

 , Dong Wu 1,3,*
, Dong Wu 1,3,*
1 State Key Laboratory of Complex Severe and Rare Diseases, Department of Gastroenterology, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, 100730 Beijing, China
2 Chinese Academy of Medical Sciences and Peking Union Medical College, 100730 Beijing, China
3 Department of Gastroenterology, The People’s Hospital of Xizang Autonomous Region, 850000 Lhasa, Xizang, China
4 Department of Pharmacy, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, 100730 Beijing, China
†These authors contributed equally.
Esophagogastroduodenoscopy (EGD) is a widely recommended screening and diagnostic method for populations at high risk of gastric and esophageal malignancies worldwide [1, 2, 3]. It is also a key diagnostic and therapeutic tool for benign upper gastrointestinal (GI) tract conditions, including gastroesophageal reflux disease, upper GI ulcers, and others.
In developed countries, EGD is routinely performed under sedation to improve patient comfort [4, 5]. However, this practice is not universally feasible. Many regions with the highest burden of gastric and esophageal cancers are developing countries [6], where the substantial demand for EGD often exceeds the availability of anesthetic resources [7]. In these resource-constrained settings, unsedated EGD remains a viable and cost-effective solution [8]. For example, in China, the world’s most populous developing country with a high demand for EGD to screen upper GI tumors, more than half of all procedures are performed under local anesthesia due to the insufficient availability of anesthesiologists, underscoring the need for strategies to improve patient experience during unsedated EGD [7]. Gagging and nausea induced by endoscope insertion remain the primary sources of discomfort and patient resistance. Various interventions have been explored to mitigate these issues. For instance, Takahashi et al. [8] demonstrated that oral breathing could facilitate the operability of unsedated EGD and may alleviate abdominal pain. Nevertheless, this intervention did not show a significant advantage in reducing overall patient discomfort. Currently, no universally accepted method has been established to improve patient experience in unsedated EGD.
Ondansetron, a highly selective 5-hydroxytryptamine-3 (5-HT3) antagonist, is commonly used to prevent post-operative and chemotherapy-induced emesis by inhibiting both peripheral and central emetic pathways. Given its oral administration, quick onset, and cost-effectiveness, we hypothesize that ondansetron could reduce the gag reflex and alleviate discomfort during unsedated EGD. This pilot study aimed to examine the feasibility and potential benefits of administering oral ondansetron prior to unsedated EGD, with the goal of determining whether progression to a larger, double-blind randomized controlled trial is warranted.
This study was a single-center randomized-controlled pilot trial conducted at Peking Union Medical College Hospital (PUMCH), a leading medical institution in China. Approximately 60–70% of EGDs at PUMCH are performed without sedation, reflecting an imbalance between the high demand for EGDs and the limited availability of anesthetic resources. This study was registered with ClinicalTrials.gov (NCT07264738, https://clinicaltrials.gov/study/NCT07264738).
Eligible participants were adults aged between 18 and 65 years who had undergone at least one unsedated EGD within the last five years at PUMCH. All unsedated EGDs were performed under topical pharyngeal anesthesia using a viscous solution of dyclonine hydrochloride. Exclusion criteria were as follows: active GI bleeding or other conditions requiring emergency endoscopy; a history of upper gastrointestinal tract surgery; severe cardiovascular, hepatic, renal, respiratory, central nervous, or hematologic diseases; pregnancy; neuropsychiatric disorders, including severe depression or severe anxiety; allergy to the anesthetic agent or 5-HT3 receptor antagonists; a history of long QT syndrome. This pilot study aims to establish proof of concept and investigate the feasibility of the ondansetron regimen in unsedated EGD procedures, while estimating key statistical parameters (e.g., variability) to inform the design of future large-scale trials. Integrating established methodological recommendations for pilot studies [9] with consideration for potential attrition and distributional variance, a sample size of 20 participants per group was determined.
