


 , Aalaa Jawad 1, Gillian Smith 2
, Aalaa Jawad 1, Gillian Smith 21 Department of Population Health, Royal Free London NHS Foundation Trust, NW3 2QG London, UK
2 Royal Free London NHS Foundation Trust, NW3 2QG London, UK
Prevention is the word of the moment in UK healthcare. One of three key government commitments for the popular state-funded National Health Service (NHS) is to shift from sickness to prevention [1]. We can define it, we have clear evidence of what works, we know how to do it…and yet we don’t routinely embed prevention in a systematic, universal and joined up fashion across the NHS and in our hospitals. Why not?
In this editorial, we aim to demystify prevention and turn it into something tangible for the hospital practitioner. We aim to explain why we cannot afford not to embed prevention as our cultural norm—our business as usual—in secondary care.
One of the Government’s five missions is to “build an NHS fit for the future” [1]. This mission requires three big reform shifts, one of which is “from sickness to prevention”.
Lord Darzi’s report [2] highlighted significant issues in the NHS and called for a cultural shift within the NHS to prioritise patient engagement and empowerment, enabling individuals to take an active role in managing their health. “By focusing on prevention and early intervention, the NHS can improve patient outcomes, enhance efficiency, and ensure long-term sustainability”. Implementing these recommendations is crucial for transforming the NHS into a more resilient and patient-centred healthcare system.
Historical increases in life expectancy are now stalling across the UK and even decreasing for women in the most deprived quintiles. There has also been a fall in healthy life expectancy (the proportion of life spent in a state of good health) [3].
The government’s ambition is to ‘halve’ the gap in healthy life expectancy between the richest and poorest regions through a shift from sickness to prevention, by becoming a service that can ‘pre-empt need, where it currently predominantly reacts to it’ [1]. The plan considers the inequalities in the distribution of healthy behaviours, and the use of prevention in ‘pushing poor health into later life - and helping millions more get on with their lives, raising their children and progressing their careers unimpeded by avoidable sickness’ [1].
The long-term conditions of cancer, cardiovascular disease and respiratory disease are major causes of death as well as major contributors to health inequalities and decreased healthy life expectancy. Currently 1 in 4 adults in England have at least two health conditions, with over 26 million people living with a diagnosed long-term condition. The number of people living with a major illness is projected to increase by 37% by 2040 creating additional financial and system pressure for the NHS [4].
