


 , Habeeb Bishi 2, Vikramman Vignaraja 3, Amogh Patil 4, Raashad Hasan 5, Charmilie Chandrakumar 6
, Habeeb Bishi 2, Vikramman Vignaraja 3, Amogh Patil 4, Raashad Hasan 5, Charmilie Chandrakumar 61 Department of Orthopaedics, Lewisham and Greenwich NHS Trust, SE18 4QH London, UK
2 Department of Orthopaedics, Royal Surrey NHS Foundation Trust, GU2 7XX Guildford, UK
3 Department of Orthopaedics, Guy’s and St Thomas’ NHS Foundation Trust, SE1 7EH London, UK
4 Department of Orthopaedics, Liverpool University Hospitals NHS Foundation Trust, L9 7AL Liverpool, UK
5 Department of Orthopaedics, Barts Health NHS Trust, E1 2ES London, UK
6 Department of Orthopaedics, King’s College Hospital NHS Foundation Trust, SE5 9RS London, UK
Abstract
This study explores the attitudes and barriers faced by UK orthopaedic trainees regarding less than full time (LTFT) training. LTFT training has become more accessible since 2022, yet surgical trainees have been slower to adopt it compared to other specialties.
A cross-sectional, questionnaire-based study was carried out via a 16-item online questionnaire which was distributed to aspiring orthopaedic surgeons registering for an orthopaedic themed teaching programme.
216 respondents met the inclusion criteria. The study found that 42% of respondents would consider LTFT training, with higher interest among female trainees. Key barriers identified included extended training duration, financial concerns, potential decline in surgical skills, and negative perceptions from colleagues.
The research highlights the need for clearer guidance, better support, and a cultural shift within orthopaedic departments to address these barriers. Initiating education and awareness programmes for senior staff and providing comprehensive information to trainees are essential steps to fostering a more inclusive and supportive environment for LTFT training in orthopaedic surgery.
Keywords
- medical education
- orthopedics
- surgical specialties
Less than full time (LTFT) training in postgraduate medical education allows doctors to work and train at a reduced schedule due to well-founded personal reasons or to increase flexibility in their careers [1]. Initially restricted to non-surgical specialties, LTFT training was expanded to include surgical trainees following a successful pilot, reflecting a broader acceptance of flexible training paths.
The concept of LTFT training is increasingly important in modern medical education. It offers numerous benefits, including improved work-life balance, reduced risk of burnout, and enhanced personal well-being for trainees. For the medical profession, LTFT training helps retain valuable professionals and promotes workforce diversity [2, 3], despite these benefits, several barriers hinder the widespread adoption of LTFT training, particularly among surgical trainees.
Common barriers to LTFT training include concerns about extended training duration, financial implications, potential decline in surgical skills, and negative perceptions from colleagues. Orthopaedic surgery, known for its rigorous training requirements and high patient volumes, exemplifies these difficulties, with ongoing concerns within the senior orthopaedic workforce that accommodating LTFT schedules may compromise patient care and training quality [4, 5].
Recent policy changes have significantly impacted LTFT training. In 2022, an agreement between the British Medical Association (BMA), Health Education England (HEE), and NHS employers removed the need for governing bodies to deem suitability for LTFT training, limiting it only by service considerations [6]. This policy shift has led to a steady increase in LTFT training adoption, with 19.5% of trainees opting for LTFT in 2023, up from 10.7% in 2017 [7]. However, surgical trainees have been slower to adopt LTFT training compared to their non-surgical counterparts, with only 10% of surgical trainees being LTFT [8].
This is a junior cohort compared to previous research done in this area, looking at trainees prior to starting higher specialty training, and what prospective candidates’ preferences and concerns are when it comes to flexible training.
The aim of this study is to explore the attitudes towards LTFT training among current UK surgical trainees and highlight potential barriers to entering LTFT, particularly in orthopaedics. By understanding these factors, we can identify strategies to promote LTFT training and foster a more inclusive and supportive environment for all surgical trainees. This study aims to provide insights into the challenges and perceptions that influence the uptake of LTFT training and propose potential solutions to address these barriers.
