

 , Chamanjeet Jassal 1, Robert Galloway 2,3,*
, Chamanjeet Jassal 1, Robert Galloway 2,3,*
1 Department of Paediatrics, University Hospitals Sussex NHS Foundation Trust, BN11 2DH Worthing, UK
2 Department of Emergency Medicine, Royal Sussex County Hospital, University Hospitals Sussex NHS Foundation Trust, BN2 5BE Brighton, UK
3 Brighton and Sussex Medical School, University of Sussex, BN1 9PX Brighton, UK
Abstract
Timely escalation of care is critical in preventing adverse patient outcomes, yet barriers such as poor communication, role ambiguity, and hierarchical challenges persist. This article explores key human factors influencing escalation, including structured communication tools, psychological safety, and simulation-based training, emphasizing their role in reducing hesitation and improving decision-making. Organizational factors such as workload, leadership, and early warning systems (EWSs) are examined for their impact on facilitating or impeding escalation efforts. The findings highlight the effectiveness of simulation-based training in reinforcing escalation skills, particularly in high-stakes environments, as well as the growing role of Patient and Family Activated Escalation Systems (PFAESs) in improving the early recognition of deterioration. Strategies to enhance escalation reliability include fostering interdisciplinary collaboration, integrating structured escalation training, and optimizing patient-involvement mechanisms to strengthen safety culture. By embedding these approaches into clinical practice, healthcare systems can create a more responsive, proactive, and safer escalation framework.
Keywords
- simulation training
- escalation of care
- hierarchical barriers
- patient and family activated escalation systems
- civility culture
- human factors
- healthcare
Patient deterioration in the hospital setting poses an ongoing and inevitable challenge to healthcare systems and the clinicians responsible for escalating care. Human factors are an expanding area of clinical research, with increasing recognition of how they influence clinical care and patient outcomes. Failure to escalate care promptly is linked to higher in-hospital mortality and unplanned intensive care unit (ICU) admissions [1, 2]. A systematic review identified failure to rescue as a key factor in poor surgical outcomes [3], while evidence suggests early warning systems (EWSs) alone are insufficient to prevent escalation delays [4].
This article explores the role of human factors in deterioration in the hospital setting, with focus on examining the success factors which facilitate escalation. We identify several key themes: interprofessional collaboration (role clarity, teamwork and communication), psychological safety (dismantling hierarchies and promoting civility culture), the role of the patient and family as advocates for care, education (simulation and human factors training), and the organizational factors and systems (e.g., early warning/rapid response systems [RRSs]) used by clinicians. By addressing both organizational/systematic and behavioural contributors to escalation delays, we offer strategies and recommendations to enhance the reliability of escalation in the deteriorating patient.
Effective collaboration for escalating deteriorating patients hinges on good communication, role clarity, teamwork, flat hierarchies and civility culture in healthcare. Good communication is fundamental to the effective escalation of deteriorating patients. A systematic review by Johnston et al. [3] emphasized that communication breakdowns—particularly when escalating to a senior colleague—are among the primary factors contributing to delays in recognizing and responding to patient deterioration in surgical contexts. Specifically, the fear of hierarchy, intimidation or criticism posed barriers to initiating necessary communication to escalate. Delays in availability of senior input, frequent interruptions and poor communication quality were also cited as barriers to timely, effective escalation.
Similarly, a qualitative review by Ede et al. [5] identified how miscommunication, poorly packaged handovers, and providing ambiguous or incomplete information may undermine credibility of the communications made to escalate care. For example, a nurse stating that a patient is “a bit unwell” without specifying vital sign abnormalities or deterioration markers can lead to requests for them to find out more information before calling back again. Similarly, without substantial evidence of urgency there may be inadequate prioritization of escalation by the receiving clinician. As such, these may lead to delays in necessary clinical reviews and interventions.
The use structured handover tools and targeted communication training are crucial to mitigating these issues. The SBAR (Situation, Background, Assessment, Recommendation) tool is widely used to standardize handovers and reduce ambiguity [6, 7]. When implemented effectively, SBAR helps structure information flow, ensuring that the receiving clinician understands both the clinical picture and the required next steps. However, their effectiveness hinges on consistent application and staff confidence in using them. SBAR improves handoff communication and reduces adverse events when properly implemented, yet its impact can be limited if not fully integrated into clinical workflows [7]. To mitigate these issues, structured training programs incorporating SBAR-focused simulations have been shown to improve confidence in using escalation frameworks effectively [6].
