

 , Yanting Wang 1, Xiluo Xu 1, Fuquan Long 1,*
, Yanting Wang 1, Xiluo Xu 1, Fuquan Long 1,* , Lin Zhu 1,*
, Lin Zhu 1,*1 Department of Sexually Transmitted Diseases, Shanghai Skin Disease Hospital, Tongji University School of Medicine, 200433 Shanghai, China
Abstract
Cerebrospinal fluid (CSF) is a crucial type of biological specimen for neurosyphilis diagnosis. This study aims to comprehensively analyse the clinical manifestations and risk factors of adverse reactions in syphilis patients following lumbar puncture (LP).
A total of 573 syphilis patients who underwent LP examinations between August 2023 and April 2024 at the Department of Sexually Transmitted Diseases, Shanghai Skin Disease Hospital, were selected. The clinical manifestations, onset timing, risk factors, and duration of relief from adverse reactions in these patients undergoing LP were statistically analysed.
Among 573 patients diagnosed with syphilis, 142 patients (24.8%) experienced adverse reactions following LP. Factors such as age, needle size, symptoms of paralysis, and the duration of postoperative bed rest were significantly associated with adverse reactions after LP (p < 0.05). Furthermore, age >30 years, the use of a 20G needle, and paralysis symptoms were identified as independent protective factors (p < 0.05), whereas bed rest duration >6 hours contributed to increased risk for adverse reactions (odds ratio [OR] = 3.544, p = 0.010). The average onset time for adverse reactions following LP was 14.34 ± 1.54 hours, while the average duration for resolution of these reactions was 5.52 ± 0.26 days postoperatively.
The high incidence of adverse reactions following LP in patients with syphilis poses challenges to restoring quality of life among affected patients. A thorough assessment of risk factors for adverse reactions could inform the selection of appropriate measures to mitigate the occurrence of such reactions.
Keywords
- syphilis
- spinal puncture
- postoperative complications
- risk factors
Syphilis is a chronic sexually transmitted disease caused by an infection with Treponema pallidum. Neurosyphilis is an irreversible disease caused by the invasion of Treponema pallidum into the central nervous system, leading to brain parenchyma destruction and central nervous system impairment [1, 2]. Lumbar puncture (LP) remains the gold-standard diagnostic procedure for neurosyphilis. However, post-LP adverse reactions, particularly post-dural puncture headache (PDPH), remain a significant clinical challenge across various populations, with reported incidence rates ranging from 10% to 40% [3, 4].
At present, the risk factors for post-LP adverse reactions remain undetermined in existing literature. Among the key determinants for the post-LP adverse reactions that have been investigated are needle size [5, 6], patient positioning [7, 8], body mass index (BMI) [5, 9, 10], and fluid replacement volume [11]. Notably, there is limited data specifically addressing syphilis patients, who may present unique characteristics due to potential central nervous system involvement. Given this knowledge gap, the current study aims to systematically evaluate the incidence, clinical manifestations, and risk factors of post-LP adverse reactions in syphilis patients.
This retrospective cohort study analysed data from 573 syphilis patients undergoing diagnostic LP at the Department of Sexually Transmitted Diseases, Shanghai Skin Disease Hospital, between August 2023 and April 2024. Clinical basic data of patients were collected with Hospital Information System (HIS) and Nursing Information System (NIS), including gender, age, height, weight, bed number, hospital number, name, admission diagnosis, and BMI [12].
The inclusion criteria are as follows: (i) syphilis patients undergoing LP
examination; (ii) patients or their family members who provided informed consent;
(iii) patients who were conscious and capable of conducting normal communication
and (iv) patients with no history of chronic headaches (to avoid confounding with
pre-existing headache conditions). Exclusion criteria of this study include: (i)
incomplete clinical data; (ii) malignant tumours; (iii) contraindications for LP
and (iv) age
All procedures were performed by experienced clinicians following a standardised protocol: patients in the lateral decubitus position with flexed knees, and LP was performed at the L4–L5 interspace under strict aseptic technique using either 20G (0.9 mm) or 18G (1.2 mm) needles.
Adverse reactions are defined as any new-onset symptoms within 96 hours post-LP, including headache, dizziness, nausea, vomiting, or back pain, as documented in medical records or reported during follow-up calls at 24 hours, 48 hours, and 7 days post-LP. Symptom severity was graded as mild (not interfering with daily activities), moderate (limiting but not preventing activities), or severe (requiring bed rest).
