

 , Junyi Ren 1, Chen Chen 2, Xiaolan Zhao 2,*
, Junyi Ren 1, Chen Chen 2, Xiaolan Zhao 2,*
1 School of Medicine, University of Electronic Science and Technology of China, 610054 Chengdu, Sichuan, China
2 Department of Gynaecology and Obstetrics, Sichuan Provincial People’s Hospital, University of Electronic Science and Technology of China, 610072 Chengdu, Sichuan, China
Abstract
Primary immune thrombocytopenia (ITP) during pregnancy is an acquired autoimmune disorder characterized by a decreased platelet count (<100 × 109/L) due to the presence of platelet-specific autoantibodies. Although ITP is rare, with an incidence of just 1–10 cases per 10,000 pregnancies, it poses significant risks of maternal hemorrhage and neonatal thrombocytopenia. Management options include first-line treatments such as corticosteroids and intravenous immunoglobulin (IVIG), while second-line therapies (high-dose steroids, or splenectomy) are reserved for refractory cases. Treatment is aimed at maintaining safe platelet thresholds (>30 × 109/L during pregnancy and >50 × 109/L for delivery) rather than achieving normal levels, thereby balancing maternal safety with fetal considerations. Multidisciplinary management involving hematologists, obstetricians, and neonatologists is essential for optimal outcomes.
6 primiparous women with severe ITP in late pregnancy (platelet count <20 × 109/L) were treated with a comprehensive regimen including prednisone, recombinant human thrombopoietin, IVIG, and platelet transfusions, resulting in increased platelet counts (range of 48 to 294 × 109/L). All 6 cases exhibited platelet counts <20 × 109/L, gestational ages ranging from 32 to 34+ weeks, and were hospitalized for induction of labor.
Individualized comprehensive treatment can effectively manage severe ITP during late pregnancy, with protocols tailored to each patient’s condition, gestational age, and platelet count fluctuations.
Keywords
- thrombocytopenia during pregnancy
- corticosteroids
- intravenous immunoglobulin
- recombinant human thrombopoietin
- platelet transfusions
- individualized treatment
Primary immune thrombocytopenia (ITP) during pregnancy is an acquired autoimmune
disorder characterized by reduced platelet count and increased risk of bleeding,
with an incidence of approximately 1–10 per 10,000 pregnant women [1]. Pregnancy
may exacerbate pre-existing ITP, or trigger its first manifestation in previously
undiagnosed cases [2]. ITP during pregnancy not only increases the maternal
hemorrhage risk, particularly during delivery, but may also cause neonatal
thrombocytopenia through the placental transfer of autoantibodies [3]. The
pathophysiology of ITP during pregnancy largely mirrors that of non-pregnant
cases, involving primarily the autoantibody-mediated destruction of platelets,
and decreased platelet production [4]. Pregnancy can influence the course of ITP
through immunomodulatory mechanisms, leading to deterioration in some patients,
whereas others may experience improvement [5]. Management of ITP during pregnancy
follows a stepwise approach. First-line treatments such as corticosteroids
(prednisolone) and intravenous immunoglobulin (IVIG) are considered relatively
safe during pregnancy. Second-line options for refractory cases include
higher-dose corticosteroids and repeated IVIG administration. In some cases,
splenectomy is also performed, but this is typically avoided during pregnancy
except in emergencies. Thrombopoietin receptor agonists (TPO-RAs) and rituximab
are generally not recommended during pregnancy due to limited safety data.
Treatment decisions must balance maternal safety with fetal risk considerations,
and therapeutic targets are therefore often set to achieve safe rather than
normal platelet counts (i.e.,
This study included 6 primiparas aged 24–33 years and admitted to our hospital
after 32 weeks of gestation. All were admitted due to low platelet counts found
during prenatal examinations. Some patients had a previous diagnosis of
thrombocytopenia. One patient presented with symptoms of skin ecchymosis and
epistaxis. The range of platelet counts for these patients at admission was 3–17
Prednisone is used to increase the platelet count. It is taken orally, with a dose range of 15–50 mg/d, and is produced by Shandong Lukang. The batch number is (2112282), and origin is (Jining, Shandong, China).
Recombinant human thrombopoietin (rhTPO) is administered by subcutaneous injection at a dose of 15,000 U/d. It is produced by Shengyang Sansheng, with batch number (2005004) and origin (Shenyang, Liaoning, China).
Intravenous human immunoglobulin was used at a dose of 22.5 g/d. It is produced by Chengdu Rongsheng, with batch number (2122304) and origin (Chengdu, Sichuan, China).
Oxytocin is used to prevent uterine atony during cesarean section. It is administered intravenously to promote uterine contractions and is produced by Shanghai, Hefeng, with batch number (1230305) and place of origin (Shanghai, China).
