
† These authors contributed equally.
Academic Editor: Peter A. McCullough
The aim of our study is to evaluate the association of rotational atherectomy (RA) operation procedural indices and baseline lipid parameters with the prognosis of the patients with severe coronary calcification who underwent RA. Our study population consists of 287 patients treated with RA in Fuwai Hospital from January 2013 to December 2019. We analyzed the patients’ rotation procedural indices including the number of burrs, the size of burrs, approach site, the size of guiding catheter, along with the baseline level of lipoprotein(a) (Lp(a)), low-density lipoprotein-cholesterol (LDL-C) and high-sensitivity C-reactive protein (hs-CRP) to examine the association of these measurements with the prognosis of these patients using Cox regression analysis and Kaplan-Meier survival analysis. We find that during the follow-up period of 56.7 months with the median, the use of single burr in the patients who underwent RA was significantly associated with the occurrence of cumulative major adverse cardiac events (MACE) when compared with using non-single burrs [Hazard Ratio (HR) 0.43, 95% confidence interval (95% CI) 0.24–0.77, p = 0.004] from univariate Cox regression analysis; (HR 0.36, 95% CI 0.20–0.66, p = 0.001) from multivariate Cox regression analysis In addition, we find a higher event-free survival rate in the single-burr group after Kaplan-Meier survival analysis (Log rank p = 0.0033). However, there was no significant association of the size of burrs with the occurrence of MACE (HR 0.90, 95% CI 0.47–1.73, p = 0.76). Similarly, we find no significant associations between the approach site and the occurrence of MACE (HR 0.79, 95% CI 0.24–2.53, p = 0.69), the baseline Lp(a) (HR 1.07, 95% CI 0.76–1.49, p = 0.71), the level of LDL-C (HR 0.83, 95% CI 0.55–1.26, p = 0.38) or hs-CRP (HR 0.85, 95% CI 0.45–1.58, p = 0.60). We find that the patients who receive RA with a single burr have better outcomes than those who receive RA with non-single burrs. Moreover,we find that the number of burrs used in RA instead of the size of burrs, approach site, the size of guiding catheter, or baseline levels of Lp(a), LDL-C or hs-CRP had significant association with the prognosis of RA patients.
Coronary heart disease (CHD) is the leading cause of mortality and morbidity worldwide, and arterial calcification is strongly associated with poor prognosis of CHD [1, 2]. Previous studies have shown that the higher coronary artery calcification (CAC) was associated with the higher risk for atherosclerotic cardiovascular disease, and the CAC score has been regarded as an effective tool for predicting cardiovascular risk [1, 3, 4, 5].
Percutaneous coronary intervention (PCI) is one important treatment for CHD, but
calcified lesions have been found to increase the possibility of failure in stent
delivery [2]. To avoid this problem, the rotational atherectomy (RA) adopted
differential cutting to ablate atherosclerotic plaques by forward advancement of
a rotating abrasive diamond-encrusted burr [6]. RA can effectively reduce the
plaque volume and enlarge the lumen, which allows easier stent deployment [7, 8, 9],
and plaque modification has been shown to decrease the risk of stent restenosis
and malapposition [10, 11, 12, 13]. RA has been traditionally performed via the
transfemoral approach, mostly utilizing large guide catheters [
Many studies have also examined the relationship between heart patients’ blood chemistry and their prognosis. Plasma lipoprotein(a) [Lp(a)], low density lipoprotein cholesterol (LDL-C), and inflammatory factor high sensitivity C-reactive protein (hs-CRP) have all been shown to be related to the prognosis of patients with atherosclerotic cardiovascular disease (ASCVD) [1, 14, 15]. Importantly, Lp(a) has been shown to be a causal risk factor for CAC [16, 17, 18, 19]. However, it remains uncertain whether the level of Lp(a), LDL-C or hsCRP is related to the prognosis of patients who undergo RA, a relationship we aim to clarify in our study.
