


 , Jianhui Xu 1, Lianying Wang 1
, Jianhui Xu 1, Lianying Wang 11 Department of Ophthalmology, The First People’s Hospital of Chun’an County, 311700 Hangzhou, Zhejiang, China
Abstract
Meibomian gland dysfunction (MGD)-related dry eye results in reduced tears, unstable tear film, ocular surface damage, and even causes keratitis. Demodex infection causes inflammatory diseases of the ocular surface. This study aimed to explore the impact of Demodex infection on the occurrence and prognosis of keratitis in patients with MGD-related dry eye.
A total of 122 MGD patients who visited the Department of Ophthalmology, The First People’s Hospital of Chun’an County from June 2022 to June 2023 were selected for retrospective study. Patients were divided into keratitis group (n = 65) and non-keratitis group (n = 57) according to the presence of keratitis. MGD patients with keratitis were followed up for one year, and divided into good prognosis group (n = 36) and poor prognosis group (n = 29) based on their prognosis. The Demodex infection status and ocular surface parameters were detected in these two groups of patients. Logistic regression was adopted to analyze the influencing factors of keratitis complicated with MGD.
The positive rate of Demodex infection in the keratitis group was 81.5%, which was significantly higher than that in the non-keratitis group (35.1%, p < 0.05). Compared with non-keratitis group, keratitis group had reduced tear film break-up time (BUT), and increased corneal fluorescein staining (CFS), meibomian gland (MG) dropout, and plugging of MG orifices (p < 0.05). Logistic multivariate regression analysis showed that Demodex infection (odds ratio [OR]: 6.209, 95% confidence interval [CI]: 2.101–18.348), CFS (OR: 2.627, 95% CI: 1.562–4.416) and plugging of MG orifices (OR: 3.174, 95% CI: 1.616–6.235) were independent risk factors for keratitis in patients with MGD-related dry eye (p < 0.05), and BUT (OR: 0.768, 95% CI: 0.606–0.972) was a protective factor (p < 0.05). The age and MG expression in the good prognosis group were lower than those in the poor prognosis group (p < 0.05). No significant difference was observed between the good prognosis and poor prognosis groups in patients with Demodex infection (p > 0.05).
The positive rate of Demodex infection is higher in patients with MGD combined with keratitis. Demodex infection, CFS and plugging of MG orifices are independent risk factors for keratitis, while the tear film BUT is a protective factor in MGD-related dry eye patients. Demodex infection does not affect the prognosis of keratitis.
Keywords
- mite
- keratitis
- meibomian gland dysfunction
- dry eye
Meibomian gland (MG) is a special type of sebaceous gland located in the eyelid meibomian plate. The fat secreted by MG is the main component of the lipid layer on the surface of the tear film, which can promote the stability of the tear film and maintain the health of eye surface [1]. Meibomian gland dysfunction (MGD) is the most common ocular surface disease in clinical setting, giving rise to symptoms such as redness, itching, irritation, dryness, decreased vision, and tearing. It is usually characterized by terminal duct obstruction and/or qualitative/quantitative changes in the glandular secretion [2]. MGD can cause abnormal tear film and ocular surface inflammation [3]. It was reported that MGD was also the main cause of various types of ocular surface diseases, such as dry eye disease, eyelid-associated keratoconjunctivitis, and keratitis [1, 4, 5]. MGD-related dry eye could experience reduced tears, unstable tear film, ocular surface damage, and even cause keratitis [1]. Keratitis is the main cause of blindness, and most vision loss caused by keratitis can be avoided through early detection and treatment [6, 7]. However, the pathological mechanism and influencing factors of keratitis are complex and remain to be elucidated.
