



1 Department of Pediatric Digestive, Women and Children’s Hospital of Ningbo University, 315012 Ningbo, Zhejiang, China
Abstract
Providing effective nursing interventions alongside pharmacological treatment is essential for enhancing children’s cooperation, alleviating clinical symptoms, and promoting recovery. This study aims to investigate the effects of therapeutic play combined with emotional soothing care on clinical outcomes, nutritional status, and sleep quality in children with acute diarrhea, and to inform a comprehensive nursing strategy for clinical management.
This retrospective study included 148 children with acute diarrhea admitted to the Women and Children’s Hospital of Ningbo University between June 2023 and May 2025. Participants were grouped according to the nursing intervention received: children receiving emotional soothing care were assigned to the control group (n = 78), whereas those receiving therapeutic play combined with emotional soothing care were assigned to the observation group (n = 70). Baseline characteristics and clinical data were extracted from the medical record system and comparatively analyzed between groups.
The observation group demonstrated significantly shorter diarrhea cessation time, abdominal pain cessation time, and length of hospital stay compared with the control group (p < 0.05). No statistically significant difference in fever resolution time was observed between the groups (p > 0.05). In the viral etiology subgroup, the observation group showed significantly shorter diarrhea cessation time, shorter abdominal pain cessation time, and a shorter length of hospital stay compared to the control group (p < 0.05). In the bacterial etiology subgroup, diarrhea cessation time and abdominal pain cessation time were also significantly shorter in the observation group (p < 0.05), whereas the difference in length of hospital stay between groups was not statistically significant (p > 0.05). Following the intervention, serum albumin (Alb), prealbumin (PA), and hemoglobin (Hb) levels in the observation group were significantly higher than those in the control group (p < 0.05). Post-intervention scores for sleep quality, sleep latency, sleep duration, sleep efficiency, sleep disturbances, daytime dysfunction, and the total Chinese version of the Pittsburgh Sleep Quality Index (PSQI) score were significantly lower in the observation group than those in the control group (p < 0.05). Although the incidence rates of dehydration, electrolyte imbalance, diaper rash, perianal breakdown, and dyspnea were lower in the observation group than those in the control group, these differences did not reach statistical significance (p > 0.05). The proportion of children experiencing at least one adverse clinical outcome was compared between the observation group and the control group (p < 0.05).
Therapeutic play combined with emotional soothing care is associated with improved clinical outcomes, enhanced nutritional status, and better sleep quality in children with acute diarrhea, thereby facilitating overall recovery.
Keywords
- play therapy
- emotional adjustment
- acute diarrhea
- children
- clinical outcomes
- nutritional status
- sleep quality
- treatment outcome
Childhood diarrhea is a common clinical condition in pediatrics, primarily caused by the immature development of the child’s digestive system, relatively weak immune function, improper feeding practices, or bacterial infections [1, 2]. Affected children often present with increased frequency of bowel movements and alterations in stool consistency, which may be accompanied by symptoms such as fever and vomiting. In some severe cases, serious complications such as water-electrolyte imbalance and acidosis may occur, posing a significant threat to their life and health [3, 4]. Current clinical management primarily focuses on symptomatic pharmacological treatment. However, due to the young age of the children, low treatment compliance, and fear of medical procedures and unfamiliar environments, they often exhibit discomfort manifested by crying, restlessness, and resistance [5], especially when accompanied by vomiting or fever. Therefore, providing effective nursing interventions alongside pharmacological treatment is essential to enhance children’s cooperation, alleviate clinical symptoms, and promote recovery.
In recent years, with the continuous advancement of clinical research, nursing methods are no longer confined to routine procedures, and various humanized nursing models have gradually been implemented in pediatric practice. Therapeutic play, as an evidence-based psychosomatic intervention for children, promotes psychological and social adaptive development through developmentally appropriate and educational play. This approach not only enables children to acquire medical knowledge and coping skills but also reduces fear of unfamiliar environments by simulating medical scenarios, thereby improving emotional responses, enhancing treatment compliance, and optimizing the overall healthcare experience [6, 7]. Multiple studies have reported positive effects of this intervention across diverse pediatric populations: Suleiman-Martos et al. [8] reported that therapeutic play interventions can alleviate preoperative anxiety during anesthesia induction in children; Szturm et al. [9] found that such interventions can improve balance function and treatment engagement in children with cerebral palsy; Kokol et al. [10] showed that serious game-based interventions exert positive effects in reducing anxiety, regulating stress, and improving emotion recognition in children with developmental disabilities; Oh et al. [11] confirmed that these interventions can ameliorate hyperactivity and impulsivity symptoms in children with attention deficit hyperactivity disorder; Ren et al. [12] demonstrated that cognitive training based on therapeutic play significantly enhances core cognitive abilities in children with neurodevelopmental disorders and is feasible for remote implementation.
