


 , Yan Yan 1,*
, Yan Yan 1,*
1 Department of Nephrology, Qingdao Municipal Hospital, 266011 Qingdao, Shandong, China
Abstract
Psychological distress is highly prevalent among patients undergoing maintenance hemodialysis and may adversely affect treatment adherence and overall quality of life. Evidence-based nursing (EBN) practices and cognitive behavioral theory (CBT)-based approaches have each shown potential value in dialysis care. However, evidence regarding their integration into routine nursing practice in real-world clinical settings remains limited. This study aims to examine the impact of exposure to a structured nursing care pathway incorporating EBN and CBT-informed supportive nursing on psychological, quality-of-life, and selected clinical stability outcomes in patients receiving maintenance hemodialysis.
This single-center retrospective cohort study included 236 adult patients with chronic renal failure undergoing maintenance hemodialysis between March 2023 and February 2024. Patients were classified according to the nursing care pathway received during routine clinical practice: standard care or a structured nursing care pathway integrating EBN and CBT-informed supportive communication. Propensity score matching (1:1) was applied to balance baseline demographic, clinical, laboratory, and psychological characteristics. Outcomes assessed over a 12-week observation period included nutritional markers (hemoglobin and serum albumin), the Kt/V, psychological status (Self-Rating Anxiety Scale and Self-Rating Depression Scale), quality of life (Generic Quality of Life Inventory-74), and dialysis-related complications.
After propensity score matching, 186 patients (93 per group) were included in the final analysis. Renal function indicators, electrolyte levels, and inflammatory markers remained stable in both groups throughout follow-up, with no significant between-group differences. Anxiety and depression scores were lower at follow-up in the structured nursing care pathway group than in the standard nursing care group (both p < 0.001), and both groups showed reductions in these scores from baseline (both p < 0.001). At follow-up, the structured nursing care pathway group had higher quality-of-life scores in the physical, psychosocial, and social domains (all p < 0.05), whereas no significant between-group difference was observed in the material well-being domain (p > 0.05). Dialysis adequacy and nutritional indicators were maintained within clinically acceptable ranges in both groups. The incidence of dialysis-related complications was lower in the structured care group, although statistical significance was not observed.
In a real-world clinical setting, exposure to a structured nursing care pathway incorporating EBN and CBT-informed supportive communication was associated with more favorable psychological outcomes and selected quality-of-life domains among patients undergoing maintenance hemodialysis, without compromising clinical stability. These findings suggest the potential value of optimizing nursing care pathways to address psychosocial needs in hemodialysis care.
Keywords
- end-stage kidney disease
- hemodialysis
- evidence-based nursing
- cognitive behavioral therapy
- complications
End-stage kidney disease (ESKD) represents the advanced stage of chronic kidney disease and is characterized by irreversible loss of renal function. Hemodialysis (HD) remains the most commonly used form of kidney replacement therapy for patients with ESKD worldwide [1, 2, 3]. Although HD is life-sustaining, patients undergoing long-term maintenance hemodialysis often experience substantial treatment-related burden, including repeated vascular access procedures, strict dietary and fluid restrictions, and persistent dialysis-related symptoms.
Psychological distress, particularly anxiety and depressive symptoms, is highly prevalent among patients receiving maintenance hemodialysis and may adversely affect subjective well-being, daily functioning, treatment adherence, self-management capacity, and health-related behaviors [4, 5]. Accordingly, psychological health and quality of life have become important components of comprehensive hemodialysis care alongside the maintenance of physiological stability.
Evidence-based nursing (EBN) emphasizes the integration of the best available evidence, clinical expertise, and patient values in nursing practice. In nephrology care, EBN-oriented approaches may contribute to more standardized nursing processes, improved health education, enhanced self-management, and, in some settings, reduced risk of dialysis-related complications [6, 7, 8, 9]. Cognitive behavioral therapy (CBT) has also shown potential for alleviating anxiety and depressive symptoms and improving quality of life in patients with chronic kidney disease, including those undergoing maintenance hemodialysis [10]. However, in routine dialysis settings, delivery of standardized CBT by trained mental health professionals is often limited due to staffing, time, and organizational constraints. Therefore, some centers have incorporated CBT-informed supportive elements into routine nursing communication as a pragmatic psychosocial care strategy [11].
Despite growing interest in both EBN and CBT-informed approaches in hemodialysis care, evidence remains limited regarding their integration into a structured nurse-led care pathway in routine clinical practice. Existing studies have often focused on isolated interventions, relatively small samples, or short follow-up periods, and data from real-world hemodialysis settings on psychological outcomes, quality of life, and clinical stability remain fragmented.
Therefore, the present study adopted a retrospective cohort design based on routine clinical and nursing records and applied propensity score matching to compare patients undergoing maintenance HD who were exposed to different nursing care pathways. Specifically, we examined the impact of exposure to a structured nursing care pathway incorporating EBN and CBT-informed supportive communication on patients’ psychological status, quality of life, and clinical stability, with the aim of providing practical evidence for nursing strategies in HD care.
This study was conducted as a single-center retrospective cohort study based on routinely collected clinical and nursing records. The study was performed in the Department of Nephrology, Qingdao Municipal Hospital, a tertiary hospital providing long-term maintenance hemodialysis services.
Adult patients receiving maintenance HD between March 2023 and February 2024 were screened for eligibility. After application of the inclusion and exclusion criteria, a total of 236 patients were identified for initial analysis (Fig. 1). Patients were categorized according to the type of nursing care pathway they were exposed to, namely standard nursing care and structured nursing care pathway incorporating EBN and CBT-informed supportive communication, during routine clinical practice. The grouping reflects differences in nursing pathways in routine clinical practice, rather than allocation according to the study protocol. The allocation process was not randomized. Some patients received structured nursing pathways due to routine management factors such as nursing scheduling, nursing team workflows, and feasibility of implementation; the remaining patients received only standard care. Patients in the standard care group may still receive routine emotional support and general health education during daily nursing interactions, but their nursing records do not show components of the structured pathway (such as individualized assessments, risk lists, and regular supportive communication).