Demodex is widely prevalent parasites that primarily feed on secreted oils. Researches have shown that Demodex infection of the eyelids was significantly associated with MGD, ocular surface inflammation, and blepharokeratoconjunctivitis [8, 9]. Previous study reported that Demodex infection was a risk factor of MGD [10]. In addition to causing direct damage to epithelial cells of the hair follicle, Demodex infection also could cause marginal corneal infiltration, phlyctenule-like lesions, and superficial corneal opacity [11, 12, 13]. Meanwhile, Demodex can carry concomitant bacteria (such as Streptococci and Staphylococci), which are capable of producing antigens and triggering immune response [14]. In addition, the metabolic byproducts of Demodex can trigger an inflammatory cascade by activating Toll-like receptor 2 (TLR2) innate immune pathway, leading to up-regulation of inflammatory cells and pro-inflammatory factors [15]. Overall, Demodex infection is associated with the inflammatory diseases of the ocular surface. Exploring the correlation between Demodex infection and MGD, a previous study found that the infection was an influencing factor for MGD, particularly prominent in elderly patients aged 41 to 70 years [16]. As studies that explore the impact of Demodex infection on the development and prognosis of keratitis remain scarce, it is still unclear whether Demodex contributed to the occurrence of keratitis in MGD patients. Thus, this study was designed to retrospectively analyze clinical data of patients with MGD-related dry eye, aiming to clarify the relationship between Demodex infection and the occurrence, clinical characteristics, and prognosis of keratitis. This study will provide a basis for the clinical diagnosis and treatment of MGD combined with keratitis.
A total of 122 patients with MGD-related dry eye who visited the Department of
Ophthalmology, The First People’s Hospital of Chun’an County from June 2022 to
June 2023 were selected for this retrospective study. This study was approved by
The First People’s Hospital of Chun’an County Ethics Committee (Approval No.
2024-04-12-06) and was conducted in compliance with the Declaration of Helsinki.
Informed consent was obtained from all patients. MGD patients were divided into
keratitis group (n = 65) and non-keratitis group (n = 57)
according to whether or not they developed keratitis. A keratitis diagnosis was
verified based on a combination of diagnostic tests, including assessment of
clinical symptoms, slit lamp examination, and laboratory findings
[17]. Patients who satisfied the following criteria
were included in the study: (1) meeting the diagnostic criteria for MGD-related
dry eye [18]; (2)
having complete clinical data; and (3) aged
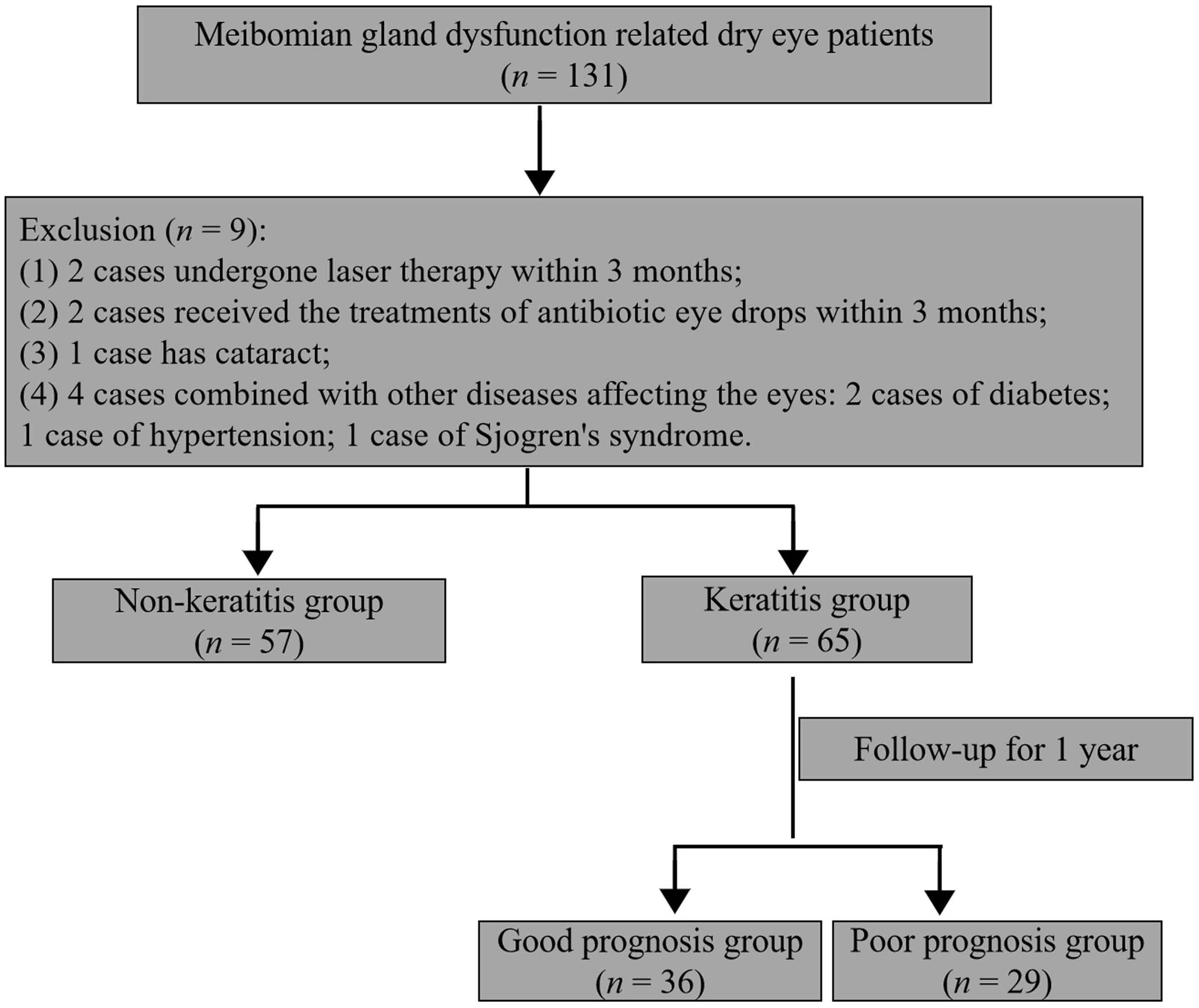 Fig. 1.