Role clarity and care accountability are equally as important, as ambiguity in patient ownership can impede escalation. A qualitative review by Ede et al. [5] concluded that poor understanding of role definitions can undermine team-work. For example, lack of clarity in the care team member were responsible for/able to provide, leads to uncertainty about whom patients should be escalated to. Similarly, Chua et al. [8] found that role ambiguity between enrolled and registered nurses contributed to delays in escalation, as enrolled nurses often expected registered nurses to act on clinical deterioration, while registered nurses assumed that concerns would be escalated if necessary. This lack of collaboration and shared responsibility sometimes led to gaps in timely intervention. Patient ownership issues may also arise with outlier patients—those cared for outside their team’s ward—who are at risk of fragmented care due to unclear accountability within and between different teams; with both junior doctors and nurses express reluctance to act decisively for these patients, citing unfamiliarity and accountability concerns [9].
We propose several strategies to overcome these systemic challenges at the interprofessional level. Firstly, we argue that clear governance in terms of policies and protocols is paramount. Examples include structured escalation pathways to aid in the formalization of ownership and to ensure timely interventions, which may be especially pertinent for the protection of outlier patients. Another example would be implementing formal guidelines emphasizing shared decision—making between enrolled and registered nurses to address gaps in role clarity and foster collaboration [8]. Awareness surrounding new clinical governance should be optimised through targeted information sharing and education—establishing explicit role definitions through interdisciplinary training, including simulation, and regular team briefings, e.g., “huddles” can ensure responsibilities are well understood [5, 9, 10]. Junior staff must be empowered by their seniors to act as full members of their own team, and to take responsibility for escalating concerns as soon as they identify them—empowering staff to act beyond immediate roles when necessary is crucial. For example, nurses may hesitate to call rapid response teams (RRTs) due to fear of criticism or breaking hierarchical norms, delaying critical interventions [9]. Reducing these fears and supporting clinicians to act decisively, arguably hinges on active dismantling of medical hierarchies, and fostering clinical environments that promote inclusivity and psychological safety—where healthcare professionals (HCPs) at all levels feel confident speaking up without fear of blame or retaliation.
Steep hierarchical structures in healthcare can present significant barriers to teamwork and communication, particularly in escalation scenarios. Junior staff may hesitate to escalate concerns due to fear of negative reactions from senior colleagues, uncertainty about whether their concerns are valid, or previous experiences of having their input disregarded. These hierarchies can transcend the interprofessional sphere too. For example, outdated or traditional structures may view nurses as subordinate to doctors, which may present a host of patient safety threats in themselves. This is exemplified by the famous Elaine Bromiley case, where a preventable patient death occurred because nurses were hesitant to challenge the airway management decisions of two senior anaesthetists despite recognizing the need to escalate with a surgical airway [10]. This tragic example demonstrates the dangers of systems which fail to protect the voices of clinicians who may perceive themselves to be of a “lower status” and therefore lack confidence in challenging decisions made by colleagues in a greater position of power. Bould et al. [11] explored this phenomenon in a qualitative study involving anaesthesiology residents, revealing that fear and intimidation were prominent factors influencing their reluctance to challenge consultants’ unethical imperatives (to give blood to a Jehovah’s witness), during simulated scenarios.
Efforts to flatten the hierarchical structures illustrated above, which threaten patient care and effective escalation, may be supported by tools and techniques for clinicians to be harnessed with. Green et al. [10] propose various strategies from their own experience, including “Probe, Alert, Challenge, Emergency (PACE)” and the “Two challenge rule”. Table 1 provides a breakdown of the “PACE” tool, which can be used in a graded approach to challenge a colleague felt to be threatening patient safety. Similarly, the “Two Challenge rule”, adapted from the aviation industry, posits that if a concern is not acknowledged after the first challenge, a second, more assertive challenge is made. This facilitates a “collaborative inquiry” approach, in which open discussion of decisions and reasoning is encouraged, allowing for questioning, learning, and team-based improvements.
