






 , Chunlin Chen 2,*
, Chunlin Chen 2,*1 Department of Midwifery, Faculty of Health, Dongguan Polytechnic, 523808 Dongguan, Guangdong, China
2 Department of Obstetrics and Gynecology, Nanfang Hospital, Southern Medical University, 510515 Guangzhou, Guangdong, China
3 Department of Obstetrics and Gynecology, Xijing Hospital of Airforce Medical University, 710032 Xi'an, Shanxi, China
4 Department of Gynecology, Fourth Hospital, Hebei Medical University, 050019 Shijiazhuang, Hebei, China
5 Department of Obstetrics and Gynecology, China-Japan Friendship Hospital, 100029 Beijing, China
6 Department of Gynecologic Oncology, Affiliated Cancer Hospital, Zhengzhou University, 450008 Zhengzhou, Henan, China
7 Department of Obstetrics and Gynecology, Shenzhen Maternal and Child Health Hospital, 518028 Shenzhen, Guangdong, China
8 Department of Obstetrics and Gynecology, Peking Union Medical College Hospital, 100193 Beijing, China
†These authors contributed equally.
Abstract
Background: To compare the oncological outcomes of Chinese patients
with International Federation of Gynecology and Obstetrics (FIGO) 2018 stage IIIC
cervical cancer (CC) receiving radical chemoradiotherapy (R-CT), abdominal
radical hysterectomy (ARH), or neoadjuvant chemotherapy and radical surgery
(NACT). Methods: Overall, 4086 patients in 47 hospitals from 2004 to
2018 were divided into groups according to stage (4029 with stage IIIC1 and 57
with stage IIIC2). Kaplan-Meier and Cox regression analyses were applied to
compare the 5-year overall survival (OS) and disease-free survival (DFS) of the
three initial treatments before and after propensity score matching (PSM).
Results: The 5-year DFS was worse in patients with stage IIIC2 than in
those with stage IIIC1 (post-PSM: 68.3% vs. 39.9%, p
Keywords
- FIGO 2018 IIIC
- cervical cancer
- radiotherapy
- prognosis
- abdominal radical hysterectomy
Cervical cancer (CC) represents a significant global health issue, with an estimated 570,000 cases and 311,000 deaths worldwide in 2018, ranking as the fourth most frequently diagnosed cancer and the fourth leading cause of cancer-related deaths in women [1]. Several studies have indicated lymph node metastasis (LNM) as a poor prognostic factor for CC [2, 3, 4, 5, 6, 7, 8, 9]. Tumor staging is high-ranking for overall management and guidance of treatment [10]. The International Federation of Gynecology and Obstetrics (FIGO) staging system [11] is relatively well-recognized for CC and includes a prominent revision to classify patients with LNM as stage IIIC. Patients with pelvic LNM are classified as stage IIIC1, whereas those with para-aortic LNM are classified as stage IIIC2. This classification emphasizes the significance of LNM and its location for prognosis and treatment.
Abdominal radical hysterectomy (ARH) and radical chemoradiotherapy (R-CT) are the primary initial treatments for CC. R-CT improves mortality in CC by approximately 30–50% [12, 13, 14, 15, 16] and can be used in all stages of CC; however, it is associated with a range of concomitant complications [17, 18, 19]. In contrast, ARH allows for the resection of tumor tissues and metastatic lymph nodes (LNs) to reduce tumor burden and determine LN status, which can guide postoperative adjuvant therapy. In recent years, neoadjuvant chemotherapy and radical surgery (NACT) have also been used to treat CC because of their positive effect in reducing tumor volume and lowering tumor stage. In the FIGO 2018 staging system [11], stage IIIC CC includes cases of FIGO 2009 stages IA to III CC with LNM. Prior to 2018, the standard initial treatments for FIGO 2009 stages IA to IIA and stages IIB to III CC were ARH and R-CT, respectively. Nevertheless, both the FIGO 2018 [11] and 2023 National Comprehensive Cancer Network (NCCN) [20] guidelines recommend R-CT for stage IIIC CC only, leading to the loss of opportunity for surgery in some patients with FIGO 2009 early-stage CC, which represents a significant departure from past treatment strategies. As a result, the treatment of stage IIIC CC remains controversial.
Overall, less developed regions account for 85% of the incidence and 90% of the mortality of CC [21]. In light of the World Health Organization (WHO) country profile for CC [22], Canada has 11 radiotherapy units per 10,000 cancer patients, whereas China has 4 and Uganda 1, highlighting the lack of radiotherapy resources in such less developed regions. Therefore, options to initial treatment for FIGO 2018 stage IIIC CC is particularly critical in less developed regions with both a high CC prevalence and a lack of radiotherapy resources. Nevertheless, most studies on stage IIIC CC have largely focused on the prognostic and influencing factors, validating their plausibility and causes, whereas fewer studies have focused on treatment strategies, and studies from less developed regions are also lacking. Consequently, this study addresses the treatment strategy for FIGO 2018 Stage IIIC CC in developing countries to provide evidence for the selection of alternative initial treatment options for less developed regions.
