


1 Department of Cardiology, Tongxiang First People’s Hospital, 314500 Tongxiang, Zhejiang, China
2 Department of Emergency, Tongxiang First People’s Hospital, 314500 Tongxiang, Zhejiang, China
Abstract
Acute heart failure (AHF) is a prevalent critical condition in the emergency department. Conventional treatment approaches typically emphasise independent medical practices and lack structured physician-nurse collaborative education, which may adversely impact patient prognosis. This study aimed to evaluate the effectiveness of a physician-nurse collaborative education management model in patients with AHF in the emergency department.
A retrospective cohort study was conducted on 110 patients with AHF admitted to Tongxiang First People’s Hospital between January 2022 and January 2024. The control group (n = 47) received routine care, while the observation group (n = 63) received a physician-nurse collaborative education management intervention. Self-care ability, emotional status, quality of life, New York Heart Association (NYHA) functional classification, N-terminal pro-B-type natriuretic peptide (NT-proBNP) levels, length of hospital stay, 3-month readmission rate, and incidence of adverse events were compared between groups.
At baseline, no significant differences were observed between the two groups in the Self-Care of Heart Failure Index (SCHFI), Self-Rating Depression Scale (SDS), Self-Rating Anxiety Scale (SAS), Minnesota Living with Heart Failure Questionnaire (MLHFQ), NYHA functional classification, or NT-proBNP levels (all p > 0.05). Six months after discharge, both groups showed significant increases in SCHFI scores (p < 0.05), with the observation group achieving higher scores (p < 0.001). SDS and SAS scores decreased in both groups, but were significantly lower in the observation group (p < 0.001). MLHFQ scores improved in both groups (p < 0.05), with greater improvement in the observation group (p < 0.001). Furthermore, the observation group demonstrated better NYHA functional classification (p < 0.05), lower NT-proBNP levels (p < 0.05), shorter hospitalisation duration (p < 0.001), and reduced 3-month readmission rates and overall adverse event incidence (p < 0.05).
The physician-nurse collaborative education management model significantly enhances self-care ability, alleviates anxiety and depression, promotes cardiac functional recovery, and improves quality of life in AHF patients. Moreover, it reduces hospitalisation duration, readmission rates, and adverse events, supporting its potential for broader clinical application.
Keywords
- heart failure
- cooperative behaviour
- patient care management
- anxiety
- depression
- quality of life
Acute heart failure (AHF) is a rapidly progressive, life-threatening emergency associated with high mortality rates and significant psychological and financial burdens on patients and their families [1]. In clinical practice, treatment goals for AHF extend beyond rapid symptom relief and hemodynamic stabilisation to include long-term management aimed at improving cardiac function, reducing complications, and ultimately enhancing patient quality of life and prognosis [2]. Prognostic assessment in AHF remains challenging due to considerable variability in individual care needs [3]. Conventional outpatient nursing models, often lacking targeted interventions, struggle to meet these diverse needs, highlighting the urgency of implementing patient-centred advanced care planning [3, 4, 5].
In recent years, with continuous optimisation of healthcare delivery, health education has emerged as a critical component of comprehensive management, demonstrating effectiveness in disease control and promoting treatment adherence [5, 6]. In this context, physician-nurse collaboration has been introduced as a novel practice model in which multidisciplinary teams, especially physicians and nurses, jointly engage in clinical decision-making, coordinate treatment planning, and implement integrated interventions [7]. This model emphasises cooperative engagement, structured role division, and complementary expertise to deliver holistic health guidance [8]. Under this model, physicians formulate individualised treatment plans based on the conditions of the patient and enhance their disease awareness through professional explanations, while nurses integrate disease-related knowledge into daily life management using illustrated materials and video resources, thereby enhancing accessibility and practicality of educational content [9]. Evidence suggests that effective physician-nurse collaboration reduces the average length of hospital stay, decreases medical costs, and enhances patient satisfaction [10]. Clinical practice in China has further demonstrated significant outcomes in areas such as enhanced recovery after surgery [11] and radiation therapy safety in oncology [12]. Additionally, studies have shown that an interprofessional collaborative team approach can effectively alleviate patients’anxiety and depressive symptoms. [13, 14].
