




 , James Miller 1, Lawrence Moulton 2
, James Miller 1, Lawrence Moulton 21 University of Exeter Medical School, EX1 2HZ Exeter, UK
2 Orthopaedics Department, Royal Cornwall Hospitals NHS Trust, TR1 3LJ Truro, UK
Abstract
Scaphoid fractures are a common but frequently missed wrist injury. Patients classically present following a fall onto an outstretched hand, with pain and tenderness in the anatomical snuffbox. When missed, scaphoid fractures can have serious complications such as avascular necrosis of the scaphoid and scaphoid non-union advanced collapse. The British Society for Surgery of the Hand has recently published guidelines on the management of suspected scaphoid fractures. Initial management involves radiographs and immobilisation with referral to a specialist within 7 days. Further management includes immobilisation for stable fractures and surgical intervention for cases with greater than 2 mm displacement, associated distal radial fractures, peri-lunate injuries, or proximal pole fractures with any displacement. Follow-up radiographs and computed tomography are used to monitor healing. This article aims to review recent advances in scaphoid fracture management, aligned with the latest British Society for Surgery of the Hand (BSSH) guidelines.
Keywords
- hand
- scaphoid
- fracture
- pain
- avascular necrosis
The scaphoid, along with the radius, lunate, and triquetrum, helps form the proximal part of the wrist joint [1]. It is the largest bone in the proximal row of carpals and plays a crucial role in wrist stability and movement [2]. It is also the most frequently fractured carpal bone, most commonly injured following hyperextension of the wrist, such as from a fall on an outstretched hand [3, 4]. The blood supply to the scaphoid is from branches of the radial artery. The superficial palmar branch enters at the distal tubercle and supplies the distal pole. The dorsal scaphoid branch enters the scaphoid distally at the dorsal ridge, supplies both the distal and proximal poles [5, 6]. The dorsal carpal branch is the only artery that supplies the proximal pole, which relies on a retrograde blood supply, making it the most likely part of the scaphoid to be affected by avascular necrosis [7].
Avascular necrosis (AVN) is one of the most common complications of scaphoid fractures, affecting between 13–50% of patients with scaphoid fractures, with an even higher incidence in those with a fracture involving the proximal one-fifth of the scaphoid [8]. Current research indicates surgical management through either proximal row carpectomy or vascularised bone grafting as the preferred option for treatment of scaphoid AVN compared to conservative management, as it results in greater improvement in pain and range of motion at the wrist [9]. Other complications include nonunion, which can be described as a fracture that persists for a minimum of nine months without signs of healing for three months. Nonunions invariably lead to instability, deformity and long-term degenerative problems in otherwise young and healthy patients [10]. A recent meta-analysis has shown that factors such as smoking significantly increase the risk of persistent post-operative non-union, making it imperative to gather this information during initial clinical evaluation [11]. This article reviews recent British Society for Surgery of the Hand (BSSH) guideline updates for scaphoid fracture diagnosis and management and provides a suggested treatment algorithm that clinicians can follow.
Scaphoid fractures occur most commonly in young males, with the highest incidence between the ages of 15 and 19. The annual incidence of scaphoid fractures is 12.4 per 100,000 people [12]. Scaphoid fractures are most commonly caused by a forced hyperextension of the wrist, usually due to a fall onto an outstretched hand. Other common causes include contact sports and road traffic accidents [5].
Scaphoid fractures are commonly misdiagnosed and treated as wrist sprain, or soft tissue injuries, leading to delayed detection and management [5]. Therefore, to ensure timely diagnosis and management, it is imperative to understand the pertinent features of a typical scaphoid fracture patient history. Patients with scaphoid fractures classically present with wrist trauma following a fall onto an outstretched hand. Patients will typically complain of swelling, pain and reduced range of motion on the affected wrist, which worsens with movement [13].
A common reason for scaphoid fracture misdiagnosis is that they can be easily missed on early imaging, leading to clinicians exploring alternate diagnoses [5]. However, in patients with a suggestive history, there should remain a strong index of suspicion even after early imaging, as delayed presentation and treatment can lead to the development of non-union, which can lead to long-term issues like arthritis for patients later in life.
Other risk factors for scaphoid non-union include female sex, regular manual labour, proximal pole fracture, presence of avascular necrosis, the degree of fracture displacement and smoking/nicotine use [14].