For this retrospective study, the data used were obtained from the Project 1538 developed through a clinical trial (Project 1538; Ethics Clearance NFEC-2017-135; Clinical trial registration number: CHiCTR1800017778, http://apps.who.int/trialsearch/), which was authorized by the Ethics Committee of Southern Hospital. The database includes 63,926 cases of CC, collected across 47 hospitals in China. Included are patients’ clinical information, pretreatment biopsy results, laboratory and imaging information, treatment plans, treatment complications, and postoperative pathology reports. Data were collected by two gynecologists, who received specific training for the clinical trial, using EpiData 3.1 (EpiData Association, Odense, Denmark) for dual data entry and standard interviews for follow-up data by telephone calls or outpatient visits. Details of the data collection and follow-up methods have been previously described [23, 24].
For our study, the selection criteria for eligible cases were as follows: age
The outcomes for this study were overall survival (OS) and disease-free survival (DFS), with a cutoff point of 5 years post-treatment. OS is the last point in time from diagnosis to valid follow-up or death for any reason. DFS is the last point in time from diagnosis to follow-up, relapse, or death.
Continuous variables were described as the mean
Based on the inclusion and exclusion criteria, 4086 CC cases were selected from the Project 1538 database, with no missing values. Fig. 1 exemplifies the patient screening process. The findings from baseline profiling for stages IIIC1 and IIIC2 are presented in Supplementary Table 1. The findings from baseline profiling for the R-CT and ARH groups, R-CT and NACT groups, and ARH and NACT groups for stage IIIC1 are described in Supplementary Tables 2,3,4, respectively. The findings from baseline profiling for the ARH and NACT groups for stage IIIC2 are depicted in Supplementary Table 5.
 Fig. 1.
Fig. 1.Patient selection flow diagram. Based on the inclusion and exclusion criteria, 4019 stage IIIC1 cases (R-CT, n = 1913; ARH, n = 1493; and NACT, n = 623) and 57 stage IIIC cases (ARH, n = 36; and NACT, n = 21) were screened from the Chinese 1538 project database. FIGO, international federation of gynecology and obstetrics; R-CT, radical chemoradiotherapy; ARH, abdominal radical hysterectomy; NACT, neoadjuvant chemotherapy and radical surgery.
Kaplan-Meier analysis revealed a marked distinction in 5-year DFS between stages
IIIC1 and IIIC2 (73.8% vs. 70.2%, p = 0.638) but not in OS
(65.6% vs. 38.5%, p
 Fig. 2.
Fig. 2.OS and DFS of stages IIIC1 and IIIC2. Direct comparison of 5-year OS (A) and 5-year DFS (B) for stage IIIC1 and IIIC2. Comparison of 5-year OS (C) and 5-year DFS (D) for stage IIIC1 and IIIC2 after PSM. PSM, propensity score matching; OS, overall survival; DFS, disease-free survival.
Cox regression analyses (post-PSM) showed that stage IIIC2 was correlated with
worse DFS (HR = 2.295, 95% CI 1.470–3.581, p
| Variables | 5-year OS (pre-PSM) | 5-year DFS (pre-PSM) | 5-year OS (post-PSM) | 5-year DFS (post-PSM) | |||||||||
| HR | 95% CI | p | HR | 95% CI | p | HR | 95% CI | p | HR | 95% CI | p | ||
| Age (years) | 1.008 | 1.000–1.015 | 0.040 | 1.001 | 0.995–1.007 | 0.772 | 1.007 | 0.979–1.036 | 0.631 | 0.998 | 0.997–1.019 | 0.826 | |
| Histological type | 0.016 | 0.005 | |||||||||||
| SCC | 1 (Ref) | - | - | 1 (Ref) | - | - | 1 (Ref) | - | - | 1 (Ref) | - | - | |
| AC | 1.689 | 1.287–2.216 | 1.585 | 1.264–1.986 | 2.517 | 1.332–4.759 | 0.004 | 2.337 | 1.399–3.905 | 0.001 | |||
| ASC | 2.231 | 1.534–3.245 | 1.592 | 1.129–2.245 | 0.008 | 1.939 | 0.264–14.268 | 0.516 | 0.763 | 0.105–5.525 | 0.789 | ||
| FIGO stage | |||||||||||||
| Stage IIIC1 | 1 (Ref) | - | - | 1 (Ref) | - | - | 1 (Ref) | - | - | 1 (Ref) | - | - | |
| Stage IIIC2 | 1.518 | 1.13–2.035 | 0.005 | 2.112 | 1.436–3.108 | 1.142 | 0.558–2.337 | 0.716 | 2.295 | 1.470–3.581 | |||
| Initial treatment modality | 0.020 | 0.017 | |||||||||||
| R-CT | 1 (Ref) | - | - | 1 (Ref) | - | - | 1 (Ref) | - | - | 1 (Ref) | - | - | |
| ARH | 0.647 | 0.599–0.700 | 0.681 | 0.591–0.785 | 0.424 | 0.165–1.093 | 0.076 | 0.657 | 0.262–1.648 | 0.371 | |||
| NACT | 0.730 | 0.657–0.812 | 1.173 | 0.995–1.383 | 0.057 | 0.789 | 0.301–2.069 | 0.630 | 1.115 | 0.441–2.822 | 0.817 | ||
PSM, propensity score matching; OS, overall survival; DFS, disease-free survival; CI, confidence interval; HR, hazard ratio; SCC, squamous cell carcinoma; AC, Adenocarcinoma ASC, adenosquamous cell carcinoma; FIGO, international federation of gynecology and obstetrics; R-CT, radical chemoradiotherapy; ARH, abdominal radical hysterectomy; NACT, neoadjuvant chemotherapy and radical surgery.