This is a cross-sectional, questionnaire-based study. A 16-item questionnaire (Appendix A) was designed following a literature review by two of the authors (HB, CC), focusing on attitudes towards LTFT training. The questionnaire was assessed for validity by the authors collectively and was piloted on local orthopaedic resident doctors prior to dissemination.
The survey was completed by all applicants to a free surgical webinar teaching series (Fundamentals of Orthopaedics) [9]. The series was aimed at resident doctors wishing to pursue a career in orthopaedics but was also attended by orthopaedic nurse practitioners and medical students. The contents aimed to equip applicants with skills and knowledge they would benefit from as a junior registrar in trauma and orthopaedics. The teaching series was delivered via Zoom (Zoom Video Communications Inc., San Jose, CA, USA) by orthopaedic registrars and consultant surgeons.
The questionnaire had a 100% response rate as it was a compulsory part of the registration process for the teaching series.
Inclusion criteria for this study were responses from anyone currently working in the UK as a resident doctor. Both doctors currently working in a training post approved by one of the four UK statutory educational bodies and doctors working in ‘non-training’ orthopaedic roles were surveyed. All non-doctor and non-UK respondents were excluded.
The data were anonymised, and statistical analysis was performed on Microsoft Excel (Microsoft 365, Microsoft Corporation, Redmond, WA, USA). The questionnaire also included free-text responses, which the authors reviewed and analysed for major themes using reflexive thematic analysis, conducted by three of the authors (HB, CC, JH).
When respondents have answered ‘no’ to the question ‘Have you ever noticed/
heard/seen discrimination or negative behaviour towards the idea of being an LTFT
trainee?’, the follow up question of ‘If you have noticed/ heard/ seen
discrimination or negative behaviour towards the idea of being an LTFT trainee,
where has this been from?’ has not been included in the results. Association of
binary variables was assessed using the chi-square test. Results were considered
statistically significant at p
Informed consent was obtained from all participants through the questionnaire. The first page of the questionnaire included a statement explaining that the information provided would be anonymised, analysed, and used for research purposes. The statement also clarified that, by completing the survey, participants were providing their consent to participate in the study. This study did not require formal ethics approval as per the NHS Health Research Authority’s online decision tool [10].
Out of 299 respondents, 216 met the inclusion criteria. Of these 216, 159 (73.6%) were male, 54 (25.0%) were female, 1 (0.5%) was non-binary, and 2 (0.9%) did not wish to reveal their gender (Table 1).
| N = 216 | Percentage (%) | ||
| Gender | |||
| Male | 159 | 73.6 | |
| Female | 54 | 25.0 | |
| Non-binary | 1 | 0.5 | |
| Prefer not to say | 2 | 0.9 | |
| Grade | |||
| CT1 | 57 | 26.4 | |
| CT2 | 71 | 32.9 | |
| Trust SHO/JCF | 39 | 18.0 | |
| Trust Registrar | 49 | 22.7 | |
CT1, Core Surgical Trainee-Year 1; CT2, Core Surgical Trainee-Year 2; SHO/JCF, Senior House Officer/Junior Clinical Fellow.
Most of the cohort were currently in core surgical training 128 (59.3%), 57 (26.4%) in Core Surgical Trainee-Year 1 (CT1) and 71 (32.9%) in Core Surgical Trainee-Year 2 (CT2). 49 (22.7%) were in ‘non-training’ orthopaedic registrar posts, and 39 (18.0%) were working in Junior Clinical Fellow (JCF) posts. In addition, participants were from a huge range of geographical areas as seen in Fig. 1.