Despite these advances, the application of physician-nurse collaborative practice models in heart failure (HF) management remains limited, particularly in terms of verifying their effectiveness in complex, high-intensity emergency department settings [15]. Therefore, this study aimed to evaluate the comprehensive impact of this management model on self-care capacity, emotional well-being, quality of life, and clinical outcomes in patients with AHF. The findings from this study will provide a scientific foundation for standardising AHF management in emergency departments and inform future optimisation of health education models.
Inclusion criteria: (1) Meeting the diagnostic and treatment criteria for AHF
and confirmed diagnosis in the emergency department [16]; (2) Aged
Exclusion criteria: (1) Not the first hospitalisation for AHF; (2) Physical disabilities impairing assessment of activity capacity or preventing effective participation in a collaborative educational program; (3) Comorbidities requiring emergent management of severe cardiovascular conditions, including but not limited to: acute coronary syndrome (unstable angina or myocardial infarction), severe valvular disease requiring urgent intervention, cardiogenic shock, or persistent ventricular tachycardia or ventricular fibrillation; (4) Concomitant infectious diseases; (5) Hepatic or renal dysfunction; (6) Serious systemic comorbidities expected to significantly affect prognosis or interfere with intervention assessment, such as uncontrolled severe chronic obstructive pulmonary disease (COPD), uncontrolled severe diabetes mellitus, or active autoimmune disease requiring immunosuppressive therapy; (7) History of prior cardiac surgery; (8) Malignant tumors; (9) Pregnant or lactating women.
A total of 110 patients with AHF admitted to Tongxiang First People’s Hospital between January 2022 and January 2024 were included in this retrospective cohort study. Based on clinical records, patients were retrospectively grouped according to the nursing interventions they received during hospitalisation at the HF centre. Specifically, they were assigned to the control group (n = 47; conventional education management model) and the observation group (n = 63; collaborative education management model involving both physicians and nurses). This study was approved by the institutional Ethics Review Committee of Tongxiang First People’s Hospital (Approval number: 2024-207) and conducted following the principles outlined in the Declaration of Helsinki. Written informed consent was obtained from all participants.
The control group received a conventional education management intervention,
which included routine electrocardiograms and arterial blood gas monitoring every
15
The observation group received a physician-nurse collaborative health education management intervention, which differed from the standard care. Medical-nursing staffing and team organisation: Each team consisted of one cardiovascular specialist, one rehabilitation physician, one head nurse, six specialist nurses, and one psychologist. Volume assessment and management protocols were developed for HF patients, together with standardised documentation forms for examination indicators and precautions. The same medical-nursing team provided continuous care throughout hospitalisation, with defined responsibilities for each member to ensure clear task division and collaboration.
(1) Collaborative assessment and plan development: Upon admission, emergency
department physicians and responsible nurses jointly performed a comprehensive
evaluation of the patient’s condition using the “Standardised Examination Form
for Acute Heart Failure Patients Upon Admission” (Supplementary Material
1), including vital signs, cardiac function indices, and biochemical parameters.