Kaplan–Meier analysis revealed notable variations in 5-year OS (pre-PSM: 68.9%
vs. 79.6%, p
 Fig. 3.
Fig. 3.OS and DFS of the R-CT and ARH groups (stage IIIC1). Direct comparison of 5-year OS (A) and 5-year DFS (B) for R-CT and ARH in stage IIIC1. Comparison of 5-year OS (C) and 5-year DFS (D) for R-CT and ARH in stage IIIC1 after PSM. PSM, propensity score matching; OS, overall survival; DFS, disease-free survival; R-CT, radical chemoradiotherapy; ARH, abdominal radical hysterectomy.
 Fig. 4.
Fig. 4.OS and DFS of the R-CT and NACT groups (stage IIIC1). Direct comparison of 5-year OS (A) and 5-year DFS (B) for R-CT and NACT in stage IIIC1. Comparison of 5-year OS (C) and 5-year DFS (D) for R-CT and NACT in stage IIIC1 after PSM. PSM, propensity score matching; OS, overall survival; DFS, disease-free survival; R-CT, radical chemoradiotherapy; NACT, neoadjuvant chemotherapy and radical surgery.
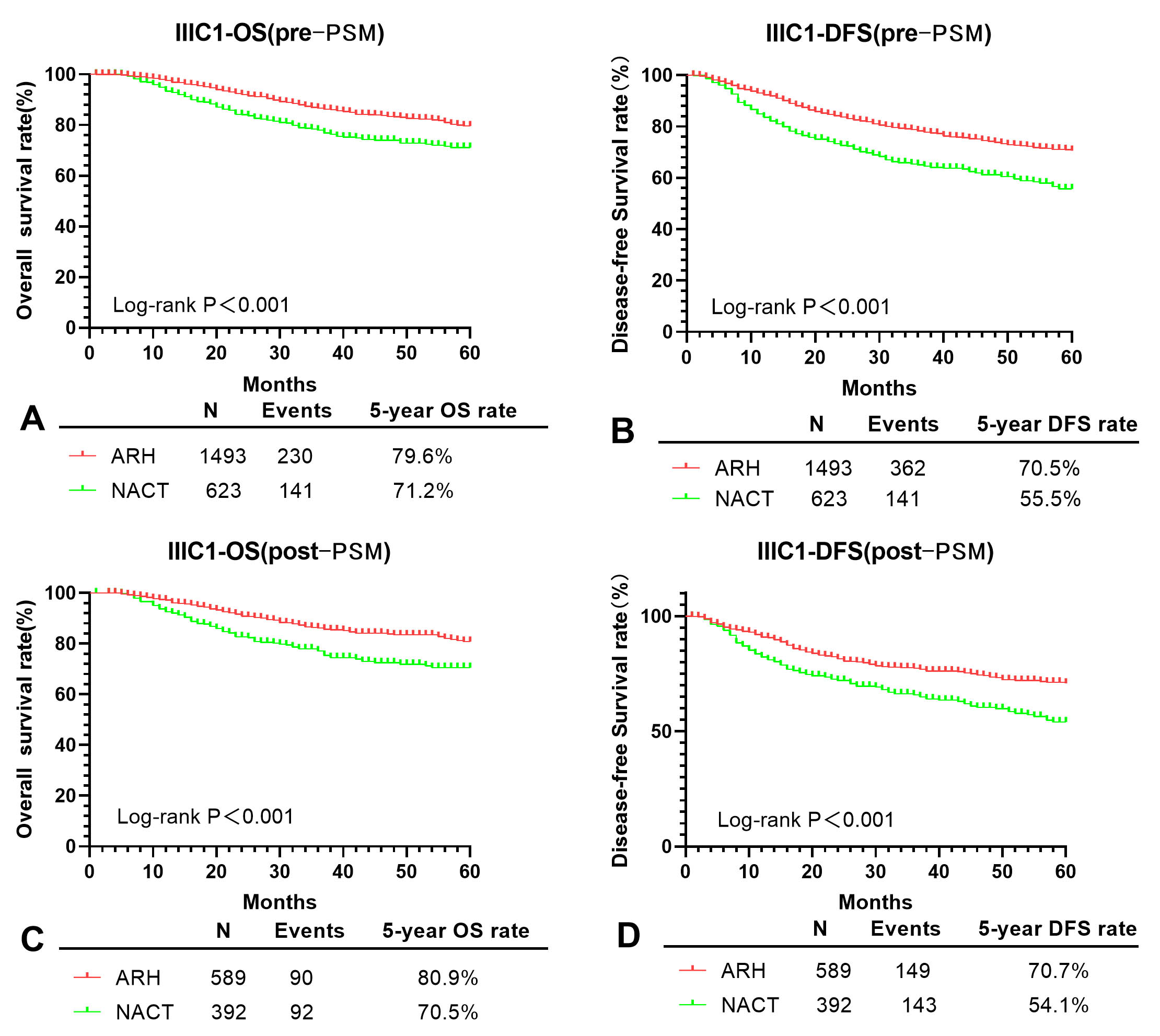 Fig. 5.