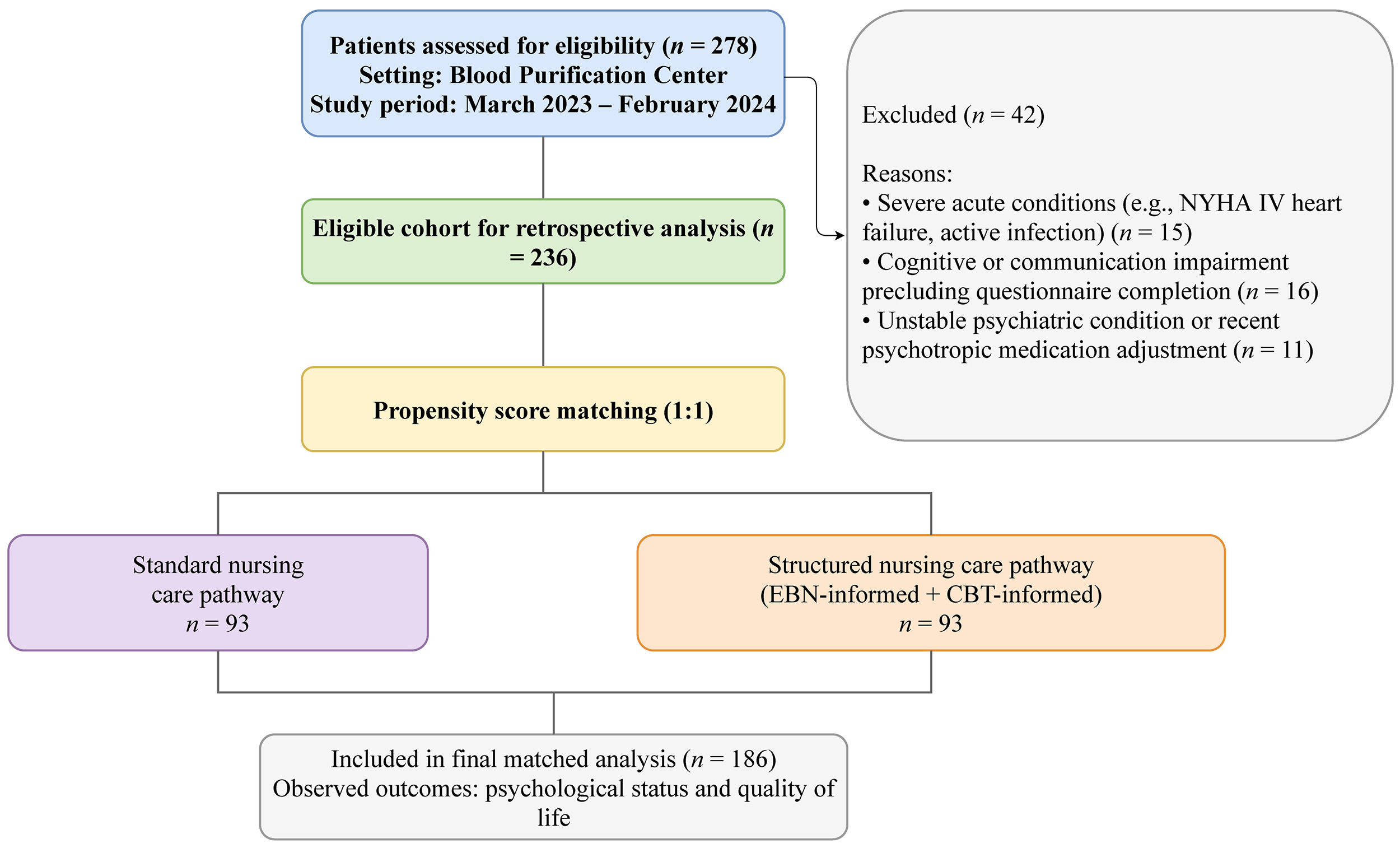 Fig. 1.
Fig. 1.
Flow diagram depicting the inclusion and exclusion of participants for the study. EBN, evidence-based nursing; CBT, cognitive behavioral therapy; NYHA, New York Heart Association.
In compliance with national regulations and institutional policies, the study protocol was approved by the Ethics Committee of Qingdao Municipal Hospital (approval No. 2025-KY-197). Given the retrospective design of this study, the use of routinely collected clinical and nursing records, the absence of any additional intervention or direct contact with participants, and the use of de-identified data for analysis, the Ethics Committee of Qingdao Municipal Hospital granted a formal waiver of informed consent. All procedures were conducted in accordance with the Declaration of Helsinki.
Patients were eligible for inclusion if they met all of the following criteria:
(1) age
To minimize potential confounding, patients were excluded if they met any of the following conditions: (1) presence of severe acute comorbid conditions, such as acute decompensated heart failure (New York Heart Association class IV) or active infection; (2) documented cognitive impairment or severe communication difficulties that precluded completion of psychological assessments; (3) unstable psychotropic medication history, defined as initiation or dosage adjustment of antidepressant or anxiolytic medications within 4 weeks prior to baseline assessment or during the 12-week observation period.
1. Standard nursing care group
Patients in the standard care group received routine nursing care as provided in the HD center. This included regular monitoring of vital signs during dialysis, vascular access care, and standard health education. Health education was delivered through routine nursing communication and periodic group education sessions, focusing primarily on general recommendations for dietary management and fluid restriction (e.g., daily fluid intake of approximately 1000 mL). Psychotropic medications, when prescribed, were maintained without proactive adjustment during the observation period unless clinically indicated.
2. Structured nursing care pathway group
In addition to standard nursing care, a subset of patients were exposed to a structured nursing care pathway during routine clinical practice. This pathway was not a formal clinical intervention but a structured organization of nursing activities over 12 weeks, without changing dialysis prescriptions, medical decisions, or pharmacological management.
The EBN component was guided by general principles of EBN, integrating available research evidence, clinical practice guidelines (including nutrition management guidelines for chronic kidney disease), and individual patient characteristics.
Nursing staff conducted individualized assessments focusing on nutritional status, fluid management, dialysis-related symptoms, and potential complication risks. Based on these assessments, nursing priorities were tailored to each patient and included: Individualized dietary and fluid management guidance; Self-management support and reinforcement of treatment adherence; Early identification of dialysis-related risks, such as intradialytic hypotension and hyperkalemia.
A pre-dialysis nursing risk checklist was routinely applied to identify potential complications, and preventive nursing measures were implemented accordingly. The checklist comprised routinely monitored nursing and clinical items, such as vascular access condition, interdialytic weight gain, blood pressure trends, dialysis-related symptoms, and electrolyte-related risk indicators. It did not introduce additional diagnostic procedures or medical interventions but functioned as a structured aid to standardize routine nursing assessment, documentation, and communication. This component was typically delivered 1–2 times per week, with each session lasting approximately 20 minutes.
The CBT-informed supportive nursing component did not involve the delivery of standardized cognitive behavioral therapy. Instead, selected supportive elements derived from cognitive behavioral theory were incorporated into routine nursing communication by senior nurses who had completed relevant training. This component aimed to support patients in understanding their illness, recognizing maladaptive illness-related cognitions, and strengthening coping strategies within the scope of nursing practice.
Supportive communication took two forms: planned sessions before dialysis or on non-dialysis days, typically once a week for 45–60 minutes, focusing on cognitive reframing, identifying stressors, and reinforcing adaptive coping strategies; brief chairside supportive interactions during the early phase of dialysis sessions, lasting approximately 15 minutes, aimed at reinforcing behavioral activation and practical coping techniques.
