








1 Department of Obstetrics and Gynecology, Beijing Shijitan Hospital, Capital Medical University, 100038 Beijing, China
Abstract
To explore the factors influencing sleep disorders in patients with polycystic ovary syndrome (PCOS) after ketogenic diet intervention and establish a predictive model.
Data of 220 PCOS patients undergoing ketogenic diet intervention at Beijing Shijitan Hospital, Capital Medical University, from January 2021 to December 2023 were retrospectively collected. Patients were randomly divided into the modelling group (132 patients) and the validation group (88 patients) in a 3:2 ratio. The modelling group was further divided into the sleep disorder group (56 patients) and the non-sleep disorder group (76 patients). Univariate and binary logistic regression analyses were conducted to determine the influencing factors of sleep disorders after administering a ketogenic diet intervention in patients with PCOS. The predictive model was constructed using SPSS, and analyses of receiver operating characteristic (ROC) curves, calibration curves and decision curve analysis (DCA) were performed in the R language to evaluate the clinical practicality of the model.
In the modelling group, anxiety (odds ratio [OR] = 1.768, 95% confidence interval [CI]: 1.284–2.434, p < 0.001), depression (OR = 1.494, 95% CI: 1.193–1.872, p < 0.001), blood sugar status (impaired fasting glucose/tolerance) (OR = 5.278, 95% CI: 1.533–18.177, p = 0.008) and low-density lipoprotein cholesterol (LDL-c; OR = 1.619, 95% CI: 1.201–2.181, p = 0.002) were significant factors affecting sleep disorders. The prediction model incorporates these factors (X1–X4), and the model expression is Logit(P) = βConstant + (β1X1) + (β2X2) + (β3X3) + (β4X4). The calibration curve showed good agreement between predicted risks and actual risks. ROC analysis showed that the area under the curve was 0.9328 (95% CI: 0.892–0.954) for the modelling group and 0.8431 (95% CI: 0.777–0.899) for the validation group, both indicating that the model has high accuracy. DCA curves showed that the model has significant positive net benefits and good clinical utility.
Anxiety, depression, blood sugar status and LDL-c are key factors influencing sleep disorders in patients with PCOS after ketogenic diet intervention. A prediction model featuring high accuracy and remarkable clinical utility was successfully established.
Keywords
- polycystic ovary syndrome
- ketogenic diet
- sleep disorders
- influencing factors
- predictive model
Polycystic ovary syndrome (PCOS) is a complex endocrine disorder characterised by reproductive dysfunction and metabolic abnormalities, including chronic anovulation, excess androgens, and insulin resistance, and is one of the most common causes of menstrual irregularities in women of reproductive age [1]. PCOS not only affects the fertility of patients but also increases the risk of developing type 2 diabetes, cardiovascular diseases, gestational diabetes, gestational hypertension syndrome, and endometrial cancer [2, 3]. Therefore, early prevention and treatment of PCOS are of paramount importance. In recent years, the ketogenic diet has shown promising effects in the treatment of PCOS as a specialised dietary intervention. The ketogenic diet, characterised by an altered dietary composition comprising very low carbohydrate intake, moderate protein intake, and high fat intake, induces a metabolic state called ketosis [4, 5]. This dietary approach aims to stimulate the production of ketone bodies as the primary energy source, thereby improving hormone levels and weight status in PCOS patients. Several studies have demonstrated significant improvements in hormone levels and weight reduction in obese PCOS patients following the ketogenic diet, leading to enhanced fertility [6, 7]. However, despite the positive outcomes achieved with the ketogenic diet in PCOS treatment, its potential side effects and complications cannot be overlooked [8].
In the first 1–2 weeks of ketone production, some patients with PCOS may
experience adaptive symptoms such as temporary drowsiness and fatigue, which are
usually related to the adaptation period of ketone body metabolism or electrolyte
loss [9]. The symptoms are mild and mostly resolve
spontaneously. In addition, discomfort such as constipation and elevated uric
acid can be improved by adjusting diet (such as increasing dietary fibre,
supplementing minerals) or symptomatic treatment. Nevertheless, the impact of the
ketogenic diet on sleep quality in patients with PCOS remains under-explored
[10]. Potential mechanisms may involve blood sugar
fluctuations, interference of ketone body metabolism on neurotransmitters (such
as
Sleep disorders represent one of the complications that may arise following ketogenic diet intervention, possibly linked to various factors, including changes in lifestyle habits, negative emotions, environmental adjustments, and physiological conditions. Sleep disorders not only impact the quality of life for patients but may also exacerbate the symptoms of PCOS, creating a vicious cycle. Therefore, this study aims to investigate the influencing factors of sleep disorders in PCOS patients following ketogenic diet intervention and establish a corresponding predictive model, with the ultimate hope of formulating preventive and treatment strategies for sleep disorders in this patient population receiving ketogenic diet.