Fig. 1.
Flowchart depicting patient inclusion and exclusion.
Three eyelashes were obtained from the upper and lower eyelids of patients,
respectively. The samples were observed under a microscope (10
The clinical information of patients, including gender, age, course of disease, history of eye trauma/burns, eye make-up, usage of contact lenses, and admission time were collected. All patients underwent ophthalmic examinations, which covered ocular surface disease index (OSDI), tear film break-up time (BUT), corneal fluorescein staining (CFS), Schirmer I test (SIT) and MG examination. The ophthalmic examinations of all patients were conducted under blinded conditions by an experienced ophthalmologist (7 years of clinical experience in ophthalmology) following standardized protocols.
The OSDI was used to diagnose patients with dry eye and evaluate the severity of the condition [20]. With a score range of 0–100, a higher score represents greater disability.
The measurement of BUT requires dropping 0.5% fluorescein sodium into the conjunctival sac of patients, who were then asked to blink several times. The appearance time of the first dry spot was recorded. The measurement was repeated three times and the average value was calculated [21].
CFS test was carried out to evaluate cornea damage [22]. The fluorescein sodium was dropped into the conjunctival sac, and the cornea were observed using a slit-lamp. The cornea was separated into four quadrants, with each quadrant scored from a range of 0–3 points according to National Eye Institute (NEI) scoring system (0 = no staining, 3 = severe). The test had a maximum of 12 points [23].
SIT was performed using a 5 mm
MG examination encompasses MG dropout, plugging of MG orifice, and MG
expression. Keratograph 5M (Oculus, Wetzlar, Germany) was used for the assessment
of MG. (1) MG dropout: 0–3 points for each eyelid: 0 = no loss; 1 = MG loss of
less than 1/3 area; 2 = MG loss between 1/3 and 2/3 area; 3 = MG loss of more
than 2/3 area. The average score of the upper and lower eyelids was calculated
[22]. (2) The plugging of MG orifices: 0–3 points for
each eyelid, 0 = no plugging; 1 = plugging
For dry eye, the patients were treated with sodium hyaluronate eye drops (H201 73249, Santen Pharmaceutical, Osaka, Japan) 4 times daily for a consecutive 4 weeks. Meanwhile, they received fumigation and MG massage once a week for 4 weeks. Specifically, an atomizer was used for fumigation for 15–20 min. After fumigation, MG massage was performed on the meibomian gland to unblock MG. For individuals with Demodex infection, Tea Tree Oil Professional Mite Removal Wipes (OcuSOFT, Beijing, China) were used to clean the roots of the eyelashes and eyelids of patients. Specifically, after cleaning the eyelids, patients apply a wet compress for 10–15 minutes, twice daily for 4 weeks. Keratitis was treated with medications to ameliorate inflammation. Among the drugs for keratitis treatment are levofloxacin eye drop (H20203122, Wanhan Pharmaceutical, Zhongshan, China), pranoprofen eye drop (H20130682, Senju Pharmaceutical, Osaka, Japan), and tobramycin dexamethasone eye drop (H20150119, Alcon NV, Puurs-Sint-Amands, Belgium), which should be chosen based on the patient’s condition.
