



1 EICU, The Affiliated Xuzhou Municipal Hospital of Xuzhou Medical University, 221006 Xuzhou, Jiangsu, China
2 Emergency Ward, The Affiliated Xuzhou Municipal Hospital of Xuzhou Medical University, 221006 Xuzhou, Jiangsu, China
3 Intervention and Vascular Surgery, The Affiliated Xuzhou Municipal Hospital of Xuzhou Medical University, 221006 Xuzhou, Jiangsu, China
Abstract
Deep vein thrombosis (DVT) is a life-threatening complication in critically ill patients, and conventional prevention strategies are often hindered by poor adherence. This study aims to evaluate the clinical effectiveness of intelligent nursing interventions based on the Integrated Theory of Health Behavior Change (ITHBC) in preventing DVT among critically ill patients.
A retrospective study was conducted on 280 critically ill patients admitted to the intensive care unit of The Affiliated Xuzhou Municipal Hospital of Xuzhou Medical University between January 2022 and December 2024. Patients were divided into a control group (n = 138), which received routine care, or an observation group (n = 142), which received additional ITHBC-based intelligent nursing interventions. The incidence of DVT, nursing adherence, hematological parameters (D-dimer, prothrombin time (PT), activated partial thromboplastin time (APTT)), complications, and patient satisfaction were compared between groups.
The incidence of DVT was significantly lower in the observation group than in the control group (7.7% vs. 18.1%, p < 0.05). Nursing adherence indicators, including turning frequency, limb exercise compliance, and mechanical prophylaxis use, were markedly higher in the observation group (p < 0.05). After intervention, D-dimer levels decreased significantly in the observation group (p < 0.05), while no significant change was observed in PT or APTT (p > 0.05). No significant differences were found in complication rates (p > 0.05). Patient satisfaction was significantly higher in the observation group (96.5% vs. 87.7%, p < 0.05).
ITHBC-guided intelligent nursing interventions effectively reduced the incidence of DVT, improved patient adherence and satisfaction, and demonstrated strong safety and clinical applicability in critically ill patients.
Keywords
- deep vein thrombosis
- critical illness
- health behavior
- nursing informatics
- patient compliance
- intensive care units
Deep vein thrombosis (DVT) is a common and high-risk complication among critically ill patients [1]. Its occurrence not only increases the risk of fatal pulmonary embolism, but also prolongs hospital stay, raises medical costs, and adversely affects both prognosis and quality of life [2]. Evidence indicates that critically ill patients are predisposed to DVT due to prolonged immobility, sedation, invasive procedures, and a hypercoagulable state [3]. Despite the widespread usage of traditional preventive strategies, including anticoagulant therapy, mechanical prophylaxis, and routine nursing interventions, their effectiveness is often limited by inadequate patient adherence and resource constraints [4].
The Integrated Theory of Health Behavior Change (ITHBC) emphasizes improving knowledge, enhancing self-efficacy, and reinforcing health beliefs to facilitate sustainable health behaviors [5, 6]. This theoretical framework has been applied in chronic disease management and rehabilitation care, where structured interventions have shown to improve adherence and self-management [7]. While ITHBC has demonstrated efficacy in chronic disease management, its application in acute critical care settings remains limited [7]. Although theory-based interventions are rarely evaluated in intensive care unit (ICU) settings and the high stakes of complication prevention [8], research on their application in critical care, particularly in preventing high-risk complications such as DVT, remains scarce. The rapid advancement of intelligent nursing technologies has enabled the development of digital, individualized care models that leverage predictive analytics and personalized learning algorithms, moving beyond reminder-based interventions [9]. However, no previous studies have attempted to integrate ITHBC’s comprehensive behavior change framework with the intelligent nursing capabilities for DVT prevention. Intelligent interactive platforms can provide real-time risk assessment, personalized intervention pathways, and dynamic adherence monitoring, offering new opportunities for clinical practice [10]. Recent studies have demonstrated the efficacy of theory-driven interventions combined with intelligent technologies in improving patient adherence and clinical outcomes in high-risk settings [11]. Integrating the ITHBC framework with intelligent nursing interventions may enhance awareness, engagement, and compliance of patients and caregivers, thereby strengthening the effectiveness and sustainability of DVT prevention strategies.