Medical and nursing staff jointly discussed cases and performed collaborative
ward rounds according to the “Procedure Specifications for Collaborative Ward
Rounds in Acute Heart Failure” (Supplementary Material 2). Rounds were
conducted twice weekly, lasting 40
(2) Implementation of structured health education: Structured education was delivered using three complementary approaches:
Face-to-face education: Each session was conducted in a standardised education
room after the condition of the patient had stabilised (post-surgery, or 24–48
hours before discharge), with each session lasting 20
Illustrated materials: A concise, portable “Self-Management Handbook for Heart
Failure” (Supplementary Material 5) was designed by specialists and
rehabilitation physicians. It summarises key disease knowledge, medication
precautions, dietary adjustment principles (e.g., low-salt and low-fat diets),
and rehabilitation exercises, allowing patients to consult conveniently at any
time. Nurses distributed the handbook and guided patients through a 10
Video education: Short modular videos (2–3 minutes each) combine animations, live demonstrations, and expert narration to explain disease mechanisms, emergency management, lifestyle strategies, and rehabilitation practices. Patients watched 3–4 modules daily (total duration: 8–12 minutes), which increased engagement and improved comprehension (https://www.pule.com/xinlishuaijie/video/pn1/).
(3) Psychological intervention: Given the severity of illness and frequent
comorbid anxiety or depression in patients with AHF, a multidisciplinary medical
team delivered a standardised psychological intervention protocol within 24 hours
of hospital admission. This single session integrated empathetic active
listening, structured psychological assessment, and cognitive-behavioural
guidance, lasting 12–18 minutes. Each session lasts approximately 15
(4) Discharge nursing guidance: Personalised follow-up records and cyclic monitoring protocols with scheduled observation intervals were developed for each patient at discharge.
(5) Post-discharge follow-up: After patients were discharged, physicians and nurses conducted at least one follow-up per month (by phone or outpatient clinic) for a total of six months. Follow-up included a systematic assessment of cardiac function status, medication adherence, and lifestyle changes. At the same time, treatment and nursing plans were adjusted as needed to enhance treatment adherence, reduce readmission rates, and optimise treatment outcomes.
(1) Baseline data characteristics: Baseline information for all patients was obtained from the electronic medical record system before the nursing intervention. Variables included gender, age, educational level, history of hypertension, history of diabetes, New York Heart Association (NYHA) cardiac function classification, and N-terminal pro-B-type natriuretic peptide (NT-proBNP) level.
(2) Self-care ability assessment: The Self-Care of Heart Failure Index (SCHFI)
was used to evaluate self-management behaviours at baseline and six months
post-discharge in both groups [17]. The
scale comprises three dimensions: (i) Self-care maintenance, which evaluates
medication adherence, dietary management, exercise routines, and symptom
monitoring; (ii) Self-care management, which assesses the ability to recognise
symptoms and respond promptly; (iii) Self-care confidence, which measures
confidence in executing behaviours. Items were rated on a 4-point Likert scale,
with dimension scores standardised to a 0–100 scale. A total score of
(3) Psychological status assessment: The Self-Rating Depression Scale (SDS)
[18] and the Self-Rating Anxiety Scale (SAS) [19] were
used at baseline and six months post-discharge to evaluate the psychological
status of patients. Each scale consists of 20 items scored on a 4-point scale,
yielding a total score range of 20–80. For the SDS, a score
(4) Quality of life assessment: The Minnesota Living with Heart Failure Questionnaire (MLHFQ) was administered at baseline and six months post-discharge [20]. The MLHFQ includes 21 items covering three domains: physical (8 items), emotional (5 items), and other relevant aspects (8 items). Each item was scored on a 0–5 Likert scale, producing a total score between 0 and 105. Higher scores indicate poorer quality of life.
(5) NYHA functional classification: Cardiac function was evaluated at baseline and six months post-discharge according to the NYHA functional classification system [21]: Class I, no limitation of physical activity, symptoms of HF occur only during strenuous exercise; Class II, mild limitation of physical activity, symptoms develop during ordinary physical activity but resolve completely at rest; Class III, marked limitation of physical activity, symptoms are triggered by minimal exertion (e.g., light household tasks) and persist partially at rest; Class IV, severe limitation, symptoms are present at rest and worsen with any physical activity.
(6) Biomarker analysis: NT-proBNP levels were compared between the two groups. Fasting venous blood samples were collected for NT-proBNP determination at baseline and six months post-discharge.
