


 , Edwina A Brown 1,2,*
, Edwina A Brown 1,2,*
1 Department of Renal Medicine, Hammersmith Hospital, Imperial College Healthcare NHS Trust, W12 0HS London, UK
2 Department of Immunology and Inflammation, Faculty of Medicine, Imperial College London, SW7 2AZ London, UK
Abstract
An ageing population in the UK has seen an increased prevalence of chronic kidney disease (CKD), with a higher proportion of old, frail people requiring kidney replacement therapy. This article aims to explore why peritoneal dialysis (PD) may be the optimal dialysis modality for older people, considering factors such as frailty and cognitive impairment. PD offers considerable benefits over haemodialysis, including improved quality of life, benefits to cognition and higher treatment satisfaction. Assisted PD supports the maintenance of treatment for those with physical or cognitive impairments and helps to alleviate caregiver burden. Despite this, challenges such as treatment burden and peritonitis should be thoroughly considered. Overall, PD aligns well with the priorities of older people, emphasising quality of life and autonomy over survival. However, there needs to be improved funding and access to assisted PD programmes going forward to ensure PD is a viable treatment option.
Keywords
- peritoneal dialysis
- frailty
- cognitive impairment
- quality of life
- assisted peritoneal dialysis
Over 11 million people in the UK are aged 65 years and older, making up almost 19% of the total population [1]. As chronic kidney disease (CKD) becomes more common with increasing age, its prevalence is increasing with higher numbers of older people subsequently requiring kidney replacement therapy (KRT) [2]. There is also an increasingly frail population [3]. Whilst clinically distinct from ageing, frailty is common in those with CKD. Discussions about KRT should therefore be tailored to consider the potential challenges of ageing and frailty experienced by older people.
KRT encompasses haemodialysis (HD), peritoneal dialysis (PD) and kidney transplantation, although older people are less likely to undergo transplantation due to issues of both short- and long-term complications related to age and/or frailty [4]. Many older patients subsequently default to HD [2], which may not be the optimal dialysis modality for the old, frail person. Alternatively, PD offers a home-based therapy which may be more suitable, with possible benefits as shown in Fig. 1. This review will explore the reasons why PD may be the best treatment for frail, elderly individuals (Fig. 2), taking into account patient characteristics that should form the basis of shared decision-making.