Therefore, this retrospective study aims to investigate the clinical application of intelligent nursing interventions guided by the ITHBC for preventing DVT in critically ill patients. By analyzing incidence rates, adherence, and related risk indicators before and after intervention, this study seeks to provide evidence for improving DVT prevention in critical care settings and to inform the broader implementation of intelligent nursing models in intensive care management.
This single-center retrospective study screened patients admitted to the ICU of The Affiliated Xuzhou Municipal Hospital of Xuzhou Medical University between January 2022 and December 2024. A total of 312 patients were initially identified through the electronic medical record system. After excluding 32 patients with incomplete data or who did not meet the eligibility criteria, 280 patients were included in the final analysis (Fig. 1).
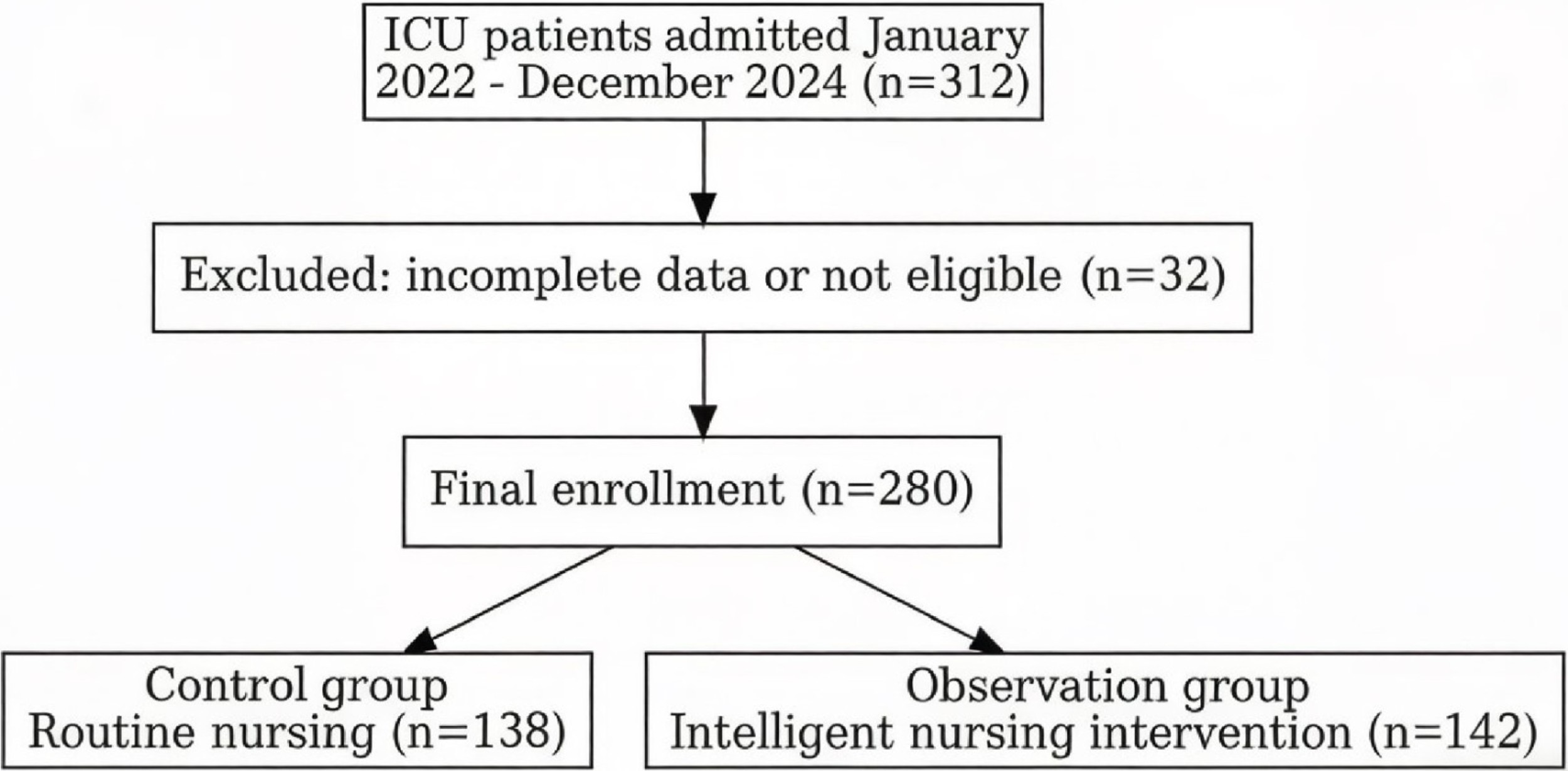 Fig. 1.