The sample size for this research was calculated using the formula N =
Zα/22
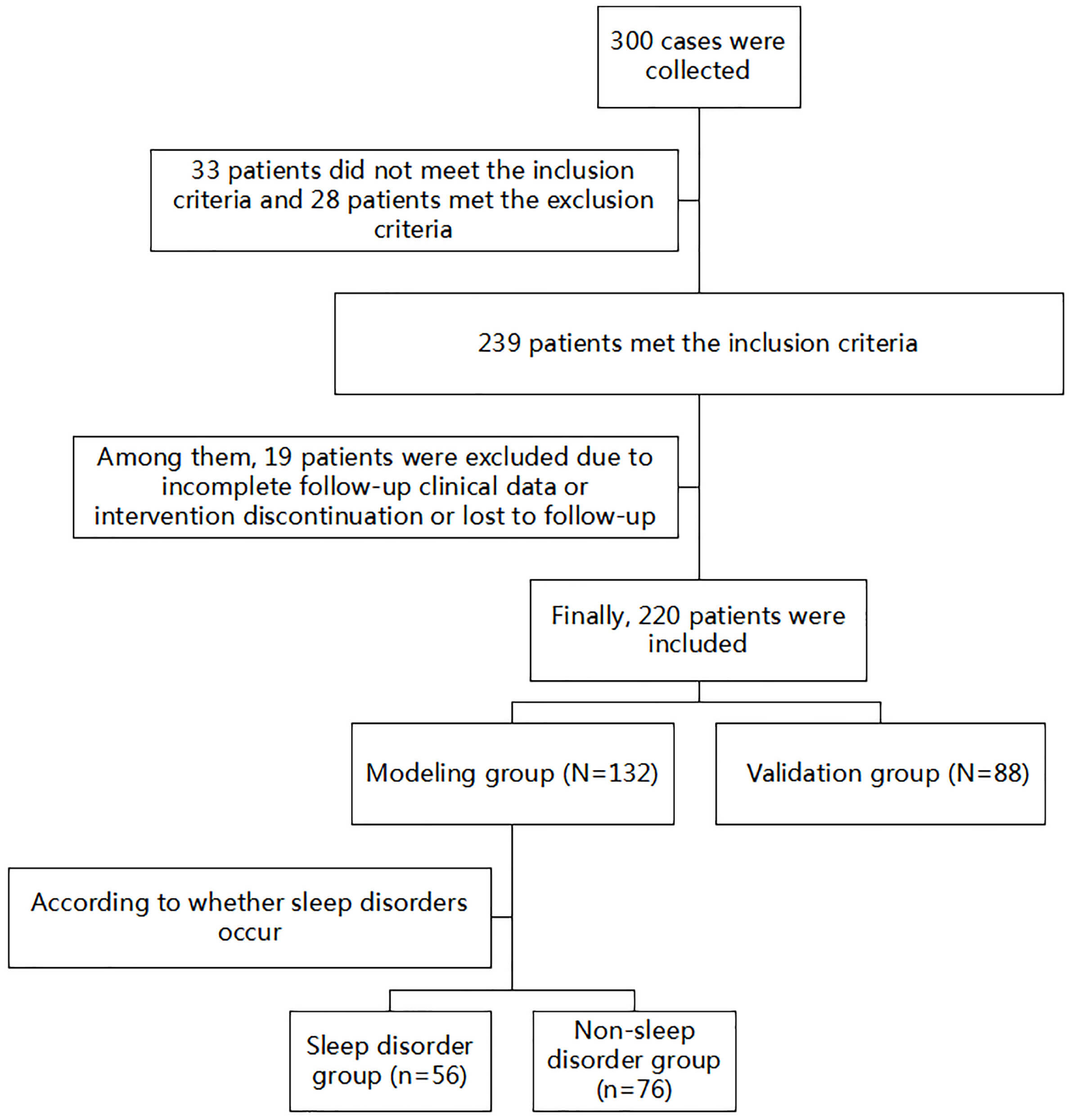 Fig. 1.
Fig. 1.
Flowchart of subject recruitment and grouping.
This study encompasses the implementation of a literature review to understand possible relevant influencing factors, the collection of clinical data, and the removal of patient information with missing data.
In reference to previous research literature, we collected general patient data (such as age, body mass index [BMI], place of residence, smoking status, etc.), anxiety, depression, blood sugar status, as well as levels of low-density lipoprotein cholesterol (LDL-c), lipoprotein, and Apolipoprotein A (ApoA). These data were gathered through the electronic medical record system and by conducting the inquiry.