Emotional soothing intervention is a systematic psychological nursing strategy, the core of which lies in optimizing the child’s psychological state through the integration of multiple sensory and emotional support pathways [13, 14]. Children are particularly sensitive to sensory experiences. Thus, modifying the medical environment based on this characteristic can effectively alleviate anxiety in both children and their families [15]. Several studies provide empirical evidence for such interventions: DeCosta et al. [16] indicated that children aged 3–6 years with chronic illnesses require the establishment of a sense of security and autonomy, primarily achieved through participation in medical activities and positive interactions with healthcare staff; Corsano et al. [17], in a study of 27 children and adolescents admitted to a hematology-oncology ward, found that children expect healthcare staff to actively encourage and respond to their emotional needs; Diogo et al. [18] emphasized the critical role of promoting emotion management in pediatric nursing; Rennick et al. [19] investigated the use of soothing interventions such as touch, reading, and music in the Pediatric Intensive Care Unit (PICU), with findings suggesting good acceptability and feasibility, and demonstrating beneficial effects on sleep quality and child-parent anxiety indicators; Lerwick [20] proposed that healthcare professionals have unique advantages in recognizing and responding to children’s fear responses and can prevent iatrogenic trauma and anxiety through standardized emotional care; Boles et al. [21] indicated that soothing protocols based on tactile, auditory, and other sensory stimuli are safe and feasible for critically ill children.
At present, the systematic application of therapeutic play combined with emotional soothing care in the nursing management of children with acute diarrhea remains insufficiently explored. Therefore, this study aims to investigate the clinical value and effects of a combined nursing model incorporating therapeutic play and emotional soothing care in children with acute diarrhea, with particular emphasis on evaluating its impact on clinical symptoms, nutritional status, and sleep quality, thereby providing a more comprehensive and humanistic integrated nursing strategy for clinical practice.
This was a retrospective analysis. The study subjects comprised 148 children with acute diarrhea admitted to the Women and Children’s Hospital of Ningbo University between June 2023 and May 2025. For this retrospective study, baseline and clinical data of the 148 children were extracted from the electronic medical record system. All data were derived from routine clinical documentation, and no additional assessments were conducted beyond standard clinical practice. Data collection was performed by the study team through a structured review of electronic medical records after discharge. The participants were grouped based on the nursing method received: those receiving emotional soothing care were assigned to the control group (n = 78), whereas those receiving therapeutic play combined with emotional soothing care were assigned to the observation group (n = 70). A flow chart of participant selection and inclusion/exclusion criteria is presented in Fig. 1.
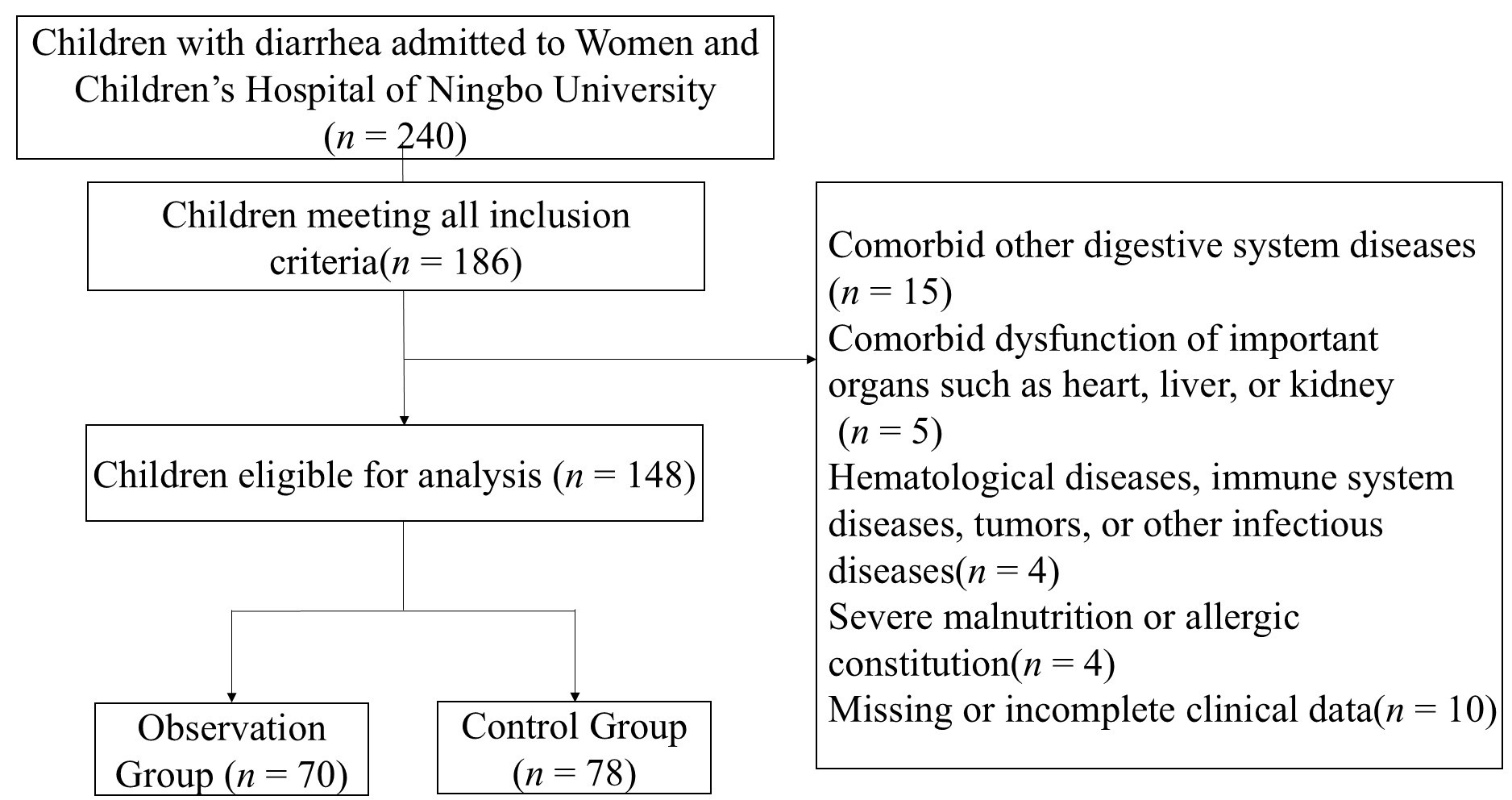 Fig. 1.
Fig. 1.
A flowchart of participant selection, including inclusion and exclusion criteria.