Fig. 5.OS and DFS of the ARH and NACT groups (stage IIIC1). Direct comparison of 5-year OS (A) and 5-year DFS (B) for ARH and NACT in stage IIIC1. Comparison of 5-year OS (C) and 5-year DFS (D) for ARH and NACT in stage IIIC1 after PSM. PSM, propensity score matching; OS, overall survival; DFS, disease-free survival; ARH, abdominal radical hysterectomy; NACT, neoadjuvant chemotherapy and radical surgery.
Cox regression analyses (post-PSM) showed that the ARH group was correlated with
better 5-year OS (HR = 0.603, 95% CI 0.493–0.738, p
| 5-year OS (pre-PSM) | 5-year DFS (pre-PSM) | 5-year OS (post-PSM) | 5-year DFS (post-PSM) | ||||||||||
| HR | 95% CI | p | HR | 95% CI | p | HR | 95% CI | p | HR | 95% CI | p | ||
| R-CT and ARH groups | |||||||||||||
| Age (years) | 1.006 | 0.998–1.014 | 0.116 | 1.001 | 0.994–1.008 | 0.774 | 1.007 | 0.996–1.018 | 0.230 | 0.999 | 0.990–1.008 | 0.788 | |
| Histological type | |||||||||||||
| SCC | 1 (Ref) | - | - | 1 (Ref) | - | - | 1 (Ref) | - | - | 1 (Ref) | - | - | |
| AC | 1.835 | 1.336–2.521 | 1.645 | 1.250–2.165 | 2.514 | 1.683–3.756 | 1.969 | 1.352–2.867 | |||||
| ASC | 2.141 | 1.350–3.394 | 0.001 | 1.657 | 1.092–2.515 | 0.018 | 2.884 | 1.657–5.021 | 2.367 | 1.439–3.894 | |||
| Initial treatment modality | |||||||||||||
| R-CT | 1 (Ref) | - | - | 1 (Ref) | - | - | 1 (Ref) | - | - | 1 (Ref) | - | - | |
| ARH | 0.552 | 0.464–0.658 | 0.684 | 0.592–0.791 | 0.603 | 0.493–0.738 | 0.727 | 0.616–0.857 | 0.001 | ||||
| R-CT and NACT groups | |||||||||||||
| Age (years) | 1.007 | 0.998–1.015 | 0.116 | 1.000 | 0.993–1.008 | 0.919 | 1.002 | 0.988–1.017 | 0.748 | 0.994 | 0.982–1.006 | 0.335 | |
| Histological type | |||||||||||||
| SCC | 1 (Ref) | - | - | 1 (Ref) | - | - | 1 (Ref) | - | - | 1 (Ref) | - | - | |
| AC | 1.685 | 1.166–2.437 | 0.005 | 1.639 | 1.201–2.235 | 0.002 | 1.767 | 1.107–2.820 | 0.017 | 2.071 | 1.419–3.022 | ||
| ASC | 2.823 | 1.777–4.486 | 2.040 | 1.316–3.160 | 0.001 | 3.596 | 2.060–6.278 | 2.675 | 1.569–4.559 | ||||
| Initial treatment modality | |||||||||||||
| R-CT | 1 (Ref) | - | - | 1 (Ref) | - | - | 1 (Ref) | - | - | 1 (Ref) | - | - | |
| NACT | 0.940 | 0.761–1.160 | 0.564 | 1.157 | 0.974–1.373 | 0.096 | 1.065 | 0.850–1.335 | 0.586 | 1.308 | 1.088–1.573 | 0.004 | |
| ARH and NACT groups | |||||||||||||
| Age (years) | 1.010 | 0.998–1.021 | 0.090 | 1.002 | 0.993–1.011 | 0.628 | 1.014 | 0.996–1.033 | 0.136 | 1.000 | 0.986–1.015 | 0.998 | |
| Histological type | 0.004 | 0.056 | 0.330 | 0.465 | |||||||||
| SCC | 1 (Ref) | - | - | 1 (Ref) | - | - | 1 (Ref) | - | - | 1 (Ref) | - | - | |
| AC | 1.527 | 1.084–2.152 | 0.016 | 1.342 | 1.016–1.772 | 0.038 | 1.199 | 0.649–2.214 | 0.563 | 1.272 | 0.803–2.012 | 0.305 | |
| ASC | 1.825 | 1.131–2.945 | 0.014 | 1.342 | 0.874–2.062 | 0.179 | 1.905 | 0.768–4.724 | 0.164 | 1.359 | 0.598–3.085 | 0.464 | |
