



1 Department of Electrocardiographic Diagnosis, Zibo Central Hospital, 255000 Zibo, Shandong, China
2 Department of Internal Medicine, Zibo Central Hospital, 255000 Zibo, Shandong, China
Abstract
Cardiac arrhythmias are common in high-risk populations, often presenting paroxysmally and asymptomatically, leading to missed diagnoses and increased cardiovascular risks. This study aimed to retrospectively analyze the clinical value of high-channel 12-lead Holter electrocardiogram (ECG) in the early identification of arrhythmias in high-risk populations and to provide a reference for cardiovascular risk prevention and control in these groups.
Clinical data from 300 patients who met the criteria for high-risk populations and received diagnosis and treatment in Zibo Central Hospital from August 2023 to June 2024 were retrospectively collected. All patients underwent both routine 12-lead ECG examination and high-channel 12-lead Holter monitoring during the same period. The detection rates of atrial fibrillation, frequent ventricular premature beats (≥30 beats/h), frequent atrial premature beats (≥100 beats/24 h), and atrioventricular block were compared between the two modalities using appropriate statistical tests. Univariate logistic regression was performed to identify factors associated with positive arrhythmia detection.
The overall arrhythmia detection rate of the high-channel 12-lead Holter (35.0%) was significantly higher than that of the routine 12-lead ECG (20.0%) (p < 0.001). The Holter showed significant advantages in detecting atrial fibrillation (11.7% vs 6.0%, p < 0.001) and frequent ventricular premature beats (14.3% vs 7.7%, p < 0.001). Univariate logistic regression revealed that smoking history, drinking history, hypertension, coronary heart disease, heart failure, higher body mass index (BMI) and type 2 diabetes mellitus were significantly associated with positive arrhythmia detection by Holter (all p < 0.001). Similar patterns were observed for routine ECG, except for diabetes and BMI.
In high-risk populations, the high-channel 12-lead Holter is highly valuable for screening paroxysmal and intermittent arrhythmias (especially atrial fibrillation and frequent ventricular premature beats). It can serve as an effective supplement to the routine ECG, providing a key basis for the early and accurate detection and intervention of arrhythmias in high-risk groups.
Keywords
- ambulatory electrocardiography
- cardiac arrhythmia
- clinical factors
- retrospective studies
Arrhythmia is a common cardiovascular disorder characterized by abnormalities or
disruptions in the normal electrical activation or contraction sequence of the
heart. It is characterized by irregular heart rhythms, which can manifest as
bradycardia (heart rate
Currently, therapeutic and management strategies for arrhythmias include antiarrhythmic drugs, pacemakers, automated external defibrillators (AEDs), and radiofrequency ablation [4]. However, arrhythmias in high-risk populations (e.g., patients with hypertension, coronary heart disease, or the elderly) often occur paroxysmally and asymptomatically, making them highly prone to missed diagnosis via routine electrocardiogram (ECG). Therefore, early and accurate identification of such arrhythmias is crucial for improving patient prognosis [5].
Routine 12-lead ECG, with its short monitoring duration (only a few minutes), frequently fails to capture abnormal ECG signals, leading to missed diagnoses, delayed treatment, and increased risks of adverse cardiovascular events such as stroke and heart failure [6]. Although traditional Holter monitors enable 24-hour recording, their limited number of channels results in insufficient integrity and accuracy of signal acquisition, which cannot meet the needs of detecting early, subtle arrhythmias [7, 8].
High-channel 12-lead Holter ECG represents an advanced form of dynamic cardiac monitoring. It integrates the continuous recording capability of traditional monitors with the comprehensive spatial information provided by standard 12-lead ECG. Through optimized channel design, it can continuously collect more comprehensive dynamic ECG data over 24 hours, theoretically improving the detection rate of early arrhythmias [9]. Compared with modern devices like adhesive patch monitors, Holter systems offer superior multi-lead resolution for complex arrhythmias [10]. In this study, we retrospectively analyzed two types of ECG data from 300 high-risk individuals, compared the detection performance between the high-channel 12-lead Holter and routine 12-lead ECG, and further verified the clinical value of high-channel 12-lead Holter in the early identification of arrhythmias, aiming to provide practical evidence for cardiovascular management in high-risk populations.