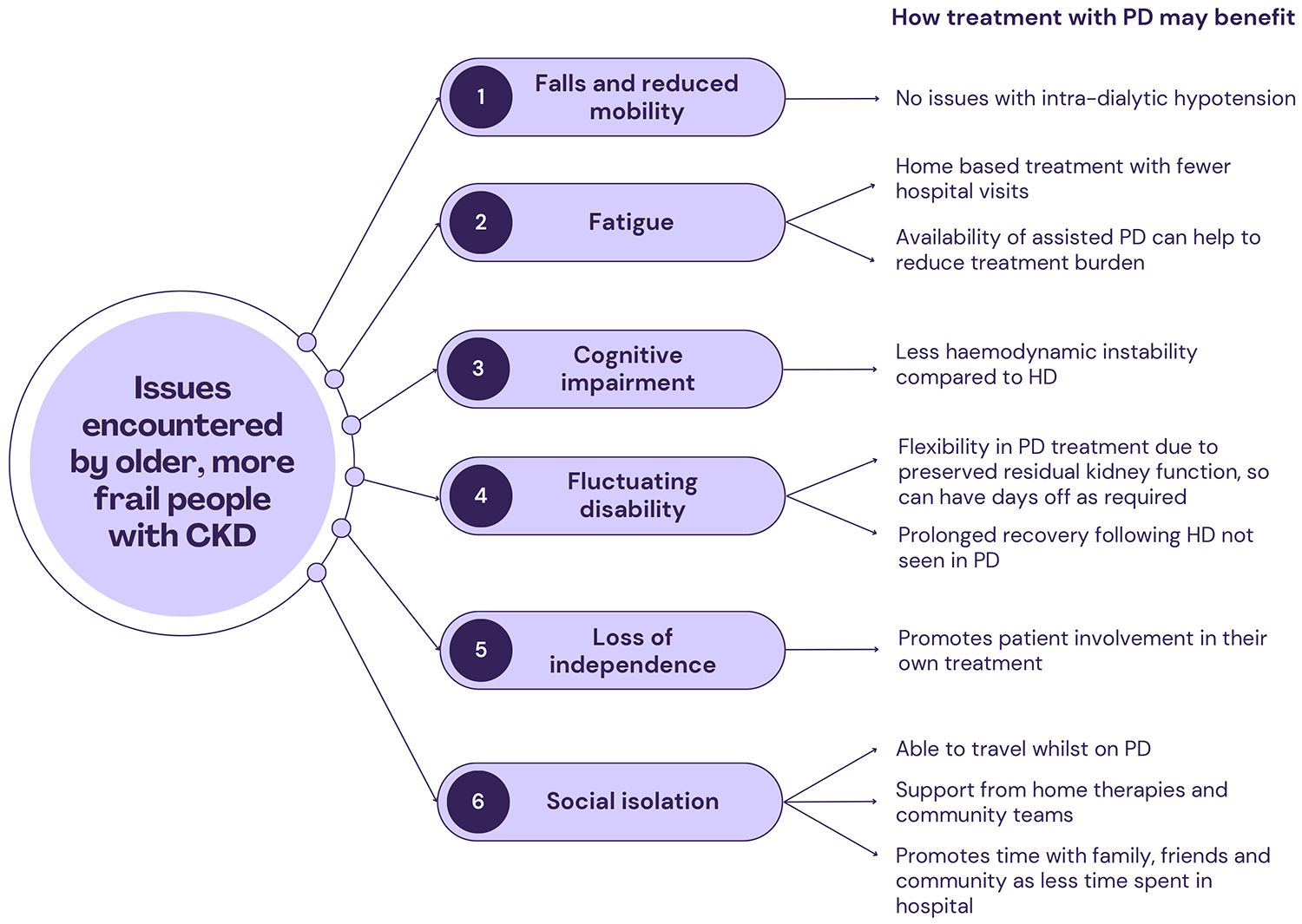 Fig. 1.
Fig. 1.
How PD may address problems encountered by elderly, frail people with CKD (Created with Canva, https://www.canva.com, 2025). PD, peritoneal dialysis; HD, haemodialysis; CKD, chronic kidney disease.
 Fig. 2.
Fig. 2.
Benefits of PD in the old, frail person (Created with Canva, https://www.canva.com, 2025).
Frailty is defined as a state of increased vulnerability alongside declining physiological function [5]. Its presence has an adverse effect on clinical outcomes for older people with CKD [6] and higher rates of mortality in dialysis patients [7]. Different models for frailty have been hypothesised. One of the most widely used is the Fried frailty phenotype which encompasses weight loss, fatigue, weakness, poor mobility and low physical activity [8]. These characteristics present a complex array of challenges and increased symptom burden for those with end-stage kidney disease (ESKD), including falls, cognitive impairment, hospitalisation and premature death [9]. Integration of elderly care physicians and use of the Comprehensive Geriatric Assessment has allowed for clearer identification and management of these frailty syndromes in the outpatient setting [10].
There is an increasing prevalence of frailty in both those with CKD and on dialysis; one study found that 82% of older people with CKD stage 5 fitted the criteria for frailty [11]. The impact of frailty was demonstrated in the Frail and Elderly Person on Dialysis (FEPOD) study. They showed that frailty was the main predictor in outcomes measured between groups of older people on assisted PD versus HD, with higher treatment satisfaction in those on assisted PD [12].
For those on HD, frailty can increase the risk of hospitalisation (odds ratio (OR), 2.47; 95%
confidence interval (CI), 1.52–4.03, p
Frailty also affects outcomes for people on PD [15], but this is comparatively understudied in the elderly. Positive treatment characteristics of PD include daily delivery of treatment with shorter recovery time, no requirement for vascular access and fewer hospital visits. These factors may help to mitigate the impact of frailty in older people, and a thorough assessment of frailty should be central to all decision-making on KRT.