Smoking impairs fracture healing and increases the risk of non-union through decreasing expression of angiogenic markers in the early bone healing phase, specifically less expression of vascular endothelial growth factor (VEGF) and von Willebrand factor (vWF). This decreases nutrient supply to the fracture site during the reparative phase of bone healing, which leads to delayed healing [15].
During initial clinical evaluation, it is important to ascertain as many of these risk factors as possible to aid management strategies moving forward.
When examining a potential scaphoid fracture, it is usually best to take a look, feel, and move approach. During inspection, it is important to look at both the hand and wrist, looking for any swelling or abnormalities (Table 1, Ref. [5, 13]). There will often not be any significant findings in this part of the examination in scaphoid fractures unless there is an associated carpal dislocation, such as a peri-lunate dislocation.
| Step | Action |
| Look | - Inspect the hand and wrist, looking for swelling and any deformities. |
| - Deformities are unlikely to be seen unless there is associated carpal dislocation, such as peri-lunate dislocation. | |
| Feel | - Palpate the anatomical snuffbox. |
| - Palpate over the distal radius, ulna and the metacarpals to assess for any associated injury. | |
| - Tenderness most commonly presents in these three areas: | |
| 1. The volar prominence at the distal wrist in distal pole fractures. | |
| 2. Anatomic snuffbox in waist or mid-body fractures. | |
| 3. Distal to Lister’s tubercle in proximal pole fractures. | |
| Move | - Ulnar deviation at the wrist. Pain in anatomical snuffbox during this is suggestive of scaphoid fracture. |
Next, it is important to palpate the hand. There should be particular focus on palpation of the anatomical snuffbox as well as the distal radius, ulna and metacarpals to assess for any additional injuries. Pain is most commonly seen at the radial side of the wrist, and at the scaphoid tubercle, with tenderness on the anatomic snuffbox [13].
For the final part of the examination, it is important to move the hand and wrist. Ulnar deviation of the wrist should be performed. Pain in the anatomical snuffbox during this is suggestive of a scaphoid fracture [5].
The management of scaphoid fractures involves immobilisation, imaging for accurate diagnosis, and deciding between surgical and conservative approaches based on the fracture type and patient-specific factors. Timely and appropriate management is crucial to reduce complications such as non-union and to ensure optimal healing [8, 16].
Scaphoid fractures are difficult to diagnose from history and examination alone, requiring further investigation to confirm or exclude the diagnosis. Furthermore, occult fractures may be easily missed without adequate imaging from multiple angles. To ensure accurate diagnosis, the BSSH have issued recent guidelines that recommend all patients with suspected scaphoid fractures should have scaphoid radiographs from at least 4 angles, including a posteroanterior, lateral, semi-prone and an elongated scaphoid view [17]. If no fracture is visible on initial plain radiographs, the wrist should be immobilised with a splint, with specialist referral within 7 days in addition to Magnetic Resonance Imaging (MRI), depending on local emergency department guidelines [18]. If a fracture is visible on radiographs, patients should be placed into a below-elbow back slab with referral to be seen by a specialist within 7 days, as per recent BSSH guidance (Fig. 1). This is an update on the 2022 guidelines, which recommended that patients with both visible and non-visible fractures on initial presentation should be seen within 7–14 days. This change highlights the importance of timely management of scaphoid fractures.
 Fig. 1.
Fig. 1.
Single-view radiograph of the wrist demonstrating an undisplaced fracture through the waist of the scaphoid bone, shown by the red arrow. Fig. 1 is adapted from [Frank Gaillard] [https://radiopaedia.org/], rID:7669, available under the CC-NC-BY-SA 3.0 license (https://creativecommons.org/licenses/by-nc-sa/3.0/legalcode).
In patients with perilunate injury on initial radiography urgent reduction should be performed, as well as additional imaging via a computed tomography (CT) scan.
Definitive management for suspected scaphoid fractures should be decided within 2 weeks of initial presentation after adequate imaging has been performed [18].
After initial assessment, repeat radiographs should be performed in one week when seen by a specialist. If these don’t show a fracture, patients should be treated conservatively using a wrist splint and discharged with safety netting and a patient information leaflet. If a fracture is present, CT should be arranged [18].
In patients with scaphoid waist fracture of greater than 2 mm displacement,
proximal pole fracture with any displacement and displaced distal radial
fracture, surgical fixation should be arranged within 2 weeks of the initial
injury, as per recent BSSH guidance. A CT should then be arranged in 6–8 weeks
to monitor union formation [19, 20]. Those with scaphoid tubercle fractures should
be immobilised for 4–6 weeks and discharged with patient-initiated follow-up.