In our study, we examine the prognosis and contributing factors in 287
individuals who underwent RA from January 2013 to December 2019 at Fuwai
Hospital. According to the RA procedural routine of our hospital, the
characteristics of lesion calcification were generally as ring with 360
We collected fasting plasma samples in the morning from all the patients, and measured plasma levels of total cholesterol (TC), triglyceride (TG), LDL-C, high-density lipoprotein cholesterol (HDL-C), and hsCRP using an automatic biochemistry analyzer (Hitachi 7150, Tokyo, Japan). And the serum Lp(a) levels using an immune-turbidimetry assay (LASAY Lp(a) auto; SHIMA laboratories, Tokyo, Japan).
All patients received follow-up examinations regularly, with a median period of follow-up of 56.7 months (30–73 months). We defined MACE as the composite of cardiac death, nonfatal myocardial infarction (MI), nonfatal stroke, unstable angina pectoris and target lesion revascularization (TLR) and hospitalization with unstable angina (UA). For the dead patients, the events were reported by their relatives. Our definition for a diagnosis of nonfatal myocardial infarction (MI) was positive cardiac troponins with typical chest pain or typical electrocardiogram (ECG) serial changes, and we defined stroke as persistent neurological dysfunction with documentation of acute cerebral infarction on computed tomography and/or magnetic resonance imaging. Finally, we use PCI or coronary artery bypass graft (CABG) during the follow-up period to indicate TLR.
According to the PCI guidelines, procedures were performed via the radial or
femoral route by experienced operators. The indications for RA included (1)
severe calcification lesions with 360
We perform statistical analyses using the R language (version 4.0.4, Feather
Spray; The R Foundation for Statistical Computing, Vienna, Austria) and measure
statistical significance as any p-value
Table 1 shows the baseline characteristics of the study population. We find no
significant differences in the single-burr group and non-single burr group in
ages (67.73
| Single burr group (n = 168) | Non-singleburr group (n = 119) | p | ||
| Age (y) | 67.73 |
67.28 |
0.65 | |
| Male, n (%) | 116 (69.05) | 75 (63.03) | 0.35 | |
| BMI (kg/m |
24.74 |
24.81 |
0.85 | |
| Hypertension, n (%) | 125 (74.40) | 81 (68.07) | 0.30 | |
| Hyperlipidemia, n (%) | 144 (85.71) | 96 (80.67) | 0.33 | |
| Diabetes mellitus, n (%) | 75 (44.64) | 45 (37.82) | 0.30 | |
| Smokers, n (%) | 85 (50.60) | 52 (43.70) | 0.30 | |
| Previous CABG, n (%) | 6 (3.57) | 2 (1.68) | 0.55 | |
| SBP (mmHg) | 135.51 |
135.87 |
0.88 | |
| DBP (mmHg) | 74.75 |
74.60 |
0.91 | |
| LVEF (%) | 60.98 |
59.45 |
0.25 | |
| HbA1c (%) | 6.77 |
6.59 |
0.29 | |
| Lp(a) (mg/L) | 120.9 [53.98–311.67] | 172.83 [52.2–418.45] | 0.08 | |
| TC (mmol/L) | 4.17 |
4.02 |
0.60 | |
| TG (mmol/L) | 2.15 |
1.56 |
0.41 | |
| HDL-C (mmol/L) | 1.26 |
1.27 |
0.86 | |
| LDL-C (mmol/L) | 2.19 |