Inclusion criteria: (1) first-time treatment; (2) age 2–6 years; (3) disease
duration
Exclusion criteria: (1) comorbid digestive system diseases (e.g., digestive system malformations, dysentery, food poisoning); (2) comorbid dysfunction of important organs such as heart, liver, or kidney; (3) hematological diseases, immune system diseases, tumors, or other infectious diseases; (4) severe malnutrition or allergic constitution; (5) missing or incomplete clinical data.
This study employed a retrospective analytical design. Baseline and clinical data of the 148 children with acute diarrhea were extracted from the electronic medical record system, including age, gender, disease duration, ethnicity, etiology, degree of dehydration, diarrhea frequency, diarrhea cessation time (defined as the time from admission to the absence of loose or watery stools for a continuous 24-hour period), abdominal pain cessation time (defined as the time from admission to the absence of pain complaints or pain-related behaviors, with no guarding upon nurse inquiry, abdominal pressure, or palpation), fever resolution time (defined as the time from admission to when axillary temperature remained below 37.5 °C for more than 24 hours without antipyretics), and length of hospital stay. Discharge criteria were based on a comprehensive clinical assessment, including cessation or marked alleviation of diarrhea, resolution of fever when present, stable clinical outcomes, adequate oral intake for hydration, and parental competence in home care management.
The cessation of abdominal pain, diarrhea and fever resolution was determined based on a combination of parental report and nurse assessment. Nutritional status indicators included serum albumin (Alb), prealbumin (PA), and hemoglobin (Hb), Alb and PA were measured using an AU5800 fully automated hematology analyzer (Beckman Coulter, Brea, CA, USA), while Hb was measured using a fully automatic hematology analyzer (BC-6800, Mindray, Shenzhen, China), following standard laboratory procedures.
Sleep quality was assessed using the Chinese version of the Pittsburgh Sleep Quality Index (PSQI), which has been demonstrated to be reliable and valid for evaluating subjective sleep quality in Chinese child cancer survivors in Hong Kong [22]. The scale, developed by Buysse et al. in 1989 [23], comprises six dimensions: sleep quality, sleep latency, sleep duration, sleep efficiency, sleep disturbances, and daytime dysfunction (the “use of sleep medication” dimension was excluded due to the young age of the children). Each item is scored from 0 to 3, with higher total scores indicating poorer sleep quality. The PSQI assessments were administered to the children’s parents by trained research assistants through structured interviews. All assessors underwent standardized training, including review of the PSQI manual, scoring criteria, and role-playing exercises, to minimize interviewer bias and ensure inter-rater reliability.
The nutritional indicators (Alb, PA, Hb) and sleep quality (PSQI) were assessed at two time points: on the day of admission (pre-intervention) and on the day of discharge (post-intervention). Considering the short disease course and recovery period in children with acute diarrhea, the PSQI assessment period was adapted to reflect sleep quality during the previous night, to more accurately capture short-term changes in sleep during hospitalization.