Patients with delayed immobilisation of
Initial radiographs should be performed, with a follow-up MRI within one week, depending on local emergency department policies, if the radiographs are inconclusive [18]. Additionally, scaphoid radiographs for all patients should be arranged one week after initial presentation. If no fracture is found on repeat imaging, other diagnoses should be considered and treated accordingly [18].
If a fracture is present on repeat imaging, a CT is recommended for further
assessment. Patients with delayed immobilisation (
 Fig. 2.
Fig. 2.
Computed tomography (CT) showing waist of scaphoid fracture with rotation of the proximal (bottom green arrow) and distal poles (top green arrow), resulting in displacement and resultant humpback deformity (red) due to volar angulation of both poles. Fig. 2 is adapted from [Frank Gaillard] [https://radiopaedia.org/], rID:18269, available under the CC-NC-BY-SA 3.0 license (https://creativecommons.org/licenses/by-nc-sa/3.0/legalcode).
Both CT and MRI are valuable imaging tools for fractures missed on plain radiographs. A study comparing the use of CT versus MRI scanning in the diagnosis of scaphoid fractures negative on plain radiograph reported that CT had a sensitivity of 0.72 and specificity of 0.99, while MRI showed a higher sensitivity of 0.88 and specificity of 1.00 (Table 2, Ref. [21]). The study shows that while the diagnostic accuracy of both modalities is generally comparable, MRI does have slightly better sensitivity and specificity. This is supported by the BSSH guidelines, which recommend that MRI be used in the diagnosis of occult scaphoid fractures and CT for further investigation of already confirmed scaphoid fractures [18].
| CT | MRI |
| Higher cost | Lower cost |
| Faster | Longer wait times |
| Lower sensitivity | Higher sensitivity |
| Lower specificity | Higher specificity |
Adapted from [21]. MRI, Magnetic Resonance Imaging.
Non-surgical management is recommended for fractures that don’t require surgery, for patients who aren’t suitable candidates for surgery, or if the patient chooses not to undergo surgery. Common indications include stable, nondisplaced fractures, including nondisplaced waist and distal pole fractures [4]. Management involves immobilisation in a wrist splint or a below-elbow cast for 6–8 weeks, with out-of-cast radiographs performed at the end of this period. If the union is progressing well, immobilisation should be continued with further review at 12 weeks with radiographs and CT if radiographs are equivocal. However, if nonunion or delayed healing is detected, the treatment plan should be adjusted, shifting to surgical intervention [18]. This is an update to the 2022 guidelines, which only stated to consider surgical intervention in these cases [17].