Fig. 1.
Flow chart depicting the patient enrollment process in this study. Abbreviation: ICU, intensive care unit.
Based on the type of nursing intervention, patients were divided into a control group (n = 138) that received routine nursing care for DVT prevention or an observation group (n = 142) that received intelligent nursing interventions guided by the ITHBC in addition to routine care.
Inclusion criteria of this study are as follows: (1) age
The exclusion criteria include: (1) a confirmed diagnosis of DVT or a history of venous thromboembolism prior to admission; (2) severe coagulation dysfunction or ongoing full-dose anticoagulant therapy; (3) active malignancy or an expected survival of less than 48 hours; and (4) incomplete or missing key clinical data.
Patients in the control group received routine nursing care for DVT prevention. (1) Basic assessment: Upon admission, the responsible nurse conducted a DVT risk assessment on the patient, which encompasses evaluation of past medical history, duration of bed rest, and coagulation parameters. (2) Pharmacological prophylaxis: Low-molecular-weight heparin or other anticoagulants were administered as prescribed, with close monitoring for potential bleeding complications. (3) Mechanical prophylaxis: For patients with prolonged immobility, intermittent pneumatic compression devices or elastic stockings were applied to promote venous return. (4) Basic nursing care: Patients received assistance with passive and active limb exercises, regular turning, and appropriate limb positioning to prevent venous stasis. (5) Health education: Patients’ families were educated about DVT-related knowledge and were encouraged to assist patients with turning, limb elevation, and other preventive measures.
On the basis of routine care, patients in the observation group received intelligent nursing interventions guided by the ITHBC. (1) Intelligent risk monitoring: Patient data, including hemodynamic parameters, duration of bed rest, mechanical ventilation status, and sedation level, were entered into the nursing information platform in real time. The platform automatically generated real-time DVT risk assessment reports using a machine learning algorithm that incorporated Caprini risk factors, hemodynamic trends, and treatment responses. By considering patient-specific contraindications and preferences, the platform offered recommendations of individualized intervention measures through a decision-support interface. (2) Health behavior guidance: A multimedia education system was employed to deliver personalized educational content aligned with the core concepts of ITHBC to patients and families, covering DVT risk factors, preventive measures, and warning signs of complications. (3) Adherence promotion: Through the intelligent reminder function of the platform, caregivers and staff were prompted to complete scheduled limb exercises and mechanical prophylaxis for the patients. The mobile application delivered push notifications with escalating urgency in response to missed interventions and incorporated gamification elements (e.g., adherence scorecards) that have been shown to improve user engagement in recent studies [12]. The system automatically tracked adherence rates and provided feedback. (4) Psychological and motivational support: Nurses conducted bedside counseling and interactive sessions through the intelligent platform to enhance patients’ self-efficacy, encouraging active participation in mobilization whenever feasible to ensure sustainability of preventive behaviors. (5) Closed-loop feedback and quality control: The nursing team regularly reviewed system-generated data to analyze adherence and intervention outcomes. The closed-loop system employed natural language processing to analyze nurse documentation and automatically adjusted intervention priorities based on detected patterns, creating a dynamic prevention protocol that evolved throughout the patient’s ICU stay. Interventions were dynamically adjusted within a closed-loop framework of “risk assessment–intervention implementation–outcome feedback–continuous optimization”.
All patients’ data were collected through the hospital’s electronic medical record system and nursing information platform during hospitalization. After discharge, follow-up was conducted through a combination of telephone interviews and scheduled outpatient visits. Follow-up time points were set at 7, 14, and 30 days after admission. Primary outcomes (e.g., DVT incidence) were assessed at the 30-day follow-up to evaluate long-term efficacy. Follow-up assessments focused specifically on DVT-related clinical indicators and adherence-related outcomes.
Incidence of lower limb DVT was confirmed by duplex ultrasonography and independently evaluated by at least two radiologists who were strictly blinded to the patients’ grouping and clinical intervention measures. A third senior radiologist was invited for final adjudication in case of diagnostic inconsistency.