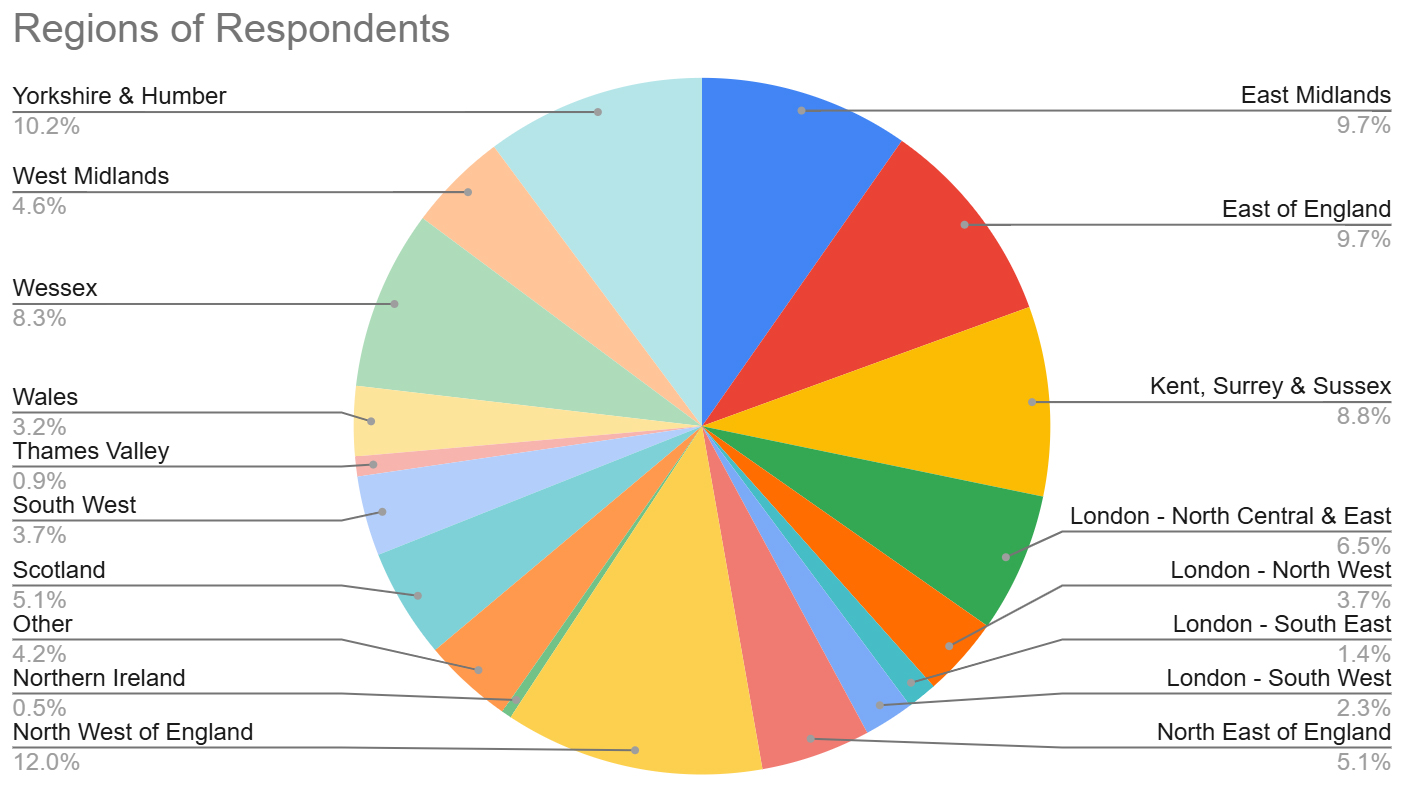 Fig. 1.
Fig. 1.
Distribution of respondents by Deanery. Figure created using Google Sheets (Google LLC, Mountain View, CA, USA).
