

 , Bibi Hu 1, Qing Zhang 1
, Bibi Hu 1, Qing Zhang 11 Department of Nursing, The Second Affiliated Hospital, Zhejiang University School of Medicine, 310009 Hangzhou, Zhejiang, China
Abstract
Young and middle-aged patients undergoing maintenance hemodialysis (MHD) experience significant physical impairment and psychological stress, resulting in reduced levels of subjective well-being. Therefore, this study aimed to assess the subjective well-being of this population and to identify its influencing factors, thereby informing the clinical development of targeted nursing strategies.
Clinical data were collected from 220 young and middle-aged MHD patients at the Blood Purification Center of the Second Affiliated Hospital, Zhejiang University School of Medicine between April 2024 and April 2025. General demographic and clinical characteristics, along with scores from relevant assessment scales, were collected. The factors influencing subjective well-being were analyzed in this patient cohort.
The mean General Well-Being (GWB) scale score among these patients was 62.44 ± 3.12. Statistically significant differences were observed across education level, per capita monthly family income, self-care ability, self-management ability, symptom distress, financial burden to the family, and social support (p < 0.05). Multiple linear regression analysis indicated that education, per capita monthly family income, self-care ability, self-management ability, symptom distress, financial burden on the family, and social support were significant predictors of subjective well-being among young and middle-aged MHD patients (p < 0.05).
The subjective well-being of young and middle-aged MHD patients remains at a moderate level and is influenced by factors such as education level, per capita monthly family income, self-care ability, self-management ability, symptom distress, financial burden on the family, and social support. Nursing care interventions should be designed and implemented based on these factors to improve the overall well-being of this patient group.
Keywords
- maintenance hemodialysis
- quality of life
- risk factors
- nursing care
Hemodialysis (HD) is a common renal replacement therapy for patients with end-stage renal disease (ESRD). [1], with the number of maintenance hemodialysis (MHD) projected to reach 870,000 by 2025 [2]. Notably, the incidence of new-onset cases is shifting toward younger age groups, and nearly 80% of patients are young and middle-aged adults [3], with an average age of 55 years, about a decade younger than their counterparts in the United States and Japan [4].
More concerningly, MHD treatment disrupts the daily routines of young and middle-aged MHD patients and often leads to social isolation [5]. Moreover, patients undergoing MHD face low employment rates, heavy financial burdens, limited social support, and psychological distress, all of which severely impair their quality of life [6]. In summary, the decline in physical function, changes in living environment and economic conditions, and the onset of psychological challenges resulting from long-term hemodialysis make MHD patients particularly vulnerable to stigma [7].
Therefore, investigating the factors that influence the subjective well-being of young and middle-aged MHD patients and developing effective nursing care interventions are of both theoretical and practical significance. However, current studies lack consensus on the factors that influence subjective well-being in this population. Based on this context, the present study conducted a cross-sectional analysis among young and middle-aged MHD patients to examine their level of subjective well-being and identify its influencing factors, aiming to provide a scientific basis for optimizing clinical nursing strategies.