Sleep disorder assessment was conducted in this study using the Pittsburgh Sleep
Quality Index (PSQI) scale, which consists of 7 items, each scored from 0 to 3,
with a total score ranging from 0 to 21 [13]. The critical
value for defining the quality of sleep is 5 points. With the PSQI score
Anxiety in patients was assessed using the Generalised Anxiety Disorder 7 (GAD-7) self-assessment scale, which comprises 7 items, each scored from 0 to 3, with a total score ranging from 0 to 21 [14]. Higher scores indicate higher levels of anxiety in patients.
Assessment of depression among the patients was performed with the use of the Patient Health Questionnaire-9 (PHQ-9) self-assessment scale, which consists of 9 items, each scored from 0 to 3, with a total score ranging from 0 to 27 [15]. Higher scores indicate higher levels of depression in patients.
Experimental data collected were analysed with SPSS 27.0 (International Business
Machines Corporation, Armonk, NY, USA). The Shapiro-Wilk test was used to assess
data normality. Normally distributed quantitative data are represented as mean
Comparison of general information between the modelling group and the validation
group of patients showed no statistically significant differences (p
| Baseline data | Modelling group (n = 132) | Validation group (n = 88) | t/ |
p-value | |
| Age (years) | 30.11 |
29.70 |
0.451 | 0.652 | |
| BMI (kg/m2) | 31.27 |
30.71 |
1.118 | 0.265 | |
| Residence | 0.098 | 0.755 | |||
| Urban | 112 | 76 | |||
| Rural | 20 | 12 | |||
| Smoking | 1.220 | 0.269 | |||
| Yes | 13 | 5 | |||
| No | 119 | 83 | |||
| Anxiety (score) | 8.02 |
7.71 |
0.979 | 0.329 | |
| Depression (score) | 13.47 |
12.83 |
1.716 | 0.088 | |
| Blood sugar status | 0.123 | 0.940 | |||
| Normal | 87 | 60 | |||
| Impaired fasting glucose/tolerance | 24 | 15 | |||
| Diabetes | 21 | 13 | |||
| LDL-c (mmol/L) | 2.92 |
2.88 |
1.543 | 0.124 | |
| Lipoprotein (mg/L) | 122.66 |
122.40 |
0.066 | 0.948 | |
| ApoA (g/L) | 1.14 |
1.15 |
1.038 | 0.300 | |
Abbreviations: ApoA, Apolipoprotein A; BMI, body mass index; LDL-c, low-density lipoprotein cholesterol.
In the modelling group, comparisons of age, BMI, residence, smoking, lipoprotein
levels, and ApoA levels showed no statistically significant differences
(p
| Baseline data | Sleep disorder group (n = 56) | Non-sleep disorder group (n = 76) | t/ |
p-value | |
| Age (years) | 30.07 |
30.14 |
0.064 | 0.949 | |
| BMI (kg/m2) | 31.67 |
30.98 |
1.381 | 0.170 | |
| Residence | 0.554 | 0.457 | |||
| Urban | 46 | 66 | |||
| Rural | 10 | 10 | |||
| Smoking | 0.082 | 0.774 | |||
| Yes | 6 | 7 | |||
| No | 50 | 69 | |||
| Anxiety (score) | 8.91 |
7.36 |
5.146 | ||
| Depression (score) | 14.80 |
12.49 |
5.077 | ||
| Blood sugar status | 26.84 | ||||
| Normal | 23 | 64 | |||
| Impaired fasting glucose/tolerance | 17 | 7 | |||
| Diabetes | 16 | 5 | |||
| LDL-c (mmol/L) | 3.02 |
2.84 |
5.411 | ||
| Lipoprotein (mg/L) | 122.58 |
122.71 |
0.027 | 0.979 | |
| ApoA (g/L) | 1.13 |
1.15 |
1.722 | 0.087 | |
Abbreviations: ApoA, Apolipoprotein A; BMI, body mass index; LDL-c, low-density lipoprotein cholesterol; PCOS, polycystic ovary syndrome.