2.12 |
0.43 | |
| hs-CRP (mg/L) | 1.18 [0.48–2.20] | 1.37 [0.63–3.41] | 0.24 | |
| eGFR (mL/min·1.73 m |
79.07 |
76.56 |
0.30 | |
| Clinical diagnosis | 0.015 | |||
| Stable angina, n (%) | 86 (72.3) | 146 (86.9) | ||
| Unstable angina, n (%) | 3 (2.5) | 1 (0.6) | ||
| NSTEMI, n (%) | 22 (18.5) | 17 (10.1) | ||
| STEMI, n (%) | 8 (6.7) | 4 (2.4) | ||
| Medications at follow-up, n (%) | ||||
| Aspirin | 167 (99.40) | 119 (100.00) | - | |
| ACEI/ARB | 31 (18.45) | 24 (20.17) | 0.83 | |
| 123 (73.21) | 95 (79.83) | 0.25 | ||
| Clopidogrel | 144 (85.71) | 100 (84.03) | 0.82 | |
| Statins | 163 (97.02) | 118 (99.16) | 0.41 | |
| Stent implantation, n (%) | 0.07 | |||
| 0 | 30 (17.86) | 16 (13.45) | ||
| 1 | 28 (16.67) | 35 (29.41) | ||
| 2 | 85 (50.60) | 46 (38.66) | ||
| 3 | 22 (13.10) | 19 (15.97) | ||
| 4 | 3 (1.79) | 3 (2.52) | ||
| Approach site | 0.85 | |||
| Radial (brachial) | 153 (91.07) | 110 (92.44) | ||
| Femoral | 15 (8.93) | 9 (7.56) | ||
| Burr:artery ratio | 0.52 |
0.51 |
0.46 | |
| Guiding catheter size, n (%) | 0.99 | |||
| 6F | 103 (61.31) | 72 (60.50) | ||
| 7F | 65 (38.69) | 47 (39.50) | ||
| Size of burrs, n (%) | ||||
| small |
136 (80.95) | 90 (75.63) | 0.35 | |
| large |
32 (19.05) | 29 (24.37) | ||
| Target vessel, n (%) | 0.85 | |||
| LAD | 122 (72.62) | 92 (77.31) | ||
| LCX | 13 (7.74) | 5 (4.20) | ||
| RCA | 33 (19.64) | 22 (18.49) | ||
| Cumulative MACE, n (%) | 24 (14.29) | 31 (26.05) | 0.02* | |
| TLR | 2 (1.19) | 3 (2.52) | 0.70 | |
| Cardiac death | 9 (5.36) | 6 (5.04) | 1.00 | |
| Stroke | 4 (2.38) | 11 (9.24) | 0.02* | |
| Nonfatal MI | 2 (1.19) | 1 (0.84) | 1.00 | |
| Hospitalization with UA | 7 (4.17) | 10 (8.40) | 0.21 | |
| BMI, body mass index; CABG, coronary artery bypass graft; SBP, systolic blood
pressure; DBP, diastolic blood pressure; LVEF, left ventricular ejection
fraction; eGFR, estimated glomerular filtration rate; TC, total cholesterol; TG,
triglyceride; HDL-C, high-density lipoprotein; LDL-C, low-density lipoprotein;
hs-CRP, high-sensitivity C-reactive protein; ACEI, angiotensin-converting enzyme;
ARB, angiotensin receptor blocker; LAD, left anterior descending; LCX, left
circumflex; RCA, right coronary artery; TLR, target lesion revascularization; MI,
myocardial infarction, UA, unstable angina. * indicates p | ||||
We find that the use of a single burr in RA patients significantly associated with the occurrence of MACE when compared to using non-single burr produces (HR 0.43, 95% CI 0.24–0.77, p = 0.004 from univariate Cox regression analysis; HR 0.36, 95% CI 0.20–0.66, p = 0.001 from multivariate Cox regression analysis, Table 2). Furthermore, we find that there was higher event-free survival probability in the single-burr group after Kaplan-Meier survival analysis (Log-rank p = 0.0065, Fig. 1). However, there we find no significant association of the size of burrs with the occurrence of MACE (HR 0.9, 95% CI 0.47–1.73, p = 0.76, Table 2).