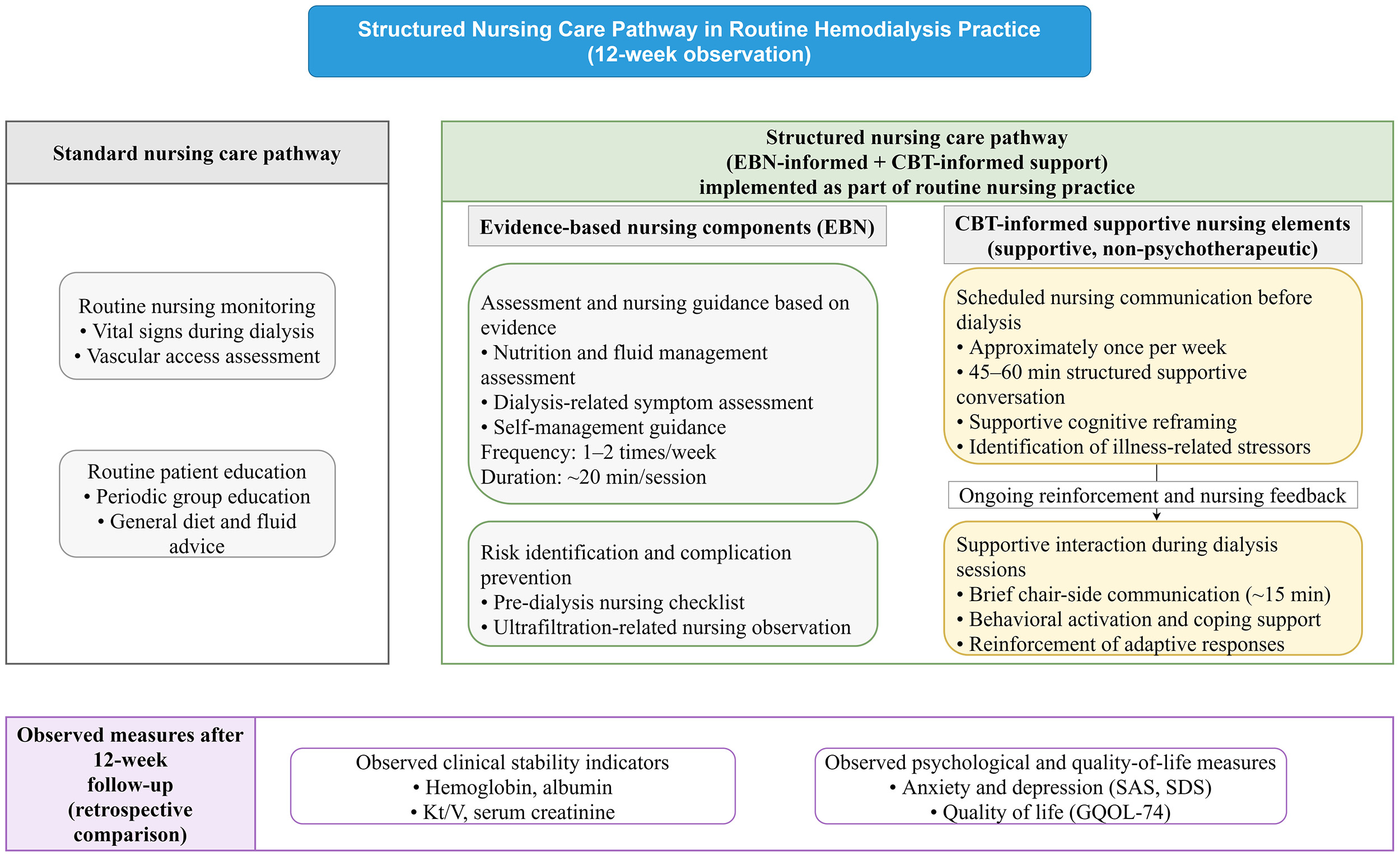
Nursing staff involved in the structured care pathway received departmental training before pathway implementation. The training focused on supportive communication principles, identification of maladaptive illness-related cognitions, basic cognitive reframing strategies within the scope of nursing practice, reinforcement of adaptive coping, and standardized documentation procedures. The pathway was delivered using predefined workflow elements, and all supportive nursing activities were documented in routine nursing records to improve consistency and traceability of care. A schematic overview of the two nursing care pathways is presented in Fig. 2.
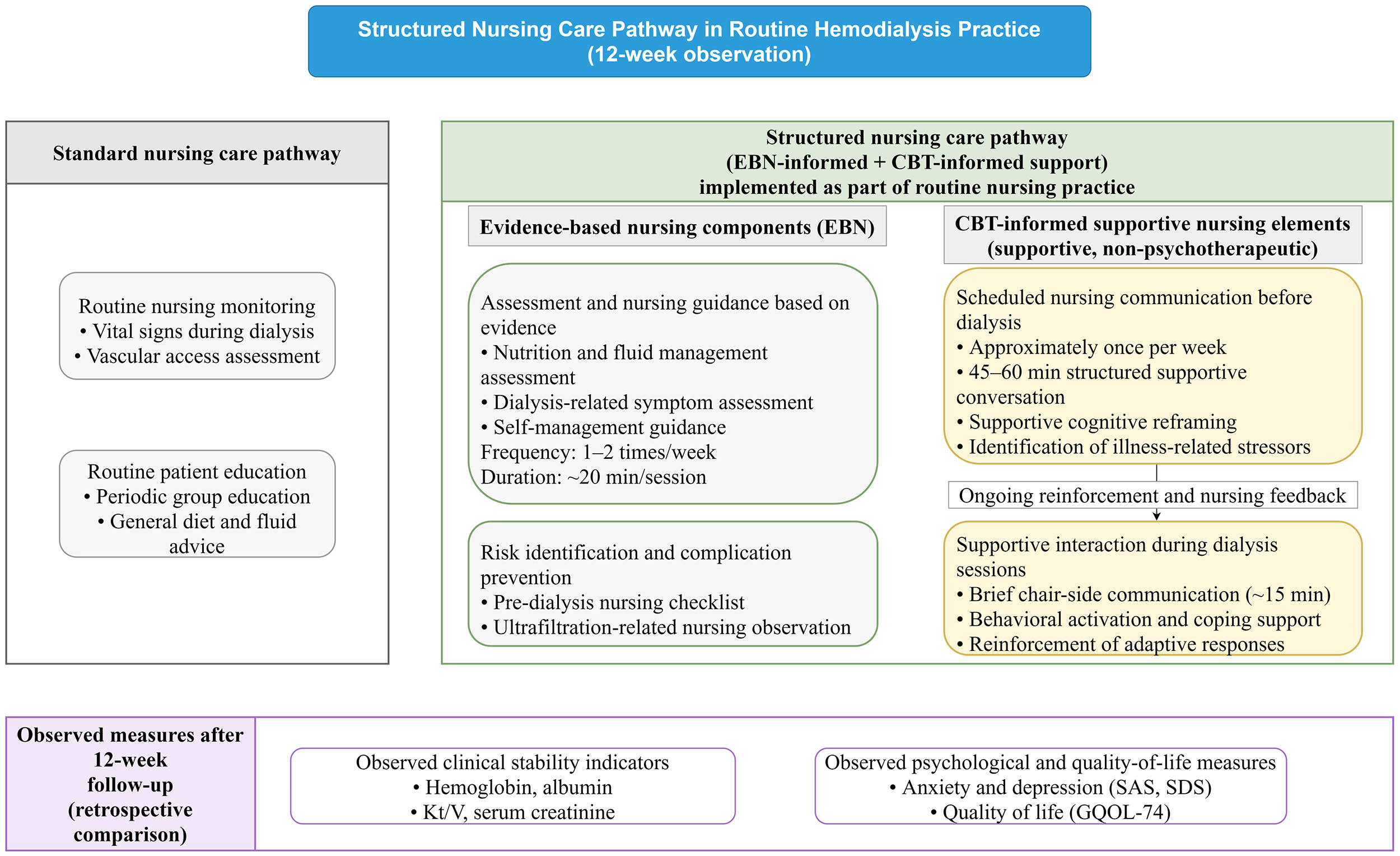 Fig. 2.