Statistically significant variables identified from the univariate analysis were
included in the binary logistic regression analysis, in which anxiety,
depression, blood sugar status, and LDL-c were regarded as independent variables,
as shown in Table 3, with the occurrence of sleep disorders as the dependent
variable (1 = occurred, 0 = not occurred). The results of the binary logistic
regression analysis indicated that anxiety, depression, blood sugar status, and
LDL-c were influencing factors for the occurrence of sleep disorders in PCOS
patients after ketogenic diet intervention (p
| Variable | Assignment |
| Anxiety | Original value |
| Depression | Original value |
| Blood sugar status | Normal = 0, Impaired fasting glucose/tolerance = 1, Diabetes = 2 |
| LDL-c | Original value |
Abbreviation: LDL-c, low-density lipoprotein cholesterol.
| Dependent variable | Standard error | Wald | p-value | Exp (β) | 95% CI | ||
| Lower limit | Upper limit | ||||||
| Anxiety | 0.570 | 0.163 | 12.196 | 1.768 | 1.284 | 2.434 | |
| Depression | 0.402 | 0.115 | 12.194 | 1.494 | 1.193 | 1.872 | |
| Blood sugar status | - | - | 8.585 | 0.014 | - | - | - |
| Blood sugar status (n = 1) | 1.664 | 0.631 | 6.953 | 0.008 | 5.278 | 1.533 | 18.177 |
| Blood sugar status (n = 2) | 1.257 | 0.717 | 3.068 | 0.080 | 3.514 | 0.861 | 14.336 |
| LDL-c | 0.482 | 0.152 | 10.016 | 0.002 | 1.619 | 1.201 | 2.181 |
| Constant | –28.470 | 6.257 | 20.703 | - | - | ||
Abbreviation: LDL-c, low-density lipoprotein cholesterol; CI, confidence interval.
Based on the results of the logistic regression analysis, with anxiety,
depression, blood sugar status, and LDL-c (named X1, X2, X3, and X4,
respectively) incorporated into the predictive model, the combined predictive
factor model expression is Logit(P) =
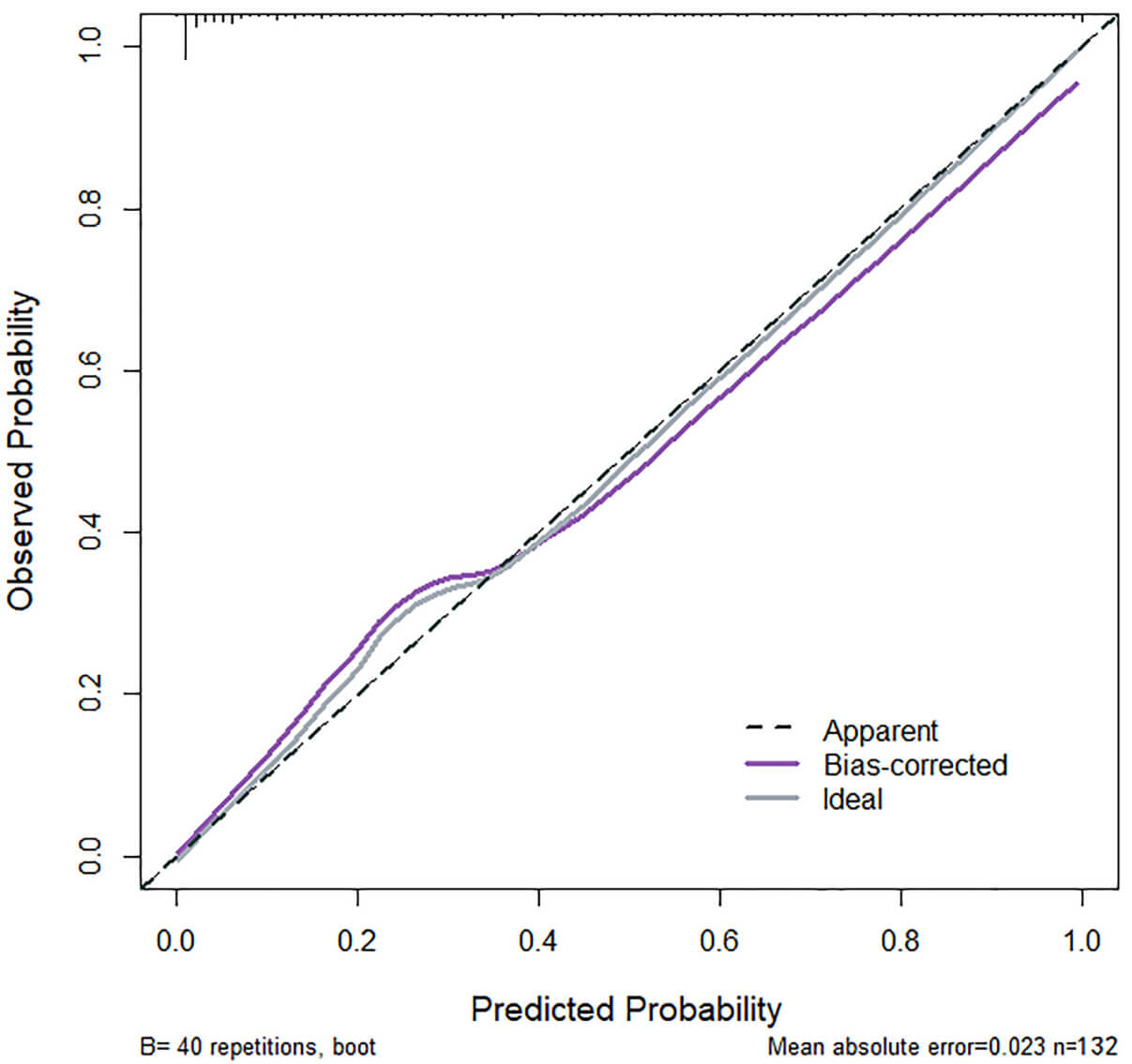 Fig. 2.
