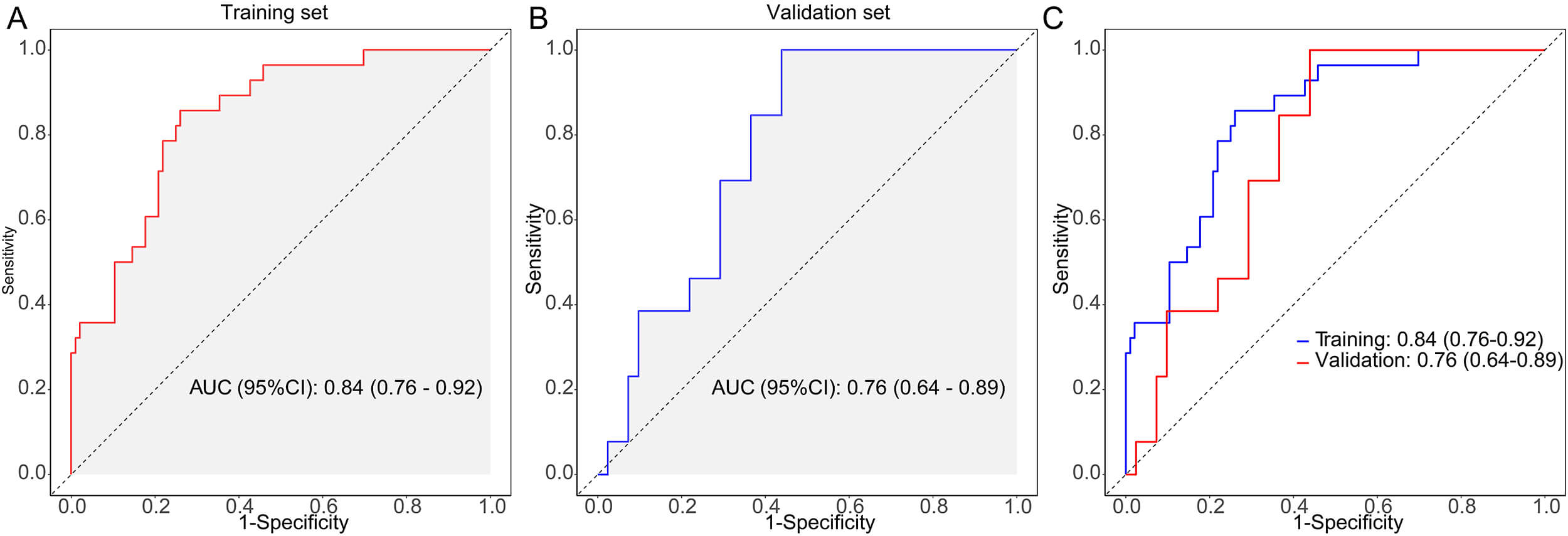 Fig. 3.
Fig. 3.
Receiver operating characteristic (ROC) curve analysis of the complication prediction model. (A) Training set (area under the curve [AUC] = 0.84, 95% confidence interval [CI]: 0.76–0.92). (B) Validation set (AUC = 0.76, 95% CI: 0.64–0.89). (C) Overlaid ROC showing consistent performance across sets.
Calibration analysis confirmed the model’s goodness-of-fit, with a non-significant Hosmer–Lemeshow test in both the training (p = 0.177) and validation (p = 0.477) sets, indicating close agreement between predicted and observed risks (Fig. 4A,B). Decision curve analysis (DCA) demonstrated clinical utility within specific threshold ranges. In the training set, the model provided a positive net clinical benefit for predicted risk thresholds of approximately 0.05–0.45, and in the validation set for thresholds of about 0.05–0.40 (Fig. 4C,D).