(7) Clinical outcome measures: Clinical outcomes included: (i) Readmission rate, recorded via telephone follow-up for any readmission event within 3 months post-discharge; (ii) Length of hospital stay, defined as the total hospital days from admission until discharge criteria were met; (iii) Adverse event incidence, obtained from the electronic medical records and including arrhythmias, pneumonia, and acute angina pectoris.
Data were analysed using SPSS Version 26.0 (IBM Corporation, Armonk, NY, USA).
The Shapiro-Wilk test and Kolmogorov-Smirnov test were used to test the normality
of the variables. Normally distributed data were tested for homogeneity of variance
using Levene’s test and were expressed as mean
As shown in Fig. 1, a total of 110 patients with AHF were enrolled
according to the inclusion and exclusion criteria, comprising 47 in the control
group and 63 in the observation group. Baseline clinical characteristics of the
two groups are summarised in Table 1. The mean age was 73.92
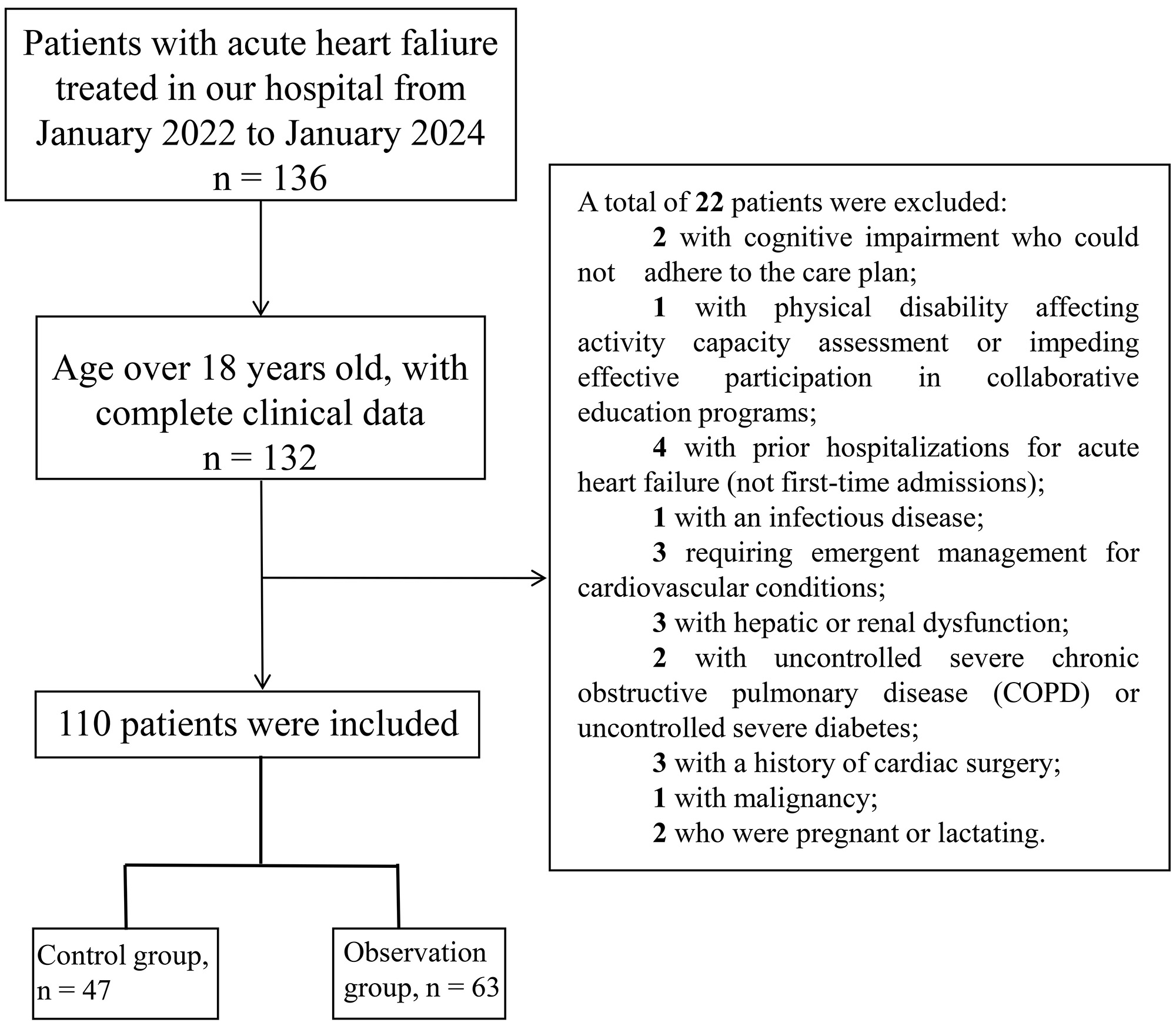 Fig. 1.