Fig. 2.
Calibration curve of the modelling group. The curve has a slope which is close to 1, indicating that the model has a good consistency between the predicted risk and the actual risk for sleep disorders in PCOS patients after ketogenic diet intervention.
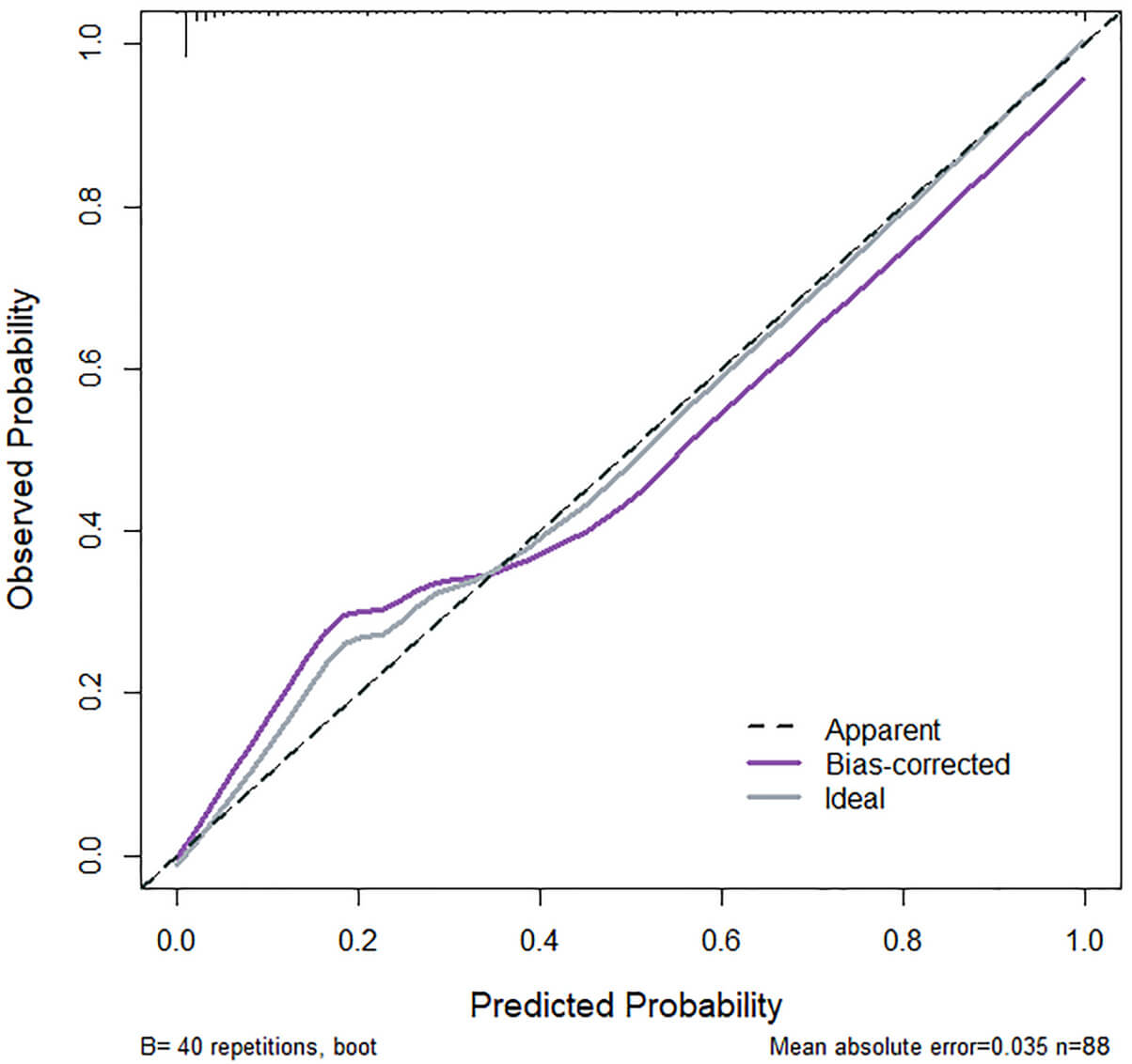 Fig. 3.