| Initial treatment modality | |||||||||||||
| ARH | 1 (Ref) | - | - | 1 (Ref) | - | - | 1 (Ref) | - | - | 1 (Ref) | - | - | |
| NACT | 1.709 | 1.366–2.137 | 1.687 | 1.412–2.016 | 1.750 | 1.306–2.345 | 1.653 | 1.312–2.083 | |||||
| Hysterectomy type | 0.821 | 0.527 | 0.785 | 0.760 | |||||||||
| Type QM-B | 1 (Ref) | - | - | 1 (Ref) | - | - | 1 (Ref) | - | - | 1 (Ref) | - | - | |
| Type QM-C1 | 0.000 | 0–2.405 |
0.927 | 0.392 | 0.055–2.799 | 0.351 | 0.00 | 0–2.112 |
0.946 | 0.00 | 0–1.001 |
0.930 | |
| Type QM-C2 | 1.074 | 0.858–1.344 | 0.534 | 1.057 | 0.885–1.264 | 0.539 | 1.121 | 0.812–1.546 | 0.488 | 1.100 | 0.853–1.420 | 0.462 | |
| Tumor diameter (cm) | 0.252 | 0.057 | 0.101 | 0.112 | |||||||||
| 1 (Ref) | - | - | 1 (Ref) | - | - | 1 (Ref) | - | - | 1 (Ref) | - | - | ||
| 1.160 | 0.929–1.448 | 0.190 | 1.132 | 0.948–1.352 | 0.172 | 1.354 | 0.992–1.849 | 0.056 | 1.232 | 0.965–1.574 | 0.094 | ||
| Unknown | 1.333 | 0.875–2.031 | 0.180 | 1.456 | 1.052–2.014 | 0.023 | 1.584 | 0.839–2.985 | 0.156 | 1.518 | 0.914–2.521 | 0.107 | |
| LVSI | |||||||||||||
| Negative | 1 (Ref) | - | - | 1 (Ref) | - | - | 1 (Ref) | - | - | 1 (Ref) | - | - | |
| Positive | 1.339 | 1.085–1.653 | 0.007 | 1.070 | 0.903–1.268 | 0.436 | 1.164 | 0.858–1.579 | 0.330 | 1.016 | 0.796–1.296 | 0.902 | |
| Cervical stromal invasion | 0.001 | 0.490 | 0.521 | ||||||||||
| 1 (Ref) | - | - | 1 (Ref) | - | - | 1 (Ref) | - | - | 1 (Ref) | - | - | ||
| 1.976 | 1.368–2.854 | 1.892 | 1.427–2.508 | 1.313 | 0.797–2.162 | 0.285 | 1.202 | 0.828–1.747 | 0.333 | ||||
| Unknown | 1.632 | 0.881–3.023 | 0.120 | 1.543 | 0.953–2.497 | 0.078 | 1.624 | 0.597–4.418 | 0.342 | 1.463 | 0.669–3.198 | 0.341 | |
| Parametrial involvement | |||||||||||||
| Negative | 1 (Ref) | - | - | 1 (Ref) | - | - | 1 (Ref) | - | - | 1 (Ref) | - | - | |
| Positive | 1.615 | 1.107–2.356 | 0.013 | 1.893 | 1.426–2.513 | 1.646 | 0.801–3.384 | 0.175 | 1.615 | 0.901–2.894 | 0.107 | ||
| Vaginal margin | |||||||||||||
| Negative | 1 (Ref) | - | - | 1 (Ref) | - | - | 1 (Ref) | - | - | 1 (Ref) | - | - | |
| Positive | 0.732 | 0.389–1.379 | 0.335 | 1.283 | 0.867–1.899 | 0.213 | 0.234 | 0.032–1.708 | 0.152 | 0.825 | 0.353–1.925 | 0.656 | |
PSM, propensity score matching; OS, overall survival; DFS, disease-free survival; CI, confidence interval; HR, hazard ratio; SCC, squamous cell carcinoma; AC, Adenocarcinoma ASC, adenosquamous cell carcinoma; R-CT, radical chemoradiotherapy; ARH, abdominal radical hysterectomy; NACT, neoadjuvant chemotherapy and radical surgery; LVSI, lymphovascular space invasion.
PSM could not be performed because of the small number of cases in both groups. Kaplan-Meier analysis revealed a marked distinction in 5-year DFS (45.4% vs. 30.1%, p = 0.025) but not in 5-year OS (69.7% vs. 73.9%, p = 0.750) between the ARH and NACT groups (Fig. 6).