| PACE step | Description | Clinical example |
| Probe | Gently ask a question or seek clarification to probe the situation. This is a non-confrontational way to bring attention to a potential issue. |
A nurse notices a patient’s blood pressure has dropped but is unsure if it’s significant. She asks the doctor: ‘Dr. Smith, I see the blood pressure is 88/50. Do you think we should reassess fluids?’ |
| Alert | Express a concern clearly and directly if the initial probe does not lead to action. Highlight specific patient changes or risks. |
The nurse sees the blood pressure has continued to drop and the patient is becoming drowsy. She alerts the doctor: ‘I’m concerned—his blood pressure is now 82/45, and he’s not as responsive. Should we intervene now?’ |
| Challenge | More assertively challenge the decision or lack of response if concerns persist. Reinforce the urgency of the situation. |
The doctor is still hesitant to act. The nurse challenges: ‘I strongly believe this patient is deteriorating. We need to reassess him immediately and consider more aggressive fluid resuscitation.’ |
| Emergency | Take immediate action if the situation is critical and previous steps have not led to an appropriate response. Escalate to the highest necessary authority. |
The patient’s blood pressure drops further, and the doctor remains unresponsive. The nurse calls the senior consultant directly: ‘This patient is in shock, and we need urgent intervention. I’m escalating this now.’ |
This offers a breakdown of how challenging clinicians may utilise the ‘Probe, Alert, Challenge, Emergency (PACE)’ tool in clinical practice, when recognizing a colleague’s action/inaction may be threatening appropriate escalation or patient safety.
But what is the point in these tools if people remain hesitant to use them? HCPs of influence within clinical environments, from senior doctors to charge nurses, must take responsibility as clinical leaders to create an environment of psychological safety proactively, in turn empowering our multiprofessional workforce to act confidently when needed. This may take the form of regular team briefings in which reminders about the freedom to speak up are reiterated. Senior clinicians should acknowledge their own infallibility and actively encourage junior staff to participate in discussions, to create an atmosphere where escalation is viewed as a fundamental component of patient safety, rather than a challenge to authority. Structured debriefing sessions following escalation events may also add value by reinforcing positive communication behaviours and normalize speaking up as an essential part of clinical practice. For example, Longstreth et al. [12] found that real-time feedback and post-escalation reviews with RRTs not only validated junior staff concerns but also improved overall confidence in raising issues.
Considerable variability in responses to early warning scores, coupled with the absence of clear escalation criteria and protocols, may contribute to delays [13]. Addressing these inconsistencies through targeted quality improvement initiatives may facilitate earlier intervention and improve timely escalation. For instance, Babroudi et al. [14] successfully implemented an escalation of care protocol for internal medicine trainees. This protocol incorporated guidelines, communication, and decision-making tools, alongside targeted education sessions. The results included enhanced trainee confidence, breakdown of perceived hierarchical barriers, and fewer adverse patient events. However, despite the existence of structured escalation pathways in some hospital settings, junior staff may still default to traditional hierarchical patterns. Walker et al. [9] found that even in environments where protocols explicitly encourage direct escalation (e.g., RRT escalation), junior doctors and nurses tend to defer to familiar authority figures, such as more senior clinicians within their home ward. This reluctance may be further compounded by previous negative experiences in which escalation attempts were dismissed or criticized, such as instances where the primary ward physician felt it was “their patient and their job to look after them” and that the junior staff had “gone over their head”, potentially reinforcing juniors’ hesitation to act in future cases [13].
Hospital-wide initiatives such as the “Civility Saves Lives” campaign have emphasized the role of mutual respect in improving communication, demonstrating that a culture of civility directly contributes to better patient outcomes. Incivility exacerbates communication challenges and teamwork in healthcare. Katz et al. [15] found that exposure to incivility significantly impaired diagnostic accuracy, vigilance, and teamwork during high-pressure surgical scenarios. Similarly, Riskin et al. [16] highlighted that rudeness impaired team performance in the neonatal intensive care setting by disrupting critical collaborative processes such as information sharing and help-seeking. A follow-up study suggested that interventions such as cognitive bias modification (CBM) can help individuals reinterpret negative interactions and maintain performance under stress [17]. The “Civility Saves Lives” campaign emerged in 2017 in response to growing evidence linking incivility in healthcare to diminished team performance and adverse patient outcomes. The campaign underscores the principle that respectful and civil interactions are not just ethical imperatives but critical components of patient safety. It demonstrates how fostering kindness and mutual respect can improve teamwork, reduce stress, and enhance the overall culture of healthcare [18].
Simulation-based education (SBE) plays a pivotal role in addressing human factors critical to the successful escalation of care. It provides a controlled environment where HCPs can practice clinical scenarios without risking patient safety. There is a growing body of evidence supporting SBE to improve practice and working relationships for doctors and nurses [6, 17, 19, 20, 21, 22]. Simulation is invaluable for early-career doctors due to its ability to enhance confidence and preparedness in managing acutely ill patients. Through repetitive practice and targeted feedback, participants experience measurable improvements in knowledge retention and application, addressing common challenges such as hesitation and fear of escalation [19].