Patients were randomly assigned to either the ondansetron group or the oral breathing group using simple randomization with a computer-generated randomization sequence. The sequence was generated in R (version 4.5.1; R Foundation for Statistical Computing, Vienna, Austria). Group allocation was concealed in opaque sealed envelopes. The ondansetron group (n = 20) received a single 8 mg oral dose of ondansetron (Qilu Pharmaceutical, Jinan, China; batch number: 4K0111DE9) 2–4 hours before EGD, followed by 10 mL of dyclonine hydrochloride viscous solution (0.01 g/mL, Yangtze River Pharmaceutical Group, Taizhou, China; batch number: 24101011) 15 minutes before examination. The dosing schedule was determined based on the pharmacokinetic properties of ondansetron and established dosing strategies for preventing post-operative nausea and vomiting [10]. The control group (n = 20) received instructions on oral breathing prior to the endoscopy by a nurse in a separate preparation room, along with the same dose of dyclonine. The oral breathing intervention served as an active control to mitigate expectancy bias for patient-reported outcomes in the absence of a placebo. Baseline anxiety was assessed using the Generalized Anxiety Disorder-7 (GAD-7) questionnaire the day before the procedure. All EGDs were conducted by a single, experienced endoscopist who was blinded to group allocation with conventional endoscopes GIF-H260, GIF-H290 (Olympus Corporation, Tokyo, Japan).
After enrollment, the patients completed a questionnaire regarding their previous endoscopic experience. After EGD completion, a second questionnaire was administered to assess their current experience. To account for inter-individual variability in this small-scale study, the primary outcome was defined as the change in overall discomfort between the previous and current examinations (measured on a 0–10 numeric rating scale (NRS)). Secondary outcomes included changes in gagging intensity (NRS, 0–10; 0 = no gagging, 10 = most severe gagging) and patient willingness to undergo an unsedated EGD again (NRS, 0–10; 0 = completely unwilling, 10 = completely willing). The endoscopist assessed the patients’ gagging intensity, satisfaction with patient cooperation, and examination quality, all scored via NRS. The NRS method has been previously employed to assess patient tolerance and compliance in unsedated EGD studies [11]. The duration of the procedure was also recorded. Heart rate and peripheral capillary oxygen saturation were monitored throughout the process. Patients were asked to report any symptoms experienced during the endoscopic procedure, and a follow-up visit was scheduled for seven days post-procedure, during which the endoscopist systematically inquired about post-procedural symptoms.
Categorical variables were analyzed using Fisher’s exact test. For
continuous variables, the independent samples t-test was applied for normally distributed
data, and the Mann–Whitney U test was used for non-normally distributed data. The
normality of continuous variables was tested using the Shapiro–Wilk test. A
p value of
From August to December 2025, a total of 40 patients who had undergone at least one unsedated EGD (conducted under topical pharyngeal anesthesia using dyclonine hydrochloride viscous solution) at PUMCH in the last five years were included in this study. All participants provided informed consent. Patients were randomly assigned to either the ondansetron group (ondansetron plus pharyngeal anesthesia) or the control group (pharyngeal anesthesia and oral breathing instructions). A flowchart of the study design is shown in Fig. 1. Disease diagnosis differed between the two groups, while other baseline demographic data did not differ significantly (Table 1).