Fig. 3.
Calibration curve of the validation group. The curve has a slope closely resembling to 1, indicating that the model has a relatively good consistency between the predicted risk and the actual risk for sleep disorders in PCOS patients after ketogenic diet intervention.
For the modelling group, the model’s area under the ROC curve (AUC) was 0.9328, indicating high performance for predicting the development of sleep disorders in PCOS patients after ketogenic diet intervention, with a standard error of 0.019 (95% confidence interval [CI]: 0.892–0.954) and a Youden index of 0.75, along with sensitivity of 92.3% and specificity of 83.4%, as shown in Fig. 4. In the validation group, the model’s AUC was 0.8431, with a standard error of 0.032 (95% CI: 0.777–0.899) and a Youden index of 0.62, along with sensitivity of 78.5% and specificity of 83.3%, as depicted in Fig. 5.
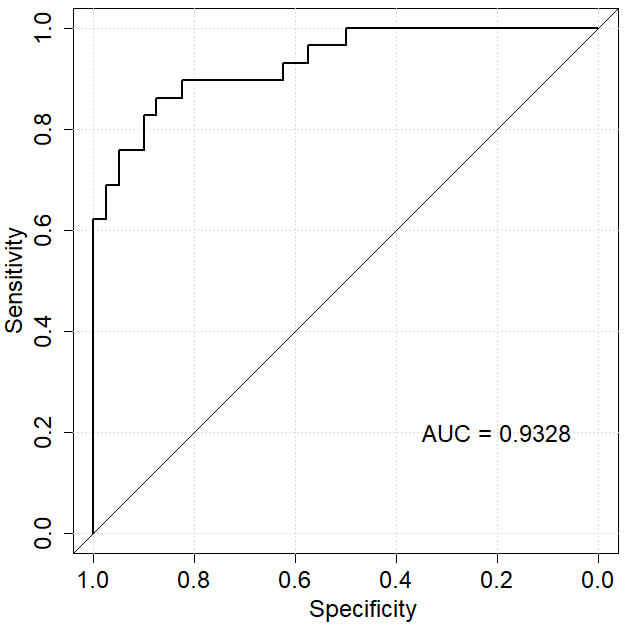 Fig. 4.
Fig. 4.
ROC curve of the modelling group. The AUC is close to 1, indicating excellent predictive performance of the model in the modelling group. Abbreviations: AUC, area under the ROC curve; ROC, receiver operating characteristic.
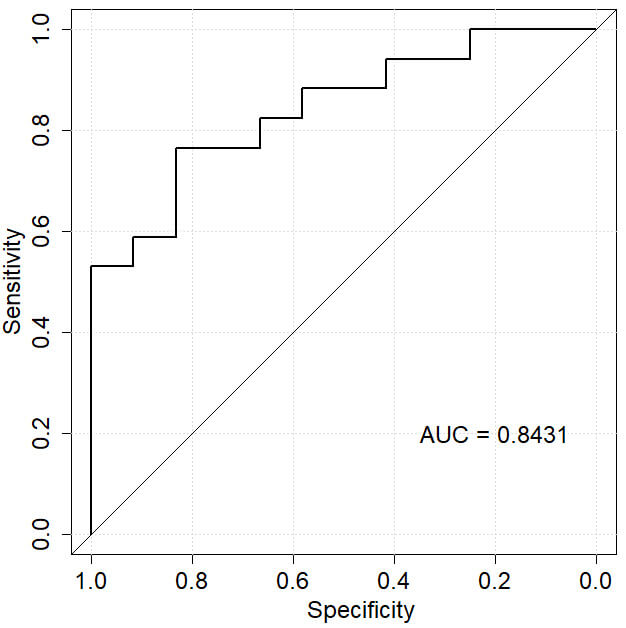 Fig. 5.
Fig. 5.
ROC curve of the validation group. With 0.7
To evaluate the clinical utility of the model in predicting therapeutic efficacy, DCA curves for the modelling and validation groups were plotted. The curves are close to the upper right and higher than the Non and All line benefits. Based on the results, it is evident that the model exhibits a clear positive net benefit, indicating good clinical utility (Figs. 6,7).