MGD patients with keratitis (n = 65) discharged from the hospital were followed up for 1 year, with a follow-up every 3 months. The follow-up entailed recording the clinical symptoms of the patient’s eyes and examining the corneal condition. The patients were categorized into a good prognosis group and a poor prognosis group according to the results of follow-up. Patients in the good prognosis group (n = 36) showed no significant eye discomfort, controlled corneal inflammation, regression of lesions, neovascularization regression, and no recurrence of keratitis, whereas for those in the poor prognosis group (n = 29), corneal inflammation was not effectively controlled or recurrence occurred.
SPSS version 21.0 software (IBM Corp., Armonk, NY, USA) was adopted for
performing statistical analysis of raw data. The normal distribution of data ware
tested using the Shapiro-Wilk test. The data with normal distribution are
presented as mean
Among all MGD patients, the incidence rate of keratitis was 53.3% (65/122), and
the positive rate of Demodex infection was 59.8% (73/122). The MGD
patients were divided into the keratitis group (n = 65) and the
non-keratitis group (n = 57) based on whether they have keratitis or
not. Among them, the positive rate of Demodex infection in the keratitis group was 81.5% (53/65), significantly higher than that in the non-keratitis
group (35.1%, 20/57) (p
| Clinical data | MGD patients (n = 122) | Keratitis group (n = 65) | Non-keratitis group (n = 57) | t/ |
p | |
| Age (years) | 36.48 |
37.38 |
35.44 |
1.378 | 0.171 | |
| Gender (male/female) | 63/59 | 34/31 | 29/28 | 0.025 | 0.875 | |
| Course of disease (months) | 13.19 |
12.46 |
14.02 |
1.310 | 0.193 | |
| Eye make-up (n, %) | 0.151 | 0.698 | ||||
| Yes | 47 (38.5%) | 24 (36.9%) | 23 (40.4%) | |||
| No | 75 (61.5%) | 41 (63.1%) | 34 (59.6%) | |||
| Contact lens usage (n, %) | 3.650 | 0.056 | ||||
| Wearing | 54 (44.3%) | 34 (52.3%) | 20 (35.1%) | |||
| Not wearing | 68 (55.7%) | 31 (47.7%) | 37 (64.9%) | |||
| History of eye trauma/burns (n, %) | 1.623 | 0.203 | ||||
| Yes | 23 (18.9%) | 15 (23.1%) | 8 (14.0%) | |||
| No | 99 (81.1%) | 50 (76.9%) | 49 (86.0%) | |||
| Admission time (n, %) | 1.745 | 0.627 | ||||
| March to May | 25 (20.5%) | 15 (23.1%) | 10 (17.5%) | |||
| June to August | 38 (31.1%) | 17 (26.2%) | 21 (36.8%) | |||
| September to November | 39 (32.0%) | 22 (33.8%) | 17 (29.8%) | |||
| December to February | 20 (16.4%) | 11 (16.9%) | 9 (15.8%) | |||
| Demodex infection (n, %) | 27.266 | |||||
| Positive | 73 (59.8%) | 53 (81.5%) | 20 (35.1%) | |||
| Negative | 49 (40.2%) | 12 (18.5%) | 37 (64.9%) | |||
Compared with the non-keratitis group, the keratitis group exhibited reduced BUT
value, increased CFS, MG dropout, and plugging of MG orifices (p
| Ocular surface parameters | Keratitis group (n = 65) | Non-keratitis group (n = 57) | t/Z | p |
| OSDI | 32.32 |
30.91 |
1.491 | 0.138 |
| SIT (mm) | 5.34 |
6.11 |
1.730 | 0.086 |
| BUT (s) | 4 (3, 6) | 6 (4, 8) | 3.634 | |
| CFS | 4 (3, 5) | 3 (1.5, 3) | 5.541 | |
| MG dropout | 2.0 (1.5, 2.5) | 1.5 (1.0, 2.3) | 2.719 | 0.007 |
| Plugging of MG orifices | 2.0 (1.5, 2.5) | 1.5 (1.0, 2.0) | 4.332 | |
| MG expression | 2.0 (1.5, 2.5) | 2.0 (1.0, 2.0) | 1.561 | 0.119 |
Note: BUT, break-up time; CFS, corneal fluorescein staining; MG, meibomian gland; OSDI, ocular surface disease index; SIT, Schirmer I test.