Fig. 2.
Description of nursing care pathways. GQOL-74, Generic Quality of Life Inventory-74; SAS, Self-Rating Anxiety Scale; SDS, Self-Rating Depression Scale. Kt/V: where K represents dialyzer urea clearance, t represents dialysis time, and V represents the volume of distribution of urea.
To ensure biological stability and minimize variability from dialysis timing, baseline (T0) and 12-week follow-up (T1) data were collected with a standardized protocol. Intermediate measurements were not included in the primary analysis because, in this retrospective cohort, interim data were subject to greater temporal heterogeneity and partial missingness, which could introduce additional measurement variability and bias.
All blood samples were collected during the mid-week dialysis session (Wednesday or Thursday) to minimize metabolic fluctuations associated with long interdialytic intervals. Pre-dialysis samples for serum creatinine (Scr), blood urea nitrogen (BUN), hemoglobin (Hb), serum albumin (Alb), serum calcium (Ca), serum phosphorus (P) and C-reactive protein (CRP) were collected from the case data.
Dialysis adequacy was assessed using the urea clearance index, expressed as Kt/V (where K represents dialyzer urea clearance, t represents dialysis time, and V represents the volume of distribution of urea). Kt/V was calculated using the single-pool Daugirdas II formula. For this calculation only, post-dialysis BUN samples were collected using a slow-flow or pump-stop technique to reduce access recirculation effects.
Psychological status and quality of life assessment were performed by dialysis
center nurses in the routine nursing assessment process. The nurses responsible
for the measurement of the scale had experience in using clinical scales and
received standardized training on standardized measurement and scoring processes
at the department level. In order to reduce the bias caused by the difference in
evaluators, we applied the same department evaluation process at baseline and
follow-up for the two groups of patients. Psychological status was evaluated
using the Self-Rating Anxiety Scale (SAS) and Self-Rating Depression Scale (SDS).
Standardized scores were used for analysis, with higher SAS and SDS scores
indicating more severe anxiety and depressive symptoms, respectively. In
addition, SAS scores
Dialysis-related complications during the 12-week observation period were extracted from routine medical records and nursing records, including hypotension during dialysis, hyperkalemia, vascular access-related thrombosis, infection, and acute decompensated heart failure requiring clinical treatment. The events were determined according to the physician’s diagnosis and/or standardized nursing records.
Missing data were assessed before analysis. Because this retrospective analysis required complete records for the primary outcomes and key covariates, patients with incomplete assessment records were excluded at the screening stage.
All statistical analyses were performed using R software (version 4.3.0; R
Foundation for Statistical Computing, Vienna, Austria). Normality of continuous
variables was assessed using the Kolmogorov-Smirnov test. Normally distributed
variables were expressed as mean
To reduce baseline imbalance between groups, propensity score matching (PSM) was
applied. The covariates included in the primary propensity score model were age,
gender, body mass index (BMI), dialysis time, marital status, education level,
baseline psychological scale scores (SAS and SDS), baseline laboratory and
dialysis-related variables (such as Scr, BUN, Hb, Alb, Kt/V, CRP). Patients were
matched using a 1:1 nearest-neighbor approach without replacement, with a caliper
width of 0.2 standard deviations of the logit of the propensity score. The
balance of covariates before and after matching was evaluated by standardized
mean difference (SMD). Compared with the p-value, SMD is less affected
by the sample size and is more suitable for balance judgment after matching. In
this study, SMD
Between-group comparisons were conducted using the independent t-test
or Mann-Whitney U test, as appropriate. Within-group comparisons were
performed using paired t-test or Wilcoxon signed-rank test.
Categorical variables were expressed as frequencies and percentages and compared
using Pearson’s chi-square test or Fisher’s exact test was used when expected
cell frequencies were small (e.g., any expected count
A total of 236 patients undergoing maintenance hemodialysis were initially screened for eligibility. After application of the inclusion and exclusion criteria, all eligible patients were included in the propensity score matching process. Using 1:1 nearest-neighbor matching, 186 patients were retained for the final analysis, with 93 patients in the structured nursing care pathway group and 93 patients in the standard care group (Fig. 1).
Baseline demographic and clinical characteristics before and after propensity score matching are summarized in Table 1. Prior to matching, differences were observed in several baseline variables between groups. After matching, the two groups were well balanced with respect to age, sex, BMI, dialysis duration, baseline laboratory parameters, baseline psychological scale scores, marital status and education level. All standardized mean differences after matching were below 0.15, indicating adequate covariate balance.