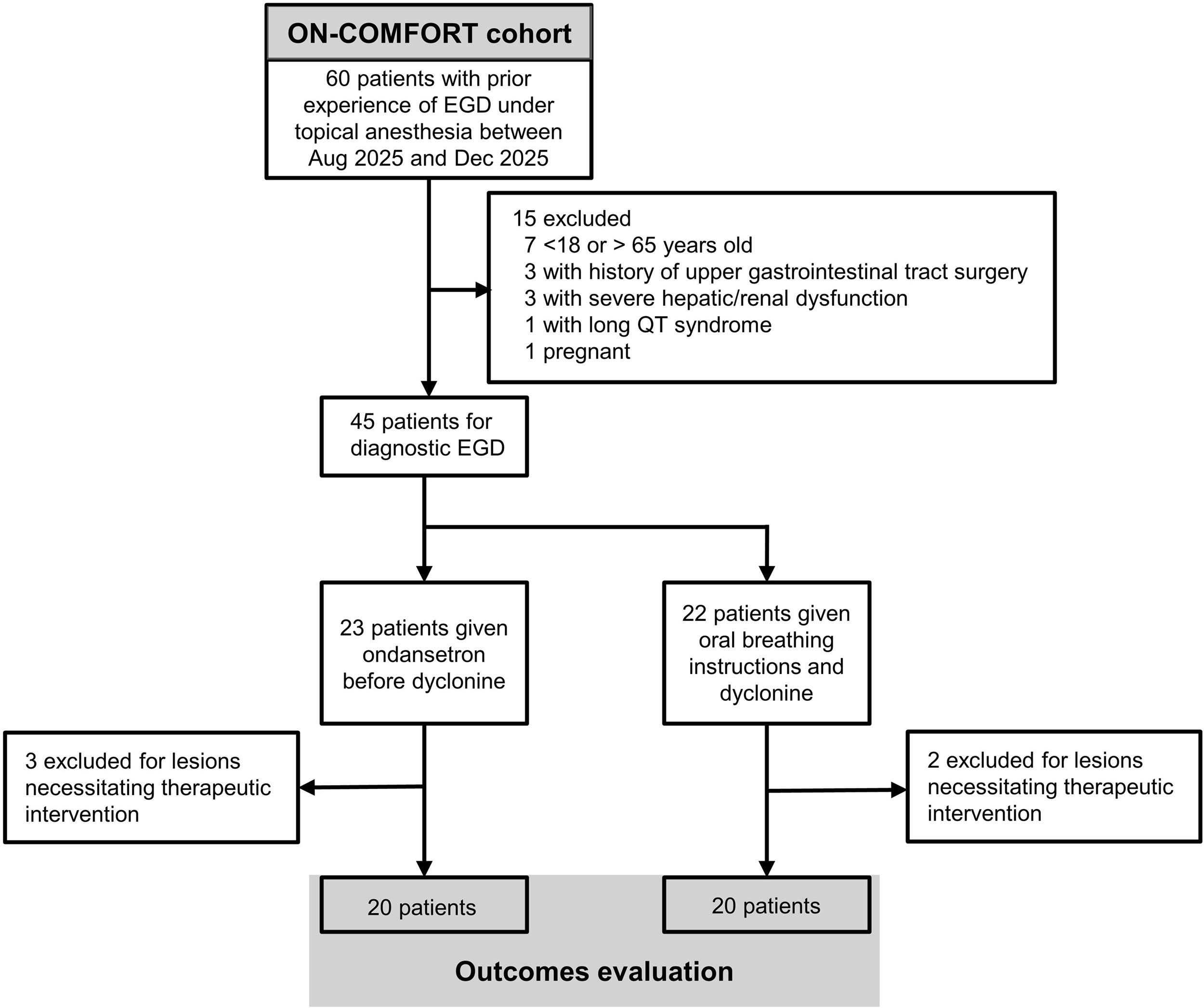 Fig. 1.
Fig. 1.
Flowchart of the study. EGD, esophagogastroduodenoscopy; ON-COMFORT, trial acronym.
| Ondansetron (n = 20) | Control (n = 20) | t/Z statistic | p value | ||
| Female, n | 10 | 8 | - a | 0.750 | |
| Age, years | 51 (48.5, 61.5) | 55.5 (46.5, 60) | –0.15 | 0.892 | |
| Body weight, kg | 69.5 (60.5, 71.5) | 65 (56, 70.5) | 1.12 | 0.266 | |
| Height, m | 1.67 |
1.66 |
0.14 | 0.893 | |
| BMI, kg/m2 | 24.76 |
23.28 |
1.37 | 0.178 | |
| Smoking, n | 2 | 5 | - a | 0.408 | |
| Drinking, n | 4 | 9 | - a | 0.176 | |
| Diabetes | 0 | 0 | |||
| Hypertension | 2 | 1 | - a | 1 | |
| GAD-7, points | 2 (1, 2) | 2 (1, 3) | –0.85 | 0.375 | |
| Indication for EGD | - | 0.502 | |||
| Abdominal pain | 10 | 8 | |||
| Regurgitation/heartburn | 3 | 1 | |||
| Bloating | 1 | 3 | |||
| Regular health examination | 2 | 5 | |||
| Others (throat pain, diarrhea, etc.) | 4 | 3 | |||
| Diagnosis | - a | 0.044 | |||
| Chronic gastritis | 8 | 8 | |||
| Gastric/duodenal ulcer | 2 | 3 | |||
| Gastroesophageal reflux disease | 5 | 1 | |||
| Gastric and esophageal polyps | 0 | 5 | |||
| Gastric cancer | 2 | 3 | |||
| Others (esophageal and gastric varices, etc.) | 3 | 0 | |||
a The categorical variables were analyzed using Fisher’s exact test; therefore, only the p value was calculated.