Fig. 1.
Flow chart of patient selection.
| Characteristic/Group | Control group (n = 47) | Observation group (n = 63) | t/Z | p-value | |
| Gender | 0.061 | 0.805 | |||
| Male | 25 (53.19) | 35 (55.56) | |||
| Female | 22 (46.81) | 28 (44.44) | |||
| Age (years) | 73.96 |
73.92 |
0.039 | 0.969 | |
| Educational level | 0.064 | 0.800 | |||
| High school and below | 31 (65.96) | 43 (68.25) | |||
| College or above | 16 (34.04) | 20 (31.75) | |||
| Hypertension, yes | 37 (78.72) | 48 (76.19) | 0.098 | 0.754 | |
| Diabetes mellitus, yes | 12 (25.53) | 17 (26.98) | 0.029 | 0.864 | |
| NYHA classification | 0.183 | 0.913 | |||
| II | 15 (31.91) | 21 (33.33) | |||
| III | 19 (40.43) | 23 (36.51) | |||
| IV | 13 (27.66) | 19 (30.16) | |||
| NT-proBNP level (ng/L) | 2775.80 (1131.70, 4440.00) | 3040. 20 (1933.30, 4117.40) | 0.208 | 0.835 | |
Notes: NYHA, New York Heart Association; NT-proBNP, N-terminal pro-B-type natriuretic peptide.
Prior to the nursing intervention, SCHFI scores across all dimensions were
comparable between the two groups, with no statistically significant difference
(p
| Group | Self-care maintenance | Self-care management | Self-care confidence | |||
| Before the intervention | After the intervention | Before the intervention | After the intervention | Before the intervention | After the intervention | |
| Control group (n = 47) | 36.19 |
41.72 |
34.59 |
38.64 |
38.55 |
46.64 |
| Observation group (n = 63) | 37.63 |
51.70 |
33.51 |
49.56 |
39.30 |
54.71 |
| t-value | 0.692 | 5.081 | 0.560 | 6.422 | 0.400 | 4.075 |
| p-value | 0.490 | 0.576 | 0.690 | |||
Notes: SCHFI, Self-Care of Heart Failure Index. Compared with pre-intervention in the same group,
*p
At baseline, SDS and SAS scores exhibited no statistically significant
differences between the two groups (p
| Group | SDS | SAS | ||
| Before the intervention | After the intervention | Before the intervention | After the intervention | |
| Control group (n = 47) | 54.62 |
44.04 |
56.49 |
43.26 |
| Observation group (n = 63) | 53.56 |
38.67 |
57.24 |
37.86 |
| t-value | 0.658 | 4.971 | 0.428 | 4.291 |
| p-value | 0.512 | 0.670 | ||
Notes: SDS, Self-Rating Depression Scale; SAS, Self-Rating Anxiety
Scale. Compared with
pre-intervention in the same group, **p
Before the nursing intervention, no significant differences were observed in
MLHFQ scores across all domains between the two groups (all p
| Group | Body | Emotion | Others | |||
| Before the intervention | After the intervention | Before the intervention | After the intervention | Before the intervention | After the intervention | |
| Control group (n = 47) | 26.64 |
20.49 |
19.30 |
15.72 |
26.68 |
23.74 |
| Observation group (n = 63) | 27.84 |
16.35 |
20.35 |
11.29 |
25.46 |
19.76 |
| t-value | 1.018 | 5.967 | 1.632 | 5.322 | 1.195 | 4.222 |
| p-value | 0.311 | 0.106 | 0.235 | |||
Notes: MLHFQ, Minnesota Living with Heart Failure Questionnaire;