| Variables | Before PSM | After PSM | |||||||||
| Total (n = 236) | Standard nursing care group (n = 133) | Structured nursing care pathway group (n = 103) | p-value | SMD | Total (n = 186) | Standard nursing care group (n = 93) | Structured nursing care pathway group (n = 93) | p-value | SMD | ||
| Age (years)a, mean |
61.47 |
60.28 |
63.01 |
0.011 | 0.346 | 62.31 |
61.91 |
62.70 |
0.490 | 0.103 | |
| BMI (kg/m2)a, mean |
22.10 |
22.24 |
21.93 |
0.268 | 0.158 | 21.89 |
21.78 |
22.00 |
0.473 | 0.109 | |
| BUN (mg/dL) T0a, mean |
29.07 |
29.43 |
28.60 |
0.347 | 0.115 | 29.03 |
28.78 |
29.28 |
0.605 | 0.070 | |
| Scr (µmol/L) T0a, mean |
547.90 |
555.80 |
537.70 |
0.386 | 0.117 | 536.46 |
540.57 |
532.34 |
0.725 | 0.053 | |
| Duration (years)b, M (Q1, Q3) | 2.50 (2.00, 6.60) | 2.50 (2.10, 6.60) | 2.40 (2.00, 6.15) | 0.443 | 0.157 | 2.40 (2.00, 6.30) | 2.30 (2.00, 6.30) | 2.50 (2.00, 6.20) | 0.437 | 0.085 | |
| SAS T0b, M (Q1, Q3) | 57.00 (52.00, 65.00) | 58.00 (52.00, 65.00) | 56.00 (52.00, 65.00) | 0.151 | 0.255 | 56.50 (52.00, 65.00) | 57.00 (52.00, 65.00) | 56.00 (52.00, 65.00) | 0.637 | 0.000 | |
| SDS T0b, M (Q1, Q3) | 52.00 (52.00, 61.00) | 53.00 (52.00, 64.00) | 52.00 (52.00, 58.00) | 0.004 | 0.640 | 52.00 (52.00, 58.00) | 52.00 (52.00, 55.00) | 52.00 (52.00, 58.00) | 0.536 | 0.055 | |
| Hb (g/L) T0b, M (Q1, Q3) | 100.00 (95.00, 104.00) | 101.00 (96.00, 104.00) | 100.00 (95.00, 104.00) | 0.223 | 0.152 | 100.00 (95.00, 104.00) | 99.00 (95.00, 104.00) | 100.00 (95.00, 104.00) | 0.871 | 0.005 | |
| Alb (g/L) T0b, M (Q1, Q3) | 35.60 (34.08, 36.70) | 35.60 (34.20, 36.70) | 35.50 (33.90, 36.75) | 0.714 | 0.081 | 35.55 (33.90, 36.68) | 35.40 (34.10, 36.40) | 35.60 (33.70, 36.80) | 0.965 | 0.032 | |
| Kt/V T0b, M (Q1, Q3) | 1.32 (1.29, 1.35) | 1.33 (1.28, 1.37) | 1.31 (1.29, 1.35) | 0.684 | 0.043 | 1.33 (1.29, 1.37) | 1.33 (1.28, 1.37) | 1.32 (1.29, 1.35) | 0.856 | 0.019 | |
| CRP (mg/L) T0b, M (Q1, Q3) | 6.80 (5.10, 8.20) | 6.90 (5.30, 8.10) | 6.50 (4.70, 8.20) | 0.303 | 0.131 | 6.85 (5.12, 8.20) | 6.80 (5.40, 7.90) | 6.90 (4.70, 8.40) | 0.638 | 0.071 | |
| Marital statusc, n (%) | 0.649 | 0.878 | |||||||||
| Unmarried/divorced/widowed | 84 (35.59) | 49 (36.84) | 35 (33.98) | 0.060 | 65 (34.95) | 33 (35.48) | 32 (34.41) | 0.023 | |||
| Married | 152 (64.41) | 84 (63.16) | 68 (66.02) | 0.060 | 121 (65.05) | 60 (64.52) | 61 (65.59) | 0.023 | |||
| Education levelc, n (%) | 0.795 | 0.979 | |||||||||
| Primary school or below | 40 (16.95) | 24 (18.05) | 16 (15.53) | 0.069 | 31 (16.67) | 15 (16.13) | 16 (17.20) | 0.028 | |||
| Secondary/high school | 125 (52.97) | 71 (53.38) | 54 (52.43) | 0.019 | 99 (53.23) | 50 (53.76) | 49 (52.69) | 0.022 | |||
| College or above | 71 (30.08) | 38 (28.57) | 33 (32.04) | 0.074 | 56 (30.11) | 28 (30.11) | 28 (30.11) | 0.000 | |||
| Genderc, n (%) | 0.218 | 0.448 | |||||||||
| Female | 93 (39.41) | 57 (42.86) | 36 (34.95) | 0.166 | 69 (37.1) | 37 (39.78) | 32 (34.41) | 0.113 | |||
| Male | 143 (60.59) | 76 (57.14) | 67 (65.05) | 0.166 | 117 (62.9) | 56 (60.22) | 61 (65.59) | 0.113 | |||
Notes: at-test; bMann-Whitney test; cChi-square test; T0, baseline; M, Median; Q1, 1st Quartile; Q3, 3rd Quartile. PSM, propensity score matching; SMD, standardized mean difference; BMI, body mass index; BUN, blood urea nitrogen; Scr, serum creatinine; Hb, hemoglobin; Alb, albumin; CRP, C-reactive protein; SD, standard deviation.
The distribution of propensity scores before and after matching is shown in Supplementary Fig. 1. Limited overlap between groups was observed prior to matching, whereas substantial overlap was achieved following matching, supporting improved comparability. Before matching, there were obvious imbalances in variables such as age and baseline SDS score; all covariates after matching were lower than the preset SMD threshold, suggesting that the comparability between groups was significantly improved. Standardized mean differences for all covariates before and after matching are illustrated in Fig. 3.