Kabei oxytocin is used in combination with oxytocin to promote uterine contractions during cesarean section. It is produced by Hainan Huanglong, with batch number (2033887) and the place of origin (Haikou, Hainan, China).
For patients with a platelet count
This study included a total of 6 patients, with ages ranging from 24–33 years.
All patients were admitted to hospital after 32 weeks of gestation. Additionally,
all patients were primigravid (i.e., first pregnancy). The primary reason for
admission was detection of a low platelet count during prenatal examination. Most
patients were asymptomatic, with only one patient (Case 6) presenting with skin
ecchymoses and epistaxis. Some patients had a previous diagnosis of
thrombocytopenia. Initial laboratory tests revealed the platelet counts ranged
from 3–17
For patients with a platelet count
The treatment strategy was critically important due to the high maternal-fetal
risks associated with severe thrombocytopenia, particularly when the platelet
count falls below 10
| Case | Age (years) | Gravidity and parity | Gestational age at admission | Platelet count at admission/ |
Treatment regimen after admission | Intraoperative blood loss (mL) | Discharge platelet count/ |
Follow-up platelet count | |||
| Blood transfusion/therapeutic unit | Corticosteroids | rhTPO | IVIG/g | ||||||||
| 1 | 28 | G1P0 | 32 + 6 w | 6 (2024.07.08) | 5 | 40 mg qd | 15,000 | 22.5 | 500 | 84 (2024.07.12) | 51 (2024.9.2) |
| 2 | 24 | G1P0 | 32 + 6 w | 17 (2024.08.13) | 2 | 50 mg qd | 15,000 | 22.5 | 600 | 110 (2024.08.23) | 81 (2024.8.30) |
| 3 | 29 | G2P0 | 34 + 2 w | 8 (2024.08.31) | 3 | 50 mg qd | 15,000 | 22.5 | 500 | 49 (2024.09.05) | 29 (2024.9.14) |
| 4 | 27 | G1P0 | 32 + 4 w | 16 (2024.09.20) | 2 | 50 mg qd | 15,000 | 22.5 | 500 | 48 (2024.09.24) | 118 (2024.12.25) |
| 5 | 29 | G2P0 | 33 + 2 w | 9 (2024.11.30) | 3 | 15 mg qd | - | - | 600 | 90 (2024.12.02) | Lost to follow up |
| 6 | 33 | G2P0 | 34 + 5 w | 3 (2024.12.03) | 3 | 50 mg qd | 15,000 | 22.5 | 400 | 294 (2024.12.14) | Lost to follow up |
G, gravidity; P, parity; w, week; rhTPO, recombinant human thrombopoietin; IVIG, intravenous immunoglobulin.
Patient #5 is a highly instructive case. This pregnant woman was diagnosed with
severe thrombocytopenia platelets (PLT)
During hospital admission, patient #5 declined treatments such as IVIG and
TPO-RAs due to financial constraints, opting instead for platelet transfusion
followed by cesarean delivery. She continued prednisone treatment at 15 mg daily
(initiated in first trimester). Prior to surgery, the transfusion of two units of
platelets rapidly increased her platelet count to 44
To address potential uterine atony during cesarean section, all patients
received intravenous oxytocin and carbetocin to promote uterine contractions.
Despite these interventions, some patients experienced suboptimal uterine contractions. The estimated blood loss during surgery ranged between 400–600 mL
across the patient group. Neonatal outcomes were favorable. One newborn had Apgar
scores of 7-9-9, while the remaining five scored 9-10-10. Due to prematurity, all
6 newborns were transferred to the Neonatal Intensive Care Unit (NICU) for
specialized medical care and monitoring. No visible congenital anomalies were
observed in any of the newborns. Birthweights ranged from 1600–2790 g,
reflecting the preterm nature of the deliveries. The newborn in Case 1 presented
with thrombocytopenia (platelet count 66
| Case | Apgar score | Birthweight (g) | Neonatal platelet count | Cutaneous ecchymoses and petechiae | Discharge platelet count | Length of hospital stay (days) |