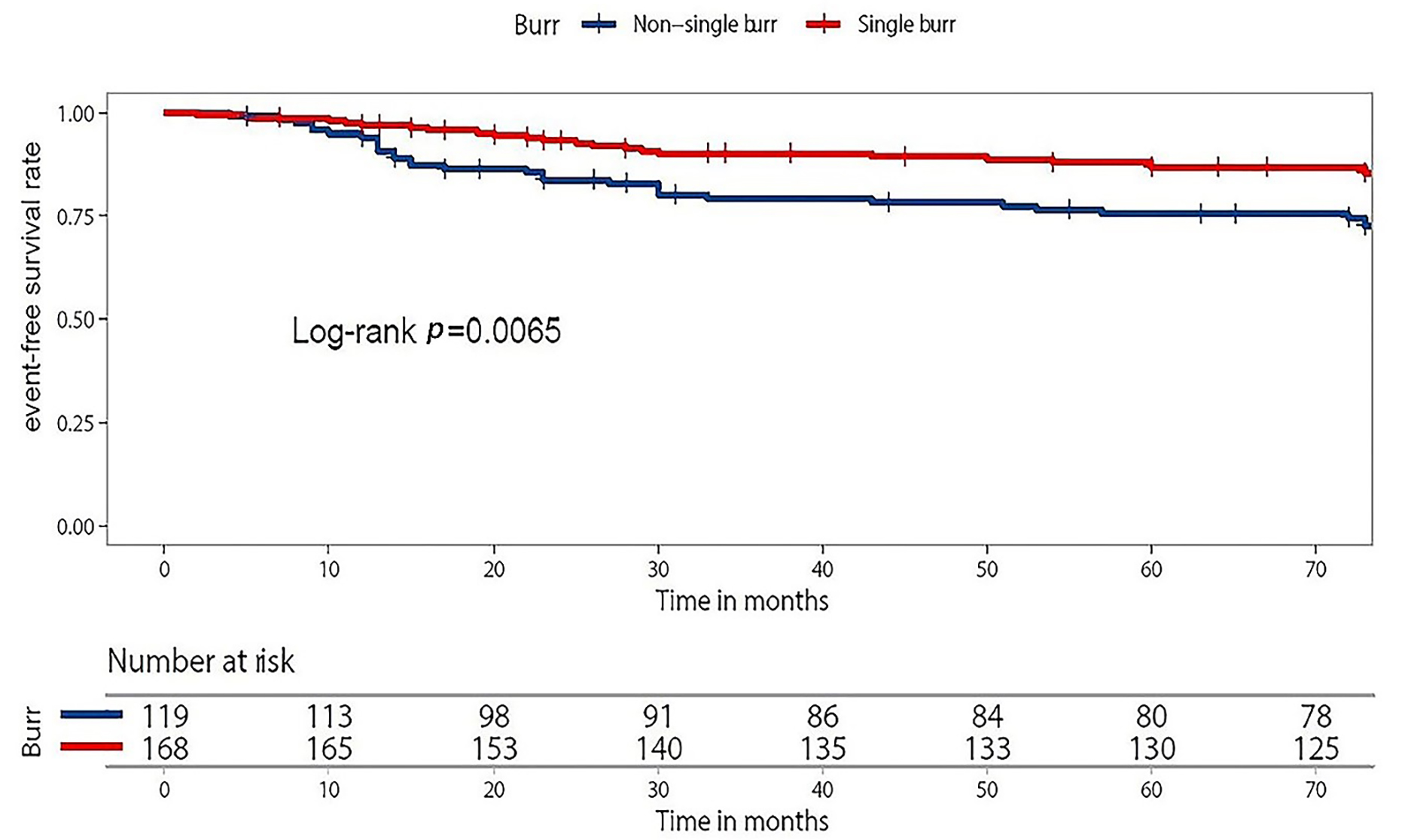 Fig. 1.
Fig. 1.Kaplan-Meier curve in the single-burr group and non-single-burr group. Overall 287 patients were categorized into non-single burr group (n = 119) and single burr group (n = 168). During the median period of follow-up of 56.7 months (30–73 months), the single-burr group had higher event-free survival probability (Log-rank p = 0.0065).