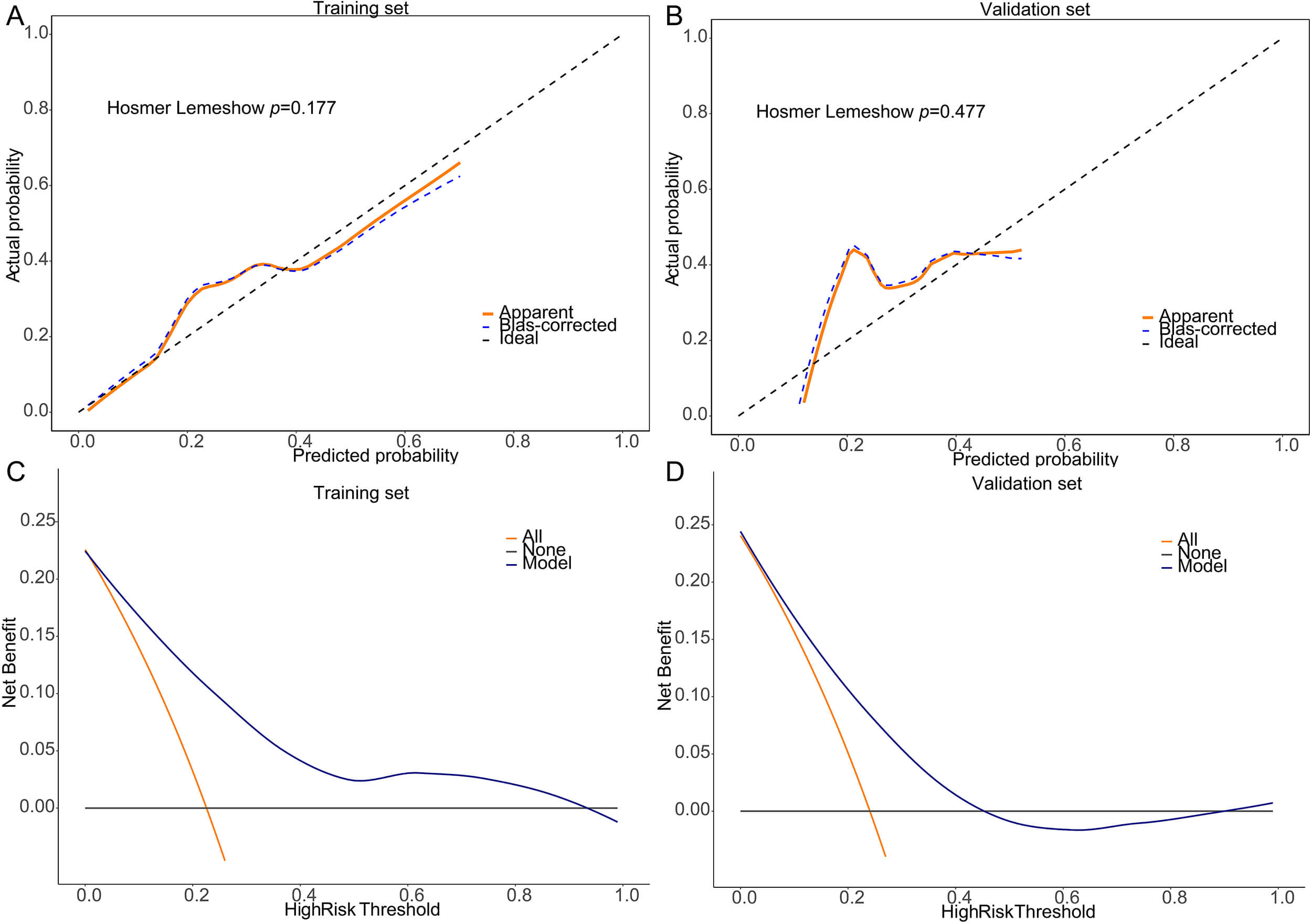 Fig. 4.
Fig. 4.
Model calibration and decision curve analysis (DCA). (A) Calibration plot for the training set (Hosmer–Lemeshow, p = 0.177). (B) Calibration plot for the validation set (p = 0.477). (C) DCA curve for training set showing net clinical benefit across thresholds. (D) DCA curve for validation set confirming practical utility.
Using a cutoff probability of 0.199, the confusion matrix revealed strong classification metrics. In the training set, the model achieved an accuracy of 77%, a sensitivity of 74%, a specificity of 86%, a positive predictive value (PPV) of 95%, and a negative predictive value (NPV) of 49%. In the validation set, accuracy was 67%, sensitivity 66%, specificity 69%, PPV 87%, and NPV 39% (Table 9).
| Data | AUC (95% CI) | Accuracy (95% CI) | Sensitivity (95% CI) | Specificity (95% CI) | PPV (95% CI) | NPV (95% CI) | Cutoff |
| Train | 0.84 (0.76–0.92) | 0.77 (0.68–0.84) | 0.74 (0.65–0.83) | 0.86 (0.73–0.99) | 0.95 (0.90–1.00) | 0.49 (0.35–0.63) | 0.199 |
| Validation | 0.76 (0.64–0.89) | 0.67 (0.53–0.79) | 0.66 (0.51–0.80) | 0.69 (0.44–0.94) | 0.87 (0.75–0.99) | 0.39 (0.19–0.59) | 0.199 |
PPV, positive predictive value; NPV, negative predictive value.