We know that healthcare services are estimated to contribute to 20% of health outcomes, and modifiable health behaviours of smoking, alcohol, physical activity and healthy eating, contribute to 30% of health outcomes (Fig. 1) [5].
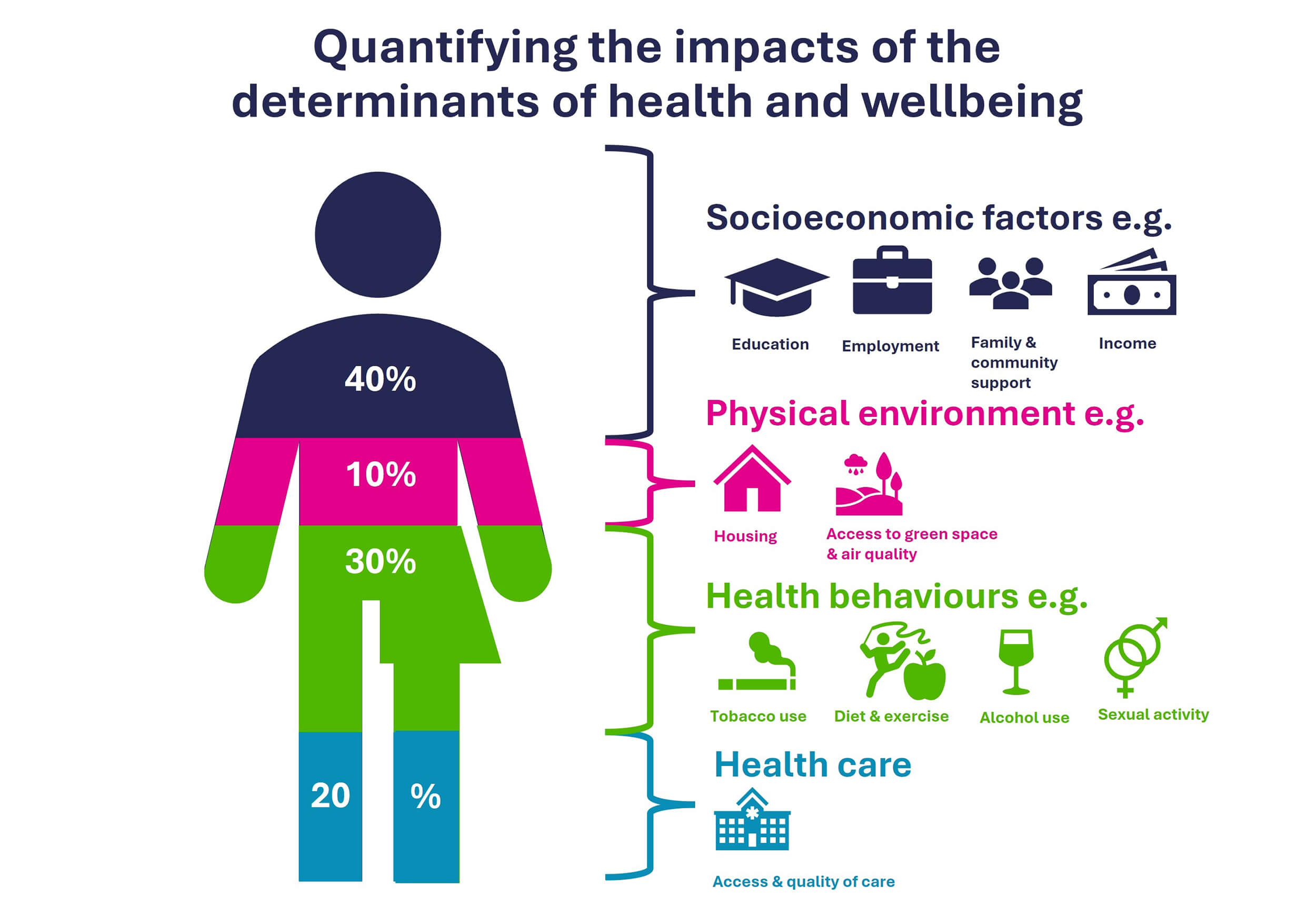 Fig. 1.
Fig. 1.
Quantifying the impacts of the determinants of health and wellbeing. Image obtained with permission from North Central London ICB, October 2025 [unpublished].
Healthcare settings provide a unique interface where we can address the significant impact of health behaviours, the wider determinants of health that drive them, and the healthcare provision itself [6]. Embedding these services locally, and working with communities, enables the actualisation of a population health approach that brings together the interconnecting parts of the same system in hospital settings.
Achieving the ambition of reducing health inequalities requires prioritising prevention through partnership working and having the systems and structures that support this, while empowering communities and individuals to make the required changes. Interventions can range from staff training and education in motivational interviewing, optimising and training in signposting and referral processes, incentivisation schemes to promote healthy behaviours, and restrictions of products and services in an organisation.
The main modifiable factors for cancer, cardiovascular disease and respiratory disease are smoking, alcohol, physical activity and diet. These factors are patterned with deprivation, with those from more deprived wards being more likely to smoke and are clustered with other behaviours such as drinking more than the recommended levels of alcohol, having a poorer diet, and being more likely to be obese [7].
The NHS sees over one million patients a day. We know that these ‘teachable moments’ are impactful. In North Central London (NCL), the prevalence of smoking is higher in our patient population (20%), than our local population (12%). Hence, taking a holistic approach with our patients as trusted healthcare professionals, who are empathetic and understanding of the complexity of their circumstances, improves the health of our population and reduces health inequalities [8]. In the NCL Integrated Care System (ICS), managing patients with long term conditions equates to 70% of the total healthcare spend, accounting for 50% of general practitioner (GP) appointments, 64% of hospital appointments and 70% of hospital bed days. There is a real opportunity to reduce system pressure through evidenced, highly clinically and cost-effective interventions that ‘make every contact count’ (MECC), as outlined in Public Health guideline [9, 10].