In the context of UK Core Medical Training, SBE enhances both technical and non-technical skills. The Joint Royal Colleges of Physicians Training Board [20] recommends simulation for critical procedures and emergency scenarios. In addition to enhancing technical competence, evidence suggests that human factor skills can be effectively taught in this setting. Within SBE, doctors can practice task prioritization, coping with distractions, and avoiding cognitive biases such as fixation error, while developing situational awareness, leadership, and teamwork skills for managing deteriorating patients [20]. SBE’s value transcends professions and experience levels. Stayt et al. [22] found that high-fidelity (HF) simulations significantly improve undergraduate nurses’ ability to recognize and escalate deteriorating patients. Similarly, O’Rourke et al. [21] emphasized the value of interprofessional simulation in nursing practice, noting that such scenarios strengthen communication, team dynamics, and collective decision-making. For medical and nursing students, the combination of SBE with targeted feedback interventions enhances both confidence and performance when using validated handover tools like SBAR [6]. SBE scenarios replicate real-life complexities, offering participants opportunities to navigate interpersonal challenges such as communication breakdowns and hierarchical tensions in a safe environment. Integrating simulation-based training into routine healthcare education, with scenarios that replicate early warning triggers and collaborative interventions, provides a structured approach to overcoming human factors that impede escalation.
While the immediate benefits of simulation training are well-documented, long-term retention and sustainability remain areas in need of ongoing research. Zeng et al. [23] found that while HF simulation significantly improves knowledge and skill acquisition, retention declines after three months without additional training, suggesting the need for regular reinforcement sessions. Similarly, Park et al. [24] highlight that although recurrent simulation sessions significantly decreased the time to intervention in trauma procedures, its impact on long-term patient outcomes is unclear, warranting further investigation into how these benefits translate into real-world practice. The importance of distributed practice—where training is spaced out over time rather than delivered in a single session, may also implicate long-term skill retention [23]. To ensure sustainability, simulation training must be embedded into structured curricula, with regular refresher sessions and competency assessments to reinforce learning [20].
Sustainability of SBE may also hinge on the investment of substantial resources involved in the facilitation of sessions, especially with respect to HF simulation. Zeng et al. [23] emphasize that HF simulation, while beneficial, is costly and resource-intensive, making it less feasible in settings with limited access to advanced equipment. In contrast, low-fidelity simulations, which rely on basic manikins, peer-to-peer role-playing, and guided case discussions may still be valuable, especially where resources are limited. The evidence of impact of simulation in low resource countries is sparse. Seethamraju et al. [25] demonstrated evidence to support simulation faculty training workshops as an effective intervention to “train the trainers” in low resource settings. Their study highlights that alternative training models—such as low-fidelity simulation (LFS) and scenario-based discussions—can offer cost-effective solutions, while equipping faculty members with tools to enhance clinical skills and teamwork.
Moreover, SBE is an essential tool for improving escalation processes, team communication, and clinical decision-making. However, sustaining its benefits requires long-term reinforcement, structured refresher training, and integration into clinical practice. While HF simulation remains the gold standard in some settings, cost-effective alternatives, including low-fidelity simulation and digital training, offer viable solutions for resource-limited environments. By prioritizing long-term implementation strategies, institutions can ensure that SBE continues to enhance patient safety and care escalation well beyond the training environment.
As more light has been shed on the importance of human factors in ensuring patient safety, more training tools have been created within organizations including the healthcare system to increase the safety margin of healthcare practices. Crew resource management (CRM) has been adapted from aviation to improve system performance and reduce accidental harm within the workplace. Whilst it remains work in progress to refine a fixed criteria that CRM comprises of, it is loaded with tools to train and test the safety of human factors in a workplace [26]. Human factor skills are teachable and do not appear to be innate [27]. The most valuable process is increasing awareness of one’s skills and limitations. A study conducted in a tertiary maternity unit used the Hospital Survey of Patient Safety Culture to evaluate the impact of maternity-oriented human factors training on high-risk intrapartum outcomes. The findings showed that after introducing human factors training, participants felt more confident in challenging decisions or actions of those in authority. The proportion of respondents who answered “most of the time or always” increased from 33% to 42% within five months, while those responding “never” decreased by 50% [28]. There is a potential for more long-term research to assess how we retain and translate skills learnt via these tools into clinical practice [27]. In view of it’s absence, there is a need for a validated tool to assess the knowledge and learning of human factors skills within healthcare [29]. This could aid the evaluation and development of educational interventions, such as targeted training or simulation-based sessions for HCPs.