High-risk individuals who attended the Department of Cardiovascular Medicine and Department of Geriatrics in Zibo Central Hospital from August 2023 to June 2024 were retrospectively selected as study subjects. Case data were extracted from the hospital’s electronic medical record system, ECG database, and clinical diagnosis and treatment records. After screening, a total of 300 eligible cases were finally included (Fig. 1). The inclusion and exclusion criteria of this study are as follows:
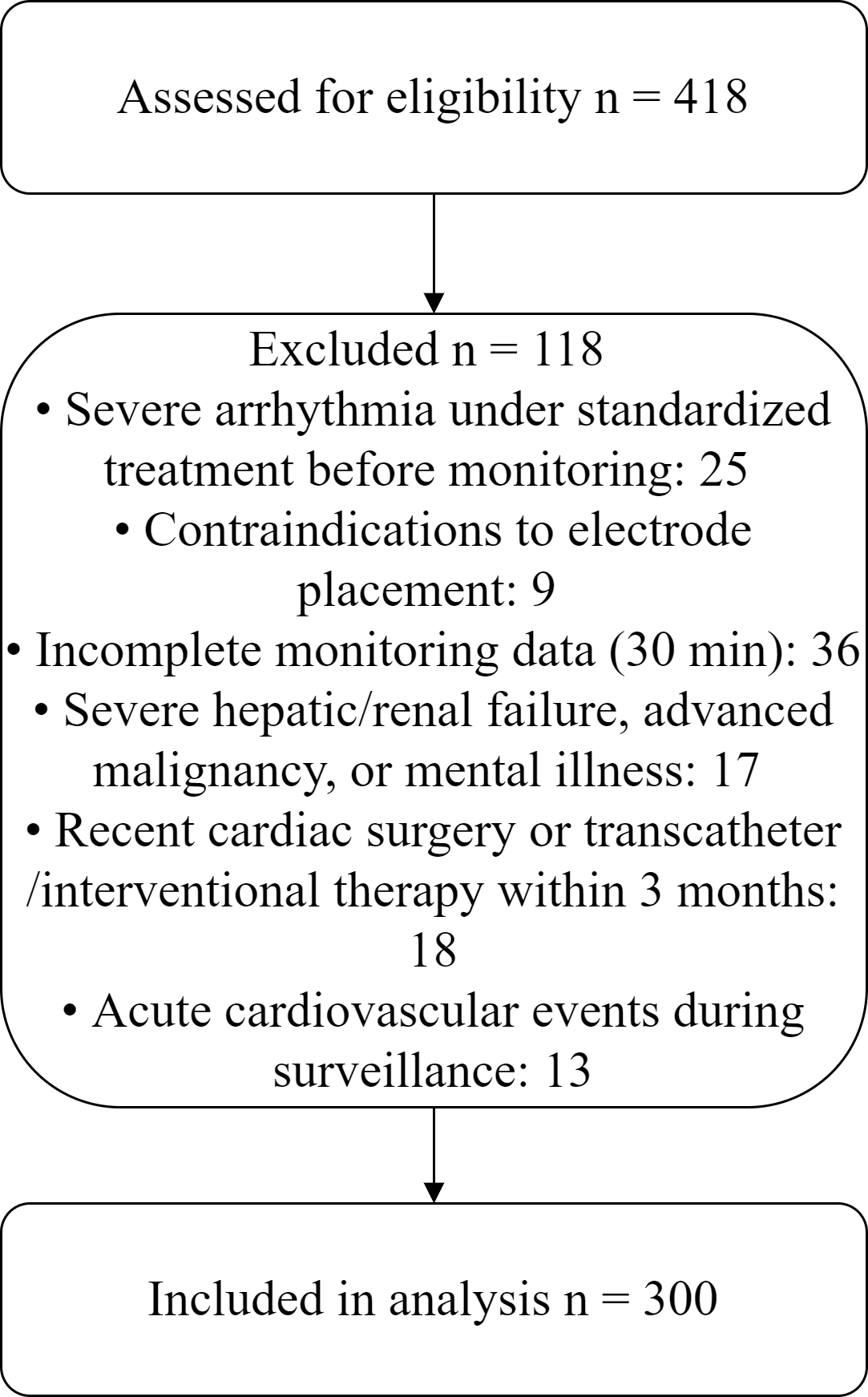 Fig. 1.
Fig. 1.
Flowchart of patient selection.
(1) Meeting the definition of “high-risk population for arrhythmia” with at
least one of the following risk factors: ① hypertension (systolic blood
pressure
(2) Completion of both routine 12-lead ECG examination and high-channel 12-lead Holter monitoring within 1 week after enrollment.
(3) Complete medical records, including baseline demographic characteristics, diagnosis and treatment records of underlying diseases, and original reports and interpretation results of both ECG tests.