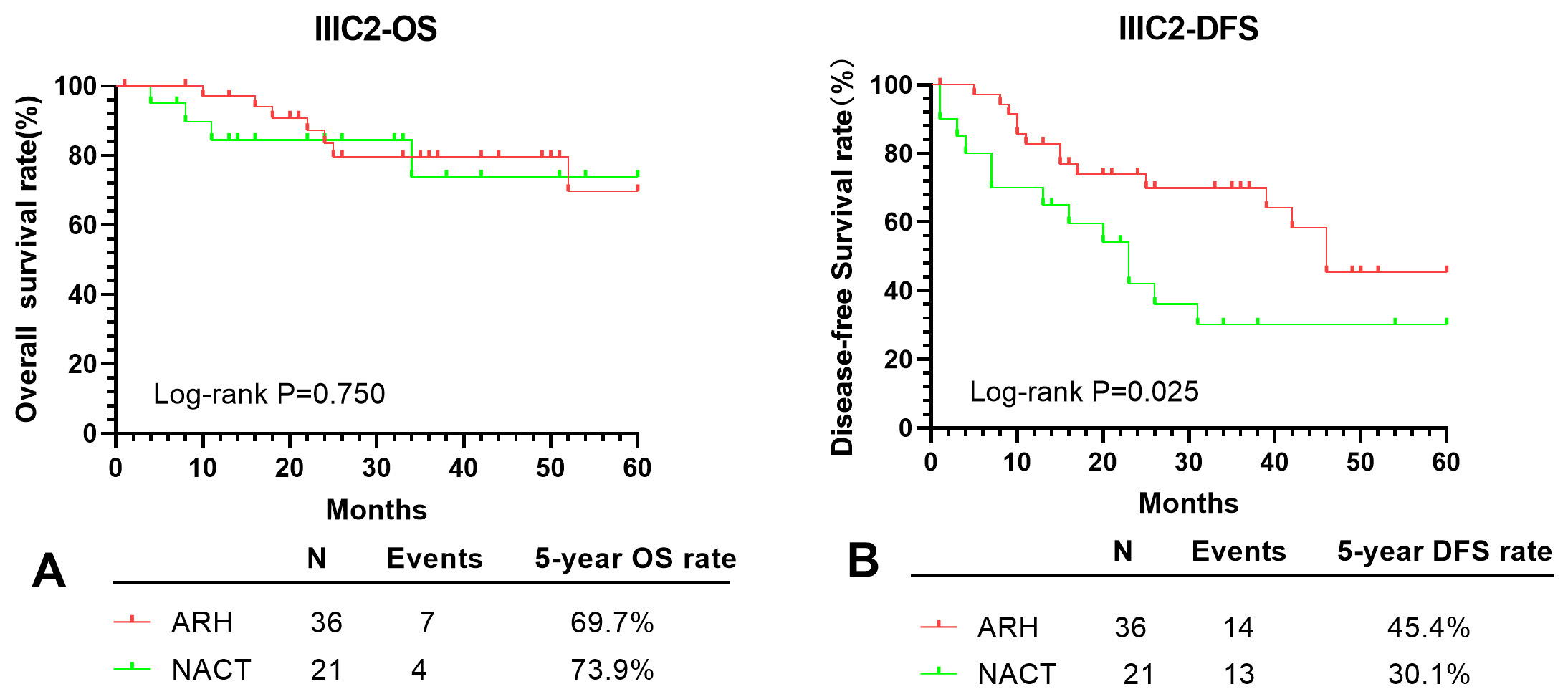 Fig. 6.
Fig. 6.OS and DFS of the ARH and NACT groups (stage IIIC2). Direct comparison of 5-year OS (A) and 5-year DFS (B) for ARH and NACT in stage IIIC2. OS, overall survival; DFS, disease-free survival; ARH, abdominal radical hysterectomy; NACT, neoadjuvant chemotherapy and radical surgery.
Cox regression analyses (pre-PSM) showed that the NACT group was related to
worse 5-year DFS (HR = 2.526, 95% CI 1.012–6.301, p = 0.047) but not
to worse 5-year OS (p = 0.825) versus the ARH group. Age was also
correlated with worse 5-year DFS (p = 0.040) but not with 5-year OS
(p = 0.868). Compared with SCC, AC was correlated with worse 5-year DFS
(p = 0.001) but not with worse 5-year OS (p = 0.075), whereas
ASC was not correlated with either 5-year OS or DFS (p
| Variables | 5-year OS | 5-year DFS | |||||
| HR | 95% CI | p | HR | 95% CI | p | ||
| Age (years) | 0.993 | 0.909–1.084 | 0.868 | 0.944 | 0.894–0.997 | 0.040 | |
| Histological type | 0.126 | 0.004 | |||||
| SCC | 1 (Ref) | - | - | 1 (Ref) | - | - | |
| AC | 7.447 | 0.815–68.093 | 0.075 | 11.118 | 2.639–46.832 | 0.001 | |
| ASC | 3.073 | 0.293–32.184 | 0.349 | 0.884 | 0.108–7.240 | 0.908 | |
| Initial treatment modality | |||||||
| ARH | 1 (Ref) | - | - | 1 (Ref) | - | - | |
| NACT | 1.194 | 0.248–5.747 | 0.825 | 2.526 | 1.012–6.301 | 0.047 | |
| Hysterectomy type | 0.820 | 0.176 | |||||
| Type QM-B | 1 (Ref) | - | - | 1 (Ref) | - | - | |
| Type QM-C1 | 0.000 | 0.000 | 0.990 | 1.266 | 0.129–12.424 | 0.839 | |
| Type QM-C2 | 0.559 | 0.092–3.406 | 0.528 | 0.338 | 0.106–1.084 | 0.068 | |
| Tumor diameter (cm) | 0.933 | 0.516 | |||||
| 1 (Ref) | - | - | 1 (Ref) | - | - | ||
| 1.254 | 0.268–5.864 | 0.773 | 1.515 | 0.545–4.209 | 0.426 | ||
| Unknown | 0.836 | 0.050–13.968 | 0.901 | 0.631 | 0.110–3.604 | 0.604 | |
| LVSI | |||||||
| Negative | 1 (Ref) | - | - | 1 (Ref) | - | - | |
| Positive | 0.977 | 0.210–4.548 | 0.976 | 0.730 | 0.265–2.009 | 0.543 | |
| Cervical stromal invasion | 0.803 | 1.000 | |||||
| 1 (Ref) | - | - | 1 (Ref) | - | - | ||
| 1.439 | 0.082–25.145 | 0.803 | 1.009 | 0.209–4.870 | 0.991 | ||
| Unknown | - | - | - | 0.00 | 0.000 | 0.984 | |
| Parametrial involvement | |||||||
| Negative | 1 (Ref) | - | - | 1 (Ref) | - | - | |
| Positive | 0.369 | 0.046–2.953 | 0.347 | 0.489 | 0.134–1.785 | 0.279 | |
| Vaginal margin | |||||||
| Negative | 1 (Ref) | - | - | 1 (Ref) | - | - | |
| Positive | 4.361 | 0.569–33.428 | 0.156 | 2.413 | 0.568–10.261 | 0.233 | |
OS, overall survival; DFS, disease-free survival; CI, confidence interval; HR, hazard ratio; ARH, abdominal radical hysterectomy; NACT, neoadjuvant chemotherapy and radical surgery; SCC, squamous cell carcinoma; AC, Adenocarcinoma; ASC, adenosquamous cell carcinoma; LVSI, lymphovascular space invasion.
The FIGO 2018 IIIC staging system highlights the relevance of LNM in oncology treatment and prognosis. For patients at this stage, the 2018 FIGO [11] and the 2023 NCCN [20] guidelines recommend only R-CT with no alternative treatment options described. However, performing R-CT is often a challenge for underdeveloped areas where radiotherapy facilities are lacking. Consequently, this study focused on FIGO 2018 stage IIIC CC patients to investigate the oncological outcomes of R-CT, ARH, and NACT and to provide a real-world basis for selecting an appropriate alternative initial treatment in less developed areas. We found that different stages and treatments affected the prognosis of stage IIIC CC patients, with higher mortality and risk of recurrence for stage IIIC2 than for stage IIIC1. In addition, for patients with stage IIIC1, ARH showed better oncological outcomes than R-CT and NACT. In contrast, for patients with stage IIIC2, ARH was superior to NACT, but R-CT data were insufficient to conclude whether it was appropriate in the current study. As such, ARH may thus represent a viable alternative treatment option.