Adverse clinical outcomes, including dehydration, electrolyte imbalance, diaper rash, perianal breakdown, and dyspnea, were diagnosed and recorded based on standard clinical criteria and physician assessments as documented in the electronic medical records.
Grouping: Children were retrospectively assigned to either the control or observation group based on nursing interventions documented in their medical records during hospitalization. The control group consisted of children who received emotional soothing care (incorporating routine care) as the standard nursing protocol on the ward. The observation group comprised children who, in addition to the emotional soothing care, received the therapeutic play intervention, as documented in the nursing records. The assignment was not randomized but reflected the actual nursing care delivered during the child’s hospital stay.
Control Group: Children received emotional soothing care incorporating routine care. This included regular nursing rounds and care tasks conducted 2–3 times per day (during day shifts), with each direct nursing contact lasting approximately 10–15 minutes. (1) Upon admission, a comprehensive condition assessment and clinical outcomes monitoring were performed promptly; intravenous access was established, and symptomatic supportive treatments such as fluid replacement, anti-infection, and antidiarrheal therapies were administered as prescribed. (2) During hospitalization, close observation and documentation of the child’s mental state, signs of dehydration, stool characteristics, and intake/output were conducted; regular perianal cleaning and care were provided to prevent diaper rash. (3) Emotional soothing care was implemented throughout hospitalization: nurses communicated with the child using a gentle and reassuring tone; with the child’s consent, gentle tactile contact (e.g., forehead, hands, shoulders, or back) was applied, and affirmation and praise were offered before and after procedures to enhance the child’s sense of security and trust. Families were instructed in directional abdominal massage; light-blocking curtains were used to create a conducive sleep environment, and caregivers were guided to facilitate falling asleep through storytelling or humming lullabies. During nighttime rounds, a quiet environment was maintained, disturbances were minimized, and continuous sleep duration was supported. (4) Individualized dietary guidance was provided based on feeding methods, such as adjusting the mother’s diet or transitioning to low-lactose formula, and caregivers were instructed on appropriate medication administration and home care practices. (5) Ward management was strengthened, visitation was limited, and education on disease prevention and management was provided. (6) Before discharge, the child’s recovery status was evaluated, and detailed instructions were given regarding dietary transition, hygiene practices, activity levels, and follow-up precautions.
Observation Group: In addition to emotional soothing care, children received a therapeutic play intervention. The intervention was conducted in a designated therapeutic play activity room, decorated in a child-friendly manner and equipped with sterilized toys, cartoon materials, books, and simple medical models (e.g., stethoscopes, syringe models) to create a relaxed and safe environment. The therapeutic play intervention included: (i) Adaptive play: within 24 hours of admission, game-based tasks such as “find the stethoscope” and “role-playing (e.g., ‘I am a little doctor’)” were used to help the child become familiar with the medical environment and reduce unfamiliarity and fear. (ii) Cognitive play: three-dimensional pathogen models and storytelling were used to explain the causes of diarrhea and the treatment process, thereby enhancing disease understanding. (iii) Operational play: dolls and medical models were used to simulate procedures such as venipuncture and medication administration, guiding the child to imitate and practice, thereby gradually reducing resistance to actual medical procedures. (iv) Cooperative and emotional regulation games: multiplayer cooperative games (e.g., “Handwashing Guardian”) and distracting activities such as building blocks and puzzles were provided to alleviate anxiety and promote emotional relaxation. The intervention frequency was twice daily (morning and afternoon), with each session lasting 20–30 minutes, continuing until discharge. During play sessions, nurses accompanied the children to ensure safety and adjusted the difficulty and duration according to age and clinical condition to prevent fatigue. Children who completed the sessions received rewards such as stickers or small toys to reinforce positive behaviors.
Quality Control: To ensure standardization and consistency of the intervention, multiple quality control measures were implemented. The intervention protocol was developed by a multidisciplinary team, including the head nurse, pediatric nursing staff, child life specialists, and psychotherapists, all with more than three years of pediatric clinical experience and relevant play therapy expertise. Before implementation, specialized training was conducted for participating nursing staff, covering psychological and behavioral developmental characteristics of children aged 2–6 years, emotional soothing techniques, and the impact of distress behavior on recovery. Standardized assessments were conducted to ensure procedural consistency. During implementation, the following measures were applied: (i) development of a detailed intervention manual specifying procedures, duration, and precautions for each activity; (ii) regular supervision and inspection by the head nurse to ensure compliance with standards for play environment setup, toy disinfection, and massage techniques; (iii) timely feedback on implementation challenges and adjustment of intervention strategies; (iv) collection of caregiver feedback to continuously optimize the intervention process. Regarding intervention adherence, among the 70 children in the observation group, 66 (94.29%) completed all planned therapeutic play sessions until discharge, while the remaining 4 children (5.71%) missed one or two sessions due to fatigue or acute discomfort; all participated in at least 80% of the total sessions.