Cognitive impairment (CI) is highly prevalent amongst the old, frail population, and to a greater degree in those with advanced CKD [16]. The implications of this are significant. There are impacts on executive function and attention [16], as well as increased mortality [17]. More widely, CI can lead directly to an increased incidence of depression, which may in turn worsen cognition and associated functioning [18]. Therefore, the presence of CI should be assessed with onward referral to the memory clinic if undiagnosed dementia is suspected.
CI is accelerated on HD via HD-induced circulatory ischaemia, white matter
insults and increased rates of cerebrovascular accidents. One study demonstrated
a reduction in global cerebral blood flow of 10% during HD in a cohort of 12
patients aged over 65 years (p = 0.03), suggesting that it was this
repeated insult which contributed to progressive CI in those on HD
[19]. Additional research explored the longer-term
consequences of HD by using magnetic resonance imaging (MRI). The images
demonstrated cerebral atrophy (p
The risk of stroke is also higher in HD patients. A large cohort study of almost
21,000 patients found that stroke rates began to increase up to 90 days before
starting HD and peaked within the first 30 days post-HD start (p
Conversely, PD has less of an impact on cognitive health as it avoids large fluid shifts and IDH. A large retrospective study of over 120,000 patients supported this by demonstrating a lower incidence of dementia in a PD cohort when compared with people on HD (PD vs HD: 3.9% (95% CI [3.3%, 4.4%]) vs 7.3% (95% CI [7.1%, 7.4%])) [27]. A subsequent direct comparison of cognitive function in 41 HD patients and 25 PD patients found that Montreal Cognitive Assessment (MoCA) scores declined more rapidly in the HD cohort over the two-year study period (coefficient = –0.12; 95% CI, –0.233 to –0.007, p = 0.037). The study also noted that cognition declined faster in those on any form of dialysis (HD or PD) when compared to people with CKD not on dialysis (coefficient = –0.03; 95% CI, –0.056 to –0.004, p = 0.025) [28]. This could suggest that severe CI may be seen as a relative contraindication to any form of KRT.
However, CI in PD patients can lead to frequent hospital admissions and increased peritonitis rates [29]. This highlights the complex interplay of the frailty syndromes and the challenges experienced by clinicians. CI should not just be viewed as an eventuality of ageing. Multi-disciplinary team (MDT) assessment of elderly patients with CI should evaluate the individual’s baseline cognition and level of function in order to determine which dialysis modality is best. Assessment by a geriatrician and/or referral to a memory clinic may also be sought. A preference for PD, if there is pre-existing dementia, can be appropriate, but it would likely be delivered via an assisted programme to ensure optimal care.
Multiple studies have shown that there may be no survival advantage to any dialysis modality for frail, elderly individuals [30, 31, 32], making survival a secondary consideration in discussions of KRT. Instead, quality of life is more likely to be prioritized [33] and can be influenced by frailty and cognitive impairment as already discussed. What contributes to a person’s quality of life should be explored to determine the goals of the individual and their expectations of treatment.
A recent study conducted a choice experiment which found that older people aged
Quality of life was examined in the Broadening Options for Long-term Dialysis in the Elderly (BOLDE) study, which compared cohorts of patients aged 65 years and over on HD versus PD [36]. Despite no difference in quality of life outcome measures, perception of illness intrusion (p = 0.006) and feelings of depression (p = 0.015) were less in the group on PD. Whilst treatment burden can be significant in home-based therapy, this study suggested that people found treatment with PD less invasive.
Despite some older people prioritizing a reduction in symptom burden in end-stage kidney disease (ESKD), it is important to acknowledge that PD often does not result in a total resolution of symptoms. Oedema can be improved; however, fatigue can persist despite starting PD [37]. Limitations of treatment should be clearly communicated.