Substantial evidence supports para-aortic LNM as a clear adverse prognostic
factor [5, 18, 19, 25, 26, 27, 28, 29]. Cho et al. [25] analyzed stage IIIC CC
patients and observed that patients with para-aortic LNM exhibited noticeably
worse 5-year OS and DFS than those without para-aortic LNM (p
Although R-CT is used in patients with all stages of CC to improve the
oncological outcomes, it may also damage nearby organs and cause adverse effects
[17, 18, 19]. Contrastingly, ARH offers several advantages, including avoidance of
the adverse effects of R-CT; removal of the primary tumor, infiltrating tissues,
and LN; and the possibility of personalized postoperative treatment based on
pathological findings. As such, ARH is the preferred treatment option for early
CC [10]. However, it was demonstrated by Wu et al. [30] and Landoni
et al. [31] that the therapeutic efficacies of ARH and R-CT are similar.
Furthermore, investigations by Yan et al. [32] and Jang et al.
[33] indicated that the prognosis after ARH was significantly better than that
after R-CT, which is in keeping with the outcomes of the present research. In the
present study, compared with the R-CT group, the ARH group had superior 5-year OS
(post-PSM: 71.0% vs. 80.0%, p
Interestingly, NACT positively lowers tumor stage, reduces tumor burden, and
enhances the chance of surgical tumor removal; however, conclusive evidence on
whether NACT has a positive effect on the prognosis of CC is still lacking
[36, 37, 38, 39]. A meta-analysis by Ye et al. [40] revealed that oncological
outcomes were significantly superior in the NACT group compared with those in the
direct surgery group (p
Duenas-Gonzalez et al. [44] also observed that, compared with R-CT,
NACT did not have an improved prognosis for CC. Similar findings were showed in
this research, where for stage IIIC1, R-CT had a better 5-year DFS than NACT, and
NACT was also correlated with a worse 5-year DFS (post-PSM: p
This current study is notable, as it is one of the largest studies based on the 2018 FIGO staging system for stage IIIC1 and IIIC2 CC from less developed regions. This study is innovative, as it stratified patients based on different LNM locations and compared the oncological prognosis of three commonly used CC treatments. In spite of the wide-ranging application of minimally invasive approaches, abdominal hysterectomy remains a general surgical procedure of intervention [46]. Furthermore, the Laparoscopic Approach to Cervical Cancer (LACC) confirmed that the prognosis of minimally invasive surgery was worse than that of ARH [47]. Therefore, only patients treated with ARH were included in this study. Nevertheless, this study has a few limitations. First, being retrospective, this study may have involved data imbalance between groups. Second, the lack of information on the specific treatment regimen, dose and duration of postoperative adjuvant therapy, R-CT, and NACT was also a shortcoming of the current study. Third, only 57 stage IIIC2 cases and no R-CT cases were available, which may have affected the reliability of the results. Fourth, stratification was performed based on only two LNM locations and did not include LN size and number and other LNM locations.