The organizational environment of healthcare significantly influences escalation capacity. Staffing levels, workload, ergonomics, and workplace culture interconnect to determine both the quality and timeliness of responses to patient deterioration. Adequate staffing is critical—each additional patient per nurse correlates with a 22% increase in inpatient mortality [1]. It is no surprise that missed care, particularly in patient surveillance, may lead delays in recognizing deterioration and subsequent adverse outcomes. The proposed premise is that high workloads lead to task prioritization and care driven by efficiency over quality, forcing clinicians to bypass less urgent but important activities like thorough patient assessments. Under excessive demand, clinicians may be more prone to cognitive overload, attentional tunnelling, and task-switching inefficiencies. As such, they may unconsciously prioritize immediate, high-stakes tasks while deferring or overlooking subtle but important patient deterioration cues. Furthermore, decision inertia—where staff may hesitate to escalate due to uncertainty or the need for additional confirmation—may be exacerbated when clinicians are under pressure. As such, these pressures perpetuate a reactive rather than a proactive approach within work-systems, compromising earlier detection of deterioration. Work-systems comprise of organization, tools and technology, the physical/cultural environment and the HCP using them at their core, with their ultimate goal to protect and serve our patients’ health needs. A systematic review by Xie and Carayon [30] outlines how proper application of human factors and ergonomics (HFE) principles can improve work systems and care processes, translating into better quality of care and better outcomes, e.g., decreased complication rates and mortality. Table 2 (Ref. [30]) provides examples of physical, cognitive, and organizational HFE-related challenges in clinical practice.
| Physical | |
| Cognitive | |
| Organizational | |
This demonstrates examples of human factors and ergonomics-based challenges that may directly or indirectly impede the escalation of care. Various examples drawn from Xie and Carayon [30].
Optimizing work-systems to align with patients’ and HCP’s needs is therefore necessary to reduce cognitive load, streamline task completion, and foster timely decision-making—all important components in escalating care. As such, we present here several evidence-based strategies for integrating the evolving healthcare-technological advancements within work-systems. Alhmoud et al. [31] demonstrate an example of user-centred-design in technology, with a clinician-friendly dashboard integrating real-time data. This quality improvement initiative enhanced clinicians’ ability to track and escalate deteriorating cases effectively—improving compliance with EWSs guidelines and reducing delays in intervention. Implementing artificial intelligence (AI) driven EWSs could also flag deteriorating patients before cognitive overload hinders recognition. Edelson et al. [32] concluded that a machine learning system, ‘eCARTv5’, outperformed other AI and non-AI scores, identifying more deteriorating patients with fewer false alarms and sufficient time to intervene. Additionally, the standardization of electronic health record (EHR) content, such as order sets and clinical documentation, has been shown to reduce unwanted variations in care and enhance clinical efficiency—A recent qualitative study emphasized that clinical standardization across facilities with EHRs, were perceived to have strong potential for improving efficiency and uniformity of care [33].
Organizational culture and good clinical leadership also underpin escalation efficacy. Organizations with cohesive and supportive cultures report better patient outcomes, including reduced mortality and adverse events [34]. Conversely, hierarchical and punitive cultures discourage staff from escalating concerns for fear of blame or dismissal. Collaborative leadership styles that promote inclusivity and shared governance have been shown to improve communication and trust among staff, enhancing their willingness to act [35]. For instance, empowering staff through education, feedback, and clinical supervision fosters confidence in recognizing and responding to early deterioration. Leaders who actively dismantle hierarchical barriers encourage a culture of openness, where escalation of care is not hindered by professional silos or fear of reprisal [35, 36]. In practice, implementing structured mentorship programs, where senior clinicians actively support and guide junior staff, could serve to reduce hierarchy-driven barriers and normalize escalation as a shared responsibility.
Effective clinical leadership transcends various human factors pertinent to the timely escalation of care. It plays a pivotal role in fostering psychological safety through inclusive attitudes and addressing dismissive behaviours. For example, creating space for debriefing sessions after critical incidents offers opportunities for reflection and positive reinforcement, addressing fears of criticism. Regular feedback mechanisms and cultural transformation initiatives further embed these practices into team dynamics [12]. In practice, this may take the form of regular interdisciplinary meetings to provide a structured forum (e.g., local faculty groups & clinical governance meetings) for junior and senior staff to engage in shared decision-making and feedback, ensuring transparency and reinforcing that all team members’ concerns are valued.