Continuous variables are presented as mean
Among 573 patients (372 males, 201 females; mean age 55.4
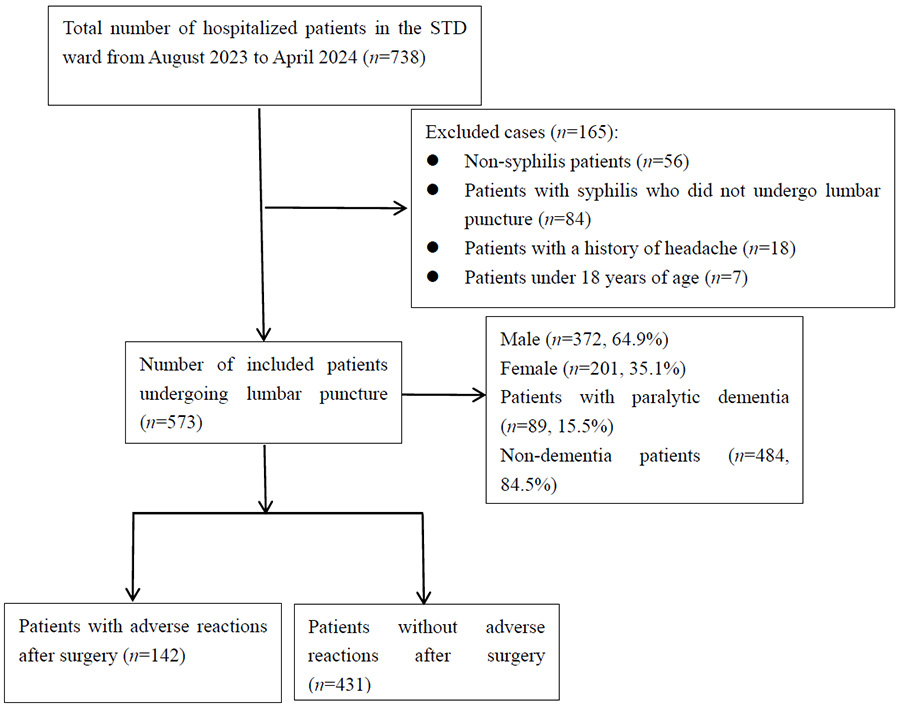 Fig. 1.
Fig. 1.
Flowchart depicting selection and inclusion of syphilis patients undergoing lumbar puncture. STD, Sexually Transmitted Diseases.
The most common adverse reactions were isolated headache/dizziness (38.7%) and isolated back pain (38.0%), nausea/vomiting (2.8%), headache/dizziness with nausea/vomiting (10.6%), headache/dizziness with back pain (9.2%), and multisystem involvement (0.7%) (Table 1).
| Clinical manifestation | n | % |
| Headache/Dizziness | 55 | 38.7 |
| Isolated back pain | 54 | 38.0 |
| Nausea/Vomiting | 4 | 2.8 |
| Headache/Dizziness + Nausea/Vomiting | 15 | 10.6 |
| Headache/Dizziness + Back pain | 13 | 9.2 |
| Multisystem involvement* | 1 | 0.7 |
Note: *Clinical manifestations with multisystem involvement include headache/dizziness, nausea/vomiting, and back pain.