In the present study, the oncological prognosis of patients with stage IIIC1 CC was generally better than that of patients with stage IIIC2, indicating that the rationale behind the classification of stage IIIC is justified. The oncological outcome of ARH was superior to those of R-CT and NACT for stage IIIC1 and superior to that of NACT for stage IIIC2. As such, ARH is an acceptable initial treatment option for patients with stage IIIC in less developed areas; however, consideration should be given to the use of NACT. Given the small number of stage IIIC2 cases analyzed, confirmation of the results of this research is warranted in future prospective studies.
The data generated in the present study are not publicly available due to privacy, ethical restrictions and relevance to unpublished research, but may be requested from the corresponding author.
All authors approved the final version of the study. YY, ZL, SK and BC made equal contributions to this work. YY conceived, structured and mentored the study, translated the data, and created and revamped the manuscript. ZL undertook the search of literature, gathered data, performed data analysis and explanation, and wrote and corrected the manuscript. SK framed and conceived the study, construed the data, and produced and modified the manuscript. BC has performed the literature search, the analysis and interpretation of data and graphs, and prepared and reviewed the manuscript. BL and LW gathered data, performed data analysis and explanation, and contributed resources. JY gathered data and contributed with resources and software. JL conceptualized the study. PL and CC conceptualized, devised and mentored the study. All authors contributed to editorial changes in the manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
This study was carried out in accordance with the ethical principles of the Declaration of Helsinki 1964. Permission for this retrospective study was obtained from the Ethics Committee of the Nanfang Hospital of Southern Medical University (approval number NFEC-2017-135 and clinical trial number CHiCTR1800017778; International Clinical Trials Registry Platform Search Port, https://trialsearch.who.int/Trial2.aspx?TrialID=ChiCTR1800017778, registered at 14/08/2018), in which they concluded that written informed consent was not necessitated owing to the retrospective nature of the study and the withholding of patient information.
We would like to thank Min Hao (The Second Hospital of Shanxi Medical University), Lixin Sun and Hongwei Zhao (Shanxi Cancer Hospital), Jihong Liu and Lizhi Liang (Sun Yat-sen University Cancer Center), Lihong Lin and Yu Guo (Anyang Tumor Hospital), Weidong Zhao (Anhui Provincial Cancer Hospital), Yan Ni (The Yuncheng Central Hospital of Shanxi Province), Wentong Liang and Donglin Li (Guizhou Provincial People’s Hospital), Xuemei Zhan and Mingwei Li (Jiangmen Central Hospital), Weifeng Zhang (Ningbo Women & Children’s Hospital), Peiyan Du (The Affiliated Cancer Hospital and Institute of Guangzhou Medical University), Ziyu Fang (Liuzhou Workers’ Hospital), Rui Yang (Shenzhen Hospital of Peking University), Long Chen (Qingdao Municipal Hospital), Encheng Dai and Ruilei Liu (Linyi People’s Hospital), Yuanli He and Mubiao Liu (Zhujiang Hospital, Southern Medical University), Zhihua Liu (Shenzhen Maternity & Child Health Hospital), Xueqin Wang (The Fifth Affiliated Hospital of Southern Medical University), Anwei Lu (Maternal and Child Health Hospital of Guiyang Province), Shuangling Jin (Peace Hospital affiliated to Changzhi Medical College), Ben Ma (Guangzhou First People’s Hospital), Zhonghai Wang (Shenzhen Nanshan People’s Hospital), Lin Zhu (The Second Hospital of Shandong University), Hongxin Pan (The Third Affiliated Hospital of Shenzhen University), Qianyong Zhu (No. 153. Center Hospital of the Liberation Army/Hospital No. 988 of the Chinese People’s Liberation Army Joint Support Force), Dingyuan Zeng and Zhong Lin (Maternal and Child Health Care Hospital of Liuzhou), Xiaohong Wang (Laiwu People’s Hospital/Jinan City People’s Hospital), and Bin Zhu (The Affiliated Yiwu Women and Children Hospital of Hangzhou Medical College) for their contributions to data collection.
This study was funded by grants from the National Science and Technology Support Program of China (Grant No.2014BAI05B03), National Natural Science Fund of Guangdong (Grant No. 2015A030311024), Dongguan Sci-tech Commissoner Program (Grant No. 20221800500661), Guangdong Higher Vocational Education Teaching Reform Research and Practice Project (Grant No. GDJG 2021008), and Science and Technology Plan of Guangzhou (Grant No. 158100075).
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.