Out of 216 respondents, 91 (42%) would consider going LTFT. 56/159 (35%) of
male respondents reported they would consider going LTFT compared to 34/54 (63%)
of females. The difference between these two groups was statistically significant
(p
The most common responses to the question ‘If you were to do LTFT, what would be your reasons?’ were childrearing/caring for a dependent (53%), burnout (36%), travelling (23%) and business interests (13%) (Table 2).
| Male, n (%) | Female, n (%) | Non-binary, n (%) | Prefer not to say, n (%) | Total participants, n (%) | |
| N = 159 | N = 54 | N = 1 | N = 2 | N = 216 | |
| Childrearing | 64 (40%) | 24 (44%) | 1 (100%) | 0 (0%) | 89 (41%) |
| Burnout | 50 (31%) | 26 (48%) | 0 (0%) | 1 (50%) | 77 (36%) |
| Travel | 36 (23%) | 11 (20%) | 0 (0%) | 2 (100%) | 49 (23%) |
| Business interests | 22 (14%) | 6 (11%) | 0 (0%) | 1 (50%) | 29 (13%) |
| Caring for a dependent | 19 (12%) | 6 (11%) | 0 (0%) | 0 (0%) | 25 (12%) |
| Sporting commitments | 16 (10%) | 3 (6%) | 0 (0%) | 0 (0%) | 19 (9%) |
| Work life balance | 1 (1%) | 5 (9%) | 0 (0%) | 0 (0%) | 6 (3%) |
| Family | 1 (1%) | 0 (0%) | 0 (0%) | 0 (0%) | 1 (0%) |
| Research | 1 (1%) | 0 (0%) | 0 (0%) | 0 (0%) | 1 (0%) |
LTFT, less than full time.
Men and women were similarly likely to cite childrearing as a reason they would consider going LTFT with males 40% and females 44%. There was no statistical significance between either gender (p = 0.589).
48% of female respondents cited burnout as a reason for going LTFT compared to 31% of men.
When asked ‘What potential barriers would stop you from pursuing LTFT
training?/What barriers have you faced?’, the most common responses were
increased length of training (68%), financial reasons (46%), negative
perceptions of colleagues (36%) and worsening of surgical skills (34%). Female
trainees were significantly more concerned about worsening of surgical skills
compared to male trainees 26/54 (48%) vs 46/159 (29%) (p = 0.010) and
the negative perceptions of colleagues 31/54 (57%) vs 44/159 (28%) (p
| Male, n (%) | Female, n (%) | Non-binary, n (%) | Prefer not to say, n (%) | Total participants, n (%) | |
| N = 159 | N = 54 | N = 1 | N = 2 | N = 216 | |
| Increased length of training | 112 (70%) | 33 (61%) | 0 (0%) | 2 (100%) | 147 (68%) |
| Finances | 73 (46%) | 26 (48%) | 0 (0%) | 1 (50%) | 100 (46%) |
| Negative perceptions of colleagues | 44 (28%) | 31 (57%) | 1 (100%) | 1 (50%) | 77 (36%) |
| Worsening of surgical skills | 46 (29%) | 26 (48%) | 0 (0%) | 1 (50%) | 73 (34%) |
| Ego/prestige | 10 (6%) | 5 (9%) | 0 (0%) | 0 (%) | 15 (7%) |
65 (30%) respondents reported hearing or seeing negative behaviour towards the idea of being an LTFT trainee. The majority of this came from senior surgeons (consultants or senior registrars) with 39 (18%) respondents having seen this. Women were twice as likely as men to experience this negative behaviour from seniors, 28% compared to 14%. Overall, women experienced more negative behaviour towards LTFT training than men: 23/54 (43%) vs 39/159 (25%). Other sources of negative behaviour towards LTFT training were hospital managers (6%) and peers (6%), with the remainder of respondents not specifying where they had witnessed this behaviour (Table 4).
| Male, n (%) | Female, n (%) | Non-binary, n (%) | Prefer not to say, n (%) | Total participants, n (%) | |
| N = 159 | N = 54 | N = 1 | N = 2 | N = 216 | |
| Senior surgeons | 22 (14%) | 15 (28%) | 1 (100%) | 1 (50%) | 39 (18%) |
| Hospital managers and admin staff | 7 (4%) | 4 (7%) | 0 (0%) | 1 (50%) | 12 (6%) |
| Peers | 10 (6%) | 4 (7%) | 0 (0%) | 0 (0%) | 14 (6%) |
Only 59 (27%) of our respondents felt that there is information readily available regarding LTFT training.