| 1 | 7 (skin color–1, muscle tone–1, respiratory effort–1) - 9 (muscle tone–1) - 9 (muscle tone–1) | 1600 | 66 | scattered hemorrhagic spots on both lower limbs | 232 | 9 |
| 2 | 9 (skin color–1) – 10 – 10 | 2450 | 165 | None | 159 | 5 |
| 3 | 9 (skin color–1) – 10 – 10 | 2790 | 115 | None | 135 | 8 |
| 4 | 9 (skin color–1) – 10 – 10 | 2220 | 120 | None | 355 | 7 |
| 5 | 9 (skin color–1) – 10 – 10 | 1870 | 303 | None | 240 | 10 |
| 6 | 9 (skin color–1) – 10 – 10 | 2600 | 159 | None | 241 | 9 |
This study reviewed the diagnostic and treatment processes for 6 patients with
severe ITP in late pregnancy. Our comprehensive therapeutic approach, comprising
prednisone, rhTPO and IVIG, as well as platelet transfusions when necessary,
yielded favorable outcomes in all cases. Following treatment, Cases 3 and 4 were
discharged with platelet counts of 49
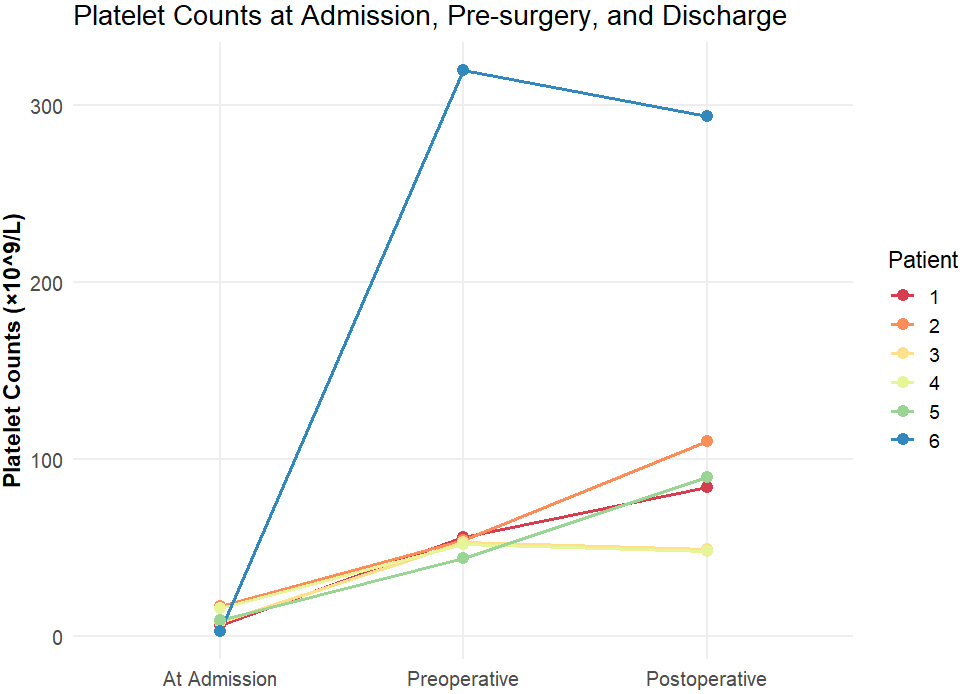 Fig. 1.
Fig. 1.
Platelet counts at admission, pre-surgery, and discharge.
This study analyzed 6 parturients with critical gestational thrombocytopenia
(PLT
PLT
PLT 10–20
The limited sample size of this study limits the generalizability of results, but the above protocol demonstrates clinical feasibility. Individualized treatment protocols and MDT consultations also played crucial roles. Treatment intensity was calibrated according to the platelet count, clinical manifestations (such as epistaxis), and gestational age, with close monitoring of platelet level fluctuations throughout therapy. Complex cases benefited from treatment plans formulated after consultation with hematology and rheumatology/immunology departments, or hospital-wide clinical conferences.
The limitations are that case series inherently may have limitations due to the small sample size and lack of a control group.
In conclusion, ITP during pregnancy requires an individualized and comprehensive treatment approach. A prednisone-based regimen, combined with rhTPO and IVIG, as well as platelet transfusion when necessary, can lead to platelet recovery, ameliorate clinical symptoms, and safeguard maternal and fetal well-being. To achieve optimal outcomes, treatment should be modified according to the condition of each patient, gestational age, and dynamic changes in platelet counts. For patients with profound thrombocytopenia, more aggressive treatment protocols may be necessary to ensure safe delivery, including emergency measures such as platelet transfusions.
The data supporting this study’s findings are available from the corresponding author upon reasonable request.
XZ, HQ was responsible for the conceptualization of the research. CC conducted the investigation. HQ participated in the review and editing of the manuscript. CC, JR, HQ analyzed the data. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
The study was carried out in accordance with the guidelines of the Declaration of Helsinki, and the protocol was approved by the Ethics Committee of Sichuan Provincial People’s Hospital (approval number: [20240801012]). All patients gave written informed consent when they participated in the study.
We would like to express our sincere gratitude to all those who helped us during the writing of this manuscript. Special thanks also go to the reviewers for their valuable comments and suggestions, which have significantly improved the quality of this paper.
The work was supported by Foundation of Science Popularization Training Project of Sichuan Provincial Department of Science and Technology (2024JDKP0048).
The authors declare no conflict of interest.
Supplementary material associated with this article can be found, in the online version, at https://doi.org/10.31083/CEOG38783.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.