This study collected clinical data from 220 young and middle-aged MHD patients
treated at the Blood Purification Center of the Second Affiliated Hospital,
Zhejiang University School of Medicine between April 2024 and April 2025. The
patient screening flowchart is shown in Fig. 1. Inclusion criteria: (1) 18–59
years; (2) receiving regular MHD for
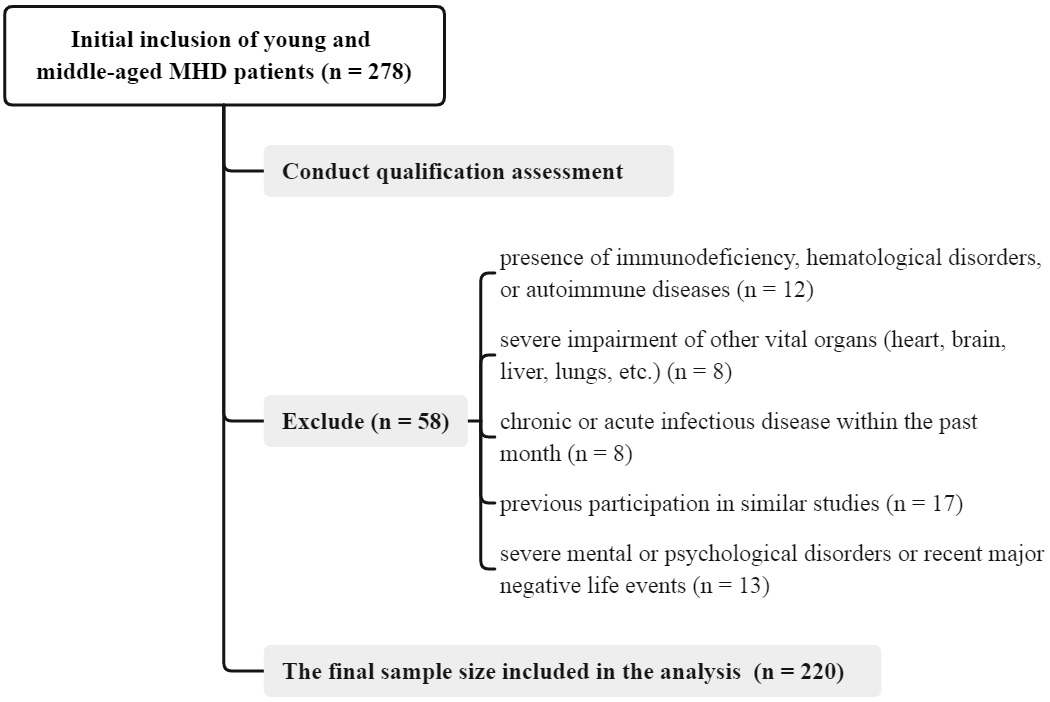 Fig. 1.
Fig. 1.
Flow chart of participant screening and enrollment in the study. MHD, maintenance hemodialysis.
Exclusion criteria: (1) presence of immunodeficiency, hematological disorders, or autoimmune diseases; (2) severe impairment of other vital organs (heart, brain, liver, lungs, etc.); (3) chronic or acute infectious disease within the past month; (4) previous participation in similar studies; (5) severe mental or psychological disorders or recent major negative life events.
The researchers developed a structured survey questionnaire to collect general information, including age, gender, marital status, education level, occupation, living conditions, disease-related knowledge, interests and hobbies, average monthly family income, and type of medical insurance. Disease-related information included duration of dialysis, weekly dialysis frequency, average duration of each dialysis session, and long-term medication status. Self-assessment of health status encompassed self-care ability, sleep quality, and the health condition of family members or caregivers. Additional items covered the caregiving and financial burdens placed on the family.
The modified GWB schedule [8] comprises six dimensions: satisfaction and
interest in life, concerns about health, control over emotions and behaviors,
happiness or depression, relaxation and tension, and energy, with a total score
of 120. Score ranges of 0–24, 25–48, 49–72, 73–96, and 97–120 correspond to
low, relatively low, moderate, relatively high, and high levels of subjective
well-being, respectively. Higher scores indicate greater subjective well-being.
The scale demonstrates good reliability and validity, with a Cronbach’s
The revised self-management scale [9] incorporates 4 dimensions:
problem-solving, partnership, emotional processing, and self-care execution. The
self-management ability of patients is evaluated using a 4-point Likert
evaluation method. The total score ranges from 20 to 80 and is categorized as
follows: 20–40 (poor), 41–60 (average), and 61–80 (good) self-management
ability. Higher scores indicate stronger self-management behavior. The scale has
demonstrated good reliability and validity, with Cronbach’s
The modified SSRS scale [10] comprises three dimensions: subjective support,
objective support, and utilization of social support. The total score ranges from
12 to 66, categorized as
The adapted DSI scale [11] comprises two dimensions and 30 items, with five
items assessing mental health symptoms and twenty-five items assessing physical
symptoms, yielding a total possible score is 150, comprising a 30-point score for symptom presence (each item scored 0 or 1) and a 120-point score for symptom distress (each item rated on a 5-point Likert scale). For the distress dimension, scores of
The uniformly trained investigators were responsible for collecting the clinical data of all patients. Two researchers independently analyzed and organized the questionnaires, followed by cross-verification to ensure the accuracy and completeness of the data.