Observation indicators employed in this study include the following:
Nursing adherence: Nursing adherence was assessed by the frequency of patient turning, compliance with limb exercises, and use of mechanical prophylaxis devices. Adherence data for the control group were documented by nurses using standardized forms during each shift, while the observation group’s adherence data were automatically captured through the intelligent nursing platform software (V2.3.1. Beijing HealthInformatics Co., Ltd., Beijing, China). The accuracy of both methods was verified via random audits conducted by research staff.
Hematological indicators: Hematological indicators include dynamic monitoring of D-dimer, prothrombin time (PT), and activated partial thromboplastin time (APTT). Hematological indicators including D-dimer, prothrombin time (PT), and activated partial thromboplastin time (APTT) were detected using the coagulation analyzer (Sysmex CA-7000, Sysmex Corporation, Kobe, Japan) with the latex-enhanced immunoturbidimetric method (for D-dimer) and one-stage clotting method (for PT and APTT). All blood samples were collected from the cubital vein in the morning after an 8-hour fast, and the detection was completed within 2 hours of sample collection in the hospital’s clinical laboratory with strict adherence to the manufacturer’s operating instructions and national clinical laboratory quality control standards.
Complications: Complications such as bleeding events or skin injuries were monitored.
Patient satisfaction: Satisfaction of patients prior to their discharge was assessed using a questionnaire, which was scored on a 5-point scale.
All clinical data were independently extracted by two researchers. Any discrepancies were resolved through review and adjudication by a senior nursing expert. Data from electronic records and the nursing platform were anonymized and stored in the hospital’s research database, accessible only to members of the study team.
All statistical analyses were performed using IBM SPSS Statistics, version 26.0
(IBM Corp., Armonk, NY, USA). Normality of continuous variables was assessed
using the Shapiro–Wilk test. Normally distributed data are expressed as mean
There were no significant differences between the control and observation groups
in terms of age, gender distribution, body mass index (BMI), prevalence of
hypertension and diabetes, smoking history, mechanical ventilation, use of
sedation and analgesia, duration of bed rest, and Acute Physiology and Chronic
Health Evaluation II (APACHE II) scores (all p
| Variable | Control group (n = 138) | Observation group (n = 142) | t/ |
p-value |
| Age (years) | 58.42 |
59.06 |
–0.440 | 0.660 |
| Male | 82 (59.4%) | 85 (59.9%) | 0.006 | 0.940 |
| BMI (kg/m2) | 24.68 |
24.35 |
0.840 | 0.402 |
| Hypertension | 64 (46.4%) | 68 (47.9%) | 0.239 | 0.811 |
| Diabetes | 39 (28.3%) | 41 (28.9%) | 0.120 | 0.905 |
| Smoking history | 41 (29.7%) | 43 (30.3%) | 0.119 | 0.905 |
| Mechanical ventilation | 77 (55.8%) | 81 (57.0%) | 0.069 | 0.793 |
| Sedation/analgesia | 84 (60.9%) | 86 (60.6%) | 0.005 | 0.946 |
| Bed rest duration (days) | 11.25 |
11.02 |
0.549 | 0.583 |
| APACHE II scores | 18.62 |
18.24 |
0.598 | 0.551 |
Abbreviations: BMI, body mass index; APACHE II, Acute Physiology and Chronic Health Evaluation II.
The incidence of DVT was significantly lower in the observation group compared
with the control group (p
| Group | DVT incidence |
| Control group (n = 138) | 25 (18.1%) |
| Observation group (n = 142) | 11 (7.7%) |
| 6.717 | |
| p-value | 0.010 |
Abbreviation: DVT, deep vein thrombosis.
Univariate logistic regression analysis was performed to screen candidate
variables associated with DVT occurrence (screening threshold: p
Multivariate logistic regression analysis was performed to identify independent
predictors of DVT occurrence, including only the variables with p
| Variable | OR | 95% CI | p-value |
| Bed rest duration | 1.2 | 1.02–1.41 | 0.03 |
| APACHE II scores | 1.1 | 1.01–1.20 | 0.04 |
Abbreviations: CI, confidence interval; DVT, deep vein thrombosis; OR, odds ratio.
The Events Per Variable (EPV) principle was used to verify the rationality of the multivariate model. In this study, there were 36 DVT events (25 in the control group and 11 in the observation group), and the model included 2 independent variables. The resulting EPV value of 18 (36/2) exceeds the minimum requirement of 10—recommended for a stable logistic regression model—indicating that the sample size is sufficient to support the statistical requirements of multivariate analysis.