SPSS version 23.0 (IBM SPSS Corp.; Armonk, NY, USA) was used for statistical
analysis. Categorical variables were expressed as frequency and percentage [n (%)]
and compared using the Pearson chi-square test, continuity-corrected chi-square
test, or Fisher’s exact test, as appropriate. Continuous variables were assessed
for normality using the Shapiro-Wilk test. Data conforming to a normal
distribution were expressed as mean
There were no statistically significant differences in age, gender, disease
duration, ethnicity, etiology, degree of dehydration, or diarrhea frequency
between the two groups (p
| Variable | Observation group | Control group | p-value | ||
| (n = 70) | (n = 78) | ||||
| Age (years) | 4.00 (3.00, 5.00) | 4.00 (3.00, 5.00) | –0.788 | 0.431 | |
| Gender [n (%)] | 0.538 | 0.463 | |||
| Male | 38 (54.29) | 47 (60.26) | |||
| Female | 32 (45.71) | 31 (39.74) | |||
| Disease duration (h) | 40.5 (29.75, 50.00) | 41.5 (31.50, 52.25) | –0.523 | 0.601 | |
| Ethnicity [n (%)] | 0.000 | 1.000 | |||
| Han | 68 (97.14) | 75 (96.15) | |||
| Other | 2 (2.86) | 3 (3.85) | |||
| Etiology [n (%)] | 0.867 | 0.973 | |||
| Rotavirus | 18 (25.71) | 20 (25.64) | |||
| Norovirus | 17 (24.29) | 17 (21.79) | |||
| Salmonella | 15 (21.43) | 17 (21.79) | |||
| Enterococcus | 10 (14.29) | 15 (19.23) | |||
| Staphylococcus aureus | 8 (11.43) | 7 (8.97) | |||
| Indigestion/Other | 2 (2.86) | 2 (2.56) | |||
| Degree of dehydration [n (%)] | 1.989 | 0.370 | |||
| None | 33 (47.14) | 30 (38.46) | |||
| Mild | 14 (20.00) | 23 (29.49) | |||
| Moderate | 23 (32.86) | 25 (32.05) | |||
| Diarrhea Frequency (times/day) | 6.00 (5.00, 8.00) | 6.00 (5.00, 7.00) | –0.499 | 0.618 | |
The diarrhea cessation time, abdominal pain cessation time, and length of
hospital stay in the observation group were shorter than those in the control
group, with statistically significant differences (p
| Variable | Observation group | Control group | Z | p-value |
| (n = 70) | (n = 78) | |||
| Diarrhea cessation time | 3.00 (2.00, 4.00) | 4.50 (3.00, 6.00) | –4.978 | |
| Abdominal pain cessation time | 2.00 (1.00, 3.00) | 3.00 (2.00, 4.00) | –3.268 | 0.001 |
| Fever resolution time | 2.00 (1.00, 2.00) | 2.00 (1.00, 3.00) | –1.493 | 0.135 |
| Length of hospital stay | 2.00 (1.75, 3.00) | 3.00 (2.00, 4.00) | –2.557 | 0.011 |
In the viral etiology subgroup (n = 72), the observation group showed
significantly shorter diarrhea cessation time, abdominal pain cessation time, and
length of hospital stay compared with the control group (p
| Variable | Observation group | Control group | Z | p-value |
| (n = 35) | (n = 37) | |||
| Diarrhea cessation time | 3.00 (1.00, 4.00) | 5.00 (3.00, 6.00) | –3.657 | |
| Abdominal pain cessation time | 2.00 (1.00, 3.00) | 3.00 (1.50, 4.00) | –2.481 | 0.013 |
| Fever resolution time | 2.00 (1.00, 2.00) | 2.00 (1.00, 3.00) | –0.575 | 0.565 |
| Length of hospital stay | 3.00 (2.00, 4.00) | 4.00 (3.00, 5.00) | –2.608 | 0.009 |
In the bacterial etiology subgroup (n = 72), the observation group also
demonstrated significantly shorter diarrhea and abdominal pain cessation times
(p
| Variable | Observation group | Control group | Z | p-value |
| (n = 33) | (n = 39) | |||
| Diarrhea cessation time | 3.00 (2.00, 4.00) | 4.00 (3.00, 6.00) | –3.154 | 0.002 |
| Abdominal pain cessation time | 2.00 (1.00, 3.00) | 3.00 (2.00, 4.00) | –2.137 | 0.033 |
| Fever resolution time | 2.00 (1.00, 2.00) | 2.00 (1.00, 3.00) | –1.414 | 0.157 |
| Length of hospital stay | 2.00 (1.00, 3.00) | 2.00 (1.00, 3.00) | –1.649 | 0.099 |
Before the intervention, there were no statistically significant differences in
serum Alb, PA, and Hb levels between the two groups (p
| Variable | Time point | Observation group | Control group | t | p-value |
| (n = 70) | (n = 78) | ||||
| Alb (g/L) | Pre-intervention | 25.25 |
25.86 |
–0.820 | 0.414 |
| Post-intervention | 33.62 |
31.45 |
3.223 | 0.002 | |
| PA (mg/L) | Pre-intervention | 176.43 |
175.85 |
0.209 | 0.834 |
| Post-intervention | 209.14 |
194.96 |
5.099 | ||
| Hb (g/L) | Pre-intervention | 82.73 |
84.41 |
–1.335 | 0.184 |
| Post-intervention | 96.80 |
92.18 |
3.996 |
Note: Alb, albumin; PA, prealbumin; Hb, hemoglobin; SD, standard deviation.