| Univariate Cox regression analysis | Multivariate Cox regression analysis | ||||||
| HR | 95% CI | p | HR | 95% CI | p | ||
| Male | 1.16 | 0.63–2.13 | 0.64 | ||||
| Age | 1.03 | 0.99–1.07 | 0.11 | 1.04 | 1.00–1.07 | 0.07 | |
| ACS | 1.24 | 0.58–2.64 | 0.58 | ||||
| BMI | 0.96 | 0.87–1.05 | 0.37 | ||||
| Hypertension | 0.88 | 0.48–1.6 | 0.67 | 0.79 | 0.41–1.50 | 0.47 | |
| smoking | 0.97 | 0.56–1.71 | 0.93 | 1.25 | 0.68–2.29 | 0.47 | |
| DM | 1.14 | 0.65–2.01 | 0.64 | 1.23 | 0.67–2.26 | 0.50 | |
| LDL-C | 0.83 | 0.55–1.26 | 0.38 | 0.81 | 0.53–1.24 | 0.34 | |
| hs-CRP | 0.85 | 0.45–1.58 | 0.60 | 0.69 | 0.37–1.31 | 0.26 | |
| eGFR, | 0.79 | 0.37–1.68 | 0.54 | ||||
| LVEF | 1.02 | 0.99–1.05 | 0.27 | ||||
| Lp(a) | |||||||
| low-level | Ref | ||||||
| medium level | 0.81 | 0.4–1.64 | 0.56 | ||||
| high level | 1.07 | 0.76–1.49 | 0.71 | ||||
| Single burr | 0.43 | 0.24–0.77 | 0.004* | 0.36 | 0.20–0.66 | 0.001* | |
| Guiding catheter size | 1.43 | 0.78–2.6 | 0.25 | ||||
| Approach site | 0.79 | 0.24–2.53 | 0.69 | ||||
| Burr/artery ratio | 1.88 | 0.11–3.26 | 0.67 | ||||
| Size of burrs | 0.90 | 0.47–1.73 | 0.76 | ||||
| ACS, acute coronary syndrome; BMI, body mass index; DM, diabetes mellitus;
LDL-C, low-density lipoprotein-cholesterol; hs-CRP, high-sensitivity C-reactive
protein; eGFR, estimated glomerular filtration rate; LVEF, left ventricular
ejection fraction; Lp(a), lipoprotein(a); * indicates p | |||||||
For the approach site, and guiding catheter size, we find no significant association between the approach site (transradial or transfemoral) and occurrence of MACE after univariate or multivariate Cox regression analysis (HR 0.79, 95% CI 0.24–2.53, p = 0.69, Table 2) and similarly, find no significant association between guiding catheter size (6F or 7F) (HR 1.43, 95% CI 0.78–2.6, p = 0.25, Table 2). In addition, our univariate Cox regression analysis shows no statistically significant association of burr-to-artery ratio with the occurrence of MACE (HR 1.88, 95% CI 0.11–3.26, p = 0.67, Table 2).
We divide all patients into three groups according to the tertile of Lp(a)
level. The low-level group includes patients with Lp(a)
We find no statistically associations between the level of Lp(a) and the
occurrence of MACE after univariate Cox regression analysis (p
CAC was defined as mineral deposition in the coronary artery wall, which was very common in the aging population of the world [20, 21]. In routine PCI procedure, CAC could impair stent delivery and expansion. Importantly, it was highly predictive for MACE. So heavily calcified lesions need to be treated by RA to facilitate subsequent procedures [1, 2]. In the European expert consensus on RA, they recommended during RA, the operators could choose burrs step by step through burrs upsizing or downsizing [6]. However, there is scant data on whether the number or size of burrs is associated with long-term outcomes for the patients who underwent RA.
In this study, we analyzed the association between RA operation procedural indices and the prognosis of patients undergoing RA after a median of 56.7 months follow-up period. In our study, RA procedures were performed according to the operators’ experience and the routine about RA of out hospital in both the groups, including that the operators checked the calcification lesion by IVUS before RA, or they decided to perform RA procedure after they failed to dilate the lesion by post-dilated balloon or cutting balloon. And they usually used cutting balloon or post-dilated balloon to dilate the lesion fully after RA. Under the abovementioned background about procedural details, the analysis showed that using single burr during RA was related with lower rate of MACE and higher event-free survival rate (Log-rank p = 0.0065). We speculated that the possible explanations included that optimization of choosing the single burr during RA was enough to facilitate the procedure of intervention about severe calcification lesions, and in addition, choosing the optimal single burr, not 2 or more burrs could shorten the whole procedural time, and had more possibility to choose transradial access and less puncture-site related complications. In previous studies, using large burrs, which was more possible in non-single-burr group, didn’t improve the outcomes of the patients undergoing RA. Moreover, the experience from Taiwan local hospital supplied convincing evidence supporting the use of a single-burr strategy for RA to treat complex calcified coronary lesions rather than a routine step-by-step strategy for RA [22].
This study finds that appropriate burr size is vital for treatment of CAC during
RA. We divided burrs into small (1.25 mm and 1.5 mm) and large (1.75 mm and 2.0
mm) groups and saw that, a burr-to-artery ratio
Chiou et al. [22] find that the single-burr strategy had the same result compared to the step-up approach pursuant to its advantages of less procedure time and complications. Levi et al. [23] report that 151 patients with small burrs achieve successful procedure, in comparison with 58 patients received the large burr (93% vs 100%, p = 0.07). In a long-term of 2616 days follow-up study about RA from a single center, Bartuś et al. [24] found that both high-risk category and mean stent(s) length were identified as independent predictors of MACCE. EuroSCORE II was confirmed to be the only independent predictor of MACE after RA [24].