When asked to rate the orthopaedic specialties receptiveness to LTFT training,
on a Likert scale of 1 (not receptive)–10 (extremely receptive), participants
gave an average score of 4.9
The results from this cross-sectional study show that there is a large proportion of orthopaedic trainees who would consider going LTFT, especially if certain barriers were addressed. However, the question is, why is it that orthopaedics as a specialty is lagging behind other medical training specialties in its receptiveness towards LTFT.
Orthopaedic surgical training, like other procedure-based specialities, requires a significant time commitment from trainees to achieve competence, which may be difficult with an LTFT schedule. Orthopaedic surgeons typically face high patient volumes and complex cases, which may make it challenging to accommodate part-time schedules without a deemed risk of compromising patient care or training quality. Additionally, there may be cultural norms within orthopaedic departments that prioritize traditional full-time training pathways and view LTFT arrangements as less desirable or less committed. Moreover, the historical lack of flexibility in orthopaedic training programmes and the perception of orthopaedics as a male-dominated field may contribute to resistance towards LTFT training, particularly among senior staff members. We wanted to explore how these factors influence the trainees themselves and what could be done to address these concerns.
Our research has identified four barriers which may prevent orthopaedic trainees from pursuing LTFT training: concerns about extended training duration, the financial implications of opting for LTFT, worries about declining surgical skills, and perceived negative perceptions from colleagues regarding LTFT training. A career in orthopaedic surgery is an expensive pursuit; in 2017, the estimated cost of achieving a Certificate of Completion of Training (CCT) in trauma and orthopaedics was £21,405.50 [12]. These costs will have increased since then approximately in line with inflation and a number of these costs are fixed to the amount of time spent in training. LTFT trainees will not only sacrifice a percentage of their earnings to become LTFT, but these fixed costs will remain, ultimately reducing their expendable income disproportionately as they will spend more years in training. To reduce this burden, it may be pertinent for memberships to the Joint Committee on Surgical Training (JCST) and the British Orthopaedic Association (BOA), for example, to be paid adjusted to the trainees’ LTFT schedule, with trainees paying the same amount over their training career, independent of how many years it takes them to complete training.
Increased time in training is a common concern for those entering LTFT orthopaedic training. CCT is competency-based rather than time-based [13], and thus it can be confusing for trainees to estimate how long LTFT will extend their training as there is little clear guidance on which sessions they will miss each week. This varies based on the time they take off and how that fits into the department they are currently rotating through. Clearer guidance on this matter could alleviate some concerns, but this may be logistically challenging given the variance between each trainee’s work schedule across different deaneries and within each orthopaedic department. A change in the structure of surgical rotations may partially alleviate some of these issues. Currently, LTFT arrangements are agreed upon when trainees rotate to a new department. Longer placements agreed upon further in advance could allow better planning of work schedules to support training experience.
A key concern seen in our study is for LTFT training leading to worsening surgical skills. Our study showed 48% of females were concerned about worsening surgical skills compared to 29% of males. This may be because women typically have longer periods out of training for parental leave [14]; as such there may be concern that LTFT may compound any existing decline in confidence or skill.
Surgical exposure in training has markedly reduced in recent years due to the introduction of the European Working Time Directive (EWTD) and 48-hour work weeks. The Temple report [15], which was carried out to assess whether working within EWTD limited hours is detrimental to surgical training, concluded that delivery of surgical training is possible in a 48-hour work week, but not if trainees have significant roles in out of hours (OOH) services, are poorly supervised or lack access to learning opportunities.