“*” indicates a statistically significant difference between pre-intervention
(day of admission) and post-intervention (day of discharge) within the same group
(p
Before the intervention, there were no statistically significant differences in
the scores for sleep quality, sleep latency, sleep duration, sleep efficiency,
sleep disturbances, daytime dysfunction, and the overall modified PSQI score
between the two groups (p
| Variable | Time point | Observation group | Control group | Z | p-value |
| (n = 70) | (n = 78) | ||||
| Sleep quality | Pre-intervention | 2.00 (2.00, 3.00) | 2.00 (2.00, 3.00) | –0.319 | 0.749 |
| Post-intervention | 1.00 (1.00, 1.00) * | 2.00 (1.00, 2.00) * | –6.678 | ||
| Sleep latency | Pre-intervention | 2.00 (1.00, 3.00) | 2.00 (2.00, 3.00) | –0.511 | 0.610 |
| Post-intervention | 1.00 (0.00, 2.00) * | 1.00 (1.00, 2.00) * | –3.174 | 0.002 | |
| Sleep duration | Pre-intervention | 2.00 (1.00, 3.00) | 2.00 (2.00, 3.00) | –0.629 | 0.530 |
| Post-intervention | 1.00 (1.00, 2.00) * | 1.00 (1.00, 2.00) * | –2.901 | 0.004 | |
| Sleep efficiency | Pre-intervention | 2.00 (2.00, 3.00) | 3.00 (2.00, 3.00) | –0.876 | 0.381 |
| Post-intervention | 1.00 (1.00, 1.00) * | 1.00 (1.00, 2.00) * | –3.412 | 0.001 | |
| Sleep disturbances | Pre-intervention | 2.00 (2.00, 2.25) | 2.00 (2.00, 2.25) | –0.178 | 0.859 |
| Post-intervention | 1.00 (1.00, 2.00) * | 2.00 (1.00, 2.00) * | –2.793 | 0.005 | |
| Daytime dysfunction | Pre-intervention | 2.00 (2.00, 3.00) | 2.00 (2.00, 3.00) | –0.738 | 0.461 |
| Post-intervention | 1.00 (1.00, 1.00) * | 1.00 (1.00, 2.00) * | –5.079 | ||
| Total score | Pre-intervention | 15.00 (13.00, 16.00) | 14.00 (14.00, 16.25) | –0.911 | 0.362 |
| Post-intervention | 7.00 (7.00, 8.00) * | 10.00 (9.00, 11.00) * | –8.725 |
Note: PSQI, Pittsburgh Sleep Quality Index. “*” indicates a statistically
significant difference between pre-intervention (day of admission) and
post-intervention (day of discharge) within the same group (p
The incidence rates of dehydration, electrolyte imbalance, diaper rash, perianal
breakdown, and dyspnea in the observation group were lower than those in the
control group. However, the differences between the two groups were not
statistically significant (p
| Variable | Observation group | Control group | p-value | |
| (n = 70) | (n = 78) | |||
| Dehydration | 1 (1.43) | 3 (3.85) | 0.158 | 0.691 |
| Electrolyte imbalance | 2 (2.86) | 5 (6.41) | 0.395 | 0.529 |
| Diaper rash | 1 (1.43) | 4 (5.13) | 0.621 | 0.431 |
| Perianal breakdown | 0 (0.00) | 2 (2.56) | Fisher | 0.498 |
| Dyspnea | 0 (0.00) | 1 (1.28) | Fisher | 1.000 |
| Children with at least one adverse clinical outcome | 4 (5.71) | 15 (19.23) | 6.023 | 0.014 |
Note: The row “Children with at least one adverse clinical outcome” indicates the number and proportion of children who experienced one or more adverse events during hospitalization. As individual children may experience multiple events, the sum of individual event frequencies may exceed this number.