Statistical analyses were performed using SPSS version 26.0 (IBM Corp., Armonk,
NY, USA). A p-value
Multiple linear regression analysis was conducted to identify factors
influencing subjective well-being among young and middle-aged MHD patients, with
a test level of
The average GWB score among the 220 young and middle-aged MHD patients was 62.44
| Dimension | Number of items | Score ( |
| Satisfaction and interest in life | 2 | 4.76 |
| Concerns about health | 2 | 5.33 |
| Control over emotions and behaviors | 3 | 11.10 |
| Happy or depressed mood | 3 | 12.15 |
| Relaxation and tension | 4 | 14.02 |
| Energy | 4 | 14.88 |
| Average GWB score | 62.44 |
GWB, General Well-Being; MHD, maintenance hemodialysis.
This study included a total of 220 young and middle-aged MHD patients,
comprising 129 males and 91 females. In terms of educational background, the
majority (144 cases) had a high school education or below. Most patients reported
a family per capita monthly income between 4001 and 6000 Chinese yuan (1 Chinese
yuan =0.14 US dollars, 61 cases). The differences in GWB scores among young and
middle-aged MHD patients with varying education levels and per capita monthly
family income were statistically significant (p
| Items | Case (n, %) | GWB score | t/F-value | p-value | |
| Age | 0.305 | 0.761 | |||
| 18–40 years | 87 (39.5) | 62.52 |
|||
| 41–59 years | 133 (60.5) | 62.39 |
|||
| Gender | 0.164 | 0.870 | |||
| Male | 129 (58.6) | 62.41 |
|||
| Female | 91 (41.4) | 62.48 |
|||
| Marital status | 0.003 | 1.000 | |||
| Married | 171 (77.7) | 62.45 |
|||
| Divorced | 21 (9.6) | 62.40 |
|||
| Widowed | 9 (4.1) | 62.38 |
|||
| Unmarried | 19 (8.6) | 62.45 |
|||
| Education level | 2.064 | 0.040 | |||
| High school or below | 144 (65.5) | 62.16 |
|||
| College degree or above | 76 (34.5) | 62.97 |
|||
| Occupation | 0.432 | 0.826 | |||
| Worker | 12 (5.5) | 62.38 |
|||
| Farmer | 45 (20.5) | 61.99 |
|||
| Office worker | 31 (14.1) | 62.57 |
|||
| Freelancer | 34 (15.4) | 62.55 |
|||
| Retired/emeritus | 67 (30.4) | 62.63 |
|||
| Other | 31 (14.1) | 61.97 |
|||
| Living status | 0.007 | 0.999 | |||
| Live alone | 18 (8.2) | 62.39 |
|||
| Live with spouse | 129 (58.6) | 62.48 |
|||
| Live with parents | 35 (16.0) | 62.45 |
|||
| Live with offspring | 38 (17.2) | 62.43 |
|||
| Disease knowledge | 0.045 | 0.954 | |||
| Not understanding | 3 (1.4) | 61.97 |
|||
| Partial understanding | 144 (65.5) | 62.43 |
|||
| Complete understanding | 73 (33.1) | 62.49 |
|||
| Interests and hobbies | 0.114 | 0.977 | |||
| Narrow range | 23 (10.5) | 61.99 |
|||
| Relatively narrow range | 22 (10.0) | 62.40 |
|||
| Average range | 148 (67.2) | 62.45 |
|||
| Relatively wide range | 23 (10.5) | 62.48 |
|||
| Wide range | 4 (1.8) | 62.51 |
|||
| Per capita monthly family income | 4.979 | 0.002 | |||
| 56 (25.5) | 61.05 |
||||
| 2001–4000 Chinese yuan | 54 (24.5) | 62.89 |
|||
| 4001–6000 Chinese yuan | 61 (27.7) | 62.90 |
|||
| 49 (22.3) | 62.95 |
||||
| Types of medical insurance | 0.002 | ||||
| Urban medical insurance | 157 (71.4) | 62.48 |
|||
| Rural medical insurance | 50 (22.7) | 62.46 |
|||
| Self-paying medical | 3 (1.4) | 62.42 |
|||
| Commercial insurance | 6 (2.7) | 62.43 |
|||
| Other | 4 (1.8) | 62.41 |
|||
GWB, General Well-Being; MHD, maintenance hemodialysis.