For normally distributed variables, data are expressed as mean
The outcomes for both groups are presented in Table 2. In comparison with the
control group, the ondansetron group demonstrated improved procedural experience.
The reduction in overall discomfort, as measured by the NRS, was significantly
larger in the ondansetron group (4.5 (3, 5.5) vs. 1 (0.5, 1), p
| Ondansetron (n = 20) | Control (n = 20) | t/Z | p value | ||
| Patient-assessed | |||||
| Overall discomfort (current), mean |
3.25 |
5.70 |
–4.83 | ||
| Overall discomfort (previous), median (Q1, Q3), 0–10 NRS | 7 (6.5, 8) | 6.5 (5, 7.5) | 1.72 | 0.080 | |
| 4.5 (3, 5.5) | 1 (0.5, 1) | 4.44 | |||
| Intensity of gagging (current), median (Q1, Q3), 0–10 NRS | 2 (1, 4.5) | 6.5 (5, 7) | –3.83 | ||
| Intensity of gagging (previous), median (Q1, Q3), 0–10 NRS | 7 (7, 8) | 7 (5, 8) | 1.16 | 0.239 | |
| 5 (3, 6) | 0 (0, 1) | 4.36 | |||
| Willingness to receive EGD again, median (Q1, Q3), 0–10 NRS | 8 (7, 10) | 5 (3.5, 7) | 3.95 | ||
| Endoscopist-assessed | |||||
| Patient gagging intensity, median (Q1, Q3), 0–10 NRS | 2.5 (2, 4) | 5 (4, 6) | –3.40 | ||
| Satisfaction with patient cooperation, median (Q1, Q3), 0–10 NRS | 8 (8, 9) | 7 (6, 7) | 3.84 | ||
| Examination quality, median (Q1, Q3), 0–10 NRS | 8 (7.5, 9) | 7 (6, 7) | 3.64 | ||
| Duration of procedure, s | 318 (288, 451) | 416 (339, 535) | –1.66 | 0.099 | |
| Adverse events | 0 | 0 | |||
a
To inform subsequent research, we exploratorily assessed the relationship between age, body weight, and treatment response. Spearman’s rank correlation analysis revealed no significant correlation between age, body weight, and overall discomfort in either group. Given the small sample size, the results were not conclusive, and the association between ondansetron treatment and anthropometric characteristics remains an area for future investigation in larger-scale clinical trials. In comparison with males, females in the ondansetron group reported lower discomfort scores (p = 0.002), a difference not observed in the control group. However, as this study was not formally powered for sex-stratified inferences due to the limited sample size, we present this finding as a hypothesis-generating observation that warrants further investigation in larger randomized controlled trials.
Unsedated EGD remains clinically valuable due to its ability to avoid sedation-related risks, such as respiratory depression and hypoxemia, while facilitating prompt patient discharge and a rapid return to daily activities. Various strategies have been explored to improve patient tolerance during unsedated EGD. Several forms of local pharyngeal anesthesia have been developed, including lozenges and ice popsicles [11]. However, their efficacy has not been consistently demonstrated, and standardization of preparation procedures remains challenging. Although virtual reality distraction has also been investigated as a method to reduce patient discomfort, no significant benefit was observed [12].