(4) Age
(1) Confirmed diagnosis of severe arrhythmia with standardized treatment before monitoring.
(2) Contraindications to electrode placement.
(3) Incomplete ECG monitoring data (Holter monitoring duration
(4) Comorbidity with severe hepatic or renal failure, advanced malignant tumors, or mental disorders resulting in inability to cooperate with diagnosis, treatment, or follow-up.
(5) Recent cardiac surgery or transcatheter/interventional therapy within the past 3 months.
(6) Occurrence of acute cardiovascular events during surveillance.
A GE MAC 5500 12-lead ECG machine (General Electric Company, USA) was used. Before the examination, patients were instructed to lie quietly in the supine position for 5 minutes and to remove metal objects from the chest and abdomen. Limb leads (Ⅰ, Ⅱ, Ⅲ, aVR, aVL, aVF) and precordial leads (V1–V6) were placed in accordance with international standards. The recording duration was adjusted flexibly based on patients’ clinical symptoms: for asymptomatic patients, continuous ECG signals were recorded for 30 seconds at a paper speed of 25 mm/s and a gain of 10 mm/mV; for patients with suspected symptoms such as palpitations and chest tightness, the recording duration was extended to 1–2 minutes, focusing on observing signal changes in leads II and V1.
The examination results were independently interpreted by 2 associate chief physicians with more than 5 years of experience in ECG interpretation, using a blinded method in which each was unaware of the other’s findings or the patient’s Holter results. Disagreements were resolved through discussion or consultation with a third senior physician. The core diagnostic criteria followed domestic authoritative consensus and ECG diagnostic principles [11, 12], with a key focus on identifying the following arrhythmias:
• Atrial fibrillation: disappearance of P waves, replaced by f waves, and absolutely irregular RR intervals;
• Ventricular premature beats: prematurely appearing wide and deformed QRS complexes with complete compensatory pauses;
• Atrial premature beats: prematurely appearing ectopic P waves with incomplete compensatory pauses;
• Atrioventricular block: Grade Ⅰ, PR interval
A BeneHeart R12 high-channel 12-lead Holter recorder (Mindray, Shenzhen, China)
was used, with the supporting analysis software BeneHeart Holter Analysis System
(version 5.0, Mindray Bio-Medical Electronics Co., Ltd., Shenzhen, China).
Before monitoring, the patient’s chest and abdominal skin were cleaned, and
silver-chloride electrode pads were attached in accordance with the standard for
the routine 12-lead ECG, ensuring the contact impedance between electrodes and
skin was
After monitoring was completed, the recorder was connected to a computer to import 24-hour continuous ECG data (sampling frequency: 500 Hz; time resolution: 1 ms). The same 2 associate chief physicians performed offline analysis using a blinded method: after the automatic analysis software initially identified abnormal ECG events, the physicians independently checked the original waveforms one by one, corrected software misjudgments (e.g., excluding false positives caused by myoelectric interference and baseline drift), and finally confirmed the type of arrhythmia, episode frequency, duration, and correlation with symptoms. They were unaware of each other’s interpretations or prior routine ECG results to minimize bias.
Two researchers independently extracted data from the electronic medical record system. The extracted content included: (1) baseline data (sex, age, body mass index [BMI], smoking history, drinking history, type of underlying disease); and (2) ECG test data (reports from the routine 12-lead ECG examination, including examination time, type of arrhythmia, and interpretation results, and from the high-channel 12-lead Holter monitoring, including monitoring time, type of arrhythmia, episode frequency, duration, and symptom correlation records). After extraction, the two researchers cross-checked the data. In case of discrepancies, the final results were confirmed by reviewing original test images (waveforms stored in the ECG machine and Holter analyzer) and consulting clinical physicians to ensure data accuracy.
The detection rates of target arrhythmias by the two test methods included:
① Atrial fibrillation (paroxysmal or persistent; duration
② Frequent ventricular premature beats (
③ Frequent atrial premature beats (
④ Atrioventricular block (Grade Ⅰ, Ⅱ, or Ⅲ, according to the above interpretation criteria).