Reduced hours mean that a greater proportion of shifts for trainees are OOH to ensure service provision. During these shifts, trainees will be exposed to learning opportunities, though they are less likely to involve surgical skill development. Trainees who are LTFT will experience further reductions in clinical exposure in theatres, leading to concerns about whether 60% or 80% LTFT is sufficient, even though the Temple report deemed 48 hours to be adequate. This issue would benefit from further research.
Since 1996, women have comprised over 50% of medical school entrants [2, 16]. However, as of 2020, only 7.3% of consultant orthopaedic surgeons were female, marking the lowest representation among the ten surgical specialties. Similarly, orthopaedics also exhibited the lowest proportion of female registrars at 20.6%. Though there is increasing representation of women in orthopaedics. It is projected that at the current rate parity is projected to be achieved in 2070 [17].
Our study focusing on prospective higher specialty training orthopaedic applicants found that 63% of female respondents expressed willingness to pursue LTFT training, in contrast to 35% of males. To ensure a diverse surgical workforce, it is crucial to enhance accessibility of orthopaedic higher surgical training (HST) for female trainees.
Many studies have shown that female medical students are often deterred from entering surgical training due to the perceived poor ‘work life balance’ [18] and the need to adopt LTFT training at some point in their training to balance work and family life [19, 20]. In our study, 9% of women cited work life balance as a reason to consider LTFT compared to 1% of men, showing that this is an ongoing valid concern that female trainees have once they have started upon a surgical career path and making LTFT an accepted and valid option will serve to make surgical training a more attractive option to those medical students.
In our survey, 48% of female respondents cited burnout as a reason they would consider going LTFT compared to 31% of male respondents. Burnout is an increasingly prevalent concern amongst doctors in training with 23% being at high risk of burnout across all specialties and 26% in surgical specialties [21]. In 2023, research revealed that 90.3% of UK orthopaedic surgeons across all grades experienced moderate to high levels of burnout [22]. Reducing burnout is not only of benefit to the trainees themselves, but also to the departments that they work in and the patient populations that they serve as it can negatively impact staff productivity and patient outcomes [23, 24].
To foster a diverse surgical workforce, implementing LTFT training could serve as a strategy to not only reduce burnout within the specialty but also, appeal to a greater number of female applicants. Our research indicates that females are more inclined to consider LTFT training due to burnout, making it a potentially effective method for attracting, retaining, and sustaining diversity within the orthopaedic specialty.
Our study revealed that childrearing emerged as the predominant motive driving aspiring orthopaedic surgeons toward pursuing LTFT training, with 40% of men and 44% of women expressing this as their primary reason. The escalating expenses associated with childcare may provide some explanation for this; recent national data shows that the average monthly cost of nursery care for a single 10-hour day per week amounts to £248 post-tax income [25]. For individuals with multiple children, the financial advantages of going 80% LTFT are evident, particularly considering the substantial savings in childcare expenses which alone can offset the financial costs. Moreover, this arrangement affords the added benefit of allocating more quality time to nurturing relationships with their young children, thereby addressing the evolving needs of the workforce.
A key factor in directing surgical trainees away from LTFT training is perceived negative perceptions from colleagues and seniors, with 81 (38%) respondents citing this as a barrier. 70 (32%) respondents reported they had witnessed negative or discriminatory behaviour towards the idea of being an LTFT trainee with this mainly coming from senior surgeons 40 (57%) along with hospital managers 12 (17%) and from peers 14 (20%) with the other 4 not reporting where they had witnessed this behaviour.
Female respondents were also more likely to be concerned about negative perceptions from colleagues with regards to going LTFT, with 57% (compared to 28%) seeing it as a barrier to them entering LTFT training. It is well documented that surgical trainees, orthopaedic trainees in particular, are often exposed to bullying and undermining behaviours during their training; this is more commonly directed towards women and those from ethnic minority backgrounds [26, 27].