PD can also be tailored to adapt to the specific needs of the individual via an incremental regimen. This step-wise approach to PD enables a gradual increase in their prescription over time as dictated primarily by symptoms, thus allowing for preservation of their residual kidney function [38]. This enables greater flexibility with the dialysis prescription whereby dialysis days can be altered to accommodate hospital appointments and social events; things that older people may prioritize more readily.
Further PD actively encourages people to be involved in delivery of their own care through performing daily exchanges or attaching themselves to the overnight cycler machine used in automated peritoneal dialysis (APD). This contributes to an increased sense of autonomy whilst remaining in a familiar home environment in close contact with family and friends [39]. Older people on PD may also act as carers for spouses or children, and so being at home is integral for them to continue in their role. These lifestyle advantages of PD can mean less frequent hospital visits and an enhanced overall well-being for patients.
Ageing and frailty may present problems with cognition and dexterity, which may in turn impact a person’s ability to carry out their own PD. In such scenarios, assisted PD is a valuable resource which can be utilised to enable ongoing dialysis at home. Assisted PD can include help from registered nurses, healthcare assistants and dialysis technicians as well as trained carers. People may initially perform independent continuous ambulatory peritoneal dialysis (CAPD) or APD before gaining assistance, or commence directly onto assisted PD. A switch from independent PD to assisted PD is often due to intercurrent events or a change in social circumstances, and can be preferable compared to transferring to HD. This flexibility makes PD a viable option for many old, frail people; some of whom may have foregone dialysis altogether had this option not been available. It may also be used as a bridge to self-care PD in the old, frail person where longer training time and support from community teams is required [40].
Assisted PD can also be provided by friends and family. These caregivers should therefore be involved in shared decision-making when discussing KRT. It is also necessary to recognise carer burnout, and assisted PD can be implemented to provide temporary respite if needed. Opposingly, older people may have reduced social support but still wish to pursue a home-based therapy. The benefits and flexibility of assisted PD and the role of the family are illustrated in the case discussion in Table 1.
| An 80-year-old male |
| Background: CKD, hypertension, type 2 diabetes mellitus |
| Mr C was an 80-year-old man with a background of CKD, hypertension and type 2 diabetes mellitus. He was regularly reviewed in the advanced kidney care clinic; however, his kidney disease progressed despite optimal CKD treatment. Having reached end-stage kidney disease, Mr C’s main goals of treatment were to remain at home and be involved with the care of his grandchildren. With the support of his clinic team, he opted to begin KRT with CAPD. Both Mr C and his family felt that he would benefit from assistance in the form of PD technicians to help with his treatment, and this was supported by the MDT. |
| He began assisted CAPD a number of weeks later, which consisted of two visits per day by the technicians to perform his dialysis. This was done five days per week, allowing Mr C two days without needing to have dialysis and giving him greater freedom and flexibility to pick his grandchildren up from school. |
| Mr C engaged well with the home therapies team over the years, and felt his symptoms were alleviated by ongoing PD. It was noted by his relatives and clinic team, however, that he was experiencing some issues with his memory and he was becoming increasingly frail. The relatives told how there were occasional episodes of him turning away unfamiliar PD technicians who visited his house, but he was much more comfortable with the ones he had formed a good rapport with over the years. It was also noted he had significant oedema, and so his PD prescription was increased to seven days per week with good effect. |
| Despite these concerns, it was felt he had a good quality of life on PD. Involvement of the wider MDT focused on treatment trajectory and prognosis, with conversations had about advanced care planning and resuscitation. Mr C maintained his wish to remain at home and that he was happy to continue PD so long as he felt it was working for him. |
| Mr C’s dementia progressed, and he now needed a care package to help with his activities of daily living. His appetite was poor and he was increasingly agitated. His relatives highlighted during a community visit from the home therapies team that they were now struggling to manage him at home, and had started to look at nursing homes for him. There were more days when he was not opening the door for the PD technicians, and so having less and less dialysis. |
| Unfortunately, just a few weeks later, Mr C had a fall at home and was admitted to hospital. On the renal ward, his severely frail state was noted. Following a best interests meeting with the family and his usual outpatient team, his PD was stopped. He was subsequently fast-tracked to a nursing home where he died two weeks later. |
| Assisted PD enabled Mr C to have autonomy over his kidney disease; allowing him to continue to be at home and see his grandchildren regularly. During 6 years on PD, Mr C had no hospital admissions until he experienced falls and progressive dementia towards the end of his life. Had assisted PD not been available, Mr C would have likely defaulted to HD, meaning thrice-weekly visits to a dialysis unit and cutting into time spent at home. The challenges in this case were managing his progressive cognitive impairment, ensuring he remained safe and that ongoing PD was in his best interests. Continuous discussions with his relatives and involvement of the MDT allowed regular review of his treatment, ensuring patient-centred care. |
KRT, kidney replacement therapy; MDT, multi-disciplinary team; CAPD, continuous ambulatory peritoneal dialysis.