This study compared minimally invasive fixation techniques for ACJ dislocation: TightRope suspension and clavicular hook plate. At 6 months postoperatively, TightRope showed better radiographic outcomes—improved CCD, ACD, ACI, and implant stability—suggesting superior biomechanical performance. Patients in the TightRope group also had higher functional scores (ASES, Constant–Murley, and UCLA), along with lower VAS pain. The overall incidence of complications was lower with TightRope than with the hook plate. Multivariate analysis identified fixation methods, intraoperative trauma, and implant displacement as independent predictors of recovery and stability, while fixation type, postoperative ACD, and intraoperative blood loss independently predicted complications. A risk predictive model incorporating these factors performed well in both the training (AUC = 0.84) and validation (AUC = 0.76) sets, with good calibration and clinical utility.
Clavicular hook plates offer rigid fixation by anchoring beneath the acromion and acting as a mechanical lever to maintain joint reduction [21]. Although effective at restoring vertical alignment, the hook inevitably exerts pressure on the subacromial space, which may lead to persistent impingement of surrounding soft tissues. Prolonged implant retention increases the risk of complications such as subacromial impingement and humeral head osteolysis [22, 23]. Therefore, early removal of the hook plate is often recommended after fracture or dislocation healing to minimize these risks [24].
In contrast, the TightRope system establishes a dynamic, suture-based suspension between the coracoid and clavicle, mimicking the function of the native coracoclavicular ligaments while preserving joint mobility [25, 26]. Because it avoids rigid metal intrusion into the joint space, it better maintains physiological kinematics and reduces the likelihood of mechanical irritation of the acromion. This dynamic fixation system also allows controlled micromotion, which may favor a more natural stress distribution during shoulder movement.
In the current study, the TightRope group achieved smaller CCD, ACD, and implant migration, reflecting comparable—if not superior—joint alignment relative to hook plate fixation. Previous biomechanical and clinical studies also support the ability of the TightRope construct to restore coracoclavicular stability [27]. While potentially offering less rigid fixation than metal plates, the TightRope system’s soft tissue–preserving design and dynamic-loading properties may yield superior functional stability.
Our findings align with previous evidence indicating better pain control and functional recovery with the TightRope approach. Wang et al. [28] observed significantly lower VAS scores and higher Constant–Murley scores in the TightRope group compared to the hook plate group at both 6 and 12 months postoperatively. A meta-analysis by Pan et al. [29] involving 179 patients with Rockwood type III–IV dislocations also reported substantially lower postoperative VAS scores in the TightRope group, although Constant–Murley or UCLA scores were comparable between the two groups. Likewise, a randomized controlled trial by Cai et al. [30] reported smaller incisions, reduced intraoperative blood loss, and significantly lower VAS scores at postoperative day 1, 3 months, and 12 months with TightRope; Constant–Murley scores or coracoclavicular distances at 12 months did not differ.
Multivariable regression revealed intraoperative blood loss as an independent predictor of postoperative complications (OR = 1.86, p = 0.017), indicating that greater blood loss increases the risk of adverse outcomes, likely reflecting the extent of surgical trauma and soft tissue injury, which can impede recovery. In contrast, although longer incision length was associated with higher complication risk in univariate analysis (p = 0.009), it was not statistically significant after adjustment (p = 0.322). This suggests that once intraoperative blood loss and implant stability are considered, the independent effect of incision length on complications is limited.
Considering the minimally invasive nature of TightRope fixation—smaller incisions, reduced tissue trauma, and minimal subacromial irritation—our findings highlight the importance of operation type and blood loss control in optimizing postoperative recovery. TightRope preserves soft tissue integrity and avoids direct mechanical stimulation of the acromion. In contrast, hook plate fixation often requires secondary removal due to chronic foreign-body irritation, and it can limit shoulder motion postoperatively, potentially delaying functional recovery [31]. Overall, TightRope fixation provides stable joint reduction while preserving joint mechanics, which supports superior functional outcomes.
In this study, overall complication rates were lower with TightRope than with hook plate fixation. The incidence of infection was relatively low in both groups. Other complications tended to occur less often after TightRope, although several differences were not statistically significant. Wang et al. [28] reported three cases of subacromial impingement, two cases of post-traumatic arthritis, and two wound infections in the hook plate cohort, versus one reduction failure in the TightRope group. Lin et al. [32] demonstrated that hook plate fixation can induce rotator cuff injury and subacromial impingement, leading to decreased functional scores. Our statistical analyses similarly confirmed the influence of operation type on complication risk: hook plate fixation is associated with implant tip irritation and a higher likelihood of secondary procedures, and suboptimal reduction or implant displacement increases the risk of recurrent dislocation, though re-dislocation rates did not differ significantly in our cohort.
Multivariate logistic regression identified operation type, immediate postoperative ACD, and intraoperative blood loss as independent predictors of complications. These results underscore the need for an optimal reduction and a carefully selected fixation method to minimize postoperative risk. A meta-analysis by Pan et al. [29] found no statistically significant difference in overall complication rates between the two techniques; that conclusion may be limited by heterogeneity in study design and definitions of complications. Overall, TightRope has advantages in terms of reduced surgical trauma and improved functional recovery. The trend of lower frequency of certain complications is consistent with the theoretical mechanism of avoiding mechanical damage to bones and soft tissues at the acromial hook.