The results of the univariate analysis of adverse reactions after LP in 573
syphilis patients showed that age, needle type, symptoms of paralytic dementia,
and postoperative bed rest time were significant influencing factors for adverse
reactions after the operation (p
| Variable | Category | Without adverse reactions (n = 431) | With adverse reactions (n = 142) | p-value | |
| Demographics | |||||
| Gender | Male | 288 (66.8%) | 84 (59.2%) | 2.757 | 0.097 |
| Female | 143 (33.2%) | 58 (40.8%) | |||
| Procedural factors | |||||
| Needle gauge | 20G (0.9 mm) | 274 (63.6%) | 74 (52.1%) | 5.882 | 0.015* |
| 18G (1.2 mm) | 157 (36.4%) | 68 (47.9%) | |||
| First ambulation time | 0–2 hours | 8 (1.9%) | 9 (6.4%) | 33.842 | |
| 2–4 hours | 22 (5.1%) | 22 (15.5%) | |||
| 4–6 hours | 391 (90.7%) | 101 (71.1%) | |||
| 10 (2.3%) | 10 (7.0%) | ||||
| Clinical factors | |||||
| Diagnosis at admission | Non-dementia** | 349 (81.0%) | 135 (95.1%) | 16.176 | |
| Dementia*** | 82 (19.0%) | 7 (4.9%) | |||
| Age group (years) | 35 (8.1%) | 23 (16.2%) | 18.713 | ||
| 31–59 | 166 (38.5%) | 71 (50.0%) | |||
| 230 (53.4%) | 48 (33.8%) | ||||
| BMI category ( |
Underweight ( |
17 (3.9%) | 9 (6.4%) | 2.075 | 0.354 |
| Normal (18.5–23.9) | 226 (52.5%) | 78 (54.9%) | |||
| Overweight ( |
188 (43.6%) | 55 (38.7%) | |||
| Fluid intake | |||||
| 24-hour volume (mL) | 262 (60.8%) | 78 (54.9%) | 1.520 | 0.218 | |
| 169 (39.2%) | 64 (45.1%) | ||||
| Substance use | |||||
| Smoking status | Yes | 90 (20.9%) | 31 (21.8%) | 0.058 | 0.810 |
| No | 341 (79.1%) | 111 (78.2%) | |||
| Alcohol consumption | Yes | 96 (22.3%) | 37 (26.1%) | 0.857 | 0.355 |
| No | 335 (77.7%) | 105 (73.9%) | |||
| Education | |||||
| Highest level attained | Below college | 229 (53.1%) | 72 (50.7%) | 0.253 | 0.615 |
| College or above | 202 (46.9%) | 70 (49.3%) | |||
| Postoperative care | |||||
| Prolonged standing ( |
Yes | 207 (48.0%) | 75 (52.8%) | 0.980 | 0.322 |
| No | 224 (52.0%) | 67 (47.2%) |
Note: *Statistically significant (p
According to the multivariate analysis results (Table 3), the risk for adverse
reactions was significantly lower in those within the age groups of 31–59 years
(odds ratio [OR]: 0.351, 95% confidence interval [CI]: 0.184–0.669, p
= 0.001) and
| Factor | Wald |
p-value | Adjusted OR (95% CI) | ||
| Age group (years) | 13.258 | ||||
| - | - | - | 1.00 | ||
| 31–59 | –1.048 (0.330) | 10.088 | 0.001* | 0.351 (0.184–0.669) | |
| –0.653 (0.227) | 8.294 | 0.004* | 0.521 (0.334–0.812) | ||
| Diagnosis at admission | |||||
| Non-dementia (reference) | - | - | - | 1.00 | |
| Dementia | –1.549 (0.437) | 12.573 | 0.212 (0.090–0.500) | ||
| Needle gauge | |||||
| 20G (reference) | - | - | - | 1.00 | |
| 18G | 0.491 (0.209) | 5.507 | 0.019* | 1.634 (1.084–2.461) | |
| First ambulation time (hours) | 31.486 | ||||
| 0–2 (reference) | - | - | - | 1.00 | |
| 2–4 | –0.587 (0.722) | 0.662 | 0.416 | 0.556 (0.135–2.287) | |
| 4–6 | –0.173 (0.574) | 0.090 | 0.764 | 0.841 (0.273–2.593) | |
| 1.265 (0.489) | 6.701 | 0.010* | 3.544 (1.360–9.239) | ||
Note: *Statistically significant (p
Among the 142 syphilis patients who had received LP, the shortest time to onset
of adverse reactions was 1 hour post-operation, while the longest was 96 hours
post-operation, with an average onset time of 14.34
| Parameter | Minimum | Maximum | Mean |
| Time to adverse reaction onset (hours) | 1 | 96 | 14.34 |
| Duration of adverse reaction relief (days) | 1 | 16 | 5.52 |
Note: SD, standard deviation.
LP is an essential diagnostic tool for neurological diseases, with primary diagnostic indications including infectious diseases, inflammation, and related conditions affecting the central nervous system [13, 14]. In our department, syphilis patients constitute 95% of the inpatients, and thus, LP stands as an essential approach to distinguishing patients with syphilis from those with neurosyphilis. PDPH is a widely recognised common complication after LP, with symptoms including neck stiffness, lower back soreness, nausea, vomiting, as well as ear and eye symptoms [15]. PDPH is a typical positional headache that worsens when the patient is upright and improves or resolves when lying flat, typically lasting for several days with severity ranging from mild to debilitating; in severe cases, medical intervention may be required [16, 17, 18]. Post-procedural lower back soreness and pain refer to pain around the puncture site in the spine [19]. According to several studies, the occurrence rates of PDPH range from 3% to 30% [11, 20]. Meanwhile, our research findings indicate that 24.8% of syphilis patients experienced adverse reactions following an LP, with headache/dizziness being the most common adverse reaction, occurring in 59.2% of cases, followed by back pain noted in 47.9% of the cases.