The results of univariate logistic analysis showed that the Demodex
infection (odds ratio [OR]: 8.171, 95% confidence interval [CI]: 3.564–18.734,
p
| Univariate analysis | Multivariate analysis& | ||||||||||
| SE | Wald | OR (95% CI) | p | SE | Wald | OR (95% CI) | p | ||||
| Age | 0.033 | 0.024 | 1.886 | 1.033 (0.986–1.083) | 0.170 | ||||||
| Male | 0.057 | 0.363 | 0.025 | 1.059 (0.520–2.158) | 0.875 | ||||||
| Course of disease | –0.037 | 0.028 | 1.693 | 0.964 (0.912–1.019) | 0.193 | ||||||
| Eye make-up | –0.145 | 0.373 | 0.151 | 0.865 (0.417–1.797) | 0.698 | ||||||
| Contact lens usage | 0.708 | 0.372 | 3.610 | 2.029 (0.978–4.210) | 0.057 | ||||||
| History of eye trauma/burns | 0.608 | 0.482 | 1.595 | 1.837 (0.715–4.724) | 0.207 | ||||||
| Admission time | |||||||||||
| March to May | / | / | / | Reference | / | ||||||
| June to August | –0.617 | 0.523 | 1.393 | 0.540 (0.194–1.503) | 0.238 | ||||||
| September to November | –0.148 | 0.521 | 0.080 | 0.863 (0.311–2.393) | 0.777 | ||||||
| December to February | –0.205 | 0.607 | 0.114 | 0.815 (0.248–2.679) | 0.736 | ||||||
| Demodex infection | 2.101 | 0.423 | 24.619 | 8.171 (3.564–18.734) | 1.826 | 0.553 | 10.909 | 6.209 (2.101–18.348) | |||
| OSDI | 0.053 | 0.036 | 2.182 | 1.054 (0.983–1.131) | 0.140 | ||||||
| SIT | –0.129 | 0.076 | 2.868 | 0.879 (0.758–1.020) | 0.090 | ||||||
| BUT | –0.312 | 0.084 | 13.753 | 0.732 (0.621–0.863) | –0.265 | 0.121 | 4.804 | 0.768 (0.606–0.972) | 0.028 | ||
| CFS | 0.968 | 0.201 | 23.301 | 2.633 (1.777–3.901) | 0.966 | 0.265 | 13.275 | 2.627 (1.562–4.416) | |||
| MG dropout | 0.678 | 0.237 | 8.175 | 1.969 (1.238–3.133) | 0.004 | 0.369 | 0.344 | 1.150 | 1.446 (0.737–2.840) | 0.284 | |
| Plugging of MG orifices | 1.103 | 0.274 | 16.149 | 3.013 (1.760–5.160) | 1.155 | 0.344 | 11.244 | 3.174 (1.616–6.235) | |||
| MG expression | 0.327 | 0.222 | 2.166 | 1.387 (0.897–2.144) | 0.141 | ||||||
Note: &p = 0.376 (Hosmer-Lemeshow test). BUT, break-up time; CI, confidence interval; CFS, corneal fluorescein staining; MG, meibomian gland; OR, odds ratio; OSDI, ocular surface disease index; SIT, Schirmer I test.