1 Chinese yuan = 0.14 US dollars.
The differences in GWB scores among young and middle-aged MHD patients with
varying self-care ability, self-management ability, and levels of symptom
distress were statistically significant (p
| Items | Case (n, %) | GWB Score | t/F-value | p-value | |
| Duration of dialysis | 0.008 | 0.992 | |||
| 4 months–3 years | 91 (41.4) | 62.47 |
|||
| 4–10 years | 102 (46.4) | 62.43 |
|||
| 27 (12.3) | 62.39 |
||||
| Weekly dialysis frequency | 0.065 | 0.949 | |||
| 18 (8.2) | 62.49 |
||||
| 202 (91.8) | 62.44 |
||||
| Average duration of each dialysis session | 0.090 | 0.928 | |||
| 13 (5.9) | 62.51 |
||||
| 207 (94.1) | 62.43 |
||||
| Long-term medication status | 0.016 | 0.984 | |||
| 1–2 types | 61 (27.7) | 62.49 |
|||
| 3–4 types | 96 (43.6) | 62.44 |
|||
| 63 (28.6) | 62.39 |
||||
| Self-care ability | 3.261 | 0.040 | |||
| Inability to self-care | 5 (2.3) | 59.02 |
|||
| Partial self-care | 37 (16.8) | 62.49 |
|||
| Complete self-care | 178 (80.9) | 62.53 |
|||
| Sleep condition | 0.002 | ||||
| Poor | 11 (5.0) | 62.42 |
|||
| Relatively poor | 36 (16.4) | 62.43 |
|||
| Average | 106 (48.2) | 62.46 |
|||
| Relatively good | 51 (23.2) | 62.45 |
|||
| Better | 16 (7.3) | 62.49 |
|||
| Health status of family members or caregivers | 0.003 | 0.997 | |||
| Relatively poor | 7 (3.2) | 62.40 |
|||
| Average | 51 (23.2) | 62.45 |
|||
| Good | 162 (73.6) | 62.47 |
|||
| Self-management ability | 46.708 | ||||
| Poor | 57 (25.9) | 59.23 |
|||
| Average | 126 (57.3) | 63.49 |
|||
| Good | 37 (16.8) | 63.54 |
|||
| Symptom distress | 48.393 | ||||
| Severe | 52 (23.6) | 58.79 |
|||
| Moderate | 131 (59.5) | 63.39 |
|||
| Mild | 37 (16.8) | 63.41 |
|||
GWB, General Well-Being; MHD, maintenance hemodialysis.
The GWB scores in young and middle-aged MHD patients differed significantly
according to the financial burden and social support of their families (p
| Items | Case (n, %) | GWB score | t/F-value | p-value | |
| Caregiving burden to families | 0.003 | ||||
| Very high | 16 (7.3) | 62.42 |
|||
| Relatively high | 52 (23.6) | 62.44 |
|||
| Average | 101 (45.9) | 62.47 |
|||
| Relatively little | 32 (14.5) | 62.49 |
|||
| Very little | 19 (8.6) | 62.50 |
|||
| Financial burden to the family | 5.039 | ||||
| Very high | 29 (13.2) | 60.56 |
|||
| Relatively high | 52 (23.6) | 62.87 |
|||
| Average | 93 (42.3) | 62.95 |
|||
| Relatively little | 27 (12.3) | 63.01 |
|||
| Very little | 19 (8.6) | 63.04 |
|||
| Social support | 53.923 | ||||
| Low level | 64 (29.1) | 59.11 |
|||
| Moderate level | 118 (53.6) | 63.52 |
|||
| Relatively high level | 38 (17.3) | 63.60 |
|||
GWB, General Well-Being; MHD, maintenance hemodialysis.