The observation group demonstrated significantly higher adherence than the
control group in terms of turning frequency, limb exercise compliance, and
mechanical prophylaxis use (p
| Indicator | Turning frequency (times/day) | Limb exercise compliance | Mechanical prophylaxis use |
| Control group (n = 138) | 4.12 |
92 (66.7%) | 88 (63.8%) |
| Observation group (n = 142) | 5.36 |
123 (86.6%) | 120 (84.5%) |
| t/ |
–9.256 | 15.631 | 15.758 |
| p-value |
Before intervention, there were no significant differences between the two
groups in terms of D-dimer, PT, and APTT levels (p
| Group | D-dimer (mg/L) | PT (s) | APTT (s) | |||
| Before | After | Before | After | Before | After | |
| Control (n = 138) | 1.82 |
1.58 |
12.56 |
12.48 |
35.24 |
35.16 |
| Observation (n = 142) | 1.79 |
1.25 |
12.61 |
12.55 |
35.31 |
35.25 |
| t value | 0.461 | 6.308 | –0.416 | –0.588 | –0.184 | –0.240 |
| p-value | 0.646 | 0.678 | 0.557 | 0.854 | 0.810 | |
Abbreviations: APTT, activated partial thromboplastin time; PT, prothrombin time. Before: Within 24 hours after ICU admission and prior to DVT preventive nursing interventions; After: On the 7th day of continuous DVT preventive nursing interventions. *: indicates a statistically significant difference in the within-group paired t-test (p
The incidence of complications, including bleeding events and skin pressure
injuries, was lower in the observation group than in the control group. However,
the differences were not statistically significant (p
| Group | Bleeding events | Skin pressure injuries | Total |
| Control group (n = 138) | 7 (5.1%) | 6 (4.3%) | 13 (9.4%) |
| Observation group (n = 142) | 5 (3.5%) | 4 (2.8%) | 9 (6.3%) |
| 0.411 | - | 0.918 | |
| p-value | 0.522 | 0.536 | 0.338 |
Fisher’s exact test was used for the statistical analysis of the total complication rate (bleeding events + skin pressure injuries) due to the expected frequency of some cells being less than 5. This test only generates a two-sided p-value and no
Patient satisfaction scores were significantly higher in the observation group
compared with the control group (p
| Group | Satisfied | Basically satisfied | Dissatisfied | Overall satisfaction |
| Control group (n = 138) | 92 (66.7%) | 29 (21.0%) | 17 (12.3%) | 121 (87.7%) |
| Observation group (n = 142) | 113 (79.6%) | 24 (16.9%) | 5 (3.5%) | 137 (96.5%) |
| - | - | - | 7.482 | |
| p-value | - | - | - | 0.006 |
The primary clinical outcome of patient satisfaction is the overall satisfaction rate (satisfied + basically satisfied). The indicators are categorical data used to calculate this overall rate and do not carry independent clinical or statistical significance; therefore, only the overall satisfaction rate is reported.
Deep vein thrombosis (DVT) is a frequent and severe complication among critically ill patients, with its development involving the classical triad of hypercoagulability, venous stasis, and endothelial injury [13, 14]. Critically ill patients are particularly susceptible due to prolonged immobilization, mechanical ventilation, sedation, and invasive procedures, all of which contribute to impaired venous return and coagulation abnormalities [15]. Once thrombi form and embolize, life-threatening pulmonary embolism may occur. Current preventive strategies mainly include pharmacological prophylaxis, such as low-molecular-weight heparin, and mechanical methods such as intermittent pneumatic compression and elastic stockings [16]. However, pharmacologic prophylaxis carries bleeding risks, and efficacy of mechanical approaches relies heavily on patient adherence, which often limits their effectiveness in practice [17, 18]. Thus, optimizing the safety, efficacy, and sustainability of DVT prevention remains a critical challenge in critical care nursing.