The above associated risk factors were included in the multivariate logistic
regression analysis. The analysis of multicollinearity indicated that the VIF
values of all variables were less than 5. Demodex infection (OR: 6.209,
95% CI: 2.101–18.348, p
Patients with keratitis (n = 65) were followed up for one year, and
divided into a good prognosis group (n = 36) and a poor prognosis group
(n = 29) based on their prognosis. The age and MG expression in the good
prognosis group were lower than that in the poor prognosis group (p
| Good prognosis group (n = 36) | Poor prognosis group (n = 29) | t/ |
p | ||
| Age (year) | 34.61 |
40.83 |
3.845 | ||
| Gender (male/female) | 16/20 | 18/11 | 2.000 | 0.157 | |
| Eye make-up (n, %) | 0.023 | 0.880 | |||
| Yes | 13 (36.1%) | 11 (37.9%) | |||
| No | 23 (63.9%) | 18 (62.1%) | |||
| Contact lens usage (n, %) | 0.837 | 0.360 | |||
| Wearing | 17 (47.2%) | 17 (58.6%) | |||
| Not wearing | 19 (52.8%) | 12 (41.4%) | |||
| History of eye trauma/burns (n, %) | 0.600 | 0.439 | |||
| Yes | 7 (19.4%) | 8 (27.6%) | |||
| No | 29 (80.6%) | 21 (72.4%) | |||
| Admission time (n, %) | 2.128 | 0.546 | |||
| March to May | 9 (25.0%) | 6 (20.7%) | |||
| June to August | 7 (19.4%) | 10 (34.5%) | |||
| September to November | 14 (38.9%) | 8 (27.6%) | |||
| December to February | 6 (16.7%) | 5 (17.2%) | |||
| Demodex infection | 2.292 | 0.130 | |||
| Positive | 27 (75.0%) | 26 (89.7%) | |||
| Negative | 9 (25.0%) | 3 (10.3%) | |||
| OSDI | 32.56 |
32.03 |
0.458 | 0.649 | |
| SIT (mm) | 5.77 |
4.82 |
1.407 | 0.164 | |
| BUT (s) | 4.69 |
4.10 |
1.184 | 0.241 | |
| CFS | 4 (3, 5) | 4 (3, 5) | 0.088 | 0.930 | |
| MG dropout | 2.0 (2.0, 2.5) | 2.0 (1.5, 2.5) | 0.519 | 0.604 | |
| Plugging of MG orifices | 2.0 (1.6, 2.5) | 2.0 (1.3, 3.0) | 0.020 | 0.984 | |
| MG expression | 2.0 (1.0, 2.4) | 2.0 (1.8, 3.0) | 2.254 | 0.024 | |
Note: BUT, break-up time; CFS, corneal fluorescein staining; MG, meibomian gland; OSDI, ocular surface disease index; SIT, Schirmer I test.
MG is a lipid-secreting sebaceous gland located in the eyelid. MGD is a chronic, diffuse inflammatory disease caused by excessive keratinization of multiple MG terminal ductal epithelium and dysfunction of their glandular secretions [26]. Dry eye caused by MGD can lead to various forms of eye discomforts and complications, affecting the stability of the tear film and the quality of tears [27]. Furthermore, MGD also causes continuous stimulation and damage to conjunctival cells and corneal epithelial cells through inflammation and immune response, leading to a variety of ocular surface inflammatory diseases, such as eyelid-associated keratoconjunctivitis and keratitis [1, 4, 28]. In this study, a total of 122 MGD-related dry eye patients were included, of whom 65 patients had keratitis, with a prevalence rate of 53.3%.
Demodex mites are parasites that feed on abnormally secreted oils. Eyelids are particularly vulnerable to Demodex infection due to the high level of secreted oils [12]. It has been confirmed that the overgrowth and colonization of Demodex mites, as well as their derived metabolites, are the foundation of MGD pathogenesis. Meanwhile, these metabolites further induce epithelial hyperkeratosis by stimulating capillary dilation and inducing inflammation. In addition, the accumulation of metabolites exacerbates glandular obstruction and terminal duct hyperkeratosis [15]. In addition, Demodex mites can serve as carriers of pathogens and pathogenic microorganisms, such as Staphylococcus and Streptococcus, which can trigger the host immune reaction [14]. Therefore, Demodex infection is also an important factor contributing to ocular surface inflammation. In the current study, the positive rate of Demodex infection in MGD patients was 59.8%. Moreover, the positive rate of Demodex infection in patients with keratitis was higher than that in the non-keratitis group, reaching 81.5%. Previous literature reported that the infection rate of Demodex in patients with refractory keratitis was as high as 100% [29], further validating the high prevalence of Demodex infection in patients with keratitis.
Our study analyzed the influencing factors of keratitis in MGD patients, revealing that Demodex infection was the independent risk factor for keratitis in MGD patients. Previous study reported that among patients with Demodex infection, the incidence of keratitis reaches 65%; in these Demodex infections, and the severity of MG loss was correlated with the severity of keratitis [30]. This also lends supportive evidence for our conclusion. It should be noted that we did not detect the influence of Demodex infection on the prognosis of MGD patients with keratitis. This indicates that Demodex infection was related to the occurrence of keratitis in MGD patients, but did not affect the prognosis of keratitis patients, probably related to the complex pathological mechanism of keratitis. Multiple factors including bacteria, viral infections, trauma, allergies, and immunity are involved in the pathogenesis of keratitis [31]. The recurrence of keratitis may be influenced by other factors. In addition, this study included a small sample of only 65 patients with keratitis for prognosis analysis, which had limited ability in examining the impact of Demodex infection on the prognosis of keratitis. Meanwhile, due to the small sample size, we did not conduct further regression analysis to explore the factors affecting the prognosis of keratitis. The influence and potential mechanisms of Demodex infections in the prognosis of keratitis should be further verified and explored using a larger cohort in the future.