At baseline, there was no statistically significant difference in the
distribution of NYHA functional classes between the two groups (p
| Group | Before the intervention | After the intervention | ||||||
| I | II | III | IV | I | II | III | IV | |
| Control group (n = 47) | - | 15 (31.91) | 19 (40.43) | 13 (27.66) | 5 (10.64) | 18 (38.30) | 18 (38.30) | 6 (12.77) |
| Observation group (n = 63) | - | 21 (33.33) | 23 (36.51) | 19 (30.16) | 16 (25.40) | 31 (49.21) | 12 (19.05) | 4 (6.35) |
| 0.183 | 8.667 | |||||||
| p-value | 0.913 | 0.034 | ||||||
Before the nursing intervention, there was no statistically significant
difference in NT-proBNP levels between the two groups (p
| Group | Before the intervention | After the intervention |
| Control group (n = 47) | 2775.80 (1131.70, 4440.00) | 2089.10 (867.90, 3434.30)** |
| Observation group (n = 63) | 3040.20 (1933.30, 4117.40) | 1296.50 (598.50, 2222.50)** |
| Z | 0.208 | 2.438 |
| p-value | 0.835 | 0.015 |
Notes: NT-proBNP, N-terminal pro-B-type natriuretic peptide. Compared with pre-intervention in the same
group, **p
Following the nursing intervention, the mean length of hospital stay in the
observation group was 10.20
| Group | Length of hospital stay (days) | Rehospitalisation rate |
| Control group (n = 47) | 13.13 |
10 (21.28) |
| Observation group (n = 63) | 10.20 |
5 (7.94) |
| t/ |
7.154 | 4.068 |
| p-value | 0.044 |
Notes: n (%), frequencies and percentages.
| Group | Arhythmia | Angina pectoris | Pulmonary infection | Total |
| Control group (n = 47) | 3 (6.38) | 4 (8.51) | 4 (8.51) | 11 (23.40) |
| Observation group (n = 63) | 1 (1.59) | 1 (1.59) | 1 (1.59) | 3 (4.76) |
| - | - | - | - | |
| p-value | 0.311 | 0.162 | 0.162 | 0.007 |
Notes: n (%), frequencies and percentages.
The findings of this study demonstrate that, compared with conventional nursing, the physician-nurse collaborative health education management model significantly improves self-care behaviours, alleviates negative emotional states, and improves quality of life in AHF patients. The effectiveness of the physician-nurse collaboration model likely stems from its structured integration of patient education, psychological support, and personalised care planning, which collectively empower patients to actively participate in disease management. Improved adherence to self-care practices may contribute to physiological stability, as evidenced by the significant reduction in NT-proBNP levels and the enhanced NYHA functional classification in the intervention group. Furthermore, the marked decreases in anxiety and depression scores highlight the critical role of addressing psychological barriers to optimise treatment outcomes. The shorter hospital stays and lower readmission rates further validate the clinical value of this model in enhancing recovery while reducing healthcare burden.