The results of this study indicate that children in the observation group who received therapeutic play combined with emotional soothing care demonstrated significant advantages across multiple clinical indicators, including shorter diarrhea cessation time, abdominal pain cessation time, and length of hospital stay compared with the control group; improved post-intervention nutritional status indicators (Alb, PA, Hb); and significantly lower scores across all sleep quality dimensions and the overall PSQI score. Furthermore, the overall incidence of adverse clinical outcomes in the observation group was lower than that in the control group. Although no statistically significant differences were observed in fever resolution time or in the incidence rates of specific adverse clinical outcomes between the two groups, the overall findings suggest that this combined nursing model promotes recovery, improves nutritional status, and enhances sleep quality in children with acute diarrhea.
In conventional pediatric nursing practice, children’s emotional states are often underemphasized, which may lead to resistant behaviors such as crying and refusal, thereby interfering with the effective implementation of nursing procedures and potentially prolonging recovery time [18]. The findings of this study show that diarrhea cessation time, abdominal pain disappearance time, and length of hospital stay in the observation group were shorter than those in the control group, indicating that the integration of therapeutic play with emotional soothing care can further enhance clinical treatment efficacy in children with diarrhea. This effect may be associated with improvements in children’s self-regulation capacity mediated by the intervention. The potential mechanisms underlying these effects can be interpreted from both physiological and psychological perspectives.
At the physiological level, directed abdominal massage may facilitate coordinated colonic peristalsis through gentle stimulation of the intestinal wall plexus, promote the expulsion of pathogens and toxins, and alleviate discomfort associated with intestinal spasms, thereby contributing to direct physiological regulation. Huang et al. [24] reported in animal studies that abdominal massage can alleviate diarrhea symptoms in immature rats by modulating intestinal microbiota composition and tight junction protein expression. Wang et al. [25] also demonstrated that abdominal massage can reduce the incidence of gastric retention in patients receiving enteral nutrition and significantly decrease gastrointestinal complications such as diarrhea.
At the psychological level, therapeutic play interventions, including role-playing and interaction with medical props, combined with emotional soothing strategies, can effectively alleviate fear, anxiety, and stress responses in children. This may attenuate the release of stress-related hormones such as catecholamines, thereby mitigating their inhibitory effects on gastrointestinal function and facilitating more effective neuro-regulation of intestinal motility. Therefore, integrating interventions targeting both physiological and psychological domains, in addition to routine care, may exert synergistic effects on symptom resolution of intestinal function in children with diarrhea.
Notably, across different etiological subgroups (viral and bacterial), a reduction in the time to symptom relief, including cessation of diarrhea and abdominal pain, was consistently observed in the intervention group. This consistency further supports the value of therapeutic play as an adjunctive nursing intervention. However, within the bacterial subgroup, no statistically significant difference in length of hospital stay was observed between the intervention and control groups. A plausible explanation is that bacterial diarrhea often responds rapidly to targeted antibiotic therapy, resulting in a relatively shorter and less variable duration of hospitalization, thereby potentially attenuating the observable effect of the nursing intervention on this outcome.
As a consumptive disease, diarrhea often leads to deterioration of the child’s nutritional status due to impaired intestinal absorption, reduced appetite, and excessive nutrient loss [26]. As core indicators for assessing the body’s protein nutritional status, serum Alb and PA can dynamically reflect nutritional reserves and metabolic status, while Hb level is directly associated with the degree of anemia and tissue oxygen delivery capacity. Together, these three parameters constitute key biomarkers for evaluating the child’s nutritional and metabolic status [27, 28]. The findings of this study demonstrate that, following the intervention, the levels of Alb, PA, and Hb in the observation group were significantly higher than those in the control group. However, this finding warrants cautious interpretation. Based on clinical considerations, short-term improvements in serum albumin and hemoglobin levels in children recovering from acute diarrhea are largely influenced by two major non-nursing factors: first, correction of dehydration after admission, which alleviates hemoconcentration; and second, effective anti-infection treatment, which suppresses inflammation, reduces catabolic activity, and facilitates restoration of anabolic processes. Therefore, the observed improvements cannot be solely attributed to nursing interventions.
Nevertheless, although these dominant non-nursing factors are acknowledged, the comprehensive nursing model implemented in this study may have exerted an adjunctive effect. Therapeutic play and emotional soothing interventions (e.g., tactile comfort, verbal encouragement, and play-based distraction) may, by alleviating negative emotional states such as anxiety and fear, improve appetite and gastrointestinal function. Directed abdominal massage may further support nutrient absorption by promoting intestinal peristalsis. Furthermore, improved sleep quality plays a regulatory role in growth hormone secretion and protein synthesis, thereby contributing indirectly to nutritional recovery. Çamlıbel and Tokatlı Demirok [29] demonstrated that nutrition education delivered through board games can effectively improve dietary intake behaviors in primary school children and enhance self-efficacy and health-related attitudes. Similarly, a randomized controlled trial by Ghadam et al. [30] showed that a digital game-based nutrition education model significantly improved dietary knowledge and behavioral adherence among adolescent girls, accompanied by a significant increase in hemoglobin levels. These findings provide converging evidence supporting the application of gamified interventions in nutrition-related health promotion.