In the current study to measured ocular surface parameters, we detected a decrease of BUT value and increases of CFS, MG dropout, and plugging of MG orifices in keratitis patients compared with non-keratitis patients, which are suggestive of ocular surface function weakening in MGD patients with keratitis. Nevertheless, OSDI score was not significantly different between the keratitis and non-keratitis groups. Despite the pathological changes on the ocular surface, subjective perception of MGD patients with keratitis did not experience significant enhancement. This may be due to the fact that the initial symptoms of keratitis are not obvious. Another reason may be the similarity and overlap in clinical symptoms between keratitis and MGD-related dry eye [1, 17], leading to nonsignificant difference in subjective perception between the cohorts separately affected by the two diseases. In addition, OSDI was usually applied to evaluate the symptoms of dry eye, but may not be suitable for assessing the eye symptoms in keratitis. Therefore, it is recommended to conduct detailed ophthalmic examinations for MGD-related dry eye patients to identify overlooked pathological changes.
In this study, multivariate logistic regression analysis showed that Demodex infestation, CFS and plugging of MG orifices were the independent risk factors for keratitis in MGD-related dry eye patients, while BUT was the protective factor. CFS can be used to evaluate the integrity of the cornea and its pathological damage. It was reported that the CFS in patients with severe keratitis complicated with dry eye were significantly reduced after treatment [32]. BUT is utilized to evaluate the stability of the tear film. Dry eye patients are unable to keep the tear film intact due to decreased tear production, exhibiting a decrease of BUT. Containing proteins, peptides, lipids, mucins, and electrolytes, the tear film plays a role in maintaining the health of the ocular surface [33]. Instability of the tear film causes damages of the corneal epithelium, where pathogens can easily colonize the corneal surface and induce keratitis. In addition, the decrease of protective tear film proteins in the patients with dry eye has been identified as a contributor to keratitis [34]. MG plugging can increase the risk of keratitis by reducing tear film lipids and tear film stability, and altering the microbial environment on the ocular surface [35, 36]. Meanwhile, the inflammatory response caused by MG plugging may also serve as a driver of keratitis [37].
Based on previous literature, contact lenses were considered a risk factor of keratitis [31]. However, in this study, we did not observe significant differences in contact lens usage between the keratitis group and the non-keratitis group. Such discrepancy is probably caused by the inclusion of different samples. Interestingly, the nonsignificant difference in age between the keratitis group and the non-keratitis group indicates that age is not a factor affecting the occurrence of keratitis in MGD patients. However, we found that subjects in the poor prognosis group were older than those in the good prognosis group, suggesting that age is related to the prognosis of MGD patients with keratitis. Previous study reported that age was a risk factor for MGD and keratitis, and older patients were at higher risk of MGD and keratitis [16, 31]. Harbiyeli et al. [38] reported that old age was associated with delayed recovery and poor visual prognosis in polymicrobial keratitis, consistent with our finding.
Several limitations of this study should be acknowledged. The sample size of this study is relatively small, especially in the keratitis patient group intended for prognosis analysis. The retrospective nature of the study does not allow for strict randomization procedures and control of confounding factors. Prospective large-scale cohort studies should be performed to validate relevant conclusions in the future.
Overall, the positive rate of Demodex infection is higher in patients with MGD complicated with keratitis than those without keratitis. Demodex infection, CFS and plugging of MG orifices are the independent risk factors for keratitis, whereas BUT is the protective factor for MGD-related dry eye patients. Additionally, Demodex infection does not significantly impact the prognosis of keratitis. In summary, this study sheds light on factors influencing the clinical diagnosis and treatment of MGD and keratitis.
The data required during the current study are available upon reasonable request from the corresponding author.
HL designed the research study. JHX and LYW collected and analyzed the data. HL wrote the first draft. All authors contributed to important editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
The research was approved by the Ethics Committee of The First People’s Hospital of Chun’an County (Approval No: 2024-04-12-06) and conducted in accordance with the Declaration of Helsinki. All patients signed the informed consent form.
Not applicable.
This research received no external funding.
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.