Enhancing self-care capability is a global priority in multidisciplinary HF management programs and represents a crucial determinant of outcomes in patients with HF [22]. Knowledge gaps and cognitive misconceptions contribute significantly to inadequate self-management capacity in HF patients, thereby negatively impacting disease prognosis. In China, patients with chronic HF often lack disease-related skills and exhibit significant room for improvement in knowledge and self-care behaviours, with self-care levels demonstrating a positive correlation with knowledge acquisition [23]. In this study, six months after discharge, the observation group demonstrated significantly superior self-management abilities compared with the control group. The mechanisms underlying this improvement may be attributed to several multidimensional intervention strategies. First, systematic face-to-face education provided patients with a structured framework of knowledge and practical guidance for skill development. Second, the use of diversified health education formats (e.g., videos, illustrated materials) reinforced comprehension and facilitated the internalisation of disease management principles. Third, efficient physician-patient communication channels enabled timely professional clarification of patient concerns. Additionally, the HF management diary served as a behavioural reinforcement tool; its continuous recording and feedback mechanisms promoted the acquisition and maintenance of healthy behaviours, thereby significantly improving self-care adherence and initiative by the patients [24].
The findings of this study also indicate that depression and anxiety scores were significantly lower in the observation group compared with the control group following the nursing intervention. This outcome aligns with the conclusions of Guan et al. [25], who demonstrated that a physician-nurse collaborative intervention model effectively alleviates anxiety and depression among cervical cancer patients undergoing three-dimensional intracavitary brachytherapy. Extending these observations, the present study reveals that multidimensional psychological interventions delivered within a medical-nursing collaborative framework can significantly improve emotional disturbances in patients with AHF. This healthcare management model, grounded in empathetic communication (e.g., active listening, positive encouragement), fosters doctor-patient trust and strengthens psychological adaptability to disease management. This mechanism may hold universal applicability, as similar patient-centred intervention frameworks combining CBT and relaxation training have demonstrated significant efficacy in alleviating negative emotions during breast cancer treatment. This suggests that psychological interventions within medical-care collaboration frameworks may extend their value beyond specific disease categories [26].
The results of this study indicate that post-intervention, patients in the observation group demonstrated significantly improved scores across three domains of the MLHFQ (physical function, emotional state, and other influencing factors) compared with the control group. These findings suggest that the medical-nursing collaborative education model holds substantial advantages in enhancing the quality of life among HF patients. Unlike conventional nursing models primarily centred on disease treatment, the core feature of the medical-nursing cooperative health education lies in its specialised division of labor and coordinated management. Physicians primarily contribute professional medical expertise concerning disease pathology and treatment regimens, while nurses focus on guiding patients in daily self-care behaviours, including dietary regulation, medication adherence, exercise rehabilitation, and follow-up scheduling [27]. Through complementary role allocation, this collaborative model establishes a closed-loop system of “disease treatment-nursing support-self-management”, effectively alleviating emotional and physical symptoms in AHF patients. Furthermore, dynamic intervention strategies ensure continuous optimisation of the management framework. Regular follow-up assessments, structured health education sessions, and close symptom monitoring allow the medical team to promptly identify non-adherence or fluctuations in patient conditions, enabling timely adjustments to individualised intervention protocols [28, 29]. This evidence-based feedback mechanism transforms health education from a static approach into a dynamic, continuously improving process. Notably, the conclusions of this study align closely with the observations of Guan et al. [25] in cervical cancer patients undergoing three-dimensional intracavitary brachytherapy, further supporting the universal applicability and effectiveness of the medical-nursing collaborative health education management model across diverse clinical settings.
The NYHA functional classification of patients and the serum NT-proBNP level in the observation group showed significant improvement compared with the control group. NT-proBNP, an endogenous hormone secreted by ventricular myocytes, reflects the degree of myocardial stress and serves as a key biomarker for clinically assessing the severity of HF [30]. The collaborative education model optimises self-management behaviours, such as consistent medication adherence and strict fluid control, by providing comprehensive, standardised guidance to patients with AHF. This integrated approach contributes to enhanced cardiac function and promotes recovery, aligning with previous findings that highlight the effectiveness of multidisciplinary healthcare interventions in HF management [4].