Embedding prevention in healthcare settings is not a linear intervention, but by embedding a culture of prevention, we can prevent or delay the development of long-term conditions in our local populations, as per the ‘Fit for the Future’ ambitions [1] through a multitude of touch points and teachable moments that encourage and support behaviour change. This culture change envelops the whole patient experience from the nudging automated notification confirming an appointment which includes a health promotion message, to the healthcare assistant trained in motivational interviewing asking about smoking, to the clinician accessing a streamlined referral process to drug and alcohol services, to the Trust promoting active travel and the trust board investing in a population health approach. This holistic approach can reduce costs, service demand, system pressure and improve outcomes.
At RFL, a large group of hospitals with over 18,000 staff working in 70 sites across North London and Hertfordshire, the Faculty of Population Health has been set up to routinely embed prevention across the trust through a staff education and training and culture change programme [11]. It aims to empower staff and patients to have culturally competent conversations to live well, improve their health, and prioritise prevention. As per National Institute for Health and Care Excellence (NICE) guidance, the faculty uses patient and visitor interactions as ‘teachable moments’ to confidently offer very brief advice and brief advice on stopping smoking, reducing alcohol intake, being physically active, and healthy eating [9, 10]. A training provider has been commissioned with a focus on upskilling staff in motivational interviewing with an emphasis placed on ensuring such conversations are culturally sensitive and in-tune with the needs of our local population. Alongside the faculty, RFL is also working on the systems and structures within the trust to make it easier to record, monitor, support and refer to local community services to improve healthy behaviours.
The impact of these teachable moments is clear. 1 in 4 people would be active if a healthcare professional advised it [12], and the feasibility of implementation is possible with a coordinated infrastructure [13]. There is published evidence of in-year financial benefit too. Implementing an inpatient smoking cessation programme will ‘save’ our trust £1 million pounds (USD 1.33 million) a year and 200 lives a year, due to decreased length of stay, reduced readmissions and reduced attendance at Accident and Emergency (A&E) 30 days after discharge [14].
We are grateful to the Royal Free Charity for funding the first three years of the Faculty. We started small, co-developing our methodology and approach with a number of pilot sites led by a diverse range of passionate and committed leaders. We have taken this learning into our second year and are embedding this learning in more strategic and trust-wide initiatives.
If large‑scale preventive work were easy, it would already be routine. We explored what gets in the way, and staff highlighted barriers such as limited confidence in discussing health behaviours, competing workload pressures, and uncertainty about whether their role allowed these conversations. Ensuring accountability, we are implementing a comprehensive co-designed and co-developed approach and are evaluating the impact through benefits to patients, staff, and the trust (including finances).
We trained 2000 staff in our first year through a series of presentations, on-the-ward training and departmental training. We listened to feedback from our staff and created a range of resources—cards, banners, posters, digital screens—to demystify MECC. Our staff told us they did not like the phrase MECC—so we call our approach ‘healthy conversations’. We plan to increase scale and scope in our second year, creating a formal community of practice, having regular lunch and learns, and setting up a sustainable train-the-trainer model.
We have a robust evidence base for cost-effective and clinically-effective prevention interventions for our patients. We see over one million patients each day in the NHS in ‘teachable moments’ that can have significant benefit on individual patients’ lives, on the lives of their families and can reduce system pressure and save money. What is your first step to embed prevention in your trust? When will you take it?
• Despite strong evidence and national policy support, prevention is not yet embedded as routine practice in hospital settings even though it is essential to address worsening health outcomes and reduce system pressure in secondary care.
• We have robust evidence base (including NICE guidance) for cost-effective and clinically effective prevention interventions for our patients.
• Hospitals offer daily opportunities for “teachable moments” that can influence patient behaviour and reduce health inequalities in the one million patients seen each day in the NHS.
• The Royal Free London Faculty of Population Health is leading a cultural and structural transformation to make prevention standard practice across the trust through systemic changes and staff training and education.
Not applicable.
JS, AJ and GS designed the work. JS drafted the manuscript. All authors contributed to important editorial revisions of the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agree to be accountable for all aspects of the work.
Not applicable.
Not applicable.
The Faculty of Population Health is funded by the Royal Free Charity Grant 1193/PE from 2024-2027.
JS is a cancer patient at RFL, as well as the RFL Director of Population Health. GS is a trustee of the Royal Free Charity, as well as RFL Group Chief Medical Officer. AJ declares no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.