Clinical manifestations such as abdominal pain and frequent bowel movements associated with gastrointestinal disorders often disrupt sleep in children. Impaired sleep quality may, in turn, compromise immune competence and repair functions, thereby delaying recovery and creating a detrimental feedback cycle [31, 32]. In the present study, post-intervention modified PSQI dimension scores and total scores in the observation group were lower than those in the control group, indicating a more significant improvement in sleep quality. The mechanism underlying this effect may involve two principal pathways. First, optimizing the sleep environment (e.g., using blackout curtains and noise-reduction measures) combined with structured bedtime routines (e.g., storytelling and humming lullabies) and gentle sensory interaction enhances the child’s sense of security, reduces nocturnal distress, and facilitates sleep onset. Second, through the desensitizing effect of therapeutic play, medical procedures such as injections and medication administration are reframed as predictable, controllable play scenarios, thereby alleviating fear and anxiety related to medical care. The combined implementation of these strategies may reduce nocturnal awakenings and sleep latency, thereby improving overall sleep quality.
Notably, this study represents one of the earliest applications of therapeutic play combined with emotional soothing care for sleep management in children with acute diarrhea, thereby providing a novel integrative intervention framework. It should also be emphasized that, in this study, the PSQI scale was adapted for pediatric patients. Specifically, the “use of hypnotic medication” dimension was excluded to align with the age characteristics of the study population, and the assessment period was shortened to “the previous night” to reflect the acute and short-term nature of diarrheal episodes and hospitalization. These modifications were intended to enhance the sensitivity and feasibility of sleep assessment in this clinical context. However, these adaptations limit direct comparability with previous pediatric studies that employed the full PSQI with a one-week recall period. Future investigations should consider this methodological variation when interpreting or comparing findings across studies.
This study has several limitations. First, as a single-center retrospective study, it is susceptible to selection bias and information bias. Participants were not randomly assigned to groups or prospectively selected. Such non-randomization may introduce selection bias. For instance, children with more severe illness may have been less likely to receive the intervention or to be included, which could confound the results. In addition, blinding of healthcare providers and outcome assessors to group allocation was not feasible in this behavioral intervention. In the absence of blinding, detection bias cannot be excluded; clinical decisions, such as discharge timing, may have been influenced by awareness of the intervention received, potentially favoring earlier discharge in the observation group. Second, the intervention population was limited to children aged 2–6 years, excluding infants younger than 2 years. The generalizability of the findings to a wider pediatric age range, therefore, requires further validation. Additionally, although all nursing staff underwent standardized training and assessment, factors such as workload, acceptance of the intervention protocol, and compliance during implementation may still have influenced the nursing outcomes.
Finally, although the comparability of the two groups in terms of baseline characteristics, underlying etiology, and treatment provides partial support for the observed effects, the inherent limitations of a retrospective design indicate residual confounding factors may remain. Furthermore, the relatively poor baseline nutritional indicators observed in the study population reflect the common clinical profile of hospitalized pediatric patients with acute diarrhea, which may limit the generalizability of the findings to outpatient children with milder disease. Future studies should adopt multicenter, large-sample prospective randomized controlled designs, expand the age range of participants, and include more diverse populations to enhance the robustness and external validity of the conclusions. Simultaneously, continuous training and quality supervision of nursing staff should be strengthened to minimize variability related to human factors.
Therapeutic play combined with emotional soothing care is associated with improvements in clinical symptoms, enhanced nutritional status, and improved sleep quality in children with acute diarrhea, thereby facilitating overall recovery. This study provides novel insights for clinical practice by supporting the implementation of systematic nursing strategies centered on children’s emotional and cognitive development.
• Therapeutic play combined with emotional soothing care is associated with shorter duration of clinical symptoms in children with acute diarrhea.
• Therapeutic play combined with emotional soothing care is associated with improved nutritional status indicators in children with acute diarrhea.
• Therapeutic play combined with emotional soothing care is associated with enhanced sleep quality in children with acute diarrhea.
• Therapeutic play combined with emotional soothing care does not increase the risk of adverse clinical outcomes in children with acute diarrhea.
All data included in this study are available from the corresponding author upon reasonable request.
All aspects of the study and subsequent write-up were conducted by the author [YH]. The author read and approved the final manuscript. The author has participated sufficiently in the work and agreed to be accountable for all aspects of the work.
This study protocol adhered to the ethical principles of the Declaration of Helsinki and was reviewed and approved by the Ethics Committee of the Women and Children’s Hospital of Ningbo University (Approval No.: NBFE-2025-KY-185). The families of all participating children were fully informed about the study and provided written informed consent.
Not applicable.
This research received no external funding.
The author declares no conflicts of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.