Funding and healthcare policies are significant barriers to the provision of assisted PD. Wide variations are seen nationally and internationally—across Europe, 40% of units providing PD were found to have no access to a formal assisted service [41]. Formal assisted programmes differ within the UK also. Assistants can be employed directly by National Health Service (NHS) trusts or organised by a partnership between commercial dialysis providers and healthcare agencies. France was one of the first countries to roll out a government-funded assisted PD programme where registered nurses are trained to undertake the PD, as well as providing catheter care and monitoring of blood pressure and fluid status. This facility has since been extended to nursing homes, providing a true holistic service [42]. Table 2 (Ref. [12, 40, 42, 43]) summarises the differing models for delivering assisted PD globally.
| Country | Description |
| Delivered by registered nurse | |
| France [42] | National model with government funding |
| Services offered—connect-disconnect service for APD, manual CAPD exchanges | |
| Up to 4 visits per day | |
| Also trained to provide exit site care and patient monitoring, e.g., blood pressure | |
| Denmark [42] | Public funding |
| Registered nurse or healthcare technician trained by PD nurses | |
| Connect-disconnect service for APD | |
| Also trained to provide exit site care and order equipment | |
| Canada [40] | Funding via government health insurance |
| Connect-disconnect service for APD | |
| Delivery of CAPD exchanges varies across provinces | |
| Delivered by non-registered practitioner or technician | |
| UK [12, 43] | APD more frequently offered than CAPD |
| Often once daily visit—morning disconnect service for APD and set up of machine for next use | |
| Patient or relative performs their own connection in the evening | |
PD, peritoneal dialysis; APD, automated peritoneal dialysis; CAPD, continuous ambulatory peritoneal dialysis.
Assisted programmes have allowed an expansion in accessibility to PD where it may not have been a viable treatment option previously. It also presents a balance of autonomy and appropriate support to ensure the goals and wishes of the individual are not compromised. The use of assisted PD has also been demonstrated to reduce the need for modality switch to HD in the elderly [44] and increase incident PD numbers in the elderly population [45]. Palliative use of assisted PD is another option for those people who elect to continue PD but do not have the capability themselves [46]. As such, early consideration and ongoing review of the need for assistance should be encouraged when reviewing old, frail people. However, this can only be appropriately done if the local programmes are funded and staffed appropriately.
The ageing population has dictated focused cost analysis of KRT in order to drive further improvements in service design and accessibility of treatment for patients. In 2023, dialysis costs in the UK totalled £1.05 billion, with an additional £225 million spent on transport to haemodialysis [47]. The cost of CAPD and APD is less than in-centre HD, and without transport costs [48]. Assisted PD has also been demonstrated to be highly cost-effective compared to HD, even when providing this service to those in long-term care facilities [49]. Financial incentives to increase numbers on PD have been employed in other countries [50], but this is less relevant in the UK given the publicly funded structure of the NHS. The rising economic implications of CKD, ESKD and KRT could therefore be alleviated by an increase in the proportion of the elderly on PD.