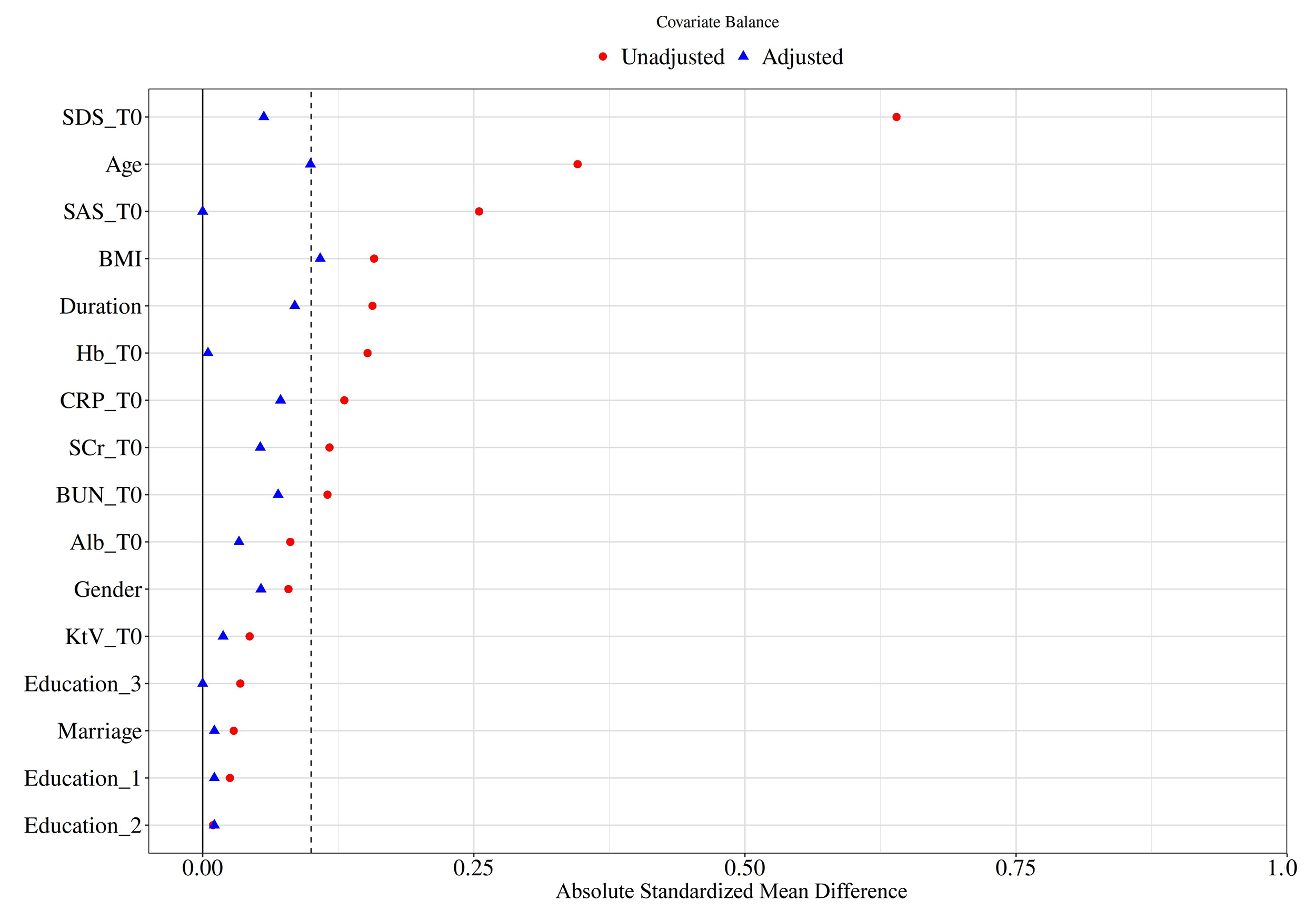 Fig. 3.
Fig. 3.
Standardized mean differences before and after matching.
Standardized mean differences (SMDs) of baseline covariates before and after
propensity score matching. After matching, all covariates showed acceptable
balance (SMD
Psychological outcomes assessed using the Self-Rating Anxiety Scale (SAS) and
Self-Rating Depression Scale (SDS) are presented in Table 2. At baseline, anxiety
and depression scores were comparable between groups (both p
| Groups | SAS T0 | SAS T1 | z | p-value | SDS T0 | SDS T1 | z | p-value |
| Standard nursing care group | 57.00 (52.00, 65.00) | 54.00 (50.00, 60.00) | −6.52 | 52.00 (52.00, 55.00) | 51.00 (49.00, 53.00) | −7.39 | ||
| Structured nursing care pathway group | 56.00 (52.00, 65.00) | 51.00 (45.00, 52.00) | −7.97 | 52.00 (52.00, 58.00) | 45.00 (42.00, 51.00) | −8.40 | ||
| Z | −0.47 | −6.20 | −0.62 | −6.56 | ||||
| p | 0.637 | 0.536 |
Notes: Z, Mann-Whitney test; z, Wilcoxon signed-rank test; T0, baseline; T1, 12-week follow-up.
During the 12-week follow-up, SAS and SDS scores were lower in patients exposed
to the structured nursing care pathway than in those receiving standard care.
Within-group analyses showed statistically significant reductions in anxiety and
depressive symptom scores over time in both groups (both p
At follow-up, patients in the structured nursing care pathway group had higher
scores in the physical function, psychosocial function, and social function
domains compared with the standard care group (all p
| Domain | Total (n = 186) | Standard nursing care group (n = 93) | Structured nursing care pathway group (n = 93) | t/Z-statistics | p-value |
| Physical function, mean |
76.37 |
73.97 |
78.77 |
t = −3.38 | |
| Social function, mean |
79.83 |
78.39 |
81.28 |
t = −3.24 | 0.001 |
| Psychosocial function, M (Q1, Q3) | 74.00 (64.00, 87.00) | 69.00 (63.00, 77.00) | 85.00 (71.00, 90.00) | Z = −5.13 | |
| Material well-being, M (Q1, Q3) | 76.00 (70.25, 85.00) | 77.00 (70.00, 86.00) | 75.00 (71.00, 81.00) | Z = −1.05 | 0.296 |
Notes: M, Median; Q1, 1st Quartile; Q3, 3rd Quartile; SD, standard deviation.
Changes in renal function parameters over the 12-week observation period are
presented in Table 4. Pre-dialysis serum creatinine and blood urea nitrogen
levels remained clinically stable in both groups from baseline to follow-up. No
statistically significant within-group changes were observed (all p
| Group | Scr T0 (µmol/L) | Scr T1 (µmol/L) | t# | p-value | BUN T0 (mg/dL) | BUN T1 (mg/dL) | t# | p-value |
| Standard nursing care group | 540.57 |
541.66 |
−0.56 | 0.579 | 28.78 |
28.83 |
−0.59 | 0.558 |
| Structured nursing care pathway group | 532.34 |
532.25 |
0.06 | 0.954 | 29.28 |
29.06 |
1.06 | 0.290 |
| t | 0.35 | 0.40 | 0.52 | –0.24 | ||||
| p | 0.725 | 0.686 | 0.605 | 0.807 |
Notes: t: t-test; #: paired t-test; T0: baseline;
T1: 12-week follow-up. All data are expressed as mean
Serum calcium and phosphorus levels remained clinically stable throughout the
follow-up period in both groups (Table 5), with no significant between-group
differences observed at follow-up (all p
| Group | Ca T0 | Ca T1 | z | p-value | P T0 | P T1 | z | p-value | CRP T0 | CRP T1 | z | p-value |
| Standard nursing care group | 2.22 (2.13, 2.31) | 2.21 (2.11, 2.32) | −0.95 | 0.343 | 1.55 (1.30, 1.63) | 1.50 (1.33, 1.72) | −1.24 | 0.214 | 6.80 (5.40, 7.90) | 5.90 (4.40, 7.70) | −2.40 | 0.016 |
| Structured nursing care pathway group | 2.26 (2.17, 2.33) | 2.25 (2.15, 2.32) | −0.63 | 0.528 | 1.49 (1.30, 1.63) | 1.50 (1.30, 1.74) | −1.22 | 0.220 | 6.90 (4.70, 8.40) | 6.00 (4.50, 7.40) | −2.72 | 0.007 |
| Z | −1.38 | −1.19 | −0.34 | −0.07 | −0.47 | −0.42 | ||||||
| p | 0.167 | 0.232 | 0.736 | 0.942 | 0.638 | 0.676 |
Notes: Z, Mann-Whitney test; z, Wilcoxon signed-rank test; T0, baseline; T1, 12-week follow-up. All data are expressed as M (Q1, Q3). Ca, serum calcium; P, serum phosphorus; CRP, C-reactive protein.