Variables with p
| Independent variable | Assignment |
| Education | High school or below = 0; College degree or above = 1 |
| Per capita monthly family income | |
| Self-care ability | Inability of self-care = 0; Partial self-care = 1; Complete self-care = 2 |
| Self-management ability | Poor = 0; Average = 1; Good = 2 |
| Symptom distress | Severe = 0; Moderate = 1; Mild = 2 |
| Financial burden to the family | Very high = 0; Relatively high = 1; Average = 2; Relatively little = 3; Very little = 4 |
| Social support | Low level = 0; Moderate level = 1; Relatively high level = 2 |
1 Chinese yuan = 0.14 US dollars.
| Variable | Regression coefficient (B) | Standard error (SE) | Standardized coefficient ( |
t-value | p-value |
| Education | 0.923 | 0.293 | 0.402 | 3.150 | 0.002 |
| Per capita monthly family income | 1.054 | 0.345 | 0.379 | 3.055 | 0.003 |
| Self-care ability | 0.887 | 0.254 | 0.384 | 3.492 | 0.001 |
| Self-management ability | 1.113 | 0.279 | 0.455 | 3.989 | |
| Symptom distress | 0.943 | 0.284 | 0.481 | 3.320 | 0.001 |
| Financial burden to the family | 0.978 | 0.334 | 0.376 | 2.928 | 0.004 |
| Social support | 1.078 | 0.224 | 0.467 | 4.813 |
Note: R2 = 0.455, adjusted R2 = 0.376, F = 15.129, p
These factors could be broadly classified into three domains, each reflecting different levels of influence on patients’ well-being. First, socioeconomic resources, such as higher education and greater family income, provided a stronger material foundation and enhanced resilience against illness-related stressors. Second, personal ability and physical condition, including stronger self-care and self-management abilities, as well as lower symptom distress, directly determined a patient’s quality of daily life and sense of independence and dignity. Third, external environmental pressure and support, such as reduced financial burden and stronger social support, served as crucial psychological buffers that contributed to alleviating feelings of isolation and economic anxiety.
Due to frequent and prolonged hospital visits, the physical and social abilities
of MHD patients gradually decline, contributing to adverse psychological
conditions [12]. In addition to physical symptoms, the present study found that
the subjective well-being (GWB score: 62.44
Although medical insurance policies help alleviate part of the perceived burden among MHD patients, the cumulative cost of long-term treatment continues to impose a substantial financial burden on patients’ families and caregivers. This financial pressure leads to a reduced quality of life and diminished subjective well-being, which may in turn exacerbate physical and psychological distress, creating a vicious cycle [14]. By incorporating quantitative measures of well-being, our research not only aligns with previous findings but also provides robust data to better characterize the psychological state of young and middle-aged MHD patients. The findings clearly demonstrate that their subjective well-being remains within a relatively low to moderate range, underscoring the need for targeted psychological and social support interventions.
The findings of this study confirmed that education is a significant factor influencing the subjective well-being of young and middle-aged MHD patients. This is consistent with the results reported by Hao et al. [15], which indicated a positive association between educational level and overall quality of life among MHD patients. Furthermore, this study revealed specific psychological pathways through which education influences subjective well-being. Patients with lower educational levels often exhibit poorer acceptance of dialysis treatment, as limited disease awareness contributes to a heightened psychological burden and consequently lower subjective well-being.