Additionally, we developed and validated a complication risk prediction model
incorporating surgical method, immediate postoperative ACD, and intraoperative
blood loss. The model demonstrated robust discriminative power (AUC = 0.76–0.84)
and favorable calibration (Hosmer-Lemeshow, p
Overall, these results suggest that TightRope fixation provides robust stability and potential for functional recovery in Rockwood III acromioclavicular joint dislocations, with lower complication rates. Given its minimally invasive profile, biomechanical advantages, and favorable patient recovery, TightRope represents a reasonable option for selected patients. However, further high-quality randomized controlled trials (RCTs) are needed to confirm their efficacy in reducing re-dislocation and overall complication rates. Treatment should remain individualized based on patient age, bone quality, economic considerations, and activity level. Postoperative management should emphasize monitoring for implant displacement and early functional rehabilitation to maximize outcomes and minimize long-term disability.
Despite compelling findings, we acknowledge several limitations. This is a single-center, retrospective cohort design with non-randomized treatment allocation, which introduces potential selection bias. Although we adjusted for known confounders such as operation type, intraoperative blood loss, and ACD, unmeasured variables (e.g., surgeon experience, soft tissue quality, and adherence to rehabilitation) may have affected outcomes. Additionally, the sample size is relatively modest and obtained from a single institution, limiting the external validity and generalizability of our findings.
To validate these findings regarding outcomes and complication risk, larger multicenter prospective randomized controlled trials (RCTs) are warranted. Long-term follow-up is also needed to assess implant durability, sustained functional recovery, and late complications. Another promising direction involves cost-effectiveness analyses to quantify the economic benefits of minimally invasive techniques such as TightRope, particularly the potential reduction in complication rates, rehabilitation duration, and overall healthcare utilization. Furthermore, future investigations should also explore the role of TightRope in higher-grade dislocations (e.g., Rockwood type V–VI), especially after high-energy trauma or when additional ligamentous injuries occur. Finally, combining TightRope with dual-suspension constructs or augmentation materials to enhance fixation strength and clinical outcomes also warrants further investigation.
This study supports the minimally invasive TightRope suspension as a biomechanically favorable, tissue-preserving alternative for managing Rockwood type III ACJ dislocations. It appears particularly suitable for patients with high functional demands or those seeking to minimize the risk of reoperation. The improvements demonstrated in stability and functional recovery highlight the clinical potential of soft-fixation strategies in managing ACJ injury. The complication risk prediction model provides a quantitative tool for individualized preoperative risk assessment and facilitates more informed surgical planning. With future validation through multicenter cohorts and cost-effectiveness analyses, the TightRope system could be adopted as a standardized, cost-effective treatment strategy that guides clinical protocols and insurance reimbursement frameworks.
• TightRope fixation demonstrated minimally invasive advantages, including shorter incision length, reduced intraoperative blood loss, and lower complication rates compared with hook plate fixation.
• Radiographic outcomes in 6 months showed superior ACJ stability in the TightRope group, with significantly improved CCD, ACD, and ACI values.
• Functional recovery was better in the TightRope cohort, evidenced by higher ASES, Constant–Murley, and UCLA scores, alongside lower VAS pain levels.
• Multivariable linear regression identified operation type, intraoperative blood loss, and implant displacement as key predictors of radiographic and functional outcomes.
• Logistic regression analysis identified TightRope fixation as an independent protective factor against complications, while greater blood loss and larger ACD were independent risk factors.
• The complication prediction model demonstrated strong discrimination, calibration, and clinical utility, with consistent performance in both the training and validation sets.
The data analyzed during the current study are available from the corresponding author upon reasonable request.
YJY contributed to conceptualization, methodology, formal analysis, writing–original draft, and visualization. RX was involved in data curation and investigation. SLH contributed to data curation, software, and validation. YHL participated in data curation and investigation. TJM was responsible for data curation, resources, and validation. HRCZ contributed to investigation and visualization. HZ was involved in investigation and resources. ZJJ contributed to investigation and validation. HXS contributed to resources and validation. FY contributed to conceptualization, project administration, and supervision. All authors contributed to revising the manuscript critically for important intellectual content. All authors approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
The study was approved by the Ethics Committee of Tongliao People’s Hospital (approval number: TLPH-EC-2025-69). As the analysis used existing medical records of the patients and presented no risk, the institutional ethics committee granted a waiver of informed consent. This study was conducted in accordance with the principles outlined in the Declaration of Helsinki.
Not applicable.
This research received no external funding.
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.