Continuous variables were expressed as median (1st Quartile [Q1], 3rd
Quartile [Q3]) if non-normally distributed (determined by
Kolmogorov–Smirnov test), and categorical variables were expressed as frequency
(n) and percentage (%). A paired design was adopted to compare the detection
rates of arrhythmias (overall and by subtype: atrial fibrillation, frequent
ventricular premature beats, frequent atrial premature beats, and
atrioventricular block) between the two methods. Paired analyses were performed
on the results of the routine 12-lead ECG examination and 24-hour Holter
monitoring from each patient. Based on the overall and subtype-specific detection
data, the number of cases with both positive, only routine ECG positive, only
Holter positive, and both negative results were calculated. The McNemar test
(paired chi-square test) was used to compare detection rate differences between
the two methods; when the expected frequency was
A total of 300 high-risk individuals with cardiovascular conditions were included in this study. Baseline characteristics showed that the study population was mainly elderly (median age: 67.00 years), with a body mass index (BMI) within the normal range (median: 23.60 kg/m2). Participants commonly had multiple cardiovascular comorbidities, including coronary heart disease, hypertension, type 2 diabetes mellitus, and heart failure, as well as risk factors such as smoking and alcohol consumption. These subjects met the inclusion criteria for a high-risk cardiovascular population, providing a representative study cohort for the subsequent comparison of the efficacy between the two ECG detection methods (Table 1).
| Variables | Total (n = 300) | |
| Age (years), M (Q1, Q3) | 67.00 (58.00, 76.00) | |
| Body mass index (BMI) (kg/m2), M (Q1, Q3) | 23.60 (21.60, 25.40) | |
| Sex, n (%) | ||
| Male | 168 (56.00) | |
| Female | 132 (44.00) | |
| Smoking history, n (%) | 104 (34.67) | |
| Drinking history, n (%) | 108 (36.00) | |
| Hypertension, n (%) | 126 (42.00) | |
| Coronary heart disease, n (%) | 84 (28.00) | |
| Type 2 diabetes mellitus, n (%) | 72 (24.00) | |
| Heart failure, n (%) | 48 (16.00) | |
Note: M, median; Q1, 1st Quartile; Q3, 3rd Quartile.
According to Table 2, the total arrhythmia detection rate of the high-channel
12-lead Holter was significantly higher than that of the routine 12-lead ECG
(35.0% vs 20.0%, p
| Indicator | Routine ECG positive, n (%) | Holter positive, n (%) | Both positive, n | Only routine ECG positive, n | Only Holter positive, n | p | |
| Total detection | 60 (20.0%) | 105 (35.0%) | 45 | 15 | 60 | 25.81 | |
| Atrial fibrillation | 18 (6.0%) | 35 (11.7%) | 15 | 3 | 20 | - | |
| Frequent ventricular premature beats | 23 (7.7%) | 43 (14.3%) | 18 | 5 | 25 | 12.03 | |
| Frequent atrial premature beats | 14 (4.7%) | 20 (6.7%) | 8 | 6 | 12 | - | 0.238 |
| Atrioventricular block | 5 (1.7%) | 7 (2.3%) | 4 | 1 | 3 | - | 0.625 |
Note:
To further clarify the detection advantages of Holter monitoring for different arrhythmia subtypes, in-depth analyses were conducted on atrial fibrillation and frequent ventricular premature beat subtypes, and their specific detection distributions are shown in Tables 3,4.
| Holter - Atrial Fibrillation = Positive | Holter - Atrial Fibrillation = Negative | Total | |
| Routine ECG - Atrial Fibrillation = Positive | 15 | 3 | 18 |
| Routine ECG - Atrial Fibrillation = Negative | 20 | 262 | 282 |
| Total | 35 | 265 | 300 |
| Holter - Frequent Ventricular Premature Beats = Positive | Holter - Frequent Ventricular Premature Beats = Negative | Total | |
| Routine ECG - Frequent Ventricular Premature Beats = Positive | 18 | 5 | 23 |
| Routine ECG - Frequent Ventricular Premature Beats = Negative | 25 | 252 | 277 |
| Total | 43 | 257 | 300 |
As shown in Table 3, Holter monitoring detected a total of 35 cases of atrial
fibrillation, among which 20 cases were Holter-positive only, while routine
electrocardiography detected only 3 cases of “routine ECG-only positive” atrial
fibrillation (p
As shown in Table 4, Holter monitoring detected 43 cases of frequent ventricular
premature beats, among which 25 were “Holter-only positive”—a number