Our research results indicated that the thickness of the puncture needle influences the occurrence of post-LP adverse reactions. Specifically, the use of an 18G puncture needle (1.2 mm) relative to a 20G needle (0.9 mm) increased the risk of post-procedural adverse reactions, consistent with the findings of Azzi et al. [3] and Destrebecq et al. [21], who recommended that smaller needles could significantly reduce the incidence of PDPH. This may be attributed to reduced dural trauma associated with a smaller skin puncture created by a finer needle [22, 23, 24], which can result in slower cerebrospinal fluid outflow during the procedure and a lower risk of post-procedural leakage at the puncture site. Therefore, smaller-gauge needles are recommended for use during the LP procedures in order to reduce the occurrence of adverse reactions in patients.
This study demonstrated that the likelihood of adverse reactions following LP decreased with advancing age. This finding contrasts with several previous reports indicating a lower rate of PDPH in patients with cognitive impairment and a higher incidence of post-procedural adverse reactions in younger populations—patterns that align with the observed rarity of such reactions in both infants and the elderly [25, 26, 27]. This trend may be attributed to the decline in cognitive impairment or the gradual onset of brain atrophy with advancing age. Additionally, it has been reported that older age acts as a protective factor against post-LP headaches [11, 28, 29].
Patients with paralytic dementia exhibit abnormal mental and behavioural symptoms, such as lack of concentration, forgetfulness, reduced judgment and memory, cognitive impairment, dementia, mood swings, depression, personality changes, delusions, mania, or psychosis [2, 30]. The results of this study indicate that symptoms of paralytic dementia act as a protective factor against adverse reactions after LP. El-Mallakh et al. [31] reported that post-LP headaches are less frequent and severe in patients with schizophrenia compared to normal individuals, due to the reduced pain perception in mentally ill patients (i.e., higher pain threshold) [32] and decreased ability to verbally express pain (i.e., reduced tendency to complain) [33]. This aligns with our research findings, although the exact mechanisms remain unclear.
In the current clinical practice, patients are typically advised to lie flat without a pillow for 4–6 hours after LP for the reason of reducing the risk of adverse reactions. However, our study found that bed rest exceeding 6 hours was associated with an increased incidence of postoperative adverse reactions.
The adverse reaction may arise from prolonged immobilisation, coupled with
anxiety toward postoperative complications, which eventually causes sleep
disruptions. Extended bed rest can also lead to muscle tension, hindering
relaxation and resulting in lower back pain and soreness. Furthermore, patients
who remain supine without pillows for more than 6 hours typically exhibit
decreased water intake compared to their more active counterparts, and the
production rate of cerebrospinal fluid is also diminished. In contrast to other
studies, our findings suggest that post-LP bed rest, regardless of the duration,
does not contribute to lowered incidence of PDPH [34, 35]. Specifically, our results contradict the findings
of Zhang [36], which indicate that haematology patients who took rest for
There are several limitations in this study. Firstly, this was a single-center study with a small sample size; therefore, additional multi-center studies with larger cohorts are needed in the future. In addition, several critical variables, such as syphilis stage, patient complications, disease course, and type of treatment, were not considered in our analysis, and it is currently unknown if the collection speed of cerebrospinal fluid during LP would affect the incidence of postoperative complications. Therefore, an in-depth study of the above-mentioned factors is warranted in the future.
Our study provides several novel insights into post-LP adverse reactions, which
impact approximately one-quarter (24.8%) of syphilis patients. These reactions
primarily manifest as headache/dizziness (59.2%) or back pain (47.9%), possibly
indicating unique pathophysiological changes in the meninges of syphilis
patients. The use of small-gauge needles (20G), age
The datasets generated during and/or analysed during the current study are available from the corresponding authors upon reasonable request.
Conceptualization: JY, LZ, YW, FL; Methodology: LZ, FL; Formal analysis and investigation: JY, YW, XX; Writing—original draft preparation: JY, LZ, YW, FL; Writing—review and editing: LZ. All authors contributed to the important editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
This study adhered to the Declaration of Helsinki and received approval from the Ethics Committee of Shanghai Skin Disease Hospital (approval number: 2024-37). Written informed consent was obtained from all participants, and all data used for research analyses were anonymised.
Not applicable.
This research received no external funding.
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.