Conversely, patients with higher educational levels demonstrate a greater capacity to access and utilize diverse information sources, which enhances their understanding of the disease, reduces psychological stress, and contributes to higher subjective well-being. Similarly, Peng et al. [16] reported that visualized health education based on the Health Belief Model significantly improves disease cognition and self-management abilities across different educational backgrounds. This suggests that systematic and visualized dissemination of health information can effectively compensate for cognitive gaps associated with lower educational levels, thereby improving self-efficacy and subjective well-being.
In clinical practice, these findings suggest that graphic manuals and short educational videos (preferably in the local dialect) should be used to explain dialysis-related knowledge to young and middle-aged MHD patients with lower educational levels. Additionally, establishing a “Question and Answer (Q & A) wall” in dialysis centers to answer common questions in an accessible language may enhance patients’ understanding and knowledge of the disease and further improve their subjective well-being.
Furthermore, this study confirmed that per capita monthly family income significantly influences patients’ subjective well-being, supporting the conclusions of Intas et al. [17], who reported that economic stress negatively affects patients’ quality of life and family burden. This research further investigated the specific impact of economic factors among young and middle-aged MHD patients, identifying subjective well-being as a key indicator. For patients with low per capita monthly family income, targeted interventions such as transportation or nutrition subsidies, the establishment of low-income patient support groups, and the integration of social work resources to facilitate benefit applications may help enhance their subjective well-being.
The findings of this study confirmed that self-care ability has a significant influence on the subjective well-being of young and middle-aged MHD patients. Those who cannot care for themselves experience limitations in daily activities, loss of adult independence, and feelings of uselessness. Furthermore, the presence of dialysis catheters, skin pigmentation, and emaciation or edema can worsen their physical self-image, leading to social withdrawal, loneliness, and ultimately reduced subjective well-being [18]. This study further revealed the central role of “self-care capacity loss” within this psychological pathway, as it affects patients’ subjective experience by impairing their sense of independence and self-worth.
For young and middle-aged MHD patients with limited self-care abilities, the provision of assistive devices, such as wheelchairs and bath chairs, can facilitate functional rehabilitation training. At the same time, psychological counseling can be offered to reduce feelings of shame. Family collaboration programs should also be developed to train caregivers to avoid excessive protectiveness and to ensure that daily activities remain within the patient’s capability, thereby enhancing their subjective well-being.
Moreover, the self-management ability was shown to be closely associated with subjective well-being among young and middle-aged MHD patients. Irregular dialysis or non-cooperative behaviors of young and middle-aged MHD patients, such as arbitrarily shortening dialysis sessions, may result in toxin accumulation, skin itching, and insomnia, leading to further decline in quality of life. MHD patients who perceive themselves as burdens to their families and believe they make no meaningful contribution are more prone to social withdrawal and escapist ideation, significantly increasing their risk of severe psychological distress [19]. For young and middle-aged MHD patients exhibiting poor self-management abilities, setting staged goals, by breaking large objectives into smaller, achievable tasks, can help reduce frustration. Moreover, enhancing confidence and self-efficacy through exposure to successful patient role models and positive feedback from healthcare providers can further improve their subjective well-being.
Symptom distress was also found to significantly impact the subjective well-being of young and middle-aged MHD patients. The results confirmed the key role of symptom management in improving well-being and provided empirical support for the existing “symptom distress-happiness decline” theory within this age group. Young and middle-aged MHD patients experiencing severe symptom distress may suffer direct physical discomfort, which can lead to a marked decline in their subjective well-being. Accordingly, a stepped-care approach to symptom management can be employed. This may include basic interventions for mild symptoms (providing symptom management manuals and encouraging patients to maintain symptom diaries); enhanced interventions for patients with moderate symptoms (specialist consultation, psychological intervention, and cognitive-behavior therapy to alleviate negative emotions); and advanced interventions for patients with severe symptoms (developing a functional rehabilitation plan through a multidisciplinary team). Implementing such graduated symptom management strategies can effectively enhance the subjective well-being of young and middle-aged MHD patients.