Hinging on clinical leadership—systemic approaches to addressing organizational challenges are essential. Strategies such as investment in ergonomic redesigns and cultivating a culture of continuous learning and improvement are vital to optimizing escalation processes [1, 30, 34]. Integrating HFE principles into organizational policies and protocols ensure that clinical environments support rather than hinder care delivery [35]. In practice, adoption of standardized escalation triggers/checklists (i.e., structured lists of clinical/behavioural indicators such as Glasgow Coma Scales (GCS) or EWSs thresholds/repeated concerns raised from staff that signal when escalation is necessary) and response protocols (i.e., predefined steps outlining who should be contacted, how quickly, and what actions should be taken when escalation is triggered) may further support equitable involvement, making it clear that escalation is a defined team process rather than an individual risk. As healthcare systems evolve, addressing these organizational factors will be critical to ensuring safer and more reliable responses to patient deterioration.
Healthcare tools such as EWS and RRS play a crucial role in identifying and managing patient deterioration promptly in non-intensive care settings. EWS tools, operate by aggregating vital signs into a single score that often triggers predefined escalation pathways [2, 37]. Evidence has highlighted that EWS tools standardize the recognition of deterioration and reduce variability associated with individual clinical judgment [4]. This allows HCPs to escalate concerns based on objective, quantifiable data, which can support the escalating clinician to communicate the degree of urgency and bridge the gap between bedside observations and rapid intervention [38].
The interplay of EWS with RRT activation is pivotal. EWS and RRS are internationally adopted systems to facilitate early identification of clinical deterioration with timely escalation on acute inpatient wards [37]. As such, early warning score thresholds are often within predefined RRT activation criteria, which, when actioned appropriately leads to the deployment of various critical care trained personnel to provide expert clinical assessment and intervention [2, 37]. The Society of Critical Care Medicine strongly recommend the provision of RRTs with clearly defined activation criteria, supported by good evidence that these systems can mitigate adverse outcomes such as death and non-ICU cardiac arrests. Further, they highlight the importance of integrating quality improvement processes within RRS [2]. Longstreth et al. [12] exemplified this best-practice statement, effectively implementing an initiative to reduce nurse hesitancy to call RRTs, through targeted education (e.g., the role, indications and communication strategies for calling) and integrated feedback mechanisms such as debriefs.
However, despite their advantages, the implementation of EWSs and RRTs are not without challenges. Barriers such as nurses’ over-reliance on numerical scores may undermine the value of clinical ‘intuition’ or clinical reasoning. Flenady et al. [39] highlight that mandated EWS may inhibit higher order thinking in the clinical judgement process—particularly amongst junior nurses—as such, leading to potential delays in escalation when clinical signs of deterioration are present but EWSs fall below predefined thresholds. Furthermore, inconsistent adherence to escalation protocols, and subjective interpretations of EWSs triggers may undermine their role in standardising escalation of care. For example, some teams may respond immediately to an elevated EWS, while others delay intervention due to miscommunication or differing interpretations of urgency [38]. This variability may lead to inconsistent outcomes, as delays in addressing early signs of deterioration may increase the likelihood of adverse events. However, to date there remains a paucity of high-certainty evidence reflecting quantifiable benefits of EWSs and RRSs—such as unplanned ICU admissions and length of hospital stay. This suggests that further research may be warranted to better support their implementation [2, 13, 37].
The active involvement of patients and families in escalating concerns about clinical deterioration is increasingly recognized as vital to patient safety. While clinicians traditionally detect warning signs, evidence shows patients and families provide unique, often critical, early insights [40, 41, 42]. They can initiate escalation by identifying and communicating concerns. The Society of Critical Care now endorses their role, with guidelines supporting patient- and family-activated rapid response [2]. Through intuitive self-awareness, patients often detect subtle changes before clinical metrics indicate deterioration, and families may recognize early signs like altered speech or energy levels [40, 42].
However, barriers such as low health literacy (e.g., patients with learning disabilities), socioeconomic and cultural factors, and language differences can hinder patients from identifying or articulating concerns. Stoicism, fear of being a burden, and uncertainty about symptom significance further discourage escalation, especially when resources seem overstretched [42, 43]. Communication breakdowns with clinicians contribute to adverse events, with patients often feeling unheard—a key trigger for seeking second opinions [41, 43, 44]. Power imbalances may deter people from speaking up, while dismissive attitudes erode trust and delay care [40, 42]. Thus, encouraging patient voice and fostering an approachable, responsive clinical culture is crucial. Clinicians widely recognize “safety netting” as a crucial tool, particularly upon discharge or in primary care. However, the risk of deterioration in hospitals highlights the need to apply these strategies early. Educating patients and families to recognize deterioration signs and navigate escalation pathways may enhance their confidence and engagement in care [40, 42]. Patient and Family Activated Escalation Systems (PFAESs) like Martha’s Rule and Ryan’s Rule offer direct escalation channels beyond the home ward, including RRTs, empowering families and breaking hierarchical barriers, while reinforcing their role as collaborative partners. These policies allow patients and families to escalate concerns and request an independent clinical review if they feel a patient’s condition is deteriorating and their worries are not being addressed. Inspired by the tragic and preventable deaths of Martha Mills and Ryan Saunders, these rules aim to improve patient safety by ensuring families have a clear, accessible pathway to urgent medical reassessment when needed [41, 45].