However, approach site also plays an important role in the RA procedure. As reported previously, the procedural success rate and long-term prognosis were found to be similar between the transfemoral approach (TFA) and transradial approach (TRA) in routine PCI without RA procedures, but radial access had a lower risk of in-hospital major bleeding, major access site complications and longer hospital stay [6, 25]. Watt et al. [25] find TRA has the same procedural success as TFA (95.2% vs 94.9%, p = 0.56) and that TRA has a lower incidence of major access site complications than TFA (0.04% vs 1.3%, p = 0.004). Similarly, Kübler et al. [26] suggest that TRA is associated with equivalent procedural success compared to TFA (95% vs 87%, p = 0.07). However, they find that TFA is prone to have major access site bleedings (13% vs 1%, p = 0.001). After 1 year, however they find that TRA maintains the same results in comparison to TFA (p = 0.41) [26]. In our study, we also find that there was no statistical significance for the long-term prognosis between TRA and TFA group (p = 0.69, Table 2), providing evidence that TRA is a useful alternative method to avoid vascular complications. Using a 7F system offers the availability of larger burr sizes, when it comes to plaque preparation, operators in our study found it adequate to use a maximum burr size of 1.75 mm, which can be accommodated in a 6F guide. And 6F guide, which were themselves usually used in transradial procedures. Larger guide catheter offers the more support for complex bifurcation [7, 27]. In our study, there was no difference in prognosis between the two catheter-size groups (p = 0.25, Table 2).
In previous studies, Lp(a) was found to be associated with CAC in patients with
or without familiar hypercholesterolemia [17, 28]. Pechlivanis et al.
[18] find that both log-transformed Lp(a) and categories of Lp(a) (Lp(a)
There are several limitations to this study. First, the rotation operation strategies were decided by the cardiovascular intervention specialist based on experience, which might induce selection bias compared with randomized controlled trials. Although we adjust the comparison between groups for possible confounders, the selection bias might still exist because of unknown confounders. Second, the sample size of our study was small. For Lp(a), large scale prospective randomized controlled trials are needed to determine the role of Lp(a) in the prognosis of patients who undergo RA. Finally, our results are tempered by the fact that all of the data we collected came from a single medical center.
In summary, we provide evidence that patients who undergo RA with a single burr may have better outcomes than patients who receive more than one burr. We find no significant association between the occurrence of MACE with the other issues of RA procedural indices including the size of burrs, approach site and guiding catheter size. Moreover, we find that baseline levels of Lp(a), LDL-C and hs-CRP have no significant predictive value for the prognosis of RA patients.
RA, rotational atherectomy; MACE, major adverse cardiac events; Lp(a), lipoprotein(a); LDL-C, low density lipoprotein cholesterol; hs-CRP, high sensitivity C-reactive protein; CHD, coronary heart disease; CAC, coronary artery calcification; PCI, percutaneous coronary intervention; ASCVD, atherosclerotic cardiovascular disease; SBP, systolic blood pressure; DBP, diastolic blood pressure; BMI, body mass index; TC, total cholesterol; TG, triglyceride; HDL-C, high-density lipoprotein cholesterol; MI, myocardial infarction; TLR, target lesion revascularization; CABG, coronary artery bypass graft; HRs, hazard ratios; TFA, transfemoral approach; TRA, transradial approach.
NQW designed the study; SZ and WJZ collected the medical records, followed up the patients and performed statistical analysis, and wrote this manuscript; HWS, ZFL, YGS participated in collecting the data and data management; JQ was the consultant of this study. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript.
All subjects gave their informed consent for inclusion before they participated in the study. The study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the Ethics Committee of Fuwai Hospital (Approval Number 2018-1086).
We would like to express our gratitude to all those who helped us during the writing of this manuscript. Thanks to all the peer reviewers for their opinions and suggestions.
This research received no external funding.
The authors declare no conflict of interest.