This pilot study showed that the ondansetron-dyclonine regimen is safe, easy to implement, and well-received by patients. The combination appears to be a promising intervention for improving patient tolerance during unsedated EGD with local pharyngeal anesthesia. This is particularly relevant in regions where anesthetic resources are constrained relative to the high demand for endoscopic procedures. In underdeveloped regions or primary healthcare facilities with an insufficient anesthetic workforce, unsedated EGD remains a crucial option for patients requiring endoscopic evaluation. By enhancing patient comfort and acceptance, the proposed regimen may strengthen the role of unsedated EGD as a viable and sustainable modality. In resource-constrained regions, this well-tolerated, cost-effective strategy could play an important role in improving participation in upper GI cancer screening.
Several limitations should be acknowledged. First, this study lacked a pharmacological placebo and was not double-blinded. Due to the resource constraints inherent in this pilot study, a placebo intervention was not feasible. To mitigate performance bias, oral breathing instructions were used as the control, providing patients with a perceived intervention and reducing potential expectancy effects relative to a no-intervention design. In the absence of a pharmacological placebo, this strategy represents a feasible and safe alternative that did not impose additional burden on participants. Nevertheless, expectancy bias may still have existed, as patients in the control group were aware that they received oral breathing instructions rather than a medication, which could have influenced their perception of discomfort. As such, the definitive efficacy of ondansetron in enhancing patient experience during unsedated EGD should be confirmed in large-scale, placebo-controlled trials.
To mitigate inter-individual variability and reduce bias inherent to small-scale studies, we exclusively enrolled patients with prior experience of unsedated EGD, utilizing their previous experience as a reference for the current procedure. However, the potential for recall bias should still be considered when interpreting the results. As shown in Table 2, patient evaluation of current overall discomfort was significantly lower in the ondansetron group, supporting the consistency of our findings despite the potential impact of recall bias.
Another limitation is the heterogeneity in baseline diagnosis between the two groups. Given the pilot nature of this trial and the small sample size, achieving complete balance in baseline characteristics was challenging. However, we excluded patients with severe comorbidities, and no significant differences were observed in EGD procedures or duration between the two groups. The findings suggest that the baseline severity of GI diseases was comparable between the groups. Taken together, these considerations make it unlikely that this imbalance substantially influenced the results.
This study presents preliminary evidence suggesting the potential value of ondansetron in improving patient experience during unsedated EGD. The results are promising and support further investigation through larger, double-blind, placebo-controlled randomized clinical trials to confirm the efficacy of this intervention.
• This is the first pilot randomized controlled trial to evaluate an oral 5-HT3 receptor antagonist for improving patient experience during unsedated EGD, with a focus on its potential for practical implementation in resource-constrained settings.
• The oral ondansetron–dyclonine regimen was well tolerated and
showed promising reductions in discomfort (median 4.5 vs. 1, p
• The study integrated patient-centered outcomes with endoscopist-based assessments, demonstrating that the intervention improved patient cooperation while ensuring examination quality and safety, thus supporting both the clinical benefit and practicality of the ondansetron–dyclonine regimen in unsedated EGD.
EGD, esophagogastroduodenoscopy; GAD-7, Generalized Anxiety Disorder-7; GI, gastrointestinal; NRS, numeric rating scale; PUMCH, Peking Union Medical College Hospital; 5-HT3, 5-hydroxytryptamine-3.
The data presented in this study are available on request from the corresponding authors due to privacy considerations.
DW, SYZ, and KH conceived and designed the project. QWJ and SYZ contributed resources for the investigation. KH, LJY, and QWJ performed the investigation. YYM, KP, and RT developed the methodology. YYM and KP analyzed and interpreted the data. YYM drafted the manuscript. SYZ and DW supervised the project. All authors contributed to revising the manuscript critically for important intellectual content. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
The study was conducted in accordance with the Declaration of Helsinki. The research protocol was approved by the institutional review board of the Peking Union Medical College Hospital (No. I-25PJ1723), and all of the participants provided signed informed consent.
Not applicable.
This research is funded by the Science and Technology Projects of Xizang Autonomous Region, China, grant number XZ202501JD0021.
The authors declare no conflicts of interest. Dong Wu and Kun He are serving as the Editorial Board Members of this journal. We declare that Dong Wu and Kun He had no involvement in the peer review of this article and have no access to information regarding its review. Full responsibility for the editorial process for this article was delegated to John Alcolado.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.