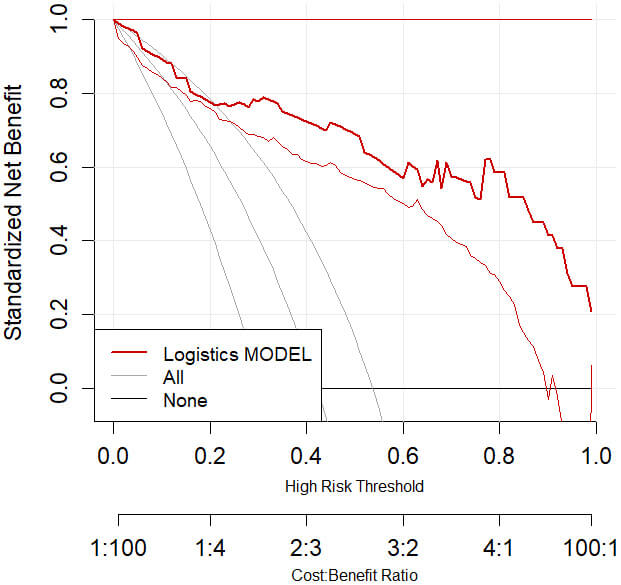 Fig. 6.
Fig. 6.
DCA curve of the modelling group. Abbreviation: DCA, decision curve analysis.
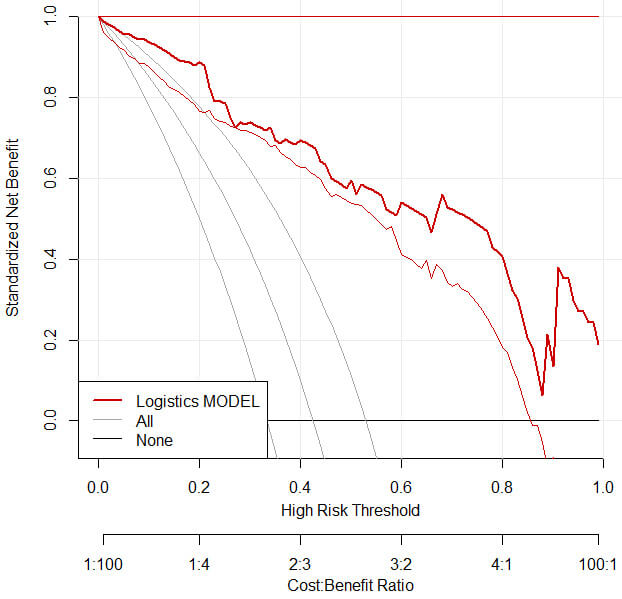 Fig. 7.
Fig. 7.
DCA curve of the validation group. Abbreviation: DCA, decision curve analysis.
This study, through an in-depth retrospective analysis, aims to reveal the factors influencing the occurrence of sleep disorders in PCOS patients following ketogenic diet intervention. By systematically collecting and analysing a large amount of clinical data, this study identified influencing factors and successfully constructed a predictive model with clinical application potential. This research not only deepens our understanding of the mechanisms underlying sleep disorders in PCOS patients following ketogenic diet intervention but also provides a scientific basis for personalised treatment and early intervention.
In this study, univariate analysis and binary logistic regression analyses were adopted to identify the main factors influencing the occurrence of sleep disorders in PCOS patients following ketogenic diet intervention. The results indicate that anxiety, depression, blood sugar level, and LDL-c level are significant influencing factors. The analysis suggests that PCOS patients often experience psychological stress and emotional fluctuations due to the impact of the disease [16]. The ketogenic diet is a specialised dietary approach that also involves significant adjustments to patients’ daily habits and alterations to their dietary structure, which may potentially increase psychological stress to some extent, thereby triggering or exacerbating anxiety and depression, ultimately leading to sleep disturbances. Research by Yang et al. [17] has demonstrated a significant relationship between anxiety/depression status and sleep conditions in PCOS patients, aligning closely with the findings of this study, further confirming the association between anxiety, depression, and sleep disturbances in PCOS patients. The ketogenic diet helps patients achieve a state of ketosis through a reduction in carbohydrate intake, which consequently lowers blood sugar levels [18]. However, excessively low blood sugar levels can lead to feelings of fatigue, dizziness and anxiety, thereby impacting sleep quality [19]. Furthermore, fluctuations in blood sugar levels may also have adverse effects on sleep. Research by Tasali et al. [20] demonstrated a close relationship between glucose tolerance in PCOS patients with the risk and severity of obstructive sleep apnea, providing concordant support to our findings that blood sugar levels are one of the significant factors influencing sleep disturbances in PCOS patients following ketogenic diet intervention. These findings collectively highlight the importance of closely monitoring patients’ blood sugar levels and taking necessary measures to maintain stable blood glucose levels during ketogenic diet interventions. Low-density lipoprotein cholesterol is a vital component of blood lipids, with elevated levels closely associated with cardiovascular disease. Interventions such as a ketogenic diet in PCOS patients can also impact LDL-c levels, leading to their fluctuations. The current study identified LDL-c levels as one of the factors influencing sleep disturbances in PCOS patients following the ketogenic diet. Hence, when implementing a ketogenic diet intervention, it is crucial to monitor patients’ lipid levels and take necessary steps to reduce LDL-c levels [21].