With this in mind, applicants may feel less empowered to choose LTFT, fearing scrutiny from seniors and colleagues for deviating from the conventional training pathway. Fostering a more receptive and inclusive senior surgical body would empower trainees to make personal choices that enhance their quality of life, improve job satisfaction, and reduce the risk of burnout, ultimately improving their overall well-being.
32% of respondents (43% of females and 25% of males) reported having witnessed or experienced discrimination or negative behaviour towards going LTFT in training. This is primarily observed among consultants and senior registrars. To foster greater receptivity toward trainees opting for LTFT training, it is essential to implement education and awareness programmes highlighting the benefits of LTFT training for both trainees’ professional development and personal well-being. These programmes should emphasize the significance of accommodating diverse needs and promoting work-life balance within surgical training. Additionally, efforts should focus on fostering a positive organizational culture that values diversity and respects individual career choices, creating an environment conducive to open communication and mutual support between trainees and senior staff. The disparity in LTFT uptake between surgical trainees (10%) and trainees across all specialties (19.5%) underscores the urgent need for a shift in attitudes and practices within surgical departments [7, 8]. Providing targeted training and resources for consultants and senior registrars, particularly in effective mentoring and coaching techniques, is essential. Equipping senior staff with the skills and knowledge to support and guide trainees pursuing LTFT training can enhance trainee well-being and foster a more understanding and accommodating approach to trainees’ preferences and needs.
Only 27% of respondents felt that there was adequate information available regarding LTFT training available to them.
Without access to comprehensive information about the process, benefits, and potential implications of LTFT training, trainees may struggle to fully understand their options and make well-informed choices regarding their career paths. This lack of information can lead to uncertainty, anxiety, and hesitation among trainees, potentially deterring them from pursuing LTFT training even if it aligns with their personal or professional needs.
Furthermore, inadequate information may perpetuate misconceptions or negative perceptions about LTFT training among trainees, senior staff, and healthcare organizations, contributing to the existing barriers and resistance towards LTFT arrangements within surgical specialties. With further accessible information and widespread integration into the surgical curriculum, these problems could be addressed.
This study has some limitations. The data we have used is all self-reported which may introduce some bias as respondents may have provided socially desirable answers or interpreted questions differently. The study’s sample, drawn from a group of orthopaedic webinar registrants, may also not be fully representative of all aspiring UK orthopaedic trainees, potentially limiting the broader applicability of the findings. Requiring questionnaire completion to register for the teaching series may have led to less thoughtful or rushed responses if respondents viewed the questionnaire as a barrier to accessing the webinar. While we have identified key barriers to the uptake of LTFT training, we have not quantitively assessed the impact of these barriers on actual training outcomes or progression. Further research would be needed to determine how LTFT impacts skills development and Annual Review of Competence Progression (ARCP) outcomes for orthopaedic trainees.
Our research highlights the significant barriers that impede orthopaedic trainees from pursuing LTFT training, including concerns about extended training duration, financial implications, worries about declining surgical skills, and negative perceptions from colleagues. Orthopaedic surgery faces challenges due to the demanding nature of the specialty, cultural norms within departments, and historical lack of flexibility in training programmes. Furthermore, gender disparities persist, with women expressing greater interest in LTFT training due to concerns about burnout, work-life balance, and childcare responsibilities.
To address these challenges and foster a more inclusive and supportive environment for LTFT trainees, it is imperative to initiate education and awareness programmes targeting consultants and senior registrars. These programmes should emphasize the advantages of LTFT training for trainees’ well-being and patient care, while also promoting diversity and work-life balance within the specialty. Additionally, efforts should be made to provide comprehensive information and support to surgical trainees considering LTFT options, thereby empowering them to make informed decisions about their career paths.
Moving forward, integrating information regarding LTFT training into the orthopaedic surgical curriculum and providing targeted resources for trainees and senior staff will be essential. By embracing LTFT arrangements and creating a more supportive and accommodating environment, orthopaedic surgery can attract and retain a diverse workforce, reducing burnout and ultimately enhancing job satisfaction.