Baseline and follow-up values for Hb, Alb, and Kt/V are summarized in Table 6.
At baseline, Hb and Alb levels were comparable between the two groups (both
p
| Group | Hb T0 (g/L) | Hb T1 (g/L) | z | p-value | Alb T0 (g/L) | Alb T1 (g/L) | z | p-value | Kt/V T0 | Kt/V T1 | z | p-value |
| Standard nursing care group | 99.00 (95.00, 104.00) | 99.00 (96.00, 103.00) | −0.72 | 0.474 | 35.40 (34.10, 36.40) | 35.50 (33.70, 36.80) | −0.35 | 0.729 | 1.33 (1.28, 1.37) | 1.35 (1.31, 1.39) | −5.94 | |
| Structured nursing care pathway group | 100.00 (95.00, 104.00) | 99.00 (95.00, 104.00) | −1.19 | 0.234 | 35.60 (33.70, 36.80) | 35.80 (33.90, 36.70) | −0.50 | 0.615 | 1.32 (1.29, 1.35) | 1.36 (1.32, 1.40) | −4.19 | |
| Z | −0.16 | −0.19 | −0.04 | −0.33 | −0.18 | −1.04 | ||||||
| p | 0.871 | 0.847 | 0.965 | 0.741 | 0.856 | 0.300 |
Notes: Z, Mann-Whitney test; z, Wilcoxon signed-rank test; T0, baseline; T1, 12-week follow-up. All data are expressed as M (Q1, Q3).
Dialysis adequacy, as assessed by Kt/V, remained clinically stable over time in
both groups. Although statistically significant within-group changes were
observed, these changes were small in magnitude, and no significant between-group
difference was identified at follow-up (p
Dialysis-related complications during the 12-week observation period are summarized in Table 7. The proportion of patients with any recorded complication was numerically lower in the structured nursing care pathway group than in the standard nursing care group (13.98% vs. 24.73%), although the between-group difference did not reach statistical significance (p = 0.063). The overall distribution of complication categories did not differ significantly between groups (p = 0.397).
| Variable | Total (n = 186) | Standard nursing care group (n = 93) | Structured nursing care pathway group (n = 93) | p-value | ||
| Complication, n (%) | 3.44 | 0.063 | ||||
| No | 150 (80.65) | 70 (75.27) | 80 (86.02) | |||
| Yes | 36 (19.35) | 23 (24.73) | 13 (13.98) | |||
| Complication category, n (%) | 0.397 | |||||
| Heart failure | 7 (3.76) | 3 (3.23) | 4 (4.30) | |||
| Hyperkalemia | 9 (4.84) | 6 (6.45) | 3 (3.23) | |||
| Hypotension | 8 (4.30) | 6 (6.45) | 2 (2.15) | |||
| Infection | 7 (3.76) | 5 (5.38) | 2 (2.15) | |||
| None | 150 (80.65) | 70 (75.27) | 80 (86.02) | |||
| Thrombosis | 5 (2.69) | 3 (3.23) | 2 (2.15) | |||
Notes: “Complication” indicates whether any dialysis-related complication occurred during the 12-week follow-up. “Complication category” indicates the mutually exclusive category of recorded dialysis-related complication during follow-up (heart failure, hyperkalemia, hypotension, infection, thrombosis, or none). The p-value for “Complication” was obtained using Pearson’s chi-square test. The p-value for “Complication category” represents an overall between-group comparison across all categories; Fisher’s exact test was used because of sparse cell counts. All data are expressed as n (%).
In this retrospective cohort study with propensity score-matched comparisons, we examined whether exposure to different nursing care pathways was associated with psychological, quality-of-life, and selected clinical stability outcomes in patients undergoing maintenance HD. The findings indicate that exposure to a structured nursing care pathway incorporating EBN and CBT-informed supportive communication was associated with more favorable psychological outcomes and selected domains of quality of life, while renal function and most biochemical parameters remained clinically stable. These results suggest that the value of this nursing model lies in supporting disease management and improving patient experience, rather than altering the underlying pathological processes of ESKD.
During the 12-week follow-up, pre-dialysis serum creatinine and blood urea nitrogen levels remained stable in both groups, with no statistically significant between-group differences at follow-up. In addition, electrolyte parameters, including calcium and phosphorus, showed no significant between-group differences during the follow-up period, while C-reactive protein decreased slightly within both groups but did not differ significantly between groups at follow-up. Given that maintenance hemodialysis functions as kidney replacement therapy and that dialysis adequacy is primarily maintained through the prescribed dialysis regimen rather than restoration of intrinsic renal function, the absence of marked improvement in renal function-related biochemical indicators was clinically expected [16]. These findings suggest that the structured nursing care pathway did not compromise biochemical or dialysis-related clinical stability during the observation period. Therefore, the observed benefits of the pathway should be interpreted mainly in relation to psychological status and selected quality-of-life domains, rather than improvement in renal function.
Hemoglobin and serum albumin levels remained largely stable over the follow-up period, with only minor numerical fluctuations observed. Previous studies have shown that hemoglobin levels in HD patients are predominantly regulated by erythropoiesis-stimulating agents and iron metabolism, while serum albumin reflects a complex interplay between nutritional intake, inflammatory burden, and metabolic status [17, 18]. Consequently, short-term nursing or supportive psychological interventions are unlikely to induce marked physiological changes in these parameters. Dialysis adequacy, as measured by Kt/V, showed small numerical increases over time in both groups. Given that dialysis prescriptions and technical parameters were not systematically modified during the study period, these within-group changes are more likely to be related to the improvement of procedural adherence and routine care optimization rather than a direct effect of the nursing care pathway itself.
An important finding of this study is that anxiety and depressive symptom scores decreased over time in both groups, with greater reductions observed among patients exposed to the structured nursing care pathway. Improvements in both groups likely reflect nonspecific factors, including time effects, the supportive influence of routine nursing care and ongoing clinical contact. Regression toward the mean may also have contributed to symptom reduction over time, particularly given the elevated baseline psychological scores. Notably, most patients remained within the range of mild psychological symptoms at follow-up, indicating symptom alleviation rather than remission across diagnostic thresholds. This pattern supports the findings of the meta-analysis by Chahal et al. [19], which highlighted the role of cognitive behavioral approaches in reducing depressive symptoms among patients with chronic kidney disease.