Advanced statistical methods like logistic regression analysis were employed in the model construction process to ensure its accuracy and reliability. Moreover, various methods such as ROC analysis, calibration curves, and DCA were used to evaluate the model’s utility, further validating its accuracy and reliability. Using logistic regression analysis, a predictive model incorporating factors such as anxiety, depression, blood sugar levels, and LDL-c was constructed to assess the risk of sleep disturbances in PCOS patients following the ketogenic diet. The comparative analysis of modelling and validation group data revealed that the model’s calibration curve slope is close to 1, and the high AUC detected through the ROC analyses indicated excellent sensitivity and specificity of the model, which are indicative of its high accuracy and reliability in application. In a comprehensive consideration of the impact of multiple factors such as anxiety, depression, blood sugar levels, and LDL-c on sleep disturbances, this predictive model enables a more holistic and accurate prediction of the risk of sleep disturbances in PCOS patients following ketogenic diet intervention. Thus, this model can assist with assessing the risk of sleep disturbances in PCOS patients following ketogenic diet intervention and provide guidance in the implementation of appropriate interventions, with the ultimate clinical goal of enhancing patient treatment outcomes and quality of life.
The predictive model established in this study holds significant promise for clinical applications. Firstly, the model can guide the development of ketogenic diet intervention plans for PCOS patients. By predicting the risk of developing sleep disturbances, physicians can promptly adjust dietary structures and intervention strategies to reduce the incidence of sleep disturbances. Secondly, the model can be utilised to evaluate the treatment outcomes of PCOS patients following ketogenic diet interventions. By comparing predicted risk values before and after treatment, physicians can objectively assess treatment effectiveness and make necessary adjustments in treatment strategies. Furthermore, the model can serve as a reference for research on other related diseases. For instance, researchers can draw inspiration from the current model construction approach and methods of this study to establish relevant predictive models when exploring the factors influencing the occurrence of sleep disturbances in patients with other endocrine or metabolic disorders following ketogenic diet interventions.
Several limitations of this research should be highlighted. First of all, due to the retrospective nature of research, this study is vulnerable to problems such as information and selection biases. Prospective research is needed in the future to further verify the accuracy and reliability of the model. Secondly, owing to the small sample size, the findings obtained in this study cannot be reliably generalised to other populations. Third, the lack of external verification (external verification refers to the process of secondary verification of conclusions using a data set or method independent of the original research sample in scientific research or data analysis) in this study limits the applicability of the model. Finally, the associations of variables detected in this study do not infer causality. Additionally, the impact of baseline anxiety/depression levels on sleep was not explored in this investigation. Patients with higher baseline anxiety/depression may have experienced worse-quality sleep before the ketogenic diet intervention; therefore, these factors are potential confounders which may interfere with the accuracy of the results. Taken together, subsequent baseline assessments need to be included to clarify causality. Furthermore, the impact of differences in ketogenic diet therapy on patient outcomes was not considered. Different lengths and types of treatment may engender varying effects on individual patients; for instance, short-term and long-term, strict ketogenic and modified ketogenic diets may impact sleep health differently. Subsequent research should refine these factors to more accurately assess their impact. In future investigations, subsequent studies should include more factors, including other potential confounders, for analysis to more accurately reveal the true connection between each factor and sleep. It is also necessary to expand the sample size and improve the statistical effectiveness of the research. In summary, data and model validation using a different cohort of patients is needed to refine the predictive model in terms of accuracy and reliability.
In conclusion, this study successfully established a model for predicting sleep disorders in PCOS patients following ketogenic diet intervention, which exhibits high levels of accuracy and reliability. The comprehensive incorporation of multiple influencing factors for sleep disorders in the construction of this model allows for more holistic and accurate prediction of the risk for sleep disorders in patients. Therefore, this model holds significant promises for clinical applications, providing practical guidance for enhancing treatment outcomes in this patient cohort and their quality of life. Moving forward, it is essential to further refine the model, in terms of accuracy and reliability, through prospective studies involving an expanded sample size.
All data included in this study are available from the corresponding author upon reasonable request.
WB designed the research study. MX and JL performed the research. MX analysed the data. MX drafted the manuscript. All authors contributed to the important editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
The study was approved by the Medical Ethics Committee of the Beijing Shijitan Hospital, Capital Medical University (IIT2024-113-001). This study was conducted in compliance with the Declaration of Helsinki, and all patients provided their informed consent.
Not applicable.
This research received no external funding.
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.