All data included in this study are available from the corresponding author upon reasonable request.
JH: Methodology, analysis, and manuscript writing. HB: Conceptualisation, data collection, analysis, and critical review of the manuscript. VV: Data collection, analysis, and manuscript editing. AP: Data collection, interpretation of results, and critical review of the manuscript. RH: Data collection, analysis, project administration, and revising it critically for important intellectual content. CC: Supervision, data collection, conceptualisation, methodology, revising it critically for important intellectual content. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
An informed consent was obtained from each participant. This study did not require formal ethics approval as per the NHS Health Research Authority’s online decision tool.
We would like to acknowledge all participants and institutions that supported this research.
This research received no external funding.
The authors declare no conflict of interest.
See Appendix A.
Section 1 of 3.
Less Than Full Time Questionnaire
Please note that this form contains a questionnaire about less than full time training. By filling in this questionnaire, you are consenting for the data to be anonymised, analysed and used for research purposes. The data will not be shared to third parties.
Please contact us if you have any queries: fun.orthopaedics@gmail.com
1. Gender:
- Female
- Male
- Non-binary
- Prefer not to say
- Other: ________
2. Ethnicity:
- Asian or Asian British
- Black, African or Caribbean or Black British
- Arab
- White – British, Irish or any other White background
- Prefer not to say
- Other: ______
3. Do you have any children/dependents?
- Yes
- No
- Prefer not to say
- Other: ______
4. Where are you currently working?
- United Kingdom (UK)
- Non-UK
Section 2 of 3.
5. Which deanery are you currently based in?
1. East Midlands
2. East of England
3. Kent, Surrey & Sussex
4. London – North Central & East
5. London – North West
6. London – South East
7. London – South West
8. North East of England
9. North West of England
10. Northern Ireland
11. Scotland
12. South West
13. Thames Valley
14. Wales
15. Wessex
16. West Midlands
17. Yorkshire & Humber
18. Other: ______
6. Current Grade:
- F1
- F2
- CT1/ST1
- CT2/ST2
- Trust SHO / Junior Clinical Fellow
- Trust Registrar
- Specialty Registrar in Training (ST3–ST8)
- Medical Student
- Other: ______
Section 3 of 3.
7. Are you currently in a HEE approved training programme? (e.g., Foundation Programme, Core Surgical Training)
- Yes
- No
8. Are you a Full Time or Less Than Full Time (LTFT) trainee?
- Yes
- No
- Not applicable
9. Would you consider going into Less Than Full Time (LTFT) training/flexible training during surgical training?
- Yes
- No
- Not applicable
10. If you were to do LTFT, what would be your reasons?
- Childrearing
- Caring for a dependent
- Sporting commitments
- Business interests
- Travelling
- Burnout
- Other: ______
11. What potential barriers would stop you pursuing Less Than Full Time (LTFT) training?/What barriers have you faced?
- Increased length of training
- Negative perceptions of LTFT by colleagues (e.g., undermining)
- Concerns of worsening surgical skills
- Ego/Prestige
- Finances (Reduced pay)
- Other: ______
12. Have you ever noticed/heard/seen discrimination or negative behaviour towards the idea of being a LTFT trainee?
- Yes
- No
13. If you have noticed/heard/seen discrimination or negative behaviour towards the idea of being a LTFT trainee, where has this been from?
- Senior surgeons (consultants/senior registrars)
- Hospital managers and admin staff
- Peers
- Not applicable, have not noticed this
- Other: ______
14. Do you feel that there is information readily available on LTFT applications?
- Yes
- No
15. On a scale of 1–10, how receptive do you feel orthopaedics is as a specialty to LTFT?
(1 = Not receptive at all, 10 = Completely receptive)
[Scale 1–10]
16. Do you have any comments/experiences regarding Less Than Full Time (LTFT) training?
- Long answer text:__________________________
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.