significantly higher than the 5 “routine ECG-only positive” cases identified by
routine ECG (p
To explore the associations between baseline characteristics and positive
arrhythmia detection using the two methods, univariate logistic regression was
performed (Table 5). For routine ECG positive detection, significant predictors
included smoking history (p
| Variables | Routine ECG Positive | Holter Positive | |||||||||
| SE | Z | p | OR (95% CI) | SE | Z | p | OR (95% CI) | ||||
| Sex | |||||||||||
| Female | 1.00 (Reference) | 1.00 (Reference) | |||||||||
| Male | –0.30 | 0.29 | –1.04 | 0.296 | 0.74 (0.42~1.30) | 0.01 | 0.24 | 0.05 | 0.961 | 1.01 (0.63~1.63) | |
| Smoking history | |||||||||||
| No | 1.00 (Reference) | 1.00 (Reference) | |||||||||
| Yes | 2.33 | 0.34 | 6.85 | 10.31 (5.29~20.09) | 1.59 | 0.26 | 6.05 | 4.90 (2.93~8.20) | |||
| Drinking history | |||||||||||
| No | 1.00 (Reference) | 1.00 (Reference) | |||||||||
| Yes | 1.62 | 0.31 | 5.25 | 5.06 (2.76~9.27) | 1.54 | 0.26 | 5.92 | 4.67 (2.80~7.78) | |||
| Hypertension | |||||||||||
| No | 1.00 (Reference) | 1.00 (Reference) | |||||||||
| Yes | 1.47 | 0.31 | 4.69 | 4.33 (2.35~8.00) | 1.81 | 0.27 | 6.80 | 6.11 (3.63~10.30) | |||
| Coronary heart disease | |||||||||||
| No | 1.00 (Reference) | 1.00 (Reference) | |||||||||
| Yes | 1.33 | 0.30 | 4.40 | 3.77 (2.09~6.81) | 1.17 | 0.27 | 4.38 | 3.22 (1.91~5.44) | |||
| Type 2 diabetes mellitus | |||||||||||
| No | 1.00 (Reference) | 1.00 (Reference) | |||||||||
| Yes | –0.05 | 0.34 | –0.14 | 0.892 | 0.96 (0.49~1.86) | 1.54 | 0.29 | 5.38 | 4.67 (2.66~8.18) | ||
| Heart failure | |||||||||||
| No | 1.00 (Reference) | 1.00 (Reference) | |||||||||
| Yes | 2.03 | 0.34 | 5.90 | 7.58 (3.87~14.85) | 3.04 | 0.46 | 6.62 | 21.00 (8.52~51.74) | |||
| Age | 0.01 | 0.01 | 0.80 | 0.424 | 1.01 (0.98~1.04) | –0.01 | 0.01 | –0.54 | 0.586 | 0.99 (0.97~1.02) | |
| BMI | –0.03 | 0.04 | –0.79 | 0.431 | 0.97 (0.90~1.05) | 0.23 | 0.04 | 5.98 | 1.26 (1.17~1.36) | ||
OR, odds ratio; CI, confidence interval; SE, Standard Error.
This study employed a paired design to compare arrhythmia detection between the routine ECG and high-channel 12-lead Holter monitoring. The results showed that Holter monitoring was significantly superior to routine ECG in terms of the overall arrhythmia detection rate and the detection of atrial fibrillation and frequent ventricular premature beat subtypes, which is consistent with the findings of previous studies [10, 13].
In the univariate logistic regression analyses, several clinical
factors—especially smoking history, drinking history, hypertension, and heart
failure—showed large odds ratios with relatively wide 95% confidence
intervals, particularly for Holter-based detection. This pattern likely reflects
the high-risk nature of our cohort (all patients met at least one high-risk
criterion, and arrhythmia prevalence was high), which reduces the number of truly
unexposed patients and can yield imprecise and apparently inflated estimates in
univariate models, especially when outcomes are common. Age was not significantly
associated with positive arrhythmia detection, which may seem inconsistent with
clinical experience; however, our sample had a narrow age range (all
From the perspective of clinical significance, the advantages of high-channel 12-lead Holter monitoring stem from its core characteristics of “long-duration, dynamic monitoring”. Clinically, approximately 1/3 of atrial fibrillation cases are “paroxysmal atrial fibrillation”, and the duration of such episodes is often short (usually less than 24 hours). Due to the limited detection time, the missed diagnosis rate of routine ECG for paroxysmal atrial fibrillation can be as high as 30%–50% [14, 15]. In this study, high-channel 12-lead Holter monitoring additionally detected 20 cases of “Holter-only positive” atrial fibrillation. This finding strongly indicates that it can effectively compensate for the shortcomings of routine ECG in screening paroxysmal atrial fibrillation, providing a more accurate screening approach for patients with unexplained stroke or obvious palpitations but normal routine ECG results. This facilitates earlier definitive diagnosis and timely targeted treatment for such patients.