This study revealed that the financial burden on families significantly affected the subjective well-being of young and middle-aged MHD patients. The cost of MHD treatment is high, with an average annual expenditure reaching tens of thousands of yuan. Even after medical insurance reimbursement, the out-of-pocket expenses remained substantial, which constrained patients’ basic living needs. Moreover, most young and middle-aged patients were compelled to reduce working hours or become unemployed due to treatment schedules and decreased physical strength, further reducing family income and forming a vicious cycle that led to reduced subjective well-being. These findings further deepen the understanding of the vicious circle mechanism linking financial burden and quality of life, highlighting the heightened vulnerability of young and middle-aged patients to income disruption. For young and middle-aged MHD patients experiencing heavy family financial burden, targeted medical assistance programs can be implemented, the reimbursement ratio for dialysis expenses can be increased, and nursing training for family members can be provided to lessen the burden of caregiving, prevent households from falling into poverty, and ultimately improve the subjective well-being of patients.
This study also confirmed that social support is a significant factor influencing subjective well-being in young and middle-aged MHD patients, consistent with the findings reported by Luo et al. [20]. Additionally, this study further supplemented the specific manifestations of insufficient social support from the perspective of patients’ subjective experiences, including emotional repression expressed as “no one understands”, and discrimination from being misunderstood as having an “infectious disease” due to visible body changes, thus refining the internal mechanism of how social support influences well-being. Young and middle-aged MHD patients with limited social support often lack confidants, leading to feelings of being misunderstood and emotionally repressed. Some patients may experience social discrimination due to the visibility of dialysis catheters or reduced physical strength, causing self-isolation and loneliness. When families and social networks fail to provide financial support or emotional support, patients may be compelled to reduce dialysis frequency or discontinue essential medications, thereby compromising their quality of life and further diminishing their subjective well-being.
For young and middle-aged MHD patients with low social support, family support can be strengthened through educational programs that train family members to provide emotional support and appropriate care. Meanwhile, establishing mutual aid networks can foster participation in dialysis patient communities, facilitate the sharing of experiences, reduce loneliness, and improve patients’ subjective well-being.
A limitation of this study is that the sample primarily consisted of young and middle-aged patients. Therefore, the findings may not be directly generalizable to MHD populations with different demographic characteristics (such as elderly patients), geographic regions, cultural backgrounds, or healthcare systems. Future research should include more diverse populations and larger sample sizes to validate the generalizability of these findings and provide a more comprehensive understanding of the factors influencing subjective well-being among MHD patients in varied settings.
Our findings underscore that improving subjective well-being in young and middle-aged MHD patients requires a comprehensive care approach that extends beyond conventional symptom management. Clinically, it is essential to integrate assessments of socioeconomic challenges and social support into routine nursing practice. Developing targeted interventions to strengthen self-management abilities and alleviate perceived financial burdens is crucial for enhancing patient outcomes. We recommend conducting longitudinal studies to further explore the internal mechanisms and causal pathways through which factors such as educational level, limited social support, and financial burden influence well-being. Future research should focus on designing, implementing, and testing such multifaceted interventions to determine their efficacy in real-world clinical settings.
• The mean GWB score was 62.44
• Education, income, self-care ability, self-management, symptom distress, financial burden, and social support were identified as key drivers of subjective well-being.
• Clinical care strategies addressing these factors may effectively enhance the subjective well-being of young and middle-aged MHD patients.
Data are available from the corresponding author upon reasonable request.
Conceptualization: MYY; Methodology: BBH; Data Curation: BBH and QZ; Writing—Original Draft: MYY, BBH and QZ. All authors contributed to revising the manuscript critically for important intellectual content. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
This study was approved by the Human Research Ethics Committee of the Second Affiliated Hospital, Zhejiang University School of Medicine (Approval No. 2024-1600), and was performed in accordance with the Declaration of Helsinki. Written informed consent was obtained from participants.
Not applicable.
This work was supported by General Research Project of Zhejiang Provincial Education Department under (Grant Number: Y202454726).
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.