Surgery is necessary for fractures with
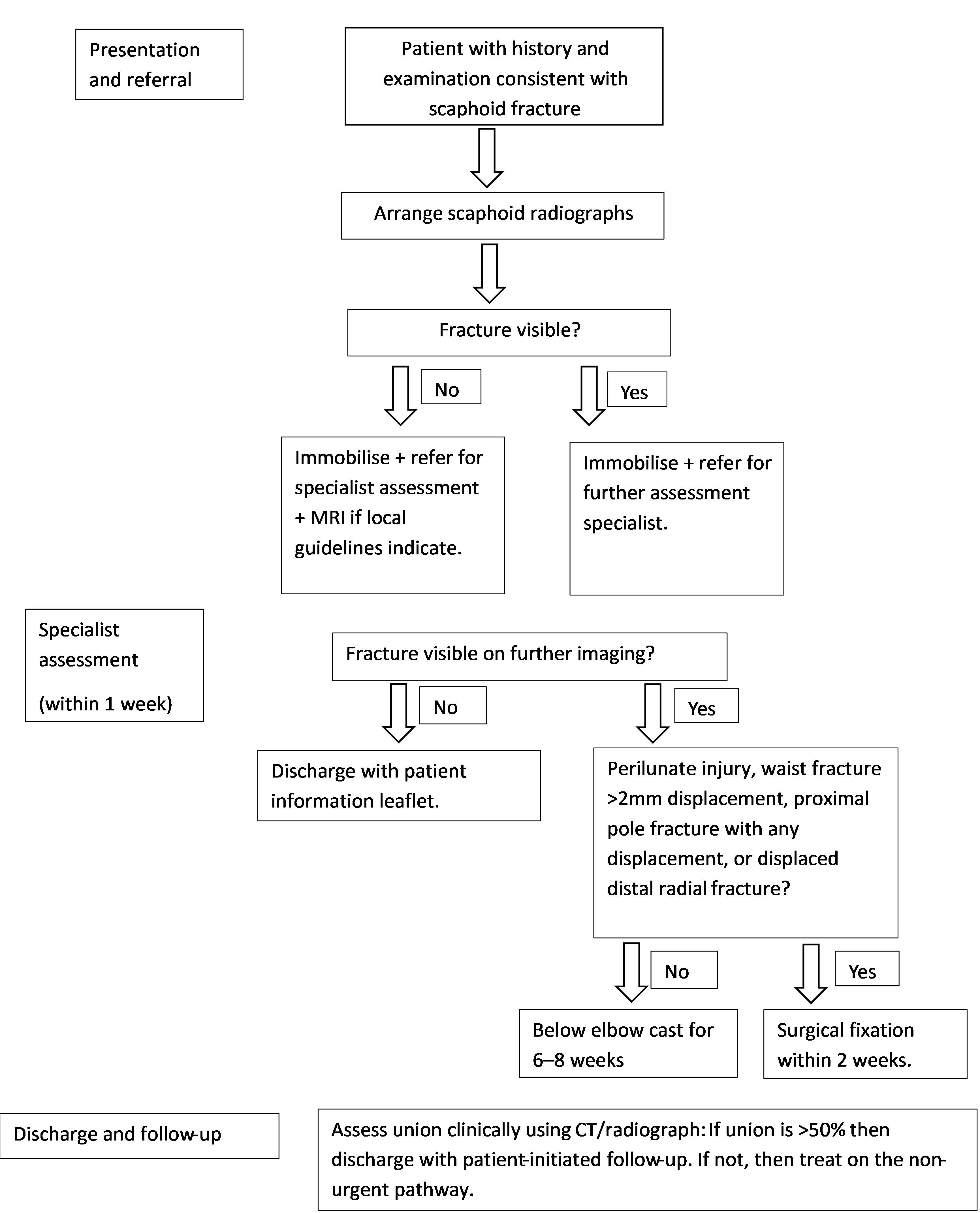 Fig. 3.
Fig. 3.
A suggested investigation and treatment algorithm for management of suspected scaphoid fractures. Figure made using Microsoft Word (version 2502 Build 16.0.18526.20168, Microsoft Corporation, Redmond, WA, USA).
| Surgical management | Non-surgical management |
| Perilunate injury | Waist fracture |
| Waist fracture |
Undisplaced proximal pole fracture |
| Proximal pole fracture with any displacement | Scaphoid tubercle fracture |
| Displaced distal radial fracture | Delayed presentation with no clear fracture gap |
| Delayed presentation with clear fracture gap in skeletally mature patients | Delayed presentation where patient is skeletally immature |
Adapted from [18].
The current gold standard for displaced scaphoid fracture fixation is open reduction and internal fixation (ORIF) and has been largely successful, with a meta-analysis showing a union rate of 90% [22]. However, open surgery does have its risks and can result in disruption of the scaphoid’s blood supply as well as capsular scaring, which may limit postoperative movement in patients [4].
Due to the risks associated with ORIF, minimally invasive (MI) surgery has become increasingly popular, presenting the theoretical advantages of minimising surgical trauma, not interfering with the native blood supply and preserving carpal ligament proprioception [23].
A recent systematic review compared the results from open versus arthroscopic-assisted nonvascularised bone grafting for delayed union and nonunion scaphoid fractures. The results found low certainty evidence that arthroscopic-assisted surgery may have reduced healing time compared to open; however, they found no statistically significant differences in union rate or time to union formation [24].
Another systematic review looking at arthroscopic surgery for scaphoid nonunion found that a postoperative union rate of 96% was achieved in an average time of 13.5 weeks. Patients reported outcomes were also significantly improved with a reported pain reduction of almost 80% compared to the preoperative level, in addition to an almost 40% improvement in grip strength, and recovery in wrist function during daily activities. Other advantages of arthroscopic surgery found in the study include reduced wrist and carpal ligament injury, as it does not require an open arthrotomy, which may lead to carpal malalignment through compromised mechanical strength and impaired proprioceptive and neuromuscular control. Additionally, long-term benefits of arthroscopic scaphoid surgery include less pain, stiffness, and scarring compared to open surgery. Some disadvantages of arthroscopic surgery include a longer intraoperative time and significant technical difficulty [25].