For frequent ventricular premature beats, their onset is closely associated with multiple factors, such as myocardial ischemia and autonomic nervous tension, exhibiting a significant feature of “temporal heterogeneity”—for example, the number of ventricular premature beats increases during physical activity but decreases at rest [16]. This dynamic variability, combined with underlying mechanisms like electrolyte imbalances or sympathetic activation, highlights Holter monitoring’s role in the quantitative assessment for interventions such as ablation [17]. By accurately assessing the load and characteristics of ventricular premature beats, clinicians can formulate more evidence-based treatment plans, avoiding over- or under-treatment.
While studies have demonstrated that adhesive patch-type electrocardiogram devices, by extending monitoring duration (e.g., to 72 hours), can significantly improve the detection rate of paroxysmal atrial fibrillation (PAF)—reportedly by 2.2 times compared to 24-hour Holter monitoring—their widespread clinical adoption must consider algorithm-enhanced accuracy and device cost [18, 19]. The single-lead design of many patch monitors may compromise signal quality, necessitating complementary advances in artificial intelligence (AI)-assisted analysis to ensure diagnostic reliability [20]. Therefore, despite the advantages of patch devices in extended monitoring and patient comfort, Holter monitoring remains a more widely adopted and logistically feasible option in routine clinical practice, particularly suitable for short- to medium-term monitoring scenarios [21].
However, this study also has certain limitations. First, the sample size is relatively small (only 300 subjects were included), which may affect the statistical power for low-incidence subtypes (e.g., atrioventricular block) and make it difficult to fully demonstrate the differences between high-channel 12-lead Holter and routine ECG in these subtypes. Second, the study did not conduct stratified analysis based on the severity of arrhythmias (e.g., CHA2DS2-VASc score for atrial fibrillation, Lown classification for ventricular premature beats), which limited the ability to further explore the detection advantages of high-channel 12-lead Holter for high-risk arrhythmias. Future studies could expand the sample size and conduct subgroup analysis incorporating arrhythmia severity to more comprehensively evaluate the clinical value of high-channel 12-lead Holter, thereby providing stronger evidence for its broader clinical application.
The high-channel 12-lead Holter significantly outperforms the routine 12-lead ECG in detecting arrhythmias in high-risk populations, particularly paroxysmal atrial fibrillation and frequent ventricular premature beats. Owing to its long-duration, dynamic monitoring capability, the high-channel 12-lead Holter provides an effective supplement to routine ECG for early identification of clinically significant arrhythmias in high-risk individuals and may support more timely risk stratification and intervention. Future studies with larger cohorts and stratified analyses across arrhythmia subtypes and severity will help further refine patient selection and monitoring strategies.
• This retrospective study demonstrates that the high-channel 12-lead Holter ECG significantly improves arrhythmia detection rates compared to the routine 12-lead ECG in high-risk populations, particularly for atrial fibrillation and frequent ventricular premature beats.
• Baseline risk factors such as smoking, hypertension, and heart failure are strongly associated with positive detections in univariate logistic regression, highlighting the need for targeted screening.
• The advantages of Holter monitoring lie in its extended monitoring capability, which captures paroxysmal events missed by short-duration methods, providing clinical value for early intervention.
• Limitations include sample size and lack of severity stratification, underscoring the need for future research with larger cohorts and subgroup analyses.
• Overall, Holter monitoring serves as an effective supplement to routine ECG, offering evidence-based support for cardiovascular risk management in high-risk populations.
The data that support the findings of this study are available from the corresponding author upon reasonable request.
LH and XHJ designed the research study. XHJ and LH performed the research. XHJ and LH analyzed the data. LH drafted this article. Both authors contributed to the important editorial changes in the manuscript. Both authors read and approved the final manuscript. Both authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
This retrospective study was approved by the Ethics Committee of Zibo Central Hospital (approval number: 2025262). Case data were extracted from the hospital’s electronic medical record system, ECG database, and clinical diagnosis and treatment records. The protocol was reviewed by the Ethics Committee of Zibo Central Hospital, which confirmed eligibility for consent waiver. The waiver was granted because (i) analyses were performed on existing records that had been anonymized before investigator access; (ii) the study involved no more than minimal risk; and (iii) participants’ privacy was safeguarded through de-identification and secure data handling. The study was conducted in accordance with the Declaration of Helsinki.
Not applicable.
This research received no external funding.
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.