Importantly, the CBT-informed support applied in this study did not constitute standardized psychotherapy delivered by mental health professionals. Instead, CBT-based supportive elements were incorporated into routine nursing communication by trained nursing staff. The observed psychological benefits are therefore more likely related to improved illness understanding, reduced feelings of helplessness and catastrophizing, and enhanced coping capacity rather than formal therapeutic intervention. Consistent with this interpretation, previous studies have reported similar psychological and quality-of-life benefits from internet-delivered CBT [20] and combined CBT–mindfulness interventions in hemodialysis populations [21].
Differences in quality-of-life scores were primarily observed in three domains of the GQOL-74, with significantly higher scores in the structured nursing care pathway group compared with the standard care group. These domains are closely linked to symptom burden, emotional well-being, and social participation, which may be particularly responsive to enhanced nursing communication and psychosocial support. In contrast, no significant between-group difference was observed in the material well-being domain, likely reflecting the stronger influence of socioeconomic factors and broader social determinants that are less amenable to modification through short-term clinical nursing interventions. These findings are consistent with the study by Alodhailah and Almutairi [22], which reported that adherence to EBN practices accounted for a substantial proportion of the variance in quality of life and was associated with improvements in both physical and mental health among patients with chronic kidney disease. Similar improvements in physical health components have also been reported in studies evaluating technology-assisted CBT in ESKD [23]. Collectively, these results suggest that optimizing nursing care pathways may contribute meaningfully to improving patients’ subjective experience of illness.
Given the short follow-up duration and low event frequency, complication outcomes should be interpreted descriptively rather than inferentially. With respect to safety outcomes, the incidence of dialysis-related complications was lower in the structured nursing care pathway group, although the difference did not reach statistical significance. The distribution of complications was consistent with the expected clinical profile of maintenance HD patients. Previous studies have suggested that EBN practices, through systematic risk assessment, patient education, and continuous monitoring, may help reduce the occurrence of certain dialysis-related complications [24, 25]. The present findings suggest that structured nursing care pathways may play a supportive role in complication prevention, but not substituting for standard medical management.
Several limitations should be acknowledged. First, this was a single-center observational retrospective cohort study. Although propensity score matching was used to improve baseline comparability between groups, unmeasured confounding and residual bias cannot be fully excluded. Unmeasured factors such as nurse communication style, variability in supportive interaction quality, patient health literacy, family or social support, and unrecorded socioeconomic characteristics may have influenced the psychological and quality-of-life outcomes and favored the structured care group in routine practice, particularly for self-reported outcomes. In addition, because no regression-based adjustment or other doubly robust method was applied after matching, the robustness of the estimates remains limited. Therefore, the findings should be interpreted as association-based and hypothesis-generating rather than as evidence that the structured nursing care pathway independently produced the observed psychological and quality-of-life benefits. The lack of baseline quality-of-life data further increased the possibility of residual imbalance in outcome measures, while the absence of implementation fidelity data prevented quantitative assessment of adherence intensity, inter-provider variability, and delivery consistency. Moreover, the reduced sample size after matching may have limited statistical power for low-incidence outcomes, and the single-center setting may restrict the generalizability of the findings. Second, group allocation was based on routine clinical practice rather than randomization, and the study was inherently open-label. Both patients and nursing staff were aware of the nursing care pathway received, and psychological status and quality of life were assessed using self-report instruments, which may have introduced measurement bias and expectancy effects. Although patients with unstable psychotropic medication use were excluded to reduce pharmacological confounding, it remains difficult to fully control for external social or life events that may influence psychological outcomes in a retrospective context. Third, the CBT-informed support applied in this study was delivered by trained nursing staff rather than professional psychotherapists and should not be equated with standardized CBT. Fourth, patients with overt cognitive impairment or severe communication difficulties were excluded to ensure the validity of psychological assessments. While this approach improved data quality, it may limit the generalizability of the findings to populations with mild cognitive impairment. Finally, the 12-week follow-up period is relatively short for assessing the persistence of psychological improvement and long-term clinical outcomes (such as recurrent complications, renal function, and nutritional indicators), and further longer follow-up studies are needed to determine whether the associations observed in this study are sustainable.
In the future, multicenter prospective studies are needed to further validate the present findings. Where feasible, randomized allocation may be considered, and more objective functional outcome measures may be included. In addition, to reduce residual confounding, future studies should prospectively collect data on patient health literacy, family and social support, psychiatric treatment history, and exposure to external psychosocial services, and should incorporate repeated quality-of-life assessments when possible. To improve the standardization of nursing pathway delivery in subsequent studies, core implementation elements and process indicators should be predefined at the protocol-development stage, including completion of individualized nursing assessments, adherence to the pre-dialysis risk checklist, frequency and duration of planned CBT-informed supportive communication, coverage of chairside supportive interactions, nurse training completion, documentation completeness, and protocol deviations. Predefining and continuously monitoring these indicators may strengthen the assessment of implementation consistency and improve reproducibility across centers.
In this retrospective cohort study, exposure to structured nursing pathways that integrate EBN and CBT-informed supportive communication was associated with better psychological outcomes and selected dimensions of quality of life in maintenance HD patients, while clinical stability was maintained. Prospective multicenter studies are warranted in the future to further assess implementation fidelity, long-term persistence, and potential causal effects.
• This retrospective cohort study, using propensity score matching, examined the impact of different nursing care pathways on psychological, quality-of-life, and selected clinical stability outcomes among patients undergoing maintenance hemodialysis.
• Exposure to a structured nursing care pathway incorporating evidence-based nursing (EBN) and cognitive behavioral theory (CBT)-informed supportive communication was associated with alleviation of anxiety and depressive symptoms and improvements in selected domains of quality of life.
• Renal function and most biochemical parameters remained clinically stable during the follow-up period, with no evidence of meaningful functional improvement.
• The incidence of dialysis-related complications did not differ significantly between groups, highlighting the inherent limitations of non-pharmacological approaches in modifying hard clinical endpoints.
• These findings support the optimization of nursing care pathways and communication strategies within routine hemodialysis practice to improve patients’ psychological well-being and treatment experience.
The data that support the findings of this study are available from the corresponding author upon reasonable request.
YL and YY designed the research study. YL performed the research. YL and YY analyzed the data. YY drafted the article. Both authors contributed to the important editorial changes in the manuscript. Both authors read and approved the final manuscript. Both authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
The study protocol was approved by the Ethics Committee of Qingdao Municipal Hospital (approval No. 2025-KY-197). Given the retrospective design of this study, the use of routinely collected clinical and nursing records, the absence of any additional intervention or direct contact with participants, and the use of de-identified data for analysis, the Ethics Committee of Qingdao Municipal Hospital granted a formal waiver of informed consent. All procedures were conducted in accordance with the Declaration of Helsinki.
Not applicable.
This research received no external funding.
The authors declare no conflicts of interest.
Supplementary material associated with this article can be found, in the online version, at https://doi.org/10.31083/BJHM49922.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.