Despite Martha’s rule having been featured in mainstream media, this knowledge may not be readily available to all patients and families. Hospital-wide campaigns with visual signposting such as informative posters and leaflets may be beneficial for raising awareness of these pathways and may reduce the underlying fear of speaking up for those with less social capital by normalizing the concept. We emphasize that this information sharing as detailed above must be equitable. Therefore, vulnerable subgroups who may be less likely to voice concerns, or with little knowledge of PFAESs such as migrants with language or cultural barriers, should be approached with extra consideration and additional resources if required. An example would be to proactively offer interpreter services, with face-to-face communication reiterating their rights to accessing escalation pathways.
Despite their benefits, PFAESs face challenges if clinicians view them as complaint mechanisms rather than valid escalation tools, potentially delaying post-activation reviews. Perceived ‘inappropriate’ activations may also be considered to strain already limited resources, impeding implementation [41]. Strategies to reduce frequent activations include bedside nursing handovers, fostering transparency between clinicians, patients, and families, and intentional rounding to listen to and address concerns proactively [46]. A clear distinction is needed between PFAESs activations for clinical deterioration requiring urgent review and those reflecting broader care concerns. Achieving this relies on effective communication. A new escalation tool could support triage by helping clinicians—particularly nurses—integrate their clinical judgment with patient and family concerns.
We introduce the “Good CATCH” tool, illustrated by Fig. 1; a stepwise approach for any HCP facing a new clinical concern. Designed to include input from all stakeholders—nurses, doctors, care assistants, allied professionals, patients, and families—it seeks to help distinguish between urgent deterioration requiring immediate response and concerns needing less urgent attention. The tool guides clinicians in determining next steps, whether activating an RRT or arranging an independent review focused on clinical assessment or communication surrounding patient/family concerns. Named to acknowledge those who make a “good catch”, it is also designed to reinforce a culture of recognition and positive teamwork.
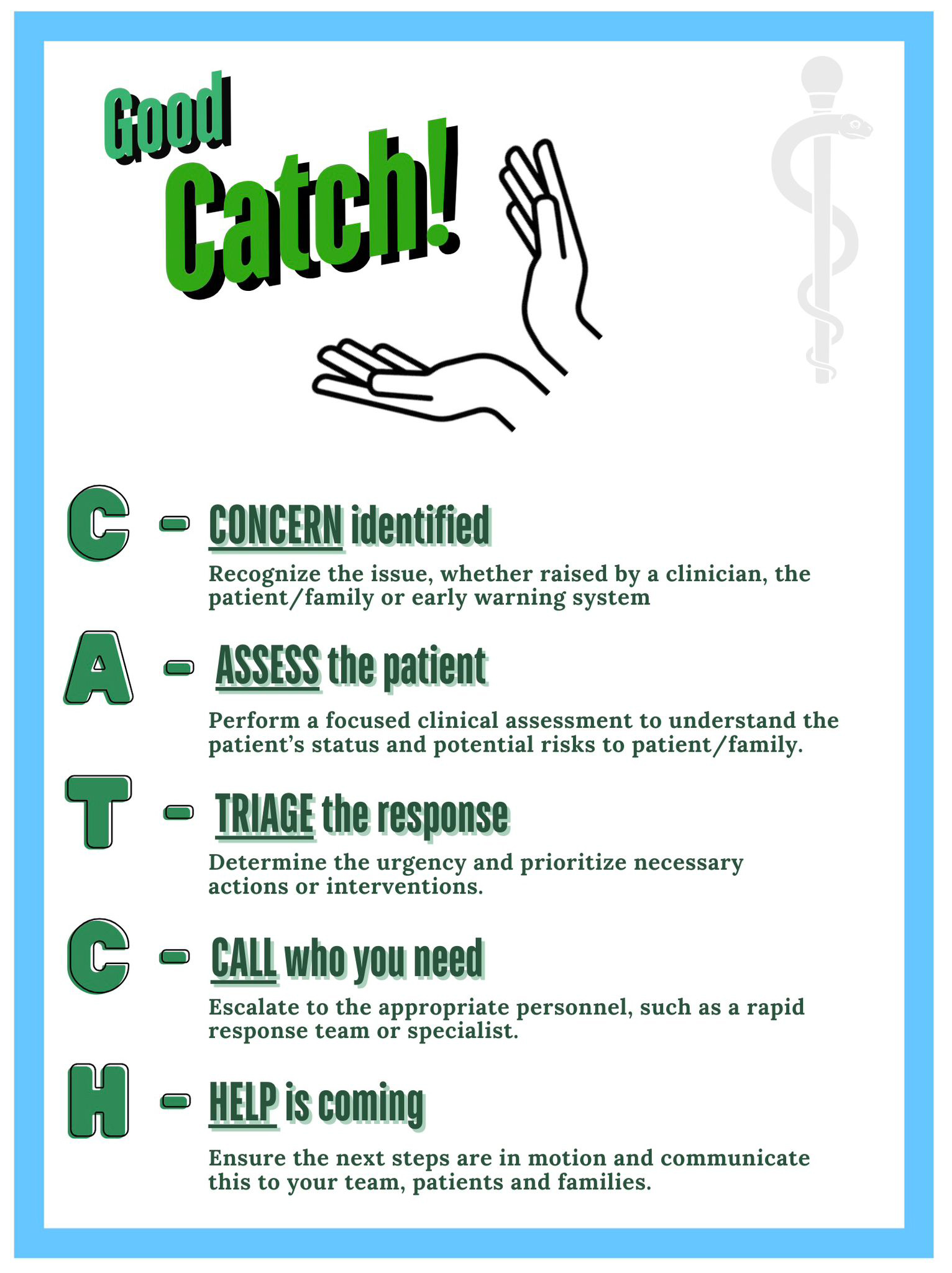 Fig. 1.
Fig. 1.
The good CATCH tool. Created with Canva (https://www.canva.cn/).
Optimizing escalation of care requires structured communication, teamwork, and a psychologically safe environment. Flattening hierarchies, fostering inclusive leadership, and implementing tools like EWSs, RRSs and PFAEs enhance escalation success. Implementing targeted strategies such as simulation-based training, human factors-specific education, standardized protocols, and leadership-driven cultural transformation fosters a proactive and resilient workforce that facilitate early escalation of care.