The present study demonstrated that the incidence of DVT was significantly lower in the observation group than in the control group, along with notable improvements in nursing adherence and patient satisfaction, without a significant increase in complication rates. These findings suggest that intelligent nursing interventions guided by the ITHBC provide a valuable supplement to traditional prevention strategies in critically ill patients. Improved adherence played a central role in reducing the risk of DVT. Through real-time risk assessment and personalized reminders, the intelligent nursing platform enhanced patients’ and caregivers’ understanding of DVT risk factors and preventive strategies. Multimedia education combined with mobile-based alerts overcame the limitations of traditional one-way health education, empowering patients to actively participate in DVT prevention efforts. Previous studies have emphasized that poor adherence is a major barrier to effective DVT prevention [19, 20]; our results confirm that a theory-based, technology-assisted nursing model can effectively address this gap. Regarding hematological indicators, the observation group showed significantly lower D-dimer levels after intervention compared with the control group, while PT and APTT levels remained comparable. D-dimer, a fibrin degradation product, is a sensitive biomarker of thrombus formation and lysis [21]. Its reduction reflects a decreased risk of thrombosis [22, 23]. This suggests that intelligent nursing interventions, by promoting frequent repositioning, encouraging limb exercises, and increasing adherence to mechanical prophylaxis, may improve venous hemodynamics and indirectly mitigate hypercoagulability.
In terms of safety, the incidence of complications such as bleeding and skin pressure injuries was slightly lower in the observation group, with no statistically significant difference. This indicates that intelligent nursing interventions are both safe and feasible in critically ill patients. Moreover, patient satisfaction scores were significantly higher in the observation group, reflecting that individualized and technology-assisted care not only improves clinical outcomes but also enhances the care experience, thereby fostering stronger patient–caregiver relationships.
This study demonstrates distinct innovations compared with conventional DVT
prevention research. While prior studies have predominantly focused on
pharmacological efficacy and mechanical device optimization [24], our approach
integrates behavioral theory with intelligent technology in a novel framework.
Our ITHBC-guided approach achieved a more substantial reduction (7.7% vs.
18.1%, p
By incorporating ITHBC into critical care practice,
this study highlights the importance of reinforcing the
knowledge-belief-behavior pathway while leveraging intelligent
platforms to achieve closed-loop management. The
present study observed significant improvement in patient
satisfaction (96.5% vs. 87.7%, p
This study, however, has certain limitations. It was a single-center retrospective study with a relatively small sample size, which may introduce selection bias. The follow-up period was relatively short, limiting the evaluation of long-term outcomes. Furthermore, patient-level heterogeneity, such as variations in nutritional status, inflammatory markers, and genetic predispositions, was not comprehensively analyzed. Therefore, future multicenter, large-sample, prospective studies with extended follow-up are needed to further validate these findings and refine individualized nursing strategies.
Intelligent nursing interventions guided by the ITHBC effectively reduced the incidence of DVT, improved adherence, and enhanced patient satisfaction in critically ill patients, without raising the incidence of complications. This model offers a novel, safe, and practical approach for DVT prevention in critical care, and holds promise for broader clinical application.
• Intelligent nursing interventions guided by the Integrated Theory of Health Behavior Change (ITHBC) significantly reduced deep vein thrombosis (DVT) incidence in critically ill patients.
• The intervention model improved nursing adherence through real-time monitoring and personalized reminders.
• Patient satisfaction was enhanced with ITHBC-guided intelligent nursing interventions, while safety was maintained, with no significant increase in complications.
• This approach represents an innovative integration of behavioral theory with intelligent healthcare technology.
• The study provides evidence for implementing theory-driven nursing models in critical care settings.
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request. The intelligent nursing platform software is proprietary and available for research collaboration through institutional agreements.
CWL and PX: conceptualization, methodology, writing-original draft. JH and YQZ: data curation, formal analysis. MYL, YQZ and HW: investigation, resources. QL and HW: software, validation. All authors contributed to revising the manuscript critically for important intellectual content. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
This study was approved by the Medical Ethics Committee of The Affiliated Xuzhou Municipal Hospital of Xuzhou Medical University (Approval No.: xyyll[2025]173). Informed consent was waived due to the retrospective nature of the study and the use of anonymized data. The study adhered to the Declaration of Helsinki and relevant institutional guidelines. All procedures were conducted in accordance with relevant guidelines and regulations, with strict measures taken to ensure patient confidentiality throughout the study.
The authors thank the nursing staff of the ICU for their assistance in data collection and implementation of the interventions.
This research received no external funding.
The authors declare no conflict of interest.
Supplementary material associated with this article can be found, in the online version, at https://doi.org/10.31083/BJHM52246.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.