The study also revealed that patients in the observation group had significantly shorter hospital stays and a lower overall incidence of adverse events compared with the control group. This finding suggests that the collaborative management model holds advantages in accelerating recovery cycles, primarily due to more efficient utilisation of medical resources and reduced risks of complications during hospitalisation. For example, nursing staff provided sustained psychological support and behavioural guidance to alleviate patient anxiety and treatment resistance, while the medical team dynamically adjusted therapeutic strategies to maintain optimal treatment outcomes [31]. Notably, the model demonstrated significant improvements in post-discharge prognosis, as evidenced by a marked reduction in readmission rates. Under conventional nursing models, patients often experience challenges in self-management post-discharge due to insufficient health knowledge and inadequate behavioural guidance [4]. In contrast, the physician-nurse collaborative education framework establishes an “in-hospital-outpatient” continuum of care. Through repeated follow-ups and dynamic assessments, healthcare professionals collectively supported patients in adopting evidence-based lifestyles and treatment habits, thereby reducing readmission risk [32].
Discharge interventions improved patient adherence to rational dietary practices, consistent medication use, healthy behaviours, and timely follow-up examinations. During the outpatient phase, enhanced adherence facilitated favourable outcomes such as healthier lifestyles, reduced medical non-compliance, and improved disease control [33]. Monthly follow-ups allowed both healthcare providers and patients to promptly detect condition changes, facilitating timely therapeutic adjustments to prevent exacerbations and relapses. Ultimately, this long-term dynamic approach yielded superior clinical outcomes [34, 35].
Despite these promising findings, several limitations should be acknowledged. First, the retrospective design of this study may introduce selection bias, while the relatively small sample size limits the generalizability of the findings. Second, the limited follow-up duration (6 months) constrains the evaluation of the long-term impact of the model on patient prognosis. Future studies should adopt extended follow-up periods to assess long-term outcomes. Finally, the single-institution setting of this study limits external validity and may not accurately reflect practices in other healthcare contexts. Future investigations on physician-nurse collaborative health education management models should therefore include randomised controlled trials across multiple institutions, with long-term follow-up, to provide more robust and generalizable evidence.
The findings of this study demonstrate that an education management model for AHF patients based on physician-nurse collaboration, by integrating professional resources, delivering structured self-management support, and offering continuous psychological counselling, significantly and practically enhances the self-care capabilities of patients. It also effectively alleviates psychological distress, including anxiety and depression, thereby contributing to a measurable improvement in overall quality of life. More importantly, this model exhibits marked value in optimising clinical pathways, as reflected in shorter hospital stays, reduced short-term risk of rehospitalisation due to exacerbation of HF in the short term, and lower incidence of adverse cardiovascular events during hospitalisation. These comprehensive benefits validate the core advantage of this collaborative model in strengthening individualised care for AHF patients, while underscoring its potential value in optimising resource allocation, improving patient flow efficiency, and enhancing overall medical safety within the critical setting of emergency departments. Implementation of this model not only provides a feasible framework for improving the short-term prognosis of AHF patients but also establishes a foundation for future investigations into broader applications, cost-effectiveness analysis, and multicentre validation studies. Collectively, these outcomes highlight its clinical translational potential and prospects for broader implementation.
All data included in this study are available from the corresponding author upon reasonable request.
GW had the original conception of the work. PL, DC, JS and FY collected the clinical data. PL, GW and JS performed the research. GW drafted the manuscript. All authors contributed to the important editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
This study was approved by the institutional Ethics Review Committee of Tongxiang First People’s Hospital (Approval number: 2024-207) and conducted following the principles outlined in the Declaration of Helsinki. Written informed consent was obtained from all participants.
Not applicable.
This research received no external funding.
The authors declare no conflict of interest.
Supplementary material associated with this article can be found, in the online version, at https://doi.org/10.31083/BJHM50382.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.