One popular MI procedure involves the placement of arthroscopic portals in the hand, to visualise the scaphoid and surrounding structures. The three main portals are the midcarpal ulnar (MCU) portal, the midcarpal radial (MCR) portal and the scaphotrapeziotrapezoid (STT) portal. The MCU portal helps to visualise the scaphoid fracture, while the remaining portals are used for the surgery. It is through these remaining portals that fibrotic tissue, bony callus and sclerotic bone are debrided until fresh cancellous bone is visualised. The scaphoid alignment is then corrected using two 1.2-mm Kirschner wires, which are inserted perpendicularly into both proximal and distal fragments. Then, a 1.0-mm Kirschner wire is percutaneously drilled into the distal pole of the scaphoid, along the central axis of the scaphoid under fluoroscopic guidance until the subchondral bone of the proximal pole is reached. After this, a cancellous bone graft from the distal radius is inserted into the drilled site. After this, two 2.4 mm diameter screws are placed over the Kirschner wires, and the Kirschner wires are subsequently removed [26].
Postoperative complications are monitored using CT, where the surgeon should assess whether over 50% union has been achieved, after which the patient may be discharged with patient-initiated follow-up [18]. Patients should also be provided with safety netting advice for potential complications, the most serious of which is compartment syndrome. Patients should be informed to return urgently if they feel extreme, disproportionate pain at the site of the operation.
The next step in post-surgical care involves immobilisation, with a cast, splint or both [27]. Currently, there is no consensus on the length of the immobilisation period required, due to positive results from both prolonged and shorter periods of immobilisation. Additionally, the immobilisation period required depends on different factors, including patient factors like age and activity levels, the type of surgery performed and the type of fracture [28].
Current evidence shows that the average immobilisation length for nondisplaced scaphoid fractures varies from zero immobilisation to immobilisation using a short arm thumb-spica for 7–10 days followed by a removable thumb splint until union, with both methods showing promising results [28].
For displaced fractures, the average immobilisation length varies from 2–8 weeks for most patients, with all immobilisation lengths achieving a high rate of union. Immobilisation is usually performed with a thumb-spica cast or splint, or in some cases a Colles-type cast. While there is no consensus on the immobilisation period required, there is agreement that an increased time to union is associated with increased age and increased preoperative displacement [28].
The final step in post-surgical care is rehabilitation exercises. These include shoulder flexion and abduction, elbow flexion and extension, finger flexion and extension, as well as thumb flexion, extension and opposition. At around 6 weeks post-operation, the cast can be removed in the clinic and bone healing assessed using CT [27, 29]. During this assessment, it is decided whether further immobilisation is required and if there has been enough healing for patients to start moving their wrist [27].
During wrist rehabilitation, it is important to emphasise flexion and extension at the wrist both with and without resistance [30].
Finally, lifestyle factors which slow down fracture healing should also be addressed. Smoking cessation is recommended during rehabilitation to speed up recovery [31]. Some common methods used to achieve this include utilisation of nicotine replacement therapy, e-cigarettes and vaping, and face-to-face or telephone counselling sessions [32].
Scaphoid fractures are a common but often missed diagnosis. Complications of missed fractures include avascular necrosis of the scaphoid and nonunion, which can lead to arthritis and deformity. To prevent these complications, it is crucial that these fractures are diagnosed in a timely manner. Radiographs from multiple views, as well as further imaging through CT and MRI, are imperative as the diagnosis is difficult to make from history and examination alone. Immobilisation is the mainstay in management, with further treatment involving surgery in some patients, and CT is used to monitor healing. There is currently no consensus on the post-operative immobilisation period for scaphoid fractures, and this should be addressed by future studies.
• Scaphoid fractures are a common but frequently missed diagnosis.
• Scaphoid radiographs from multiple views should be arranged in all suspected scaphoid fractures with can and/or MRI where fracture is not immediately visible.
• Patients are often managed conservatively using wrist splints or below elbow back slab.
• Patients with peri lunate injury, waist fracture
Not applicable.
BI, JM, and LM made substantial contributions to the conception and design of the work, as well as to the acquisition, analysis, and interpretation of the data. LM provided supervision and advice on article content. BI drafted the manuscript. All authors were involved in critical revisions of the article. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
Not applicable.
We would like to thank Frank Gaillard for providing the images (Fig. 1, rID: 7669; Fig. 2, rID: 18269; https://radiopaedia.org/) and granting permission for their use in this work.
This research received no external funding.
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.