Potential challenges of PD should also be considered, and are summarised in
Table 3. Peritonitis is a significant complication and its risk remains
controversial. One study showed similar peritonitis rates between age groups,
with an incidence of peritonitis of 1 episode per 23.6 patient-months in those
aged
| Patient factors | Treatment factors | Healthcare factors |
| • Visual impairment | • Treatment fatigue | • Lack of understanding of PD, thus not discussed early on when planning KRT |
| • Cognitive impairment | • Carer burnout | • Lack of training for resident doctors |
| • Dexterity issues, including arthritis | • Adherence issues | • Lack of funding for assisted PD programmes |
| • Sarcopaenia and reduced muscle strength, unable to lift bags | • Less social engagement compared to in-centre HD | |
| • Reduced mobility | • Issues with fluid removal | |
| • Frailty | • Persistence of symptoms of ESKD despite PD | |
| • Communication issues | • Fewer financial incentives for PD | |
| • Need for assistance |
HD, haemodialysis; PD, peritoneal dialysis; ESKD, end-stage kidney disease; KRT, kidney replacement therapy.
Another consideration is the repetitive nature of PD. Patients often carry out 2–3 exchanges per day which can contribute to a significant treatment burden. In turn, this may negatively impact on perceived quality of life, alongside carer burnout if family assistance is heavily relied upon. To mitigate this, incremental regimens and preservation of residual kidney function allow for dialysis flexibility with scheduled days off as needed [57]. Assisted PD further helps to reduce dependency on relatives.
In-centre HD may also be a good option for older people who physically cannot do their own PD for reasons of dexterity or mobility, or if they are limited by visual or cognitive impairment. There also may be positive impacts of HD which a frail, elderly person may find encouraging. Loneliness in the elderly is a growing problem and the benefit of regular social contact within a dialysis unit should not be overlooked, particularly for those people who live alone [58]. Further, modality change to HD may be seen for PD patients with infection, catheter dysfunction and ultrafiltration failure [59].
However, HD presents a different set of problems, including vascular access issues [60], rigid weekly schedules [61] and extra time spent on hospital transport [62]. Weighing up the benefits and burdens of each modality is therefore important to ensure an individualised treatment plan.
Maximal conservative management, whereby medications are used in place of dialysis treatments to manage symptoms of ESKD, should also be considered where appropriate. Elderly patients starting dialysis can experience only marginal improvements in life expectancy with less time spent at home [63]. When considering this alongside frailty and other comorbidities, PD may still be too burdensome for some. In this scenario, early involvement of the palliative care teams is paramount to ensuring patient-centred care with clear decisions around advanced care planning and resuscitation.
Decisions around KRT in the old, frail population can be complex. However, where appropriate, PD offers a home-based treatment that can be flexible to suit the needs of the individual. The goals of treatment of the older person are less likely to be centred on survival, and may instead focus on quality of life, treatment satisfaction and maintenance of independence. These aims are well aligned with what PD offers as a dialysis modality, and are also supported by numerous large cohort studies. The impact of cognition and frailty should be closely examined and discussed with both the person and the wider MDT to ensure individualised care. When challenges are identified that may hinder the delivery of PD in elderly patients, assisted PD should be considered to help to maintain their independence and continue with their dialysis.
Looking to the future, the role of assisted PD programmes is likely to become more important with an ageing population and the increasing prevalence of frailty. The economic benefits of PD should also be evaluated as the pressure on HD units continues to rise. As such, there is a need for improved funding and restructuring of services to enable the development and provision of assisted programmes across the UK. Sharing of models of care between renal units to enhance learning should be encouraged. Further, external funding options from private dialysis companies should be considered for the provision of staff and training to enable this treatment option to be offered more readily to those who require it.
All the data of this study are included in this article.
Both JS and EAB contributed to the conception, design, writing and editing of this review article. Both authors have reviewed and approved the final manuscript. Both authors agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
The information of the case discussed is anonymous and the verbal consent was obtained from the next of kin.
Not applicable.
This research received no external funding.
Figs. 1,2 was created using Canva (https://www.canva.com). The authors have no financial or personal relationship with Canva, and the use of this tool does not imply any endorsement. Edwina A Brown is on the advisory board and receives speaker fees from Fresenius Medical Care, as well as speaker fees from Baxter Healthcare. Jessica Selwood declares no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.