There is considerable scope for future research, particularly with respect to the role of Simulation, advancing technology and PFAESs. Future research should explore the long-term impact of simulation training, particularly how it sustains clinical decision-making and real-world application. Additionally, technological advances in AI and workflow ergonomics offer opportunities to enhance escalation efficiency, yet further investigation is needed to determine how these innovations integrate with human factors strategies without undermining clinical judgment. The role of PFAESs also warrants further study. While these systems empower patients and families, their effectiveness, optimal implementation, and impact on clinical workflows remain underexplored. Research should focus on ensuring they complement existing escalation frameworks without overburdening staff. Advancing these research areas could further refine escalation processes, improving early recognition of deterioration, reducing preventable harm, and fostering a safer healthcare environment.
• Standardized Communication (e.g., SBAR) and Escalation Tools Improve Escalation.
• Psychological Safety: Flat Hierarchies and Embedded Civility Culture Encourages Early Action.
• Educational Strategies (e.g., simulation) is essential to Foster Awareness and Skills in Escalating Care.
• Optimize Workload and System Design to Improve Escalation Efficiency.
• Use human factors and ergonomics (HFE) principles to Optimize Escalation Systems.
• Empower Families to Recognize and Express Concerns to Aid Early Escalation with access to PFAESs.
Not applicable.
CR led and contributed to the conceptualization, methodology, literature search, writing—original draft, visualization, project administration, and designed the “Good CATCH” escalation tool. CJ contributed to conceptualization through early discussion of scope and aims, authored the subsection on human factors training. RG contributed to conceptualization and provided clinical oversight and acted as primary corresponding author. All authors contributed to revising the manuscript critically for important intellectual content. All authors have read and agreed to the final version and are accountable for all aspects of the work.
Not applicable.
We wish to acknowledge with thanks the contributions of the University Hospitals Sussex Librarians for their assistance in sourcing and accessing literature throughout the writing process, and to thank colleagues at University Hospitals Sussex for their support during the development of this work.
This research received no external funding.
The authors declare no competing interests. Fig. 1 was created using Canva. The authors have no financial or personal relationship with Canva, and